
Abstract
Background
This pilot study explored the feasibility, acceptability, and usability of a web-based intervention for survivors of physical inactivity-related cancers through a two-arm, 12-week randomized controlled trial. Secondarily, this study tested the change in physical activity (PA) and sedentary time with intervention exposure.
Methods
Prior to randomization to the intervention (n = 45) or behavior “as usual” wait-listed control (n = 40) groups, participants completed baseline surveys and an accelerometer protocol. The intervention focused on increasing PA and decreasing sedentary time through social cognitive theory techniques. Follow-up acceptability/usability surveys (intervention group only) and accelerometers were sent after the intervention period. Information on intervention completion, adverse events, and user statistics were collected to determine feasibility. Median login time and mean acceptability/usability scores were calculated.
Results
Participants (mean age = 60 ± 7 years) included female (n = 80, 94%) and male survivors of breast (82%), colon (6%), endometrial (6%), bladder (4%), and kidney (2%) cancer. Seventy-eight (91.7%) participants returned partially or fully complete post-intervention data. There were no reported injuries or safety concerns. Intervention participants logged into the website for a total of 95 min (Q1, Q3 = 11, 204). System usability scores (72 ± 3) indicated above average usability of the website. Changes in time spent active and sedentary were not statistically significantly different between groups (p = 0.45), but within-group changes suggested intervention group participants spent more time active and less time sedentary after the intervention.
Conclusion
Results of this pilot study suggest its feasibility and acceptability for survivors of several inactivity-related cancers. Additional research to determine long-term efficacy is warranted. This low-cost online-only intervention has the potential to have a very broad reach.
Trial Registration
Clinical Trials Number: NCT03983083. Date registered: June 12th, 2019
Similar content being viewed by others


Introduction
There are approximately 16.9 million cancer survivors in the USA, and this population is expected to grow with improved cancer survival rates [1]. Cancer survivors experience a myriad of long-term side effects following treatment, including fatigue, decreased muscle mass, balance issues, decreased cognitive function, and an increased risk of comorbidities. Observational studies and randomized controlled trials demonstrate that physical activity (PA) is a safe and effective non-pharmacological strategy for improving some of these side effects [2,3,4,5,6,7]. Despite this evidence, it is estimated (using self-reported data) that around 70% of cancer survivors do not meet PA guidelines and, although there are no established sedentary time guidelines, it is likely that many cancer survivors also spend too much time sedentary [8, 9]. Therefore, it is imperative to develop evidence-based, broad-reaching PA interventions tailored specifically for cancer survivors.
Many existing PA interventions for cancer survivors require in-person training sessions supervised by exercise professionals [5, 10, 11]. While many of these interventions have reported statistically and clinically significant changes in PA, in-person sessions are resource-intensive and may not be sustainable or cost-effective. Further, there exists little evidence that in-person behavior change interventions are more effective for increasing PA compared to broad-reach (i.e., not face-to-face) interventions [10]. One review of 14 PA interventions for breast cancer survivors included highly structured, supervised interventions, and phone- and e-mail-based interventions and found that studies with the most intense supervision did not necessarily produce the largest increase in PA [10]. Although patients undergoing treatment may require face-to-face instruction to assure safety, results from a review of PA interventions for a wider range of cancer survivors suggested that broad-reach interventions are safe and appropriate for survivors who have recently completed treatment [12]. The broad-reach mode of intervention delivery, specifically internet delivery, has the potential to reach a larger population of cancer survivors; therefore, the impact of an internet-based intervention can be quite meaningful at the population level, even if individual increases in PA are somewhat small [13]. Finally, most PA interventions target a single survivor group, largely breast cancer, leading to a number of largely unanswered calls for more research engaging more diverse groups of survivors [12, 14, 15].
