
Abstract
Background
The prognosis of tetralogy of Fallot with absent pulmonary valve (TOF/APV) without operation is poor. We evaluated the surgical outcome of TOF/APV in a single center.
Methods
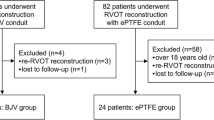
Twenty-two TOF/APV patients underwent complete surgical correction in our hospital. Right ventricular outflow tract reconstruction was performed using bovine jugular vein (BJV)-valved conduit implantation (n = 10), homograft-valved conduit implantation (n = 2), or monocusp-valve patch (n = 10). Health-related quality of life (QOL) was evaluated during follow-up.
Results
The overall survival at 5 and 10 years was 86.4 ± 7.3% (confidence interval 69.4–97.2%). The survival rates were significantly different between patients with and without bronchial stenosis (40 and 100%, P = 0.0003, log-rank test). The survival of patients aged > 6 months was higher than those ≤ 6 months (100 vs. 40%, P = 0.0003, log-rank test). Patients with BJV-valved conduits had higher systolic gradients from the right ventricle to the pulmonary artery (RV–PA) compared to those with monocusp-valve patches. BJV-valved conduit implantation was a risk factor for post-operative pulmonary-valve stenosis. The QOL score for patients with BJV-valved conduits was lower than those with monocusp-valve patches (P < 0.05). No reoperation was performed during follow-up.
Conclusions
Bronchial stenosis and lower age (≤ 6 months) were the main factors influencing post-operative survival. The use of a BJV-valved conduit was a main reason for RV–PA restenosis; thus, the use of a BJV-valved conduit may increase the need for repeat intervention and decrease the post-operative quality of life.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Absent pulmonary-valve (APV) syndrome is a rare malformation that was first described by Chevers in 1846 [1, 2]. It occurs in 3–6% patients with tetralogy of Fallot (TOF/APV) [3, 4]. The malformation comprises rudimentary or nearly APV—with aneurysmal dilatation of the pulmonary arteries—some with obstruction of its first- and second-order branches resulting in severe respiratory distress, especially during the neonatal period [5]. The mortality from surgical repair in TOF/APV patients has decreased in recent years [6,7,8], but it is still high in newborns and infants with severe respiratory compromise [5, 9].
The material to be used for the reconstruction of the right ventricular outflow tract (RVOT) in TOF/APV remains controversial. The bovine jugular vein (BJV) (Contegra, Medtronic Inc, Minneapolis, MN, USA) was introduced into clinical practice in 1999 [10]. The recognized advantages of the BJV in RVOT reconstruction include: 1) the structural continuity between the wall of the jugular vein of the conduit and valve leaflets; 2) the unlimited “off-the-shelf” availability in sizes from 12 to 22 mm in diameter; 3) the availability of long inflow and outflow that obviate the need for either proximal or distal augmentation and facilitate conduit tailoring and positioning; and 4) lack of antigenic reaction due to glutaraldehyde fixation [11]. Despite of the advantages of BJV, stenosis at the level of the distal anastomosis of the conduit, with proximal conduit dilatation, aneurysm, or pseudoaneurysm, has been reported in 6–50% of patients [12, 13].
The monocusp-valve patch was also used in RVOT reconstruction to prevent pulmonary regurgitation. Monocusp valves of various materials such as polytetrafluoroethylene (PTFE) membranes [14], pericardial patches [15, 16], homografts [17], and BJV [18] are used in the clinic. The monocusp appears advantageous in preventing severe intermediate-term pulmonary insufficiency (PI) and facilitates the preservation of RV function [14].
In this study, we retrospectively reviewed 22 TOF/APV patients who underwent a complete repair in our hospital evaluated the surgical outcome of these patients and assessed the effect of BJV-valved conduit and monocusp-valve patch in RVOT reconstruction in TOF/APV patients.
