
Abstract
Background
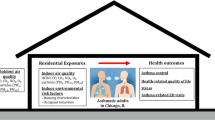
Outdoor air pollution, including ozone (O3) pollution, and childhood family environments may interact and impact asthma exacerbations in children. Previous epidemiology studies have primarily focused on stress in the home, rather than support, and whether psychosocial factors modify the association between pollution and health outcomes, rather than whether pollution exposure modifies associations between psychosocial factors and health outcomes.
Methods
Data from the cross-sectional 2003 representative, population-based California Health Interview Survey were linked with air quality monitoring data on O3 pollution from the California Air Resources Board. Adolescents (N = 209) ages 12–17 who reported an asthma diagnosis and lived within 5 mi of the nearest air monitoring station had linked O3 data for a 12-month period preceding the survey interview date. Adolescents reported perceived available support from an adult at home and frequency of asthma symptoms.
Results
In unadjusted models, for adolescents living in high O3 pollution regions, greater perceived support was related to lower asthma symptom frequency. Follow-up analyses suggested that the most plausible interpretation of the interaction was that O3 exposure modified the association between perceived support and symptom frequency. O3 × perceived support interactions were not statistically significant after adjusting for covariates.
Conclusions
These data provide preliminary evidence that the association between the lack of support in the home environment and worse asthma symptoms may be stronger in areas with higher O3 exposure. Future work may benefit from incorporating personal pollution exposure assessments, comprehensive family environment assessments, and longitudinal follow-up of asthma exacerbations over time.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Environmental exposures that can impact asthma severity range from the composition of the air that children breathe [1,2,3] to the quality of the home family environment [4,5,6,7]. Environmental and social exposures likely interact, which may explain why the association between outdoor air pollution and asthma exacerbations in children and adolescents has a small and heterogeneous effect size (ORs between 1.03 and 1.05) [2, 3]. Contributors to heterogeneity include the wide range, mix, and sources of pollutants, including ozone (O3,) nitrogen oxides (NOx), and particulate matter and individual “host factors” (gender, age, race/ethnicity, etc.) [1]. Unpacking such heterogeneity is critical for developing personalized asthma control strategies [8] that can mitigate the harmful effects of different exposures.
Innate immune-mediated inflammation may explain how pollution and the home family environment interact to impact asthma symptoms [4,5,6]. In the airways, pollutants can increase oxidative stress, stimulate innate immune responses, and enhance acquired immune responses to inhaled allergens implicated in allergic asthma, thereby worsening asthma symptoms [1]. Moreover, growing up in a family characterized by high conflict and low warmth may prime the immune system to vigorously respond to danger signals such as cellular damage caused by environmental pollutants [4,5,6, 9, 10]. At the same time, innate immune responses may influence social cognition and behavior [11] via neural pathways involved in social information processing [12,13,14] which may then have downstream impacts on peripheral inflammation [15]. While biologically plausible, epidemiological data are needed to provide evidence of the phenomenon and inform the direction of the interaction. That is, does the social environment modify the association between pollution exposure and asthma outcomes, or does pollution exposure modify the association between social environments and asthma outcomes?
Two studies in the Los Angeles region, which ranks near or at the top of the list of most polluted cities in the USA [16], primarily focused on stressful family environments magnifying the association between pollution exposure and respiratory function [17, 18]. In the Children’s Health Study (N = 1,399), the association between higher NO and NOx exposure at home and lower forced expiratory volume was larger for children whose parents reported high perceived stress [17]. In the Los Angeles Family and Neighborhood Survey (N = 551), greater NOx exposure was related to worse lung function for children without a father at home [18]. In both studies, psychosocial factors did not show a main effect association with lung function and measures of the family psychosocial environment were limited — neither included well-validated child reports of conflict or support in the family environment. Moreover, neither study focused on children with diagnosed asthma nor reported whether pollution exposure modified the association between psychosocial factors and lung function.
Thus far, the only study to report whether the association between psychosocial factors and lung function in children with asthma might be modified by pollution exposure comes from a sample of 73 children and adolescents with asthma [4]. At lower relative levels of nitrogen dioxide (NO2) exposure, greater chronic stress exposure was related to worse lung function. At higher relative levels of NO2 exposure, greater chronic stress exposure was related to better lung function. Importantly, the study was conducted in Vancouver, British Columbia, Canada, which has a lower air pollution burden compared to many urban areas around the world, including in the USA [19].
The aforementioned studies focused on stress and conflict, but the balance of conflict and support in the home plays a central role in how family relationships impact children’s health [20]. Support in the home, defined as interpersonal interest, involvement, and assistance [21] may protect children from the detrimental effects of environmental exposures on health through pathways that include greater medication adherence [22] and lower innate immune-mediated inflammation [23]. However, to date no studies have examined whether support in the home environment may interact with pollution exposure to impact asthma symptoms.