Despite recent discoveries about the deleterious effects of excess sedentary behavior for people of varying activity levels [16, 17], most PA interventions for cancer survivors focus solely on the promotion of moderate-to-vigorous intensity aerobic physical activity (MVPA). As far as publicly available activity guidance, one study reviewed almost 400 websites with PA information for cancer survivors and found that < 10% of the websites included information on sedentary behavior [18]. Ignoring the importance of decreased sedentary time has consequences, as PA programs without a sedentary behavior component often do not decrease sedentary time, even if MVPA increases [13]. This highlights the need for interventions that additionally promote the reduction of sedentary time through increased light intensity physical activity (LPA), as only a very small handful of such interventions tailored for the specific needs of cancer survivors exist [19].
The Health and Energy through Active Living Every Day (HEALED) pilot study is a 12-week, web-based PA and sedentary time randomized controlled intervention based on the social cognitive theory. HEALED materials were designed for survivors of cancers with a 5-year survival of at least 65% (at Stages I and II) and for which the level of evidence for association with physical inactivity is strong according to the 2018 Physical Activity Guidelines Advisory Committee Report; this includes breast, colon, endometrium, kidney, and bladder cancer [13]. The purpose of this pilot study was to determine the feasibility, acceptability, and usability of the web-based HEALED intervention, and secondarily, to test the change in time spent physically active (light intensity PA, MVPA, and strength training) and sedentary.
Methods
Study Participant Recruitment and Eligibility
Participants were recruited through the Cancer Prevention Study-3 (CPS-3). CPS-3 is a prospective cohort study of cancer incidence and mortality initiated by the American Cancer Society (ACS). Over 254,000 CPS-3 participants aged 30 to 65 years with no history of cancer (except for basal or squamous cell skin cancer) completed a baseline survey at enrollment and are sent triennial surveys to update exposure information [20]. All CPS-3 participants will be followed up for cancer incidence and mortality from any cause for at least the next 20 years. All aspects of CPS-3 have been approved by the Emory University Institutional Review Board.
Eligibility for HEALED was determined based on data from the two most recent CPS-3 surveys (2015, 2018). In addition to having responded to the 2015 and/or 2018 English version of the survey(s), participants were invited by email if they (1) had a confirmed Stage I or II breast, colon, endometrium, kidney, or bladder cancer diagnosis (verified through medical record abstraction or linkage with state cancer registries); (2) had an e-mail address on record; (3) reported less than 150 min MVPA/week and/or less than 2 days/week of strength training; and (4) reported the ability to walk unassisted. A total of 431 eligible CPS-3 participants were invited by email to register for HEALED.
Interested participants completed a short screening questionnaire and provided informed consent online. The screening questionnaire included a physical activity readiness questionnaire (PAR-Q) and items regarding current cancer treatment and recurrence. Participants responding “yes” to one or more of any of the following items were contacted regarding their response and were excluded from the HEALED intervention if unsupervised PA was deemed to be unsafe: (1) has your doctor ever said that you have a heart condition and that you should only perform physical activity recommended by a doctor? (2) do you lose your balance because of dizziness or do you ever lose consciousness? (3) do you have a bone or joint problem that could be made worse by a change in your physical activity? (4) do you know of any other reason why you should not engage in physical activity? or (5) are you currently undergoing active cancer treatment (e.g., chemotherapy, radiation therapy)?
Study Design
The HEALED study had a two-arm design, including an intervention group and a wait-listed control group that was instructed to continue behavior “as-usual” during the 12-week intervention period.
Once an eligible participant completed the screening questionnaire and provided online informed consent, they were mailed an accelerometer with instructions for wear, a four-page baseline survey, and return shipping materials. The baseline survey included questions on current weight, history of cancer treatment, and self-reported time spent on strength training per week. Participants were randomized to the intervention or control group by an independent researcher using a random number generator after completed baseline materials were returned.
Immediately after the 12-week intervention period, participants were re-sent the accelerometer and a follow-up survey. Upon receipt of the follow-up survey and accelerometer, wait-listed control group participants were given access to the full 12-week intervention.
Measures
Feasibility
User statistics, including number of HEALED website logins, time logged in per session, and total time logged in, were collected to determine feasibility among intervention group participants. Data on adverse events (including reported injuries or safety issues) were collected, and completion rates (percent returning fully complete, partially complete, or incomplete post-intervention materials) were calculated.