Methods
From December 2003 to January 2016, 22 consecutive TOF/APV patients who underwent surgical repair in our center were included in this study (Table 1). The protocol of this study was carried out according to the principles of the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Cardiovascular Institute and our hospital. Written informed consent was obtained from all the participants (or their parents) before enrollment. All patients (10 male and 12 female) were identified by echocardiography and then computed tomography (CT) scan to evaluate bronchial stenosis. The central venous pressure and left atrial pressure were measured in the recovery room on the day after operation. The chest tube drainage was calculated as the ratio of total chest tube drainage/basic surface area (mL/m2).
The evaluation of pulmonary regurgitation by echocardiography was semi-quantitative in our hospital. We used Arabic numerals 1, 2, 3, and 4 as the standards for no, mild, moderate, and severe pulmonary regurgitations, respectively. In mild regurgitation, the reversal of diastolic pulmonary flow was restricted within the pulmonary-valve ring. For moderate regurgitation, the pulmonary reversal flow reached the pulmonary artery trunk, but never surpassed the branches of the pulmonary artery. In severe regurgitation, the pulmonary reversal flow could be seen in branches of the pulmonary artery [19]. For comparison of echocardiographic parameters, we used a standardized diameter, e.g., the standardized diameter of the pulmonary valve was the diameter of the pulmonary valve/body surface area (BSA) at that time (PVst). We chose as endpoints, death, PV stenosis (systolic gradient ≥ 40 mmHg), PV regurgitation (severe regurgitation), and PV dysfunction (PV stenosis and regurgitation).
The BJV-valved conduit was homemade. The preparation process was as follows. First, the BJV-valved conduits obtained from cattle were rinsed, trimmed, and cleaned in ice. Second, they were fixed in 0.6% glutaraldehyde for 48 hours and then 0.3% glutaraldehyde for 2 weeks. Third, the BJV-valved conduits were taken out for further trimming and marking and then sterilized in a mixture of 25% isopropanol and 1% glutaraldehyde. Finally, they were fixed in 0.3% glutaraldehyde until clinical application.
Evaluation of health-related quality of life
To assess health-related quality of life (QOL), the parents of the patients completed the Pediatric QOL (PedsQL) Inventory [20]. The PedsQL Inventory has different versions designed for babies (13–24 months), toddlers (ages 2–4 years), young children (ages 5–7 years), children (ages 8–12 years), and teens (ages 13–18 years). QOL scores from different age groups can be compared directly. The 23-item PedsQL 4.0 Generic Core Scales encompass physical functioning, emotional functioning, social functioning, and school functioning. Here, we used the parent proxy-report formats of the PedsQL scales. Items were reverse scored and linearly transformed to a 0–100 scale, so that higher scores indicated better QOL. To create a psychosocial health summary score, the mean was computed as the sum of the items divided by the number of items in the emotional, social, and school functioning scales. In the 27-item PedsQL 3.0 Cardiac Module, there were five scales, related to heart problems/symptoms, perceived physical appearance, treatment anxiety, cognitive problems, and communication. The communication scale is not included for toddlers and young children, because they do not have the cognitive or language ability to verbalize questions to understand explanations about their hearts.
Statistical analysis
All the data are presented as the mean ± standard deviation (SD) or median with range. Comparisons between two groups were performed with Student’s t test or the paired t test. Comparisons amongst the three groups were performed with ANOVA for continuous variables. The X2 test or Fisher’s exact test was used for categorical data. For survival analysis, the patients were censored at the time of death or withdrawn alive at the time of the last follow-up. Estimates for long-term survival were performed by the Kaplan–Meier method. Differences between survival curves were evaluated with the log-rank test. Univariate analysis of time-related events was done with the log-rank test and the univariate Cox model, which allowed the selection of the variables (P < 0.05) that were included in the multivariate analysis. The multivariate Cox regression analysis was performed as conditional backward stepwise proportional hazards regression and was used for the analysis of freedom from the endpoints. All P values were two-sided, and P values < 0.05 were considered statistically significant. All analyses were performed using SPSS version 17.0.0 (SPSS Inc, Chicago, IL, USA).
Results
Patient information
The median age at operation was 10 months (range from 2.8 months to 11 years). Five patients were less than 6 months of age, while seven were between 6 months and 1 year of age. The average weight was 10.54 ± 5.89 kg. Three patients acquired a respiratory infection 1 month before their operation, but recovered pre-operatively. Bronchial stenosis was identified in five patients by CT scan and bronchoscopy (Table 1). Other cardiac anomalies are listed in Table 1. No intubation or ventilator support was required before the operations. The median follow-up time was 45.14 months (range from 0.4 to 137.3 months).