Thus, using cross-sectional data from the 2003 biennial, population-based California Health Interview Survey (CHIS), this study examined whether support from an adult in the home interacted with pollution exposure to predict asthma symptom frequency in adolescents with asthma. In addition to including questions about perceived social support in the home environment [24], respondents’ residential addresses in the 2003 CHIS were linked to air pollution data from the nearest California Air Resources Board (CARB) air monitoring station.
We focused on O3, which is formed through chemical reactions involving NOx, volatile organic compounds, and solar radiation and importantly has a more uniform spatial distribution compared to other pollutants [2, 25]. In addition, ambient outdoor O3 exposure levels may be more accurately estimated for adolescents who spend more time outdoors compared to very young children [25]. Data from air monitoring stations, while limited compared to exposure modeling [26], may provide proof of concept for examining interactions between pollution exposure and the family psychosocial environment, even after controlling for family socioeconomic status as a background stressor. We explored two possibilities: (1) greater perceived support may buffer against the negative impact of O3 exposure on asthma outcomes, such that in adolescents reporting higher perceived support, we would observe no association between O3 exposure and asthma symptom severity, or (2) greater O3 exposure may increase sensitivity to the social environment, such that for adolescents living in regions characterized by high air pollution, greater perceived support at home would be related to lower asthma symptoms and exacerbations.
Methods
Participants and Procedures
The 2003 CHIS Adolescent sample (N = 4010 between ages 12 and 17 [27]), was obtained through a random-digit dial telephone survey of households from August 2003 to February 2004, within 41 geographic strata representing all counties in California, with oversampling of underrepresented minority households. In households with children, one child (age < 12) and/or one adolescent was randomly selected and interviewed after obtaining parent/guardian consent [details in 24]. Interviews lasted an average of 21.5 min [24]. The overall household response rate was 57.3% for the adolescent interview and 83% in households where parents gave permission for the adolescent interview. For this study, respondents (N = 476) were included if they responded “yes” to the question “Has a doctor ever told you or your parents that you have asthma?” and “yes” to one of the following two questions: “Do you still have asthma?” or “During the past 12 months, have you had an episode of asthma or an asthma attack?” Participant data was linked to data from the nearest CARB air monitoring station within 20 mi of the respondent’s residential address (Esri ArcGIS, Redlands, CA) or nearest cross-streets or zip codes if residential address was not available (4.2% and 11.9% of the sample, respectively). Because the spatial variability of ozone increases considerably after 5 mi from air monitoring sites, similar to prior work with these data [25], we further restricted analyses to participants who lived within 3 and 5 mi of the nearest air monitoring station (N = 112 and 209, respectively; participant characteristics are shown in Table 1). Secondary data analyses of CHIS data were approved by UCLA’s Institutional Review Board.
Measures
Ozone Pollution
Annual averages of daily 8-h maximums provided by CARB were computed for the 12-month period preceding the respondent’s CHIS interview date. At least 15 daily values/month had to be available for a given monthly average. Annual averages were then computed for participants who had 12 monthly values available. For regression analyses, annual average O3 was scaled by 10 ppb (descriptive statistics are reported as in 1 ppb units), a common practice in epidemiological studies of air pollution.
Perceived Support at Home
Adolescents were asked to endorse how true (1 = not at all true, 4 = very much true) the following six statements were about “your home or the adults with whom you live” and whether there was a parent or some other adult in the home who “cares about your schoolwork,” “listens to you,” “talks with you about your problems,” “wants you to do your best,” “believes you will be a success,” and “notices your bad moods.” The first five items were derived from a measure of supportive relationships at home that is part of an optional module of the California Healthy Kids SurveyFootnote 1 assessing environmental assets that contribute to resilience [28]. Responses were averaged across items (Cronbach’s α = 0.80). The perceived support from an adult at home score was negatively skewed, as most adolescents reported support in the “pretty much true” to “very true” range (Table 1). These items have only appeared on the 2003 and 2016 CHIS Adolescent surveys.
Asthma Outcomes
Adolescents responded 1 = not at all, 2 = less than once a month, 3 = monthly, 4 = every week, or 5 = every day, to a single item about past 12-month frequency of symptoms: “how often have you had asthma symptoms such as coughing, wheezing, shortness of breath, tightness or phlegm?” The primary outcome was symptom frequency analyzed as a continuous dependent variable. As a secondary outcome, respondents were defined as having persistent asthma (with 4 = daily or 5 = weekly symptoms) vs. intermittent asthma (with 3 = monthly, 2 = less than monthly, or 1 = no symptoms)Footnote 2 [30, 31]. Secondary asthma-related outcomes included two yes or no items: “have you had an episode of asthma or an asthma attack” and “have you visited the emergency room (ER) or urgent care for asthma” in the past 12 months.