Acceptability
The follow-up survey included an acceptability scale, where participants indicated their level of agreement (five response options ranging from strongly agree to strongly disagree) with five statements such as “information shared through HEALED motivated me to be more active” and “being a HEALED participant is enjoyable.” This survey also included a space for write-in comments.
Usability
The follow-up survey also included the System Usability Scale. The System Usability Scale is a commonly used, 10-item survey (five response options ranging from strongly agree to strongly disagree) for quantifying perceived usability of software, mobile applications, and websites [21]. The total score from the scale was calculated according to the scoring manual; scores below 68 indicate below average usability and scores ≥68 indicate above average usability [21].
LPA, MVPA, and Sedentary Time
Participants were instructed to wear an Actigraph GT3x+ accelerometer (Pensacola, FL) on the hip aligning with the midline of the non-dominant thigh for seven consecutive days during all waking hours at baseline (before exposure to the HEALED intervention website) and at follow-up (immediately after the 12-week intervention period), except when bathing or participating in water-based activities (e.g., swimming) [22]. Actigraph data were processed using two hybrid machine learning approaches: first, the Choi algorithm was used to calculate accelerometer wear time, then the Sojourn-3 axis algorithm was used to estimate daily sedentary and active time by intensity [23,24,25]. The change in the proportion of wear time spent sedentary, in LPA, and MVPA was assessed. Sufficient accelerometer wear was defined as having ≥ 4 days of data and a minimum of 14 h/day; a longer wear time minimum was used as sedentary time was a primary outcome [26].
Strength Training
As time spent strength training cannot be captured with accelerometry, both baseline and follow-up surveys included a validated questionnaire asking participants, “During the past year, estimate the hours per day you spent on typical weekdays and weekends in each of the following activities. Please average your seasonal physical activities over the entire year.” Account for all 24 h per day and items “weight training” and “other resistance exercises” were used to capture total strength training [27]. Item responses were “0, < 1, 1–2, 3–4, 5–6, 7–8, 9–10, 11+ hours per day,” and the mean number of hours within the response categories (i.e., 0, 0.5, 1.5, 3.5, 5.5 hours per day) were summed to obtain daily average time spent strength training. Baseline to follow-up change in self-reported strength training time was collapsed into three categories: decreased time, no change in time, and increased time spent strength training.
Intervention
Theoretical Framework
Theory-based interventions are often more effective in increasing and maintaining physical activity among cancer survivors than interventions not guided by theory [28]. Accordingly, we used the social cognitive theory (SCT) as the theoretical framework for developing HEALED [29]. The SCT suggests that there are reciprocal interactions among the personal, social, and environmental influences that shape behavior, and it has been shown to be associated with increased exercise behavior among cancer survivors specifically [30, 31].
Website
The HEALED website required a password and username to log-in and allowed participants to set up a user profile using a unique study identifier (no names were used). HEALED intervention group participants received monthly motivational e-mails (as prior studies suggest that monthly is the most effective delivery time interval for interventions involving cancer survivors [32]) announcing one new website feature (e.g., a new exercise video, a new goal-setting tool) to prompt return to the website. All emails included links to the web-based platform, which provided a range of support tools that align with behavior change techniques of the SCT, including (1) increase PA self-efficacy: at-home/equipment-free aerobic and strength training exercise demonstrations and videos (that include modifications for those with lymphedema), aerobic PA and strength training recommendations for survivors (ACSM guidelines) [7], positive messaging around exercising and sitting less during bouts of sadness and/or low energy, and guidance on how to safely return to activity after an abdominal or breast surgery; (2) align PA and sedentary time outcome expectations: aerobic PA, strength training, and sitting time educational information (evidence-based resources on the benefits of PA and detrimental effects of excess sitting specific to survivors), a space for goal setting (including examples of specific, measurable, attainable, relevant, and time-based [SMART] goals); and (3) facilitate social support: videos of other cancer survivors’ personal stories of post-diagnosis behavior change, and a discussion board [33]. Many of these materials were downloadable and/or printable, so participants could participate in certain activities offline if they preferred.