Operative technique
All procedures were performed through midline sternotomy. Cardiopulmonary bypass was established through standard aortic and bicaval venous cannulation. Moderate hypothermia (26–31 °C) and antegrade cold crystal perfusion liquid were used for myocardial protection. The mean cardiopulmonary bypass time was 130.45 ± 38.00 minutes, and mean aortic cross-clamping time was 92.64 ± 29.46 minutes (Table 1). Complete correction was performed for all TOF/APV patients. PA arterioplasty was performed in seven patients by pulmonary plication, resection or pericardial patch widening (Table 1).
The RVOT was reconstructed by monocusp valve (n = 10, 45%), homograft-valved conduit (n = 2, 9%), or homemade BJV-valved conduit (n = 10, 45%) (Table 1). In monocusp-valve repair, a valve was fashioned from homograft (n = 5, 23%), self-pericardium (n = 2, 9%), or BJV-valved conduit (n = 3, 14%). The sizes of the two homograft-valved conduits were 18 and 24 mm, respectively, while the size of the BJV-valved conduit ranged from 12 to 20 mm.
Operative result
The mean pediatric intensive care unit (PICU) stay time was 119.23 ± 95.04 hours; the median ventilation support time was 50.65 hours (15.8–336 hours); and the average length of hospital stay was 19.82 ± 8.12 days (Table 1). There were three major post-operative complications: 1) delayed sternal closure (n = 1); 2) reopening with bleeding (n = 2); and 3) residual VSD leakage (n = 1), in one of the post-operative bleeding patients.
Operative mortality (defined as death within 30 days from surgery) was 13.64% (3/22). One patient was a 3.6-month-old male, whose CT scan suggested an expanding PA compressed the proximal end of the left main bronchus and the right lobe bronchus, causing stenosis. The distal left main bronchus had secondary expansion. This patient received complete repair of the TOF/APV with a 14-mm BJV-valved conduit. However, he could not be withdrawn from mechanical ventilation after the operation, and the patient developed Klebsiella pneumoniae. He died 20 days later from respiratory failure. The second patient was a 6-month-old female, whose CT scan showed stenosis of both the left and right main bronchus. A 12-mm BJV-valved conduit was used to reconstruct the RVOT. The chest was reopened because of bleeding later on the day of operation. However, mechanical ventilation could not be withdrawn because of the bronchial stenosis, and this patient died 12 days later from respiratory failure. The third patient was a 2.9-month-old female, whose diagnosis was TOF/APV and absence of the left pulmonary artery. Her CT scan showed an expansion of the right pulmonary artery (RPA) which was compressing the right main bronchus, causing stenosis. A monocusp-valve patch fashioned from a homograft was used to reconstruct the RVOT, and the main pulmonary trunk was widened by a self-pericardial patch, which was 11 mm after repair. The expanded RPA wall was partially resected to reduce the lumen from 50 to 12 mm. This patient had delayed sternal closure, and died 13 days after the operation because of a lower respiratory tract obstruction, which progressed into heart and lung failure.
Late results
No late deaths occurred during the follow-up. The median follow-up time was 45.14 months (0.40–137.30 months) (Fig. 1a). The Kaplan–Meier curve indicated that overall survival at both 5 and 10 years was 86.4 ± 7.3% (confidence interval 69.4–97.2%). The survival rates for patients with and without bronchial stenosis were 40 and 100%, respectively (P = 0.0003, log-rank test; Fig. 1b). Patients with bronchial stenosis were younger, had a lower weight, were shorter with a smaller (BSA), and had a longer ICU stay time than those without bronchial stenosis (Supplemental Table 1). The survival of patients older than 6 months was 100%, which was higher than those who were less than 6 months of age (40%) (P = 0.0003, log-rank test; Fig. 1c). The latter group also required a longer ventilation support time and ICU stay, but had shorter bypass time and aortic clamping time than those older than 6 months (Supplemental Table 2). Some patients developed respiratory tract infections within 1 month prior to the operation. There was significant difference in survival between patients with and without infection before the operation: 33.3 and 94.7%, respectively, (P = 0.005, log-rank test; Fig. 1d). None of these patients were readmitted to the hospital for a further operation.