Covariates
Adjusted models included the following covariates: adolescent-reported age (in years, centered); gender (0 = male); race/ethnicity including White, African American, Latino and all others; and current daily prescription asthma medication use (0 = none); parent-reported health insurance status (0 = currently insured); and calculated poverty level based on parent-reported household income and size (301% federal poverty level and above, 201–300%, 101–200%, and 0–100%) (more information available at [30]).
Data Analysis
The two-stage geographically stratified random-digit dial sample design of CHIS required proper weighting and variance calculation using jackknife replicate weights to reduce selection and non-respondent biases [24]. Weighting adjustments used a raking method that accounted for demographics, geographic variables, household composition, and socioeconomic variables. These sample weights were applied in all data analyses. Any missing values were replaced by random selection from the distribution of respondents and hot deck imputation without replacement. All analyses described below were repeated with adolescents living ≤ 3 mi and ≤ 5 mi from the nearest air monitoring station. The ≤ 3 mi sample, while it has a smaller sample size, should have more accurate estimates of O3 for a given individual. The ≤ 5 mi sample has a larger sample size; depending on the radius of adolescents’ daily activity areas, this might still provide a valid O3 measurement for a given individual.
Our primary dependent variable of interest was asthma symptom frequency, which was analyzed using linear regressions, and significant statistical interactions between support and O3 were interpreted by computing simple slopes and Johnson–Neyman regions of significance [32]. Secondary dependent variables modelled with logistic regressions were likelihood of having intermittent vs. persistent asthma over the past year, likelihood of having an asthma episode/attack, and an ER or urgent care visit for asthma in the past 12 months. Unless otherwise specified, all regression coefficients (B’s) are unstandardized, and values between brackets indicate 95% CIs.
Results
Descriptive Statistics for Asthma Outcomes
Adolescent-reported symptom frequency corresponded to between less than once a month to every month (Table 1). Most adolescents reported intermittent symptoms (59.8–60.7%). Just over one-third of the sample reported taking daily prescription controller medication, and one-third of the sample reported experiencing an episode or attack in the past 12 months. The prevalence of ER/urgent care visits in the past 12 months was < 10%.
Associations Among Demographics, Asthma Outcomes, Ozone Pollution, and Support
Higher O3 was related to higher perceived support, ≤ 3 mi B = 0.47 [0.10, 0.84], p = 0.013, R2 = 0.07, and ≤ 5 mi B = 0.40 [0.12, 0.69], p = 0.006, R2 = 0.04. O3 was not related to asthma symptom frequency at ≤ 3 mi, B = − 0.13 [− 0.37, 0.11], p = 0.29, or ≤ 5 mi, B = − 0.06 [− 0.26, 0.13], p = 0.51.
To present associations among demographics, perceived support, and asthma outcomes, we focus on the ≤ 5 mi sample. Perceived support was not related to age, race/ethnicity, daily medication use, or having insurance. Adolescents from the lowest poverty level (0–99%) reported less perceived support compared to adolescents from the highest poverty level (> 300%), B = − 0.25 [− 0.46, − 0.04], p < 0.05; perceived support did not differ between the three highest poverty level groups. Older children reported greater symptom frequency, B = 0.10 [0.004, 0.20], p = 0.042. However, symptom frequency and medication use were not related to sex, race/ethnicity, poverty level, or having insurance. Reporting using daily asthma medication use was related to higher symptom frequency, B = 0.67 [0.31, 1.04], p < 0.001. The likelihood of having an asthma attack or visiting the ER/urgent care in the past year was not related to age, sex, poverty level, or insurance status. White adolescents were more likely to report an asthma attack in the past year, OR = 2.81 [1.01, 7.83], p = 0.048, compared to Latino adolescents (the reference group, which did not differ from African American or American Indian/Asian/Pacific Islander/other categories). Children in the American Indian/Asian/Pacific Islander/other category were less likely to visit the ER, OR = 0.23 [0.08, 0.68], p = 0.009, compared to Latino adolescents (who did not differ from African American or White adolescents).