Analysis
Descriptive statistics, including percentages for categorical variables and means and standard deviations for continuous variables, were calculated. Comparisons of baseline variables between the intervention and control groups to assess for imbalance used the Wilcoxon rank sum test for continuous variables or the Fisher exact test for categorical variables. Mean scores of each item on the acceptability and usability surveys were also calculated. The number of logins and time logged in was highly skewed; thus, median values were calculated.
Although the primary aims of the current study were to determine feasibility, acceptability, and usability, secondary outcomes of the pilot were explored using group by time interactions in an analysis of covariance for PA and sedentary time. Complete case comparisons were made using F tests. Models adjusted for (1) accelerometer wear time (continuous) and (2) accelerometer wear time, age (continuous), sex, cancer type, and time since diagnosis (continuous). SAS v.9.4 (Cary, North Carolina) was used for all analyses.
Results
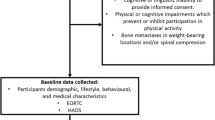
Of the 99 cancer survivors who registered for the intervention, 96 were eligible for participation and were sent an accelerometer and baseline survey (Fig. 1). Eighty-five participants (88.5%) returned complete baseline accelerometer and survey data and were randomized to the intervention (n = 45) or wait-listed control (n = 40) groups. Baseline characteristics did not differ significantly between those randomly assigned to the intervention and control groups (Table 1). Participants were female (94.1%) and male (5.9%) survivors of breast (82.4%), colon (5.9%), endometrial (5.9%), bladder (3.5%), and kidney (2.4%) cancer. Participants’ mean age was 60 years (SD = 7.4), and they were diagnosed 7 years (SD = 1.9) prior to baseline. The majority of participants were overweight or obese (64.7%). According to baseline accelerometry data, participants spent an average of 19 min/day in MVPA and almost 14 h/day sedentary.

Flow of participants
Feasibility
Forty-one (91.1%) intervention group participants and 37 (92.5%) wait-listed control participants returned partial (n = 11, 14.1%) or full (n = 67, 85.9%) post-intervention data. There were no reported injuries or safety concerns during the intervention.
Most intervention group participants (n = 34, 82.9%) logged into the HEALED website at least once during the 12-week intervention. Intervention participants logged into the website four times (median; quartile 1, quartile 3 [Q1, Q3] = 1, 8 times) during the intervention period, and spent 16 min (Q1, Q3 = 6, 21 min) on the website each session (Table 2). Total time logged in throughout the 12-week intervention was 95 min (Q1, Q3 = 11, 204 min).
Acceptability
Among the intervention group participants who logged in at least once and completed the acceptability surveys (n = 32), mean ratings of motivation were 3.77 and enjoyment of the HEALED website were 3.62 (possible scores 1–5; Table 2). Participants did not feel that the exercises promoted throughout the HEALED website were too difficult (1.60). The level of agreement with the statement, “I would like to use this website frequently” varied widely (mean = 2.65, range = 1.0, 5.0).
Usability
Total scores from the System Usability Scale averaged 72 (range = 67, 78), indicating above average usability of the HEALED website (Table 2).
Change in PA and Sedentary Time
Participants wore the accelerometer (N = 81 with complete accelerometry data) for a mean time of 928 min per day at baseline and 917 min per day at follow-up for an average of 6.9 days at both time points (combined baseline and follow-up daily wear time mean = 922 min per day). Baseline to follow-up changes in the proportion of wear time spent sedentary, in LPA, and in MVPA were not statistically significantly different between the intervention and control group (p = 0.45 model 1; p = 0.49 model 2); however, intervention group participants spent more time in LPA (+ 9 min/day on average) and MVPA (+ 4 min/day) and less time sedentary (− 13 min/day) at follow-up compared to baseline. Control group participants spent, at follow-up, less time in LPA (− 36 min/day on average), the same amount of time in MVPA, and more time sedentary (+ 36 min/day; Fig. 2) compared to baseline.