Kaplan–Meier survival curves. a Whole Kaplan–Meier survival was 86.4%; b survival of patients with and without bronchial stenosis; c survival of patients aged below and above 6 months; d survival of patients with and without respiratory tract infection within 1 month before operation
By Cox univariate analysis, we identified eight risk factors for survival (P < 0.05) in TOF/APV patients (Supplemental Table 3). However, using the Cox multivariable regression model, we were unable to identify any significant demographic or operative factors for long-term survival (Supplemental Table 4). After 10 years, 73, 87.1, and 63.5% of the patients were free of PV stenosis, regurgitation, and dysfunction, respectively (Supplemental Table 5).
Outcome comparison of patients with bovine jugular vein-valved conduit and those with monocusp-valve patch
According to RVOT reconstruction, the patients were divided into two groups: ten patients in one group were reconstructed by BJV-valved conduit (BJV-valved conduit group), and the other ten patients had a monocusp-valve patch (monocusp-valve group). The median age was 0.8 year (range 0.30–3.07 years) for the BJV-valved conduit group and 0.9 year (range 0.24–11 years) for the monocusp-valve group. The perioperative parameters of patients with BJV-valved conduits and monocusp-valve patches were compared. We did not find any significant difference between those two groups in perioperative parameters (P > 0.05) (Table 2), nor did we find a difference in ventilation time, ICU stay, hospital stay, central venous pressure, left atrial pressure, or chest tube drainage.
There was no significant difference in the systolic pressure gradient of the right ventricle to the pulmonary artery (RV–PA) between these two groups in echocardiography before the operation, or at 7-day post-operation (P > 0.05) (Fig. 2a), but the systolic pressure gradient RV–PA in the BJV-valved conduit group was higher than that of the monocusp-valve group at the last follow-up (P < 0.05) (Fig. 2a). In the BJV-valved conduit group, the gradient decreased greatly from 88.47 ± 18.47 mmHg before the operation to 20.71 ± 8.11 mmHg at 7-day post-operation, and then, it increased to 45.03 ± 26.09 mmHg at the last follow-up (Fig. 2a). However, at the last follow-up, the systolic gradient of RV–PA was over 40 mmHg in five patients with BJV-valved conduits in RVOT reconstruction. In the monocusp-valve group, there was a decreasing trend through these three timepoints (preoperation vs. 7-day post-operation and preoperation vs. last follow-up, P < 0.01); however, there was no increase again at the last follow-up (7-day post-operation vs. last follow-up, P > 0.05) (Fig. 2a). The difference among these three timepoint was significant (P < 0.01) (Fig. 2a).

Comparisons between patients with a BJV-valved conduit and a monocusp-valve patch. a Systolic pressure gradient of RV-PA; b pulmonary regurgitation; c standardized left ventricular end-diastolic diameter; d standardized right ventricular end-diastolic diameter. RV right ventricle, PA pulmonary artery, BJV bovine jugular vein. *P < 0.05 for BJV-valved conduit group vs. monocusp-valve patch group, †P < 0.01 for preoperation vs. 7-day post-operation, ‡P < 0.01 for preoperation vs. last follow-up, §P < 0.01 for 7-day post-operation vs. last follow-up
For pulmonary regurgitation, we did not find any difference between the two groups at any time. Nor did we find any significant difference when pulmonary regurgitation was compared among these three timepoints in each group (P > 0.05) (Fig. 2b). The standardized left ventricular end-diastolic diameter (LVst) in the BJV-valved conduit group was larger than that in the monocusp-valve group at the last follow-up (P < 0.05) (Fig. 2c). The LVst in the BJV-valved conduit group significantly increased from preoperation to the last follow-up (P < 0.01) (Fig. 2c). The LVst in the last follow-up was also higher than that at 7-day post-operation (P < 0.01), but there was no difference between the LVst preoperation and 7 days after operation in the BJV-valved conduit group (P > 0.05) (Fig. 2c). In the monocusp-valve group, there was no difference in the LVst among these three timepoints (P > 0.05). In BJV-valved conduit group, the standardized RVst decreased from 42.81 ± 8.72 preoperation to 33.78 ± 5.70 at 7-day post-operation (P < 0.01), but it increased to 38.12 ± 6.36 at the last follow-up (Fig. 2d). In the monocusp-valve group, there was no difference in the standardized RVst among these three timepoints (P > 0.05). No difference was found in the RVst between these two groups at any time (P > 0.05) (Fig. 2d).