Primary Analyses: Support × Ozone Pollution Interactions
When asthma symptom frequency was treated as a continuous variable, there were no main effects of O3 and of perceived support on frequency of symptoms, and significant O3 × perceived support interactions were observed for participants living ≤ 3 and ≤ 5 mi of an air monitoring station but only in unadjusted models (top portion of Table 2). We computed two sets of Johnson–Neyman regions of significance, one where support was the moderator and the other where O3 exposure was the moderator. When support was the moderator, the region of significance for the association between O3 exposure and symptom frequency becoming statistically significant was well outside the plausible range of values for the support moderator. Thus, the most plausible interpretation of the interaction was that O3 exposure modified the association between perceived support and symptom frequency. Figure 1A shows that in the ≤ 5 mi sample, high perceived support at home was related to lower symptom frequency but only for adolescents living in a region with high O3 exposure. For example, the simple slope of the association between perceived support and symptom frequency in a low O3 exposure region (mean –1 SD) was 0.06 (SE = 0.21), t = 0.31, p = 0.76; by comparison, in a high O3 exposure region (mean + 1 SD), the simple slope was − 0.51 (SE = 0.25), t = -2.04, p = 0.045. Figure 1B shows that the slope of the association between perceived support and symptom frequency becomes statistically significant when O3 ≥ 48.8 ppb. However, after controlling for covariates, the O3 × perceived support interaction was in the same direction but no longer statistically significant (both ≤ 3 and ≤ 5 mi samples).

A Self-reported asthma symptom frequency as a function of yearly average O3 (− 2 SD to + 2 SD) and perceived support from an adult at home in the ≤ 5 mi sample. Points are jittered vertically and horizontally to minimize overlap. Orange lines and dots represent higher O3. B Slope of the association between perceived support from an adult at home and asthma symptom frequency, as a function of yearly average O3. The shaded region of significance indicates when the slope of the association between the perceived support from an adult at home and asthma symptom frequency is statistically significant, at ≥ 48.8 ppb. The unshaded region indicates the slope is not significantly different from zero at values < 48.8 ppb. The color version is available online. The figure is in grayscale in the print version
Approximately 40% of the sample reported persistent asthma symptoms (Table 1). Similar to the linear regressions, there were no main effects of O3 and of perceived support on likelihood of intermittent vs. persistent symptoms in unadjusted and adjusted models (Table 3). At the same time, there was a statistically significant O3 × perceived support interaction in unadjusted models (≤ 3 mi B = − 2.61 [− 4.3, − 0.92], t = − 3.1, p = 0.003; ≤ 5 mi B = − 1.08 [− 2.06, − 0.10], t = − 2.2, p = 0.035). Figure 2 shows that high perceived support at home was related to lower likelihood of persistent asthma symptoms but only for adolescents in a region with high O3 exposure. For example, in adolescents living in a high O3 exposure region (mean + 1 SD) in the ≤ 5 mi sample, the estimated probability of reporting persistent symptoms was 52.5% [30.8, 74.1] for those reporting –1 SD perceived support (3.27 on the 4-point scale) compared to 31.8% [15.7, 41.3] for those reporting perceived support = 4 (because of skew the mean + 1 SD was outside of the scale range).

Probability of persistent asthma in the past year as a function of yearly average O3 (− 1 SD and + 1 SD) and perceived support from an adult at home in the ≤ 5 mi sample. Bands represent 95% CIs around probability estimates. The color version is available online. The figure is in grayscale in the print version
In unadjusted and adjusted logistic regressions with the ≤ 3 and ≤ 5 mi samples, there were no main effects of O3 concentration or perceived support on the likelihood of an episode or attack, or ER/urgent care visits, or statistically significant O3 × perceived support interactions (all p’s > 0.09).
Discussion
As adolescents become more independent, knowing that adults/parents are available when needed takes on increasing importance [20]. In unadjusted models, consistent with prior theories [5, 6, 9, 10], among adolescents with 12-month average O3 exposure greater than 48.8 ppb, reporting more perceived support at home was related to lower asthma symptom frequency, and reporting less perceived support at home was related to greater risk of persistent asthma symptoms. While our analyses suggested that O3 exposure modified the association between perceived support and asthma symptoms, rather than perceived support buffering against the effects of O3 exposure, after adjusting for covariates, the O3 × perceived support interaction was no longer statistically significant. While associations with intermittent vs. persistent symptoms were independent of SES (% poverty level) and daily prescription asthma medication use, the same pattern did not extend to reporting an asthma attack or a visit to the ER or urgent care because of asthma in the past year. Prior studies focused on stress in the family environment [4, 17, 18]; while the findings should be considered preliminary, this is the first study to examine whether outdoor air pollution exposure may strengthen the associations between perceived support in the home and symptom severity.