Baseline and follow-up proportion of daily wear time (mean: 922 min/day) spent sedentary, in light intensity physical activity (LPA), and in moderate-to-vigorous intensity physical activity (MVPA) as measured by accelerometry. a Intervention group baseline. b Intervention group follow-up. c Control group baseline. d Control group follow-up
Changes in self-reported strength training (N = 64 with complete pre- and post-intervention strength training data) were not statistically significant between groups (p = 0.11), but a larger proportion of intervention group participants increased their strength training (n = 7, 22.6%) compared to control group participants (n = 3, 9.1%; Table 3).
Discussion
This pilot study examined the feasibility, acceptability, and usability of a web-based PA intervention tailored for survivors of cancers associated with physical inactivity. Overall, participants reported feeling motivated by the content delivered through the HEALED website and found the website easy to use. As telemedicine, video calls, and other at-home options are increasingly prevalent (and potentially safer in the time of a global pandemic), a digital strategy for the promotion of active living is even more important and timely. This study adds to the minimal evidence base for low-cost, web-based PA interventions for a broader range of cancer survivors.
Results of the current study support an expansion of the HEALED study in a fully powered randomized controlled trial, and this study provided a lot of information that will help to improve future iterations. For example, the average score for the acceptability item, “the exercises in the HEALED intervention were too difficult” was lower than anticipated (mean = 1.60, with scores ranging from 1.0 to 3.0); plans to improve and expand the pilot would include a larger offering of exercise videos to challenge a wider range of ages and abilities. Additionally, we found that a web-based intervention was not necessarily suitable for all participants; several intervention group participants never logged into the HEALED website (n = 7, 17.1%) and cited reasons for non-use including misplacing their password and lack of internet access. Accordingly, it will be important to add participant prompts for those who have not logged in and allow them quick access to personal password recovery in the expanded version of this intervention. Engagement may also be boosted by further facilitating social support, as only 15% of participants posted on the discussion board, and by incorporating self-monitoring via wearable commercial devices that are compatible with the website.
Though this pilot study was not powered to detect changes in physical activity and sedentary time, there were trends indicating increases in LPA, MVPA, and strength training, and a decrease in sedentary time among the intervention group participants; importantly, time spent active and sedentary was accelerometer-measured. One review of ten web-based PA interventions for survivors (including five studies that were also based on the SCT) found that all studies reported improvements in PA of a similar magnitude as the current study (eight studies reported statistically significant improvements); however, nine of these studies used self-reported measures of PA and one used a commercial device [34]. An online pilot study not included in the review of 84 breast, prostate, and colon cancer survivors of a similar age and time since diagnosis as the current study reported an increase of 42 min/day of PA (statistically non-significant), though this was measured via self-report [35]. Since that review, another pilot of a 12-week web-based sedentary time intervention for 46 prostate cancer survivors reported an average decrease in accelerometer-measured sedentary time of 65 min/day and an average increase in accelerometer-measured MVPA of 6 min/day, though this study used a pre-post design and therefore did not compare these results to a control group [36]. A newer review of online PA interventions tailored specifically for breast cancer survivors included 16 studies, 8 of which were RCTs; the one included RCT that used device-based measures of PA reported a modest, but statistically significant, increase in MVPA associated with intervention exposure [37].
Strengths
This study was strengthened by the randomized controlled design and the use of accelerometer-measured PA and sedentary time. This study also included both male and female (albeit a limited number of male) survivors of several cancer types; this is an important distinction as many existing interventions were designed and evaluated only for female breast cancer survivors. Finally, the HEALED intervention is entirely web-based, making this a no-contact intervention that can be disseminated at a fairly low cost.