For long-term survival, we did not find any difference between these two groups (log-rank test, P > 0.05) (Fig. 3a), but the 10-year survival of BJV-valved conduit group (80%) was lower than that in the monocusp-valve group (90%) (Fig. 3a). In the univariate analysis of risk factors for PV stenosis, regurgitation, and dysfunction, the use of the BJV-valved conduit was a risk factor for PV stenosis post-operation (Supplemental Table 3), but after multivariate analysis, we did not find a BJV-valved conduit as a risk factor for PV stenosis, regurgitation, dysfunction, or death (Supplemental Table 4). However, we did find that the monocusp-valve group had a better result in post-operative PV stenosis than the BJV-valved conduit group (log-rank test, P = 0.019) (Fig. 3b). The two groups were similar in the rates of PV regurgitation and of PV dysfunction (log-rank test, P > 0.05) (Fig. 3c, d). There was no severe PV regurgitation in the BJV-valved conduit group during the follow-up period. Two severe PV regurgitation episodes were found in the monocusp-valve group during the follow-up period.

Actuarial dynamics of the endpoint events in the BJV-valved conduit group and monocusp-valve group. a Survival comparison between patients with a BJV-valved conduit and a monocusp-valve patch; b freedom from PV stenosis in patients with a BJV-valved conduit and a monocusp-valve patch; c freedom from PV regurgitation in patients with a BJV-valved conduit and a monocusp-valve patch; d freedom from PV dysfunction in patients with a BJV-valved conduit and a monocusp-valve patch comparison. PV pulmonary valve, BJV bovine jugular vein
The evaluation of pediatric quality of life in patients with a BJV-valved conduit and patients with a monocusp-valve patch
In the parent proxy report of PedsQL Generic Core Scales, the total score in the BJV-valved conduit group was 78.12 ± 7.55, which was slightly but not significantly lower than that of the monocusp-valve group (87.24 ± 9.98) (P = 0.053) (Table 3). This suggested that the BJV-valved conduit patients had the same QOL as those with a monocusp-valve patch. For further comparison, there was no significant difference between patients with and without a BJV-valved conduit in physical health, psychosocial health, emotional functioning, social functioning, or school functioning. The cardiac module of the Parent Proxy Report of PedsQL scale was then performed to evaluate patients with cardiovascular disease. Although there was no difference in total score between those two groups, the health problems and treatment score in the BJV-valved conduit group were significantly lower than that of the monocusp-valve group (82.59 ± 7.25 vs. 91.64 ± 8.34, P = 0.03) (Table 3). No difference was present between these two groups in the other aspects, such as physical appearance, treatment anxiety, cognitive problems, and communication (Table 3).
Discussion
Although the mortality from surgical repair of complex CHD has deceased in recent years with the evolution of surgical skills and perioperative management, the surgical repair of TOF/APV patients remains a challenge, and the mortality of TOF/APV patients, especially with bronchial stenosis, remains high in most reported series [21, 22]. The BJV-valved conduit for RVOT reconstruction has been used in complex CHD worldwide [11, 23], but whether BJV-valved conduit or monocusp-valve patch in TOF/APV is a more suitable reconstruction material is not known.