Two primary reasons for considering the reported findings preliminary are the differences between unadjusted and adjusted models and the cross-sectional study design. In adjusted models, poverty level was the only covariate systematically related to perceived support and was not systematically related to symptom frequency. In contrast, several covariates showed relatively strong associations with symptom frequency, age, Latino or African American ethnicity, and taking daily prescription control medication, with the latter two related to lower symptom frequency. Notably, other analyses of CHIS data found higher likelihood of daily asthma medication use among Latino and African American children [31, 33]. Thus, accounting for more severe symptoms in Latino and African American adolescents, as well as adolescents whose asthma severity necessitates daily asthma controller medications, may have reduced the O3 × perceived support effect.
These preliminary, cross-sectional data suggest several plausible interpretations that should be explored in future prospective longitudinal work. First, by increasing airway inflammation, pollution may also increase neural sensitivity to social experiences, which may further increase systemic and airway inflammation contributing to symptom severity. O3 interacts with molecules in the airway to stimulate innate inflammatory responses from lung macrophages and dendritic cells [2]. Experimental evidence shows that inducing inflammation through low-dose endotoxin injections has social cognitive effects [12], including heightened neural responses to pictures of close others in reward-related neural regions [13] and heightened neural responses to socially threatening pictures (fear faces) in threat-related neural regions like the amygdala [34]. Heightened amygdala reactivity to stressors may be related to heightened peripheral inflammation [35] and, in adult asthma patients, upregulated inflammatory signalling in the airway and increased airway inflammation [14]. Innate inflammatory response in the airway can then induce allergic inflammatory processes that lead to asthma exacerbations [36]. Furthermore, macrophages and dendritic cells are implicated in links between family conflict, exposure to chronic stressors, and a proinflammatory phenotype characterized by greater upregulation of genes regulated by the proinflammatory transcription factor nuclear factor-κB [23, 37] and lower sensitivity to anti-inflammatory glucocorticoids [9, 38].
Another possible interpretation is even though increased symptoms may occur because of high pollution exposure, a supportive home environment may alleviate the effects due to better adherence to medication and other treatment regimens. In cross-sectional data, greater family conflict or stress is related to lower adherence [39]; less is known about adult support and adolescent adherence in asthma. However, in this sample, greater perceived support was not related to reporting using daily prescription control medication.
The interpretations from this study should be considered in the context of limitations to inference and generalizability. This study focused on O3 rather than pollutants with high spatial variability like NOx and particulate matter, where exposure modeling of multiple variables (e.g., traffic volume, wind speed, elevation, air monitoring data) enables estimating pollutant levels at a specific geographic location (i.e., respondent address) [4, 17, 18, 26]. O3 has less spatial variation compared to NOx, particularly in rural areas [2]. While air monitoring stations are less ideal for documenting personal exposures, estimates of risk associated with O3 exposure are generally similar across types of exposure assessment and spatial concentration of air monitors [2]. The population effect size for O3 and asthma symptoms is small (OR = 1.02 in children [3]), requiring thousands of children for sufficient power to observe a main effect of O3. While air monitoring data provided reliable estimates of average O3 exposures, acute O3 elevations may be more health-relevant than long-term exposures [2]. Finally, CHIS did not include measures of family conflict or stress (except for poverty level). Given that greater chronic stress, such as poverty, shows modest associations with more negative parenting including less perceived adolescent support [40, though for more nuanced data see 41], a critical direction for future work is examining whether interactions between support and pollution exposure are independent of proposed exacerbating effects of stress exposures [5,6,7]. Similarly, given the potential role of affective reactivity in proposed airway inflammation → social-cognitive neural circuitry → peripheral inflammation pathway, future work should determine whether interactions between social factors and pollution exposure are independent of (or explained by) emotion-related mechanisms.
Regarding generalizability, because of requirements related to living within 5 mi of an air monitoring station, the subsample of adolescents with asthma in CHIS is small, underpowered for detecting small effects, and may not be representative of adolescents with asthma in California or other regions. In our sample, greater perceived support showed a small to modest association with higher O3 levels, which may be explained by two observations in the literature. First, O3 concentrations are higher in suburban and rural areas that are downwind of air pollution sources, which are also higher income relative to urban areas [2]. Second, higher family SES is related to greater parent involvement in academics [42] and greater perceived parent social support during adolescence [43].
The observed findings are consistent with models that integrate psychosocial and pollution exposures to explain poor outcomes in at-risk populations [4,5,6,7, 9]. Future prospective research should include larger samples; more sophisticated family assessments, including indicators of affective sensitivity to the family environment; immune measures in the lung compartment; and personal exposures to pollution. Regarding translational implications, future work could test whether existing family interventions in asthma [e.g., 44] may show greater benefit in children living in high air pollution regions. Ultimately, behavioral pathways that increase adherence [22] or reduce pollution exposure via staying indoors or increasing exposure to green space [45] likely play a role in the interplay among family environments and air pollution. Finally, in this study, associations between perceived support at home and asthma symptoms were observed with exposures greater than 48 ppb, which is below the federal standard of 70 ppb. If future replications obtain similar results, the proportion of children with asthma that has health-relevant sensitivity to the home psychosocial environment may be considerable.
Notes
The California Healthy Kids Survey was commissioned by the California Department of Education to assess student well-being in children age 10 and above (more information is available at https://calschls.org/about/the-surveys/).
According to the National Asthma Education and Prevention Program guidelines [29], intermittent asthma severity is defined in part as having daytime symptoms ≤ 2 days/week. Persistent asthma severity is defined as having daytime symptoms > 2 days/week. CHIS did not measure other components of severity (nighttime awakenings, use of short-term symptom control medications, daily interference, and lung function). The CHIS measure did not have fine-grained distinctions over a weekly timeframe but instead asked about a yearly timeframe (e.g., monthly, weekly). Thus, the 39.2% participants in the 5 mi sample (40.2%, 3 mi sample) who reported “weekly” and “daily” asthma could be considered as having persistent asthma according to published guidelines.
Abbreviations
- CARB:
-
California Air Resources Board
- CHIS:
-
California Health Interview Survey
- ER:
-
Emergency room
- mRNA:
-
Messenger ribonucleic acid
- NF-κB:
-
Nuclear factor-κB
- NO2 :
-
Nitrogen dioxide
- NOx :
-
Nitrogen dioxides
- O3 :
-
Ozone
- Ppb:
-
Parts per billion
References
Guarnieri M, Balmes JR. Outdoor air pollution and asthma. Lancet. 2014;383:1581–92. https://doi.org/10.1016/S0140-6736(14)60617-6.
U. S. Environmental Protection Agency. Integrated science assessment (ISA) of ozone and related photochemical oxidants. Washington, DC. 2020. https://www.epa.gov/isa/integrated-science-assessment-isa-ozone-and-related-photochemical-oxidants. Accessed 9 May 2022.
Orellano P, Quaranta N, Reynoso J, Balbi B, Vasquez J. Effect of outdoor air pollution on asthma exacerbations in children and adults: systematic review and multilevel meta-analysis. PLoS ONE. 2017;12: e0174050. https://doi.org/10.1371/journal.pone.0174050.
Chen E, Schreier HMC, Strunk RC, Brauer M. Chronic traffic-related air pollution and stress interact to predict biologic and clinical outcomes in asthma. Environ Health Perspect. 2008;116:970–5. https://doi.org/10.1289/ehp.11076.
Alvarez HAO, Kubzansky LD, Carnpen MJ, Slavich GM. Early life stress, air pollution, inflammation, and disease: an integrative review and immunologic model of social-environmental adversity and lifespan health. Neurosci and Biobehav Rev. 2018;92:226–42. https://doi.org/10.1016/j.neubiorev.2018.06.002.
Clougherty JE, Kubzansky LD. A framework for examining social stress and susceptibility to air pollution in respiratory health. Environ Health Perspect. 2009;117:1351–8. https://doi.org/10.1289/ehp.0900612.
Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am. 2011;31:19–39. https://doi.org/10.1016/j.iac.2010.09.011.
Busse W, Banks-Schlegel S, Noel P, Ortega H, Taggart V, Elias L. Future research directions in asthma - an NHLBI working group report. Am J Respir Crit Care Med. 2004;170:683–90. https://doi.org/10.1164/rccm.200311-1539WS.
Miller GE, Chen E, Parker KJ. Psychological stress in childhood and susceptibility to the chronic diseases of aging: moving toward a model of behavioral and biological mechanisms. Psychol Bull. 2011;137:959–97. https://doi.org/10.1037/a0024768.
Repetti RL, Robles TF, Reynolds B. Allostatic processes in the family. Dev Psychopathol. 2011;23:921–38. https://doi.org/10.1017/s095457941100040x.
Weitekamp CA, Hofmann HA. Effects of air pollution exposure on social behavior: a synthesis and call for research. Environ Health. 2021;20:72. https://doi.org/10.1186/s12940-021-00761-8.
Muscatell KA, Moieni M, Inagaki TK, et al. Exposure to an inflammatory challenge enhances neural sensitivity to negative and positive social feedback. Brain Behav Immun. 2016;57:21–9. https://doi.org/10.1016/j.bbi.2016.03.022.
Inagaki TK, Muscatell KA, Irwin MR, et al. The role of the ventral striatum in inflammatory-induced approach toward support figures. Brain Behav Immun. 2015;44:247–52. https://doi.org/10.1016/j.bbi.2014.10.006.
Rosenkranz MA, Esnault S, Gresham L, Davidson RJ, Christian BT, Jarjour NN, Busse WW. Role of amygdala in stress-induced upregulation of airway IL-1 signaling in asthma. Biol Psychol. 2022;167: 108226. https://doi.org/10.1016/j.biopsycho.2021.108226.
Rosenkranz MA, Esnault S, Christian BT, Crisafi G, Gresham LK, Higgins AT, Moore MN, Moore SM, Weng HY, Salk RH, Busse WW, Davidson RJ. Mind-body interactions in the regulation of airway inflammation in asthma: a PET study of acute and chronic stress. Brain Behav Immun. 2016;58:18–30. https://doi.org/10.1016/j.bbi.2016.03.024.
American Lung Association. State of the air 2021. Washington DC. 2021. https://www.lung.org/research/sota. Accessed 9 May 2022.
Islam T, Urman R, Gauderman WJ, et al. Parental stress increases the detrimental effect of traffic exposure on children’s lung function. Am J Respir Crit Care Med. 2011;184:822–7. https://doi.org/10.1164/rccm.201104-0720OC.
Bandoli G, von Ehrenstein O, Ghosh JK, Ritz B. Synergistic effects of air pollution and psychosocial stressors on adolescent lung function. J Allergy Clinical Immunol. 2016;138:918-20.e4. https://doi.org/10.1016/j.jaci.2016.04.012.
World Health Organization. WHO Global Urban Ambient Air Pollution Database (update 2016). 2016. Available from: http://www.who.int/phe/health_topics/outdoorair/databases/cities/en/. Accessed 9 May 2022.
Chen E, Brody GH, Miller GE. Childhood close family relationships and health. Am Psychol. 2017;72:555–66. https://doi.org/10.1037/amp0000067.
Hostinar CE, Sullivan RM, Gunnar MR. Psychobiological mechanisms underlying the social buffering of the hypothalamic–pituitary–adrenocortical axis: a review of animal models and human studies across development. Psychol Bull. 2014;140:256–82. https://doi.org/10.1037/a0032671.
Drotar D, Bonner MS. Influences on adherence to pediatric asthma treatment: a review of correlates and predictors. J Dev Behav Pediatr. 2009;30:574–82. https://doi.org/10.1097/DBP.0b013e3181c3c3bb.
Robles TF, Repetti RL, Reynolds BM, Chung PJ, Arevalo JMG, Cole SW. Family environments and the leukocyte transcriptome in children and parents. Dev Psychopathol. 2018;30:235–53. https://doi.org/10.1017/S0954579417000591.
California Health Interview Survey. CHIS 2003 methodology series: report 2 – data collection methods. Los Angeles, CA: UCLA Center for Health Policy Research. 2005. https://healthpolicy.ucla.edu/chis/design/Documents/CHIS2003_method2.pdf. Accessed 9 May 2022.
Wilhelm M, Meng YY, Rull RP, English P, Balmes J, Ritz B. Environmental public health tracking of childhood asthma using California Health Interview Survey, traffic, and outdoor air pollution data. Environ Health Perspect. 2008;116:1254–60. https://doi.org/10.1289/ehp.10945.
Jerrett M, Arain A, Kanaroglou P. A review and evaluation of intraurban air pollution exposure models. J Expo Anal Environ Epidemiol. 2005;15:185–204. https://doi.org/10.1038/sj.jea.7500388.
California Health Interview Survey. California health interview survey 2003 adolescent public use file, release 3. UCLA Center Health Policy Res. 2010. http://healthpolicy.ucla.edu/chis/data/Pages/GetCHISData.aspx.
Hanson TL, Kim JO. Measuring resilience and youth development: the psychometric properties of the Healthy Kids Survey. (Issues & Answers Report, REL 2007 – No. 034). Wasnighton, DC: U.S. Department of Education, Institute of Education Sciences, National Center for Education Evaluation and Regional Assistance, Regional Educational Laboratory West. 2007. https://ies.ed.gov/ncee/edlabs. Accessed 9 May 2022.
National Asthma Education and Prevention Program. Expert panel report 3: guidelines for the diagnosis and management of asthma. Bethesda, MD: National Heart, Lung, and Blood Institute (US). 2007. https://www.ncbi.nlm.nih.gov/books/NBK7232/. Accessed 9 May 2022.
UCLA Center for Health Policy Research. Constructed variables; CHIS 2003 Adolescent Survey. Los Angeles, CA: UCLA Center for Health Policy Research. https://healthpolicy.ucla.edu/chis/data/public-use-data-file/Documents/2003PUF_constructs_t.pdf. Accessed 9 May 2022.
Meng YY, Wilhelm M, Ritz B, Balmes J, Lombardi C, Bueno A, Pickett M. Is disparity in asthma among Californians due to higher pollution exposures, greater vulnerability, or both? Report prepared for the California Air Resources Board and the California Environmental Protection Agency. 2012. https://ww2.arb.ca.gov/sites/default/files/classic/research/apr/past/07-309.pdf. Accessed 9 May 2022.
Preacher KJ, Curran PJ, Bauer DJ. Computational tools for probing interactions in multiple linear regression, multilevel modeling, and latent curve analysis. J Educ Behav Stat. 2006;31:437–48. https://doi.org/10.3102/10769986031004437.
Wright K. Examining racial and ethnic disparities and predictors of medication use among California’s African-American, Latino, and White children with asthma. J Natl Black Nurses Assoc. 2007;18(2):1–15.
Inagaki TK, Muscatell KA, Irwin MR, Cole SW, Eisenberger NI. Inflammation selectively enhances amygdala activity to socially threatening images. Neuroimage. 2012;59(4):3222–6. https://doi.org/10.1016/j.neuroimage.2011.10.090.
Leschak CJ, Dutcher JM, Haltom KEB, Breen EC, Bower JE, Eisenberger NI. Associations between amygdala reactivity to social threat, perceived stress and C-reactive protein in breast cancer survivors. Soc Cogn Affect Neurosci. 2020;15(10):1056–63. https://doi.org/10.1093/scan/nsz103.
Hammad H, Lambrecht BN. Dendritic cells and airway epithelial cells at the interface between innate and adaptive immune responses. Allergy. 2011;66:579–87. https://doi.org/10.1111/j.1398-9995.2010.02528.x.
Chen E, Miller GE, Walker HA, Arevalo JM, Sung CY, Cole SW. Genome-wide transcriptional profiling linked to social class in asthma. Thorax. 2009;64:38–43. https://doi.org/10.1136/thx.2007.095091.
Murphy MLM, Slavich GM, Chen E, Miller GE. Targeted rejection predicts decreased anti-inflammatory gene expression and increased symptom severity in youth with asthma. Psychol Sci. 2015;26:111–21. https://doi.org/10.1177/2167702612455743.
Kaugars AS, Klinnert MD, Bender BG. Family influences on pediatric asthma. J Pediatr Psychol. 2004;29:475–91. https://doi.org/10.1093/jpepsy/jsh051.
Grant KE, Compas BE, Thurm AE, et al. Stressors and child and adolescent psychopathology: evidence of moderating and mediating effects. Clin Psychol Rev. 2006;26(3):257–83. https://doi.org/10.1016/j.cpr.2005.06.011.
Luthar SS, Latendresse SJ. Comparable “risks” at the socioeconomic status extremes: preadolescents’ perceptions of parenting. Dev Psychopathol. 2005;17(1):207–30. https://doi.org/10.1017/s095457940505011x.
Hill NE, Castellino DR, Lansford JE, et al. Parent academic involvement as related to school behavior, achievement, and aspirations: demographic variations across adolescence. Child Dev. 2004;75:1491–509. https://doi.org/10.1111/j.1467-8624.2004.00753.x.
Wang MT, Eccles JS. Social support matters: longitudinal effects of social support on three dimensions of school engagement from middle to high school. Child Dev. 2012;83:877–95. https://doi.org/10.1111/j.1467-8624.2012.01745.x.
Naar-King S, Ellis D, King PS, et al. Multisystemic therapy for high-risk African American adolescents with asthma: a randomized clinical trial. J Consult Clin Psychol. 2014;82:536–45. https://doi.org/10.1037/a0036092.
Chen E, Miller GE, Shalowitz MU, et al. Difficult family relationships, residential greenspace, and childhood asthma. Pediatrics. 2017;139. https://doi.org/10.1542/peds.2016-3056.
Acknowledgements
The authors wish to thank Beate Ritz and John Balmes for their comments on earlier versions of the manuscript.
Funding
This research project was supported by Contract No. 07–309 “Is Disparity in Asthma among Californians due to Higher Pollution Exposures, Greater Vulnerability, or Both?” to the UCLA Center for Health Policy Research under the sponsorship of the California Air Resources Board, UCLA Academic Senate, and NIH grant R03HD077387.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
These data were presented at the 2019 biennial meeting of the Society for Research in Child Development, Baltimore, MD.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Robles, T.F., Bai, S. & Meng, YY. Ozone Pollution, Perceived Support at Home, and Asthma Symptom Severity in the Adolescent Sample of the California Health Interview Survey. Int.J. Behav. Med. 30, 398–408 (2023). https://doi.org/10.1007/s12529-022-10103-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-022-10103-8