Limitations
This study is not without limitations. Importantly, several of the intervention group participants had no actual intervention dose, as they were unable or unwilling to log into the HEALED website. We were also unable to track participant engagement beyond login frequency and time (e.g., which website tools received the most “clicks,” how many participants read discussion board posts) on the platform used to develop the HEALED website. Similarly, several HEALED materials were downloadable or printable, so while it is possible that participants were still engaging when they were not logged in, we were unable to track offline engagement. Additionally, this study may be limited by the relatively short intervention period. While 12 weeks may be sufficient for a pilot study, we are unable to determine if this intervention may be associated with long-term changes or maintenance in PA or sedentary time. Finally, the results of this study (in particular, participation and completion rates) may not be generalizable as the participants in the current study were recruited from CPS-3, an ongoing longitudinal cohort study, and are therefore already committed study participants.
Overall, results of this pilot randomized controlled trial suggest that the web-based HEALED intervention is feasible and acceptable for male and female survivors of several cancers associated with physical inactivity, including breast, colon, endometrium, kidney, and bladder. The potential reach of this intervention is very broad given that it is low-cost and entirely web based. Further research is needed to determine long-term efficacy of the HEALED intervention in a larger group of cancer survivors and would benefit from the inclusion of survivors with metastatic disease, undergoing treatment, and/or in poorer general health.
Data Availability
The authors confirm that some access restrictions apply to the data underlying the findings. Data are from the Cancer Prevention Study-3 and are available from the American Cancer Society by following the ACS Data Access Procedures (https://www.cancer.org/content/dam/cancer-org/research/epidemiology/cancerprevention-study-data-access-policies.pdf) for researchers who meet the criteria for access to confidential data.
Code Availability
The authors confirm that some access restrictions apply to the SAS code underlying the findings. Code is available by following the ACS Data Access Procedures. (https://www.cancer.org/content/dam/cancer-org/research/epidemiology/cancerprevention-study-data-access-policies.pdf) for researchers who meet the criteria.
Change history
13 February 2023
A Correction to this paper has been published: https://doi.org/10.1007/s12529-023-10158-1
References
American Cancer Society. Cancer treatment & survivorship facts & figures 2019–2021. Atlanta: American Cancer Society; 2019.
Ballard-Barbash R, Friedenreich CM, Courneya KS, Siddiqi SM, McTiernan A, Alfano CM. Physical activity, biomarkers, and disease outcomes in cancer survivors: a systematic review. J Natl Cancer Inst. 2012;104(11):815–40.
Schmid D, Leitzmann MF. Association between physical activity and mortality among breast cancer and colorectal cancer survivors: a systematic review and meta-analysis. Ann Oncol. 2014;25(7):1293–311.
Cormie P, Zopf EM, Zhang X, Schmitz KH. The impact of exercise on cancer mortality, recurrence, and treatment-related adverse effects. Epidemiol Rev. 2017;39(1):71–92.
Fong DY, Ho JW, Hui BP, Lee AM, Macfarlane DJ, Leung SS, et al. Physical activity for cancer survivors: meta-analysis of randomised controlled trials. BMJ. 2012;344:e70.
Mishra SI, Scherer RW, Geigle PM, Berlanstein DR, Topaloglu O, Gotay CC, et al. Exercise interventions on health-related quality of life for cancer survivors. Cochrane Database Syst Rev. 2012;8:Cd007566.
Campbell KL, Winters-Stone KM, Wiskemann J, May AM, Schwartz AL, Courneya KS, et al. Exercise guidelines for cancer survivors: consensus statement from international multidisciplinary roundtable. Med Sci Sport Exerc. 2019;51(11):2375–90.
Centers for Disease Control and Prevention, National Center for Health Statistics. National Health Interview Survey, 1997–2016.
Arem H, Mama SK, Duan X, Rowland JH, Bellizzi KM, Ehlers DK. Prevalence of healthy behaviors among cancer survivors in the United States: how far have we come? Cancer Epid Bio Prev. 2020;29(6):1179–87.
Bluethmann SM, Vernon SW, Gabriel KP, Murphy CC, Bartholomew LK. Taking the next step: a systematic review and meta-analysis of physical activity and behavior change interventions in recent post-treatment breast cancer survivors. Breast Cancer Res Treat. 2015;149(2):331–42.
Turner RR, Steed L, Quirk H, Greasley RU, Saxton JM, Taylor SJ, et al. Interventions for promoting habitual exercise in people living with and beyond cancer. Cochrane Database Syst Rev. 2018;9:Cd010192.
Goode AD, Lawler SP, Brakenridge CL, Reeves MM, Eakin EG. Telephone, print, and web-based interventions for physical activity, diet, and weight control among cancer survivors: a systematic review. J Can Surviv. 2015;9(4):660–82.
The 2018 Physical activity guidelines advisory committee scientific report. Part F: Health and Human Services; 2018. Chapter 4 and 11.
Speck RM, Courneya KS, Masse LC, Duval S, Schmitz KH. An update of controlled physical activity trials in cancer survivors: a systematic review and meta-analysis. J Can Surviv. 2010;4(2):87–100.
Alfano CM, Bluethmann SM, Tesauro G, Perna F, Agurs-Collins T, Elena JW, et al. Nci Funding trends and priorities in physical activity and energy balance research among cancer survivors. J Natl Cancer Inst. 2016;108(1).
Ekelund U, Brown WJ, Steene-Johannessen J, Fagerland MW, Owen N, Powell KE, et al. Do the associations of sedentary behaviour with cardiovascular disease mortality and cancer mortality differ by physical activity level? A systematic review and harmonised meta-analysis of data from 850 060 participants. Br J Sport Med. 2019;53(14):886–94.
Ekelund U, Steene-Johannessen J, Brown WJ, Fagerland MW, Owen N, Powell KE, et al. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. The Lancet. 2016;388(10051):1302–10.
Goodwin BC, Crawford-Williams F, Castro O, Rowe A, De Cocker K. Online physical activity and sedentary behaviour information for cancer survivors. J Can Surviv. 2020;14(5):677–88. Epub 2020/04/18. https://doi.org/10.1007/s11764-020-00881-z.
Lynch BM, Nguyen NH, Moore MM, Reeves MM, Rosenberg DE, Boyle T, et al. A randomized controlled trial of a wearable technology-based intervention for increasing moderate to vigorous physical activity and reducing sedentary behavior in breast cancer survivors: The ACTIVATE Trial. Cancer. 2019;125(16):2846–55. Epub 2019/04/24. https://doi.org/10.1002/cncr.32143.
Patel AV, Jacobs EJ, Dudas DM, Briggs PJ, Lichtman CJ, Bain EB, et al. The American Cancer Society’s Cancer Prevention Study 3 (CPS-3): recruitment, study design, and baseline characteristics. Cancer. 2017;123(11):2014–24.
System Usability Scale [Available from: https://www.usability.gov/how-to-and-tools/methods/system-usability-scale.html.
Keadle SK, Shiroma EJ, Freedson PS, Lee I-M. Impact of accelerometer data processing decisions on the sample size, wear time and physical activity level of a large cohort study. BMC Public Health. 2014;14(1):1210.
Choi L, Liu Z, Matthews CE, Buchowski MS. Validation of accelerometer wear and nonwear time classification algorithm. Med Sci Sport Exerc. 2011;43(2):357–64.
Choi L, Ward SC, Schnelle JF, Buchowski MS. Assessment of wear/nonwear time classification algorithms for triaxial accelerometer. Med Sci Sport Exerc. 2012;44(10):2009–16.
Lyden K, Keadle SK, Staudenmayer J, Freedson PS. A method to estimate free-living active and sedentary behavior from an accelerometer. Med Sci Sport Exerc. 2014;46(2):386–97. Epub 2013/07/19. https://doi.org/10.1249/MSS.0b013e3182a42a2d.
McGrath R, Vella CA, Scruggs PW, Peterson MD, Williams CJ, Paul DR. The impact of low accelerometer wear time on the estimates and application of sedentary behavior and physical activity data in adults. J Phys Act Health. 2017;14(12):919–24.
Subbiah K, Rees-Punia E, Patel AV. Reliability and validity of self-reported muscle-strengthening exercise in the Cancer Prevention Study-3. Med Sci Sport Exerc; 2020. Accepted October (In Press).
Bluethmann SM, Bartholomew LK, Murphy CC, Vernon SW. Use of theory in behavior change interventions: an analysis of programs to increase physical activity in posttreatment breast cancer survivors. Health Educ Behav. 2017;44(2):245–53.
Bandura A. Social foundations of thought and action: a social cognitive theory. Upper Saddle River, NJ: Prentice Hall; 1986.
Hatchett A, Hallam JS, Ford MA. Evaluation of a social cognitive theory-based email intervention designed to influence the physical activity of survivors of breast cancer. Psychooncology. 2013;22(4):829–36.
Stacey FG, James EL, Chapman K, Courneya KS, Lubans DR. A systematic review and meta-analysis of social cognitive theory-based physical activity and/or nutrition behavior change interventions for cancer survivors. J Can Surviv. 2015;9(2):305–38.
Short CE, Rebar A, James EL, Duncan MJ, Courneya KS, Plotnikoff RC, et al. How do different delivery schedules of tailored web-based physical activity advice for breast cancer survivors influence intervention use and efficacy? J Can Surviv. 2017;11(1):80–91.
Robertson MC, Tsai E, Lyons EJ, Srinivasan S, Swartz MC, Baum ML, et al. Mobile health physical activity intervention preferences in cancer survivors: a qualitative study. JMIR Mhealth Uhealth. 2017;5(1):e3.
Haberlin C, O’Dwyer T, Mockler D, Moran J, O’Donnell DM, Broderick J. The use of ehealth to promote physical activity in cancer survivors: a systematic review. Supp Care Can. 2018;26(10):3323–36.
Forbes CC, Blanchard CM, Mummery WK, Courneya KS. Feasibility and preliminary efficacy of an online intervention to increase physical activity in Nova Scotian cancer survivors: a randomized controlled trial. JMIR Cancer. 2015;1(2):e12.
Trinh L, Arbour-Nicitopoulos KP, Sabiston CM, Berry SR, Loblaw A, Alibhai SMH, et al. Risetx: testing the feasibility of a web application for reducing sedentary behavior among prostate cancer survivors receiving androgen deprivation therapy. Int J Behav Nutr Phys Act. 2018;15(1):49.
Dorri S, Asadi F, Olfatbakhsh A, Kazemi A. A systematic review of electronic health (Ehealth) interventions to improve physical activity in patients with breast cancer. Breast Cancer. 2020;27(1):25–46.
Acknowledgements
The authors express sincere appreciation to all Cancer Prevention Study-3 participants and to each member of the study and biospecimen management group. We also acknowledge the contribution to this study from central cancer registries supported through the Centers for Disease Control and Prevention's National Program of Cancer Registries and cancer registries supported by the National Cancer Institute's Surveillance, Epidemiology, and End Results Program. The views expressed here are those of the authors and do not necessarily represent the American Cancer Society or the American Cancer Society–Cancer Action Network.
Funding
The American Cancer Society funds the creation, maintenance, and updating of the Cancer Prevention Study-3.
Author information
Authors and Affiliations
Contributions
ER-P: conceptualization, data collection, formal analysis, methodology, writing—original draft, writing—review and editing. CRL: conceptualization, writing—review and editing. JLW: methodology, writing—review and editing. LFD: data collection, writing—review and editing. AMR: data collection, writing—review and editing. JRN: methodology, writing—review and editing. AVP: conceptualization, methodology, writing—review and editing.
Corresponding author
Ethics declarations
Ethics Approval
Emory University Institutional Review Board approves all aspects of the CPS-3, including the HEALED study.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
The authors affirm that research participants provided informed consent for publication.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Rees-Punia, E., Leach, C.R., Westmaas, J.L. et al. Pilot Randomized Controlled Trial of Feasibility, Acceptability, and Preliminary Efficacy of a Web-Based Physical Activity and Sedentary Time Intervention for Survivors of Physical Inactivity-Related Cancers. Int.J. Behav. Med. 29, 220–229 (2022). https://doi.org/10.1007/s12529-021-09999-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-021-09999-5