In our study, the overall operative mortality rate was 13.64%, which is in the middle range of the reported early mortality rates ranging from 4 to 21% [5, 7, 9, 22, 24, 25]. Overall survival at 5 and 10 years in our study was 86.4%. This is consistent with that the 81.4% reported by Yong and associates [5] and the 78% reported by Hew and colleagues [22] at 10 years. TOF/APV presenting with respiratory distress often requires early mechanical ventilation and has poor outcomes [7]. However, as our study did not include patients requiring pre-operative mechanical ventilation support (a sign indicating severe respiratory distress), the mortality in our study might be higher than that in studies which included severely distressed patients. In the study by McDonnell et al., surgical repairs for patients with pre-operative intubation were associated with an increased risk of death or reoperation [24]. Because we do not have a pediatric medicine department, we did not have patients with lower weight severe respiratory distress requiring intubation immediately before the operation. However, TOF/APV with bronchial stenosis is still a major reason for respiratory distress, ventilation support, and poor outcomes. Nørgaard et al. found that ventilator dependency due to airway stenosis was a major risk factor, and the survival rate of patients with pre-operative ventilator dependency was also lower than that of patients with spontaneous ventilation [26].
In our study, all three deaths occurred before 6 months of age. The survival of patients older than 6 months was significantly higher than that of patients less than 6 months. Previous studies had found that patients under 1 year old had a lower survival rate. Alsoufi et al. found that all perioperative deaths were in the neonates [9]. In the study by Yong et al., early mortality occurred in two neonates (66.7%, 2 of 3) and 5 infants (20.8%, 5 of 24). There were no deaths (0%, 0 of 25) in patients older than 1 year at the time of operation. McDonnell et al. found that surgical repair in infancy was associated with an increased risk of death [24]. The high mortality of TOF/APV in infants suggested that these patients might have severe bronchial stenosis and respiratory distress, and early operation intervention was carried out to save their lives.
The management of the pulmonary valve in the surgical treatment of TOF/APV is controversial. An absent pulmonary valve results in pulmonary artery dilation, hyper-pulsatility, and secondary bronchial compression [4]. Good PV repair could prevent later PV regurgitation and RV arrhythmias, and preserve the RV function [27]. PV repair can be achieved either by valved conduit (BJV or homograft) or by monocusp-valve patch. In this study, ten patients underwent BJV repair, ten patients had monocusp-valve patches, and two received homograft-valved conduit implantation. Good prevention of severe regurgitation was seen in this study—from 10 (45%) before operation to 2 (9%) at the last follow-up (Supplemental Fig. 1). Because the homografts are not always available, BJV and monocusp-valve patch remain the most widely used techniques in TOF/APV repair.
To investigate whether the use of BJV-valved conduit for RVOT reconstruction influenced the perioperative and long-term survival, we compared the BJV-valved conduit group and the monocusp-valve group. We found no difference in perioperative parameters. These results suggest that there was no difference in perioperative recovery between patients who underwent TOF/APV repair by a BJV-valved conduit or by a monocusp-valve patch. Long-term survival study suggests the BJV-valved conduit group had a slightly lower (80%) survival than the monocusp-valve group (90%) (P = 0.54). The survival rate in patients with a BJV-valved conduit (71.4%) was lower than the monocusp-valve group (100%) in the studies by Hu et al. [8] and Nørgaard et al. [26]. Together, these data suggest that the use of a BJV-valved conduit decreases the survival rate of TOF/APV patients.
Although none of the surviving patients underwent any reoperation in our study, the higher gradients in the BJV-valved conduit group (5/10 over 40 mmHg) suggested a higher probability for re-intervention in the future. Since the Contegra BJV-valved conduit has not yet been introduced, the BJV-valved conduits in China were all homemade by local centers. The BJV-valved conduit that our center used for RVOT reconstruction has proved safe over the years [18]. Fiore et al. found that the 10-year survival of patients with the Contegra BJV-valved conduit was 88%, which was similar to our survival rate of 80% [23]. However, at 10 years, freedom from PV dysfunction was 85% in their study [23], which was higher than our result (42.9%). In another study, Breymann et al. found that the 5-year freedom from stenosis was 75%, while the 5-year freedom from regurgitation was 50% [28]. In our long-term follow-up, both the 5- and 10-year freedom from stenosis was 42.9% in the BJV-valved conduit patients, while the 5- and 10-year freedom from regurgitation was 100%, which shows that our center’s homemade BJV-valved conduit achieved a better result in regurgitation prevention, but was less favorable in stenosis prevention than the Contegra BJV-valved conduit.
The monocusp-valve patch was also applied in ten of our patients. We did not find a significant difference between the monocusp-valve group and the BJV-valved group in central venous pressure, left atrial pressure, chest tube drainage or pulmonary regurgitation after operation. The RVst in monocusp-valve group was no larger than that in the BJV-valved group after operation. The different tissue used for monocusp valves can explain some of the different results. Nath et al. found that pulmonary homograft monocusp valve provided early but gradually diminishing protection against pulmonary insufficiency without a risk of stenosis; and its function decreased over time as the RVOT grew, as the tissue underwent structural deterioration [17]. The pericardial monocusp neither reduced the severity of pulmonary insufficiency nor improved right or left ventricular function after 3-year follow-up [16]. The PTFE membrane monocusp appears to have an advantage in preventing severe intermediate-term pulmonary insufficiency and facilitates the preservation of RV function. Although we used a pericardial patch, homograft, and BJV for monocusp-valve patch in this study, the monocusp-valve group had a better LVst, better freedom from PV stenosis, and a higher QOL score than the BJV-valved group. Since the construction of the monocusp is simple, inexpensive, and reproducible, the monocusp-valve patch may be superior for RVOT reconstruction.
As surgical skills develop, we not only want to help patients’ survival, but also allow them to achieve good QOL after surgery. In this study, we evaluated the patients’ QOL by PedsQL scores, which are used worldwide [29]. During the long-term post-operative time, patients with the BJV-valved conduit had a lower QOL than patients without a BJV-valved conduit, which suggests that by the careful choice of material for RVOT reconstruction, surgeons might not only save patients’ lives, but give them a higher quality of life.
This study has some limitations. First, we do not have a pediatric medicine department in our hospital, and thus, we had no severe TOF/APV patients needing ventilation support. Second, the patient number was small, which might have influenced the results. Third, Contegra BJV was not available in China, so we had to use a homemade BJV; lastly, longer term follow-up was needed.
Pre-operative bronchial stenosis and a patient age of less than 6 months greatly influence the TOF/APV patients’ survival. A full evaluation before the operation is necessary for patients with TOF/APV. In our study, the use of a BJV-valved conduit was the main reason for RV–PA restenosis. Furthermore, long-term follow-up revealed that the use of a BJV-valved conduit for RVOT reconstruction may increase the likelihood of re-intervention and decrease the patient’s QOL after the operation. Thus, the material for RVOT reconstruction should be carefully considered.
References
Chevers N. A collection of facts illustrative of the morbid conditions of the pulmonary artery, as bearing upon the treatment of cardiac and pulmonary disease. Lond Med Gaz. 1846;38:828–35.
Chevers N. The investigation of pulmonary artery diseases. Arch Gen Med. 1847;15:488–508.
Rao BN, Anderson RC, Edwards JE. Anatomic variations in the tetralogy of Fallot. Am Heart J. 1971;81:361–71.
Lev M, Eckner FA. The pathologic anatomy of tetralogy of Fallot and its variations. Dis Chest. 1964;45:251–61.
Yong MS, Yim D, Brizard CP, Robertson T, Bullock A, d’Udekem Y, et al. Long-term outcomes of patients with absent pulmonary valve syndrome: 38 years of experience. Ann Thorac Surg. 2014;97:1671–7.
Dunnigan A, Oldham HN, Benson DW Jr. Absent pulmonary valve syndrome in infancy: surgery reconsidered. Am J Cardiol. 1981;48:117–22.
Brown JW, Ruzmetov M, Vijay P, Rodefeld MD, Turrentine MW. Surgical treatment of absent pulmonary valve syndrome associated with bronchial obstruction. Ann Thorac Surg. 2006;82:2221–6.
Hu R, Zhang H, Xu Z, Liu J, Su Z, Ding W. Late outcomes for the surgical management of absent pulmonary valve syndrome in infants. Interact Cardiovasc Thorac Surg. 2013;16:792–6.
Alsoufi B, Williams WG, Hua Z, Cai S, Karamlou T, Chan CC, et al. Surgical outcomes in the treatment of patients with tetralogy of Fallot and absent pulmonary valve. Eur J Cardiothorac Surg. 2007;31:354–9 (discussion 359).
Bové T, Demanet H, Wauthy P, Goldstein JP, Dessy H, Viart P, et al. Early results of valved bovine jugular vein conduit versus bicuspid homograft for right ventricular outflow tract reconstruction. Ann Thorac Surg. 2002;74:536–41 (discussion 541).
Prior N, Alphonso N, Arnold P, Peart I, Thorburn K, Venugopal P, et al. Bovine jugular vein valved conduit: up to 10 years follow-up. J Thorac Cardiovasc Surg. 2011;141:983–7.
Palma G, Mannacio VA, Mastrogiovanni G, Russolillo V, Cioffi S, Mucerino M, et al. Bovine valved venous xenograft in pulmonary position: medium term evaluation of risk factors for dysfunction and failure after 156 implants. J Cardiovasc Surg (Torino). 2011;52:285–91.
Corno AF, Qanadli SD, Sekarski N, Artemisia S, Hurni M, Tozzi P, et al. Bovine valved xenograft in pulmonary position: medium-term follow-up with excellent hemodynamics and freedom from calcification. Ann Thorac Surg. 2004;78:1382–8 (discussion 1382-8).
Kumar M, Turrentine MW, Rodefeld MD, Bell T, Brown JW. Right ventricular outflow tract reconstruction with a polytetrafluoroethylene monocusp valve: a 20-year experience. Semin Thorac Cardiovasc Surg. 2016;28:463–70.
Gundry SR, Razzouk AJ, Boskind JF, Bansal R, Bailey LL. Fate of the pericardial monocusp pulmonary valve for right ventricular outflow tract reconstruction. Early function, late failure without obstruction. J Thorac Cardiovasc Surg. 1994;107:908–12 (discussion 912-3).
Promphan W, Attanawanit S, Wanitkun S, Khowsathit P. The right and left ventricular function after surgical correction with pericardial monocusp in tetralogy of fallot: mid-term result. J Med Assoc Thai. 2002;85(Suppl 4):S1266–74.
Nath DS, Nussbaum DP, Yurko C, Ragab OM, Shin AJ, Kumar SR, et al. Pulmonary homograft monocusp reconstruction of the right ventricular outflow tract: outcomes to the intermediate term. Ann Thorac Surg. 2010;90:42–9.
Hu S, Xie Y, Li S, Wang X, Yan F, Li Y, et al. Double-root translocation for double-outlet right ventricle with noncommitted ventricular septal defect or double-outlet right ventricle with subpulmonary ventricular septal defect associated with pulmonary stenosis: an optimized solution. Ann Thorac Surg. 2010;89:1360–5.
Williams RV, Minich LL, Shaddy RE, Pagotto LT, Tani LY. Comparison of Doppler echocardiography with angiography for determining the severity of pulmonary regurgitation. Am J Cardiol. 2002;89:1438–41.
Varni JW, Seid M, Rode CA. The PedsQL: measurement model for the pediatric quality of life inventory. Med Care. 1999;37:126–39.
Kirshbom PM, Kogon BE. Tetralogy of Fallot with absent pulmonary valve syndrome. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2004;7:65–71.
Hew CC, Daebritz SH, Zurakowski D, del Nido PI, Mayer JE Jr, Jonas RA. Valved homograft replacement of aneurysmal pulmonary arteries for severely symptomatic absent pulmonary valve syndrome. Ann Thorac Surg. 2002;73:1778–85.
Fiore AC, Ruzmetov M, Huynh D, Hanley S, Rodefeld MD, Turrentine MW, et al. Comparison of bovine jugular vein with pulmonary homograft conduits in children less than 2 years of age. Eur J Cardiothorac Surg. 2010;38:318–25.
McDonnell BE, Raff GW, Gaynor JW, Rychik J, Godinez RI, DeCampli WM, et al. Outcome after repair of tetralogy of Fallot with absent pulmonary valve. Ann Thorac Surg. 1999;67:1391–5 (discussion 1395-6).
Chen JM, Glickstein JS, Margossian R, Mercando ML, Hellenbrