
Abstract
The constraint level of TKR is essential for ensuring product performance to prevent knee joint dislocation. Computer modeling and simulation (CM&S) technology is widely used in the medical device industry due to its advantages such as reducing testing time and costs. However, there is a lack of research on the constraint level of TKR according to the size and flexion angle of the femoral component. In this study, the constraint levels of AP draw, ML shear, and rotary laxity were tested according to the size and flexion angle of TKR products using finite element analysis. A TKR model was constructed using a 3D scanner, and a finite element model with mechanical testing and error rates of 2.49% and 3.00% was developed through AP draw testing. In AP draw, as the size of TKR decreases, the constraint level increases by about 3.6%, and rotary laxity also increases by about 1.3%. In all tests, the constraint level increased as the bending angle of the femoral component increased. We found that the curvature and contact area of a TKR influenced the constraint level. Through this study, it is believed that CM&S technolaogy can be widely used in evaluating the unique performance of medical devices.
Similar content being viewed by others

1 Introduction
Total knee replacement (TKR) is a common orthopedic surgery that allows many patients suffering from pain and movement restrictions due to degenerative arthritis, inflammatory arthritis, and avascular necrosis to improve their quality of life [1]. In addition to the patient'’s bone stock and soft tissue capacities, the unique features of TKR products must also be considered to select the appropriate TKR procedure for the patient [2]. In particular, the constraint level of TKR products must be evaluated in conjunction with the condition of the patient’s soft tissues to prevent dislocation and allow the knee joint to function normally. For example, a patient with good soft tissue health may need a TKR with a lower constraint level, while a patient with poor soft tissue health may require a TKR with a higher constraint level.
Therefore, regulatory agencies such as the Food & Drug Administration (FDA) in the US, and the Ministry of Food & Drug Safety (MFDS) in South Korea require that data on TKR constraints be provided to obtain approval for sales and clinical use [3]. The ASTM F1223 specification covers the standard method for quantitatively testing the constraint level of TKR products. It provides methods for evaluating the constraint level for anterior–posterior (AP) draw, medial–lateral (ML) shear, rotary laxity, varus-valgus rotation, and distraction [4].
Haider and Walker investigated the influence of all degrees of freedom of motion, excluding translation and rotation along the specified directions being tested during AP draw and internal–external rotation tests [5]. Moran et al. used computer simulation to assess the constraint levels of AP draw and internal/external rotation using a single TKR model. They subsequently validated these findings through mechanical testing [6]. These studies evaluated a single TKR model and did not evaluate the effects according to the TKR model’s size and flexion angle. ASTM F1223 requires constraint levels to be assessed at flexion angles of 0°, 30° and 90°. If there are products with different sizes, the worst case that evaluates the lowest constraint level must be selected.
In this study, the constraint levels of AP draw, ML shear, and rotary laxity were tested according to the size and flexion angle of TKR products using finite element analysis. The aim was to assess the effects of product size and flexion angle. A finite element model for evaluating TKR constraint levels was developed, and subsequently validated by comparing its outcomes with mechanical test results obtained through dedicated equipment.
2 Material and Method
2.1 FE Model for TKR
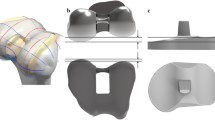
The TKRs used in this study were ATTUNE Knee Systems (Large size: #8, Small size: #3) from DePuy Synthes, which are widely used in clinical practice. The components of the differently sized TKRs (femoral component, insert, baseplate) were modeled in three dimensions using a 3D scanner (MetraScan Black Elite, Creaform, CA). The femoral component jig, baseplate jig, and rail were designed using SolidWorks 2016 (Dassault System, Massachusetts, USA) to assign loads and boundary conditions to the TKR. Simplification was performed by integrating the jig with each TKR component to reduce finite element analysis time and errors. The femoral component was placed at 0°, 30°, and 90° of flexion (Fig. 1). The material properties of the femoral component, baseplate, and jig (femoral component jig, baseplate jig, rail) were Co-Cr–Mo ally (CoCr, Young’s modulus = 21,000 MPa, Poisson’s rate = 0.33) [7]. The material properties of the insert were ultra-high molecular weight polyethylene (UHMWPE, Young’s modulus = 900 MPa, Poisson’s rate = 0.42) (Table 1) [8].

Modeling of total knee replacement and jig rail
2.2 Loading and Boundary Condition
A tie contact condition was applied as a common boundary condition, assuming the insert and baseplate were completely tied and there was no friction between the baseplate jig and rail. In addition, a 0.05 friction coefficient was applied between the femoral component and the insert [9]. As for the loading conditions, a vertical load of 710 N (BW 70 kg) was applied to the upper jig based on ASTM F1223-20 (Fig. 2).

DOF of constraint test
In the AP draw test, two degrees of freedom were applied for translation and valgus-varus rotation in the TKR’s ML direction, and the baseplate (with jig) was translated by 15 mm each in the anterior and posterior directions. In the ML shear test, two degrees of freedom were applied for translation in the AP direction, and the baseplate (with jig) was translated by 15 mm in the medial direction. In the rotary laxity test, two degrees of freedom were applied for translation in the AP direction and valgus-varus rotation, and the femoral component (with the jig) was rotated by 30° (Fig. 2).
All simulations were run using ABAQUS (Dassault Systemes Simulia Corp., Johnston, RI, USA), a commercial software package for finite element analysis. The elements of each component were implemented as C3D10 tetrahedral elements, and the analysis was performed by applying isotropic and homogeneous material properties.
2.3 Mechanical Test for FE Model Validation
In this study, a proprietary TKR constraint level tester was fabricated to validate the finite element model (Fig. 3). The testing apparatus is designed to facilitate monitoring and control of axial loads, lateral loads, and lateral displacements.

Total knee replacement mechanical test system
A load cell is mounted on a stage capable of lateral movement to measure the constraint levels of Total Knee Replacement (TKR) originating from the Anteroposterior (AP) or Mediolateral (ML) directions. Lateral displacement is monitored using a linear stage with a step motor, where the motor rotation angle and screw lead are calculated for accurate tracking. All sensors used in the testing apparatus undergo prior calibration.
The baseplate-fixed stage utilizes low-friction linear bearings in both the AP and ML directions, allowing free movement. Varus-valgus rotation is facilitated by bearings, permitting unrestricted rotation. The femoral component can be securely affixed at various flexion angles (0, 30, 45, 60, 90, and 120 degrees) using a jig, which is then fixed to the top of the testing apparatus. Vertical loads are applied using weight hangers, ensuring a consistent load. This advantageously allows for a constant load even during axis displacement caused by flexion in constraint-level testing.
The femoral component can be fixed at the top of the tester and a constant vertical load can be applied with a weight. The baseplate and insert can be fixed at the bottom of the tester, allowing the system to achieve two degrees of freedom by enabling X-axis translation and Y-axis rotation. The system uses a motor to enable movement in the Y-axis (artificial translation in the AP or ML direction) at a constant speed for constraint tests.
Mechanical testing to assess the constraint level on the large size (#8) model was performed in the AP direction at 0° flexion, according to the ASTM F1223 test method. A vertical load of 710 N, equivalent to an adult’s body weight of 70 kg, was applied. The lower plate was then moved at a speed of 10 mm/s to simulate artificial dislocation. The displacement and force generated were recorded at a rate of 10 Hz and compared with the finite element analysis results.
3 Results
3.1 FE Modeling
Finite element models of the TKR components (femoral component, insert, baseplate) and jig (femoral component jig, baseplate jig, rail) were created using ABAQUS software, as shown in the table. The contact surface between the femoral component and the insert was adjusted in more detail.
In the mesh convergence study, refinement of element sizes was conducted for the AP model at a 0-degree flexion angle until the contact pressure and constraint level exhibited convergence with less than 5% change from one mesh size to the next. The element sizes were reduced in increments of 0.5 mm from 5 to 1 mm. It was observed that the element sizes of the femoral component and insert converged when they were below 3 mm and 1 mm, respectively.
3.2 Validation of FE Model
The mechanical test results in the AP direction showed that the maximum constraint level required for TKR dislocation in the anterior and posterior directions was 422.57 N and 205.87 N, respectively. The simulation results were 412.01 N in the anterior direction and 212.06 N in the posterior direction. The errors between the mechanical test and simulation results were 2.49% and 3.00%, respectively (Fig. 4). Both figures fell within the 5% validation error range specified in ASME V&V 40, confirming the reliability of the TKR finite element model used in this study.

Comparison of simulation with mechanical test results: validation
3.3 Constraint of TKR
In the case of the AP draw test, different TKR sizes yielded varying constraint levels. Specifically, for the large-size TKR, measurements showed 412.01 N and 212.06 N in the anterior and posterior directions, respectively. Conversely, the small-size TKR showed constraint levels of 426.86 N and 209.89 N in the anterior and posterior directions, respectively. As the TKR size decreased, the constraint level increased in the anterior direction and decreased in the posterior direction. In rotary laxity, the results were 9.57 N m for large size TKR and 10.71 N m for the small size. Similar to the AP draw, the smaller the TKR, the higher the constraint level (Fig. 5).

Simulation results according to TKR size: a AP Draw; b Rotary laxity
As for the difference in constraint level according to the flexion angle, the constraint level decreased as the flexion angle increased in AP draw, with 426.86 N, 411.08 N, and 411.19 N measured at 0°, 30° and 90° in the anterior direction, respectively. The same trend was observed in the posterior direction with 209.89 N, 210.98 N, and 207.45 N, respectively. In ML shear, 426.86 N, 380.37 N, and 379.35 N were measured at 0°, 30° and 90°, respectively. In rotary laxity, the results were 10.71 N m, 10.87 N m, and 10.92 N m, showing the same trend as the AP draw (Fig. 6).

Simulation results according to flexion angle: a AP Draw; b ML shear; c Rotary laxity
4 Discussion
The constraint level of TKR is essential for ensuring product performance to prevent knee joint dislocation. It also plays a fundamental role in the selection of an appropriate implant according to the patient’s soft tissue conditions. However, performing constraint-level tests for various product sizes and all required flexion angles to determine worst-case scenarios is costly and time-consuming. This is due to repeated specimen fabrication and testing procedures [10]. Recently, computational modeling with finite element analysis has begun replacing these bench tests as a tool for evaluating medical devices [11,12,13,14]. However, regulatory agencies rarely acknowledge simulation results due to reliability issues. In this study, a finite element model was developed to assess TKR constraint levels using finite element analysis. The model’s reliability was then validated by comparison with a mechanical testing system. Also, the effect on constraint level according to TKR size and flexion angle was analyzed to help select the worst-case TKR.
At the same angle, it was found that smaller product sizes were associated with higher constraint levels. This indicates that the curvature of the femoral component and insert, which form the articular surface of the TKR, affects the constraint level. The size and curvature of a TKR are generally proportional to its size. In particular, as the curvature of the insert decreases, the inclination of the femoral component’s moving path increases relatively, thus increasing the constraint level. The results are consistent with research results that show that the lower the curvature of the articular surface in TKR design elements, the higher the constraint level [15].
As the flexion angle increased, the constraint level decreased, which was believed to be due to changes in the contact area caused by differences in the femoral component’s curvature. As for the TKR used in this study, the contact area between the femoral component and the insert decreased as the flexion angle increased. In particular, the largest change occurred when the flexion angle increased from 0° to 30°, which was consistent with the analysis results, in which the constraint level was lower at 30° than at 0°. The same trend was also observed in ML shear and rotary laxity. These results show that the contact area affects the constraint level in an environment where the same insert flexion, vertical load, and friction coefficient are applied.
Constraint tests using finite element analysis have clear advantages over bench tests. Using a validated finite element model based on ASME V&V 40 will enable the assessment of unique TKR product performance and facilitate design validation during the development process [16]. Regulatory authorities in the US, Korea, and Europe are issuing related guidelines and standards to recognize the results of product-specific performance evaluation through finite element analysis [17]. Furthermore, as ASTM International is also publishing more standards for medical device evaluation using finite element analysis, their scope of application will gradually expand [18, 19].
This study has some limitations. First, it used only one product, and while the curvature of the articular surface is generally determined in proportion to the product’s size, further research is needed in this area. Second, the study conducted a quasi-static analysis without considering time. The results of the quasi-static analysis are significant because their reliability was confirmed through mechanical tests. However, future research applying dynamic analysis is also necessary. Third, the viscoelastic properties of UHMWPE were not applied. TKR constraint tests were performed within the elastic range of all materials, with careful consideration to avoid any material deformation.
5 Conclusion
In this study, a finite element model was developed and its reliability was validated through comparison with mechanical tests. The model was then used to analyze the impact on constraint level according to TKR size and flexion angle. The findings of this study will contribute to assessing unique product performance using a finite element model validated through TKR constraint-level tests. Furthermore, this will promote the increased use of computer simulations in the development of medical devices.
References
Fornalski, S., McGarry, M. H., Bui, C. N., Kim, W. C., & Lee, T. Q. (2012). Biomechanical effects of joint line elevation in total knee arthroplasty. Clinical Biomechanics, 27(8), 824–829. https://doi.org/10.1016/j.clinbiomech.2012.05.009
Halewood, C., Athwal, K. K., & Amis, A. A. (2018). Pre-clinical assessment of total knee replacement anterior-posterior constraint. Journal of Biomechanics, 73, 153–160. https://doi.org/10.1016/j.jbiomech.2018.03.042
Orthopedic Devices Branch Division of General, Restorative, and Neurological Devices, Office of Device Evaluation. (2013). Knee joint patellofemorotibial and femorotibial metal/polymer porous-coated uncemented prostheses - Class II special controls guidance document for industry and FDA. Food and Drug Administration.
Orthopedic and Restorative Device Division. (2020). Guidance Cobalt-chrome alloy manufactured by 3D printer artificial joint. National Institute of Food and Drug Safety Evaluation.
ASTM International. (2020). F1223–20 standard test method for determination of total knee replacement constraint. ASTM International. https://doi.org/10.1520/F1223-20
Haider, H., & Walker, P. S. (2005). Measurements of constraint of total knee replacement. Journal of Biomechanics, 38(2), 341–348. https://doi.org/10.1016/j.jbiomech.2004.02.014
Moran, M. F., Bhimji, S., Racanelli, J., & Piazza, S. J. (2008). Computational assessment of constraint in total knee replacement. Journal of Biomechanics, 41(9), 2013–2020. https://doi.org/10.1016/j.jbiomech.2008.03.020
De Ruiter, L., Janssen, D., Briscoe, A., & Verdonschot, N. (2017). A preclinical numerical assessment of a polyetheretherketone femoral component in total knee arthroplasty during gait. Journal of Experimental Orthopaedics, 4, 1–8. https://doi.org/10.1186/s40634-017-0078-4
Cawley, D. T., Kelly, N., Simpkin, A., Shannon, F. J., & McGarry, J. P. (2012). Full and surface tibial cementation in total knee arthroplasty: A biomechanical investigation of stress distribution and remodeling in the tibia. Clinical Biomechanics, 27(4), 390–397. https://doi.org/10.1016/j.clinbiomech.2011.10.011
Askari, E., & Andersen, M. S. (2021). On the effect of friction on tibiofemoral joint kinematics. Applied Sciences, 11(16), 7516. https://doi.org/10.3390/app11167516
Office of Device Evaluation. (2016). Reporting of computational modeling studies in medical device submissions- Guidance for industry and food and drug administration staff. Food and Drug Administration.
Baumann, A. P., Hsieh, M. T., Dmitriev, A. E., & Lotz, J. C. (2023). The relative influence of model parameters on finite element analysis simulations of intervertebral body fusion device static compression performance. Computer Methods in Biomechanics and Biomedical Engineering, 26(14), 1742–1751. https://doi.org/10.1080/10255842.2022.2139145
Bae, T. S., & Kwak, D. S. (2022). Biomechanical effects of loop thickness in ACL graft: A simulation study. International Journal of Precision Engineering and Manufacturing, 23(2), 205–211.
Yi, J. W., Kim, J. U., Kim, A. Y., Oh, B. H., Ahn, J. Y., & Tae, K. S. (2022). Evaluating the stability of locking screw on locking compression plate according to various screw insertion angles. International Journal of Precision Engineering and Manufacturing, 23(7), 789–796.
Yadav, S. K., Sikidar, A., & Kalyanasundaram, D. (2023). Design of polymeric orthopedic screws with variable stiffness and multi-objective optimization of injection molding process. International Journal of Precision Engineering and Manufacturing, 24(4), 629–643.
Willing, R., & Kim, I. Y. (2011). Design optimization of a total knee replacement for improved constraint and flexion kinematics. Journal of Biomechanics, 44(6), 1014–1020. https://doi.org/10.1016/j.jbiomech.2011.02.009
The American Society of Mechanical Engineering. (2018). Assessing credibility of computational modeling through verification and validation: Application to medical devices V&V 40. The American Society of Mechanical Engineering.
Center for Devices and Radiological Health. (2023). Assessing the credibility of computational modeling and simulation in medical device submissions- Guidance for industry and food and drug administration staff. Food and Drug Administration.
ASTM International. (2016). F3161–16 standard test method for finite element analysis (FEA) of metallic orthopaedic total knee femoral components under closing conditions. ASTM International. https://doi.org/10.1520/F3161-16
ASTM International. (2020). F2996–20 standard practice for finite element analysis (FEA) of non-modular metallic orthopaedic hip femoral stems. ASTM International. https://doi.org/10.1520/F2996-20
Acknowledgements
This research was supported by a Grant (RS-2023-00215638) from Ministry of Food and Drug Safety in 2023.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kang, KS., Jung, TG. Finite Element Analysis and Mechanical Assessment for the Constraint of Total Knee Replacement. Int. J. Precis. Eng. Manuf. 25, 843–849 (2024). https://doi.org/10.1007/s12541-024-00986-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12541-024-00986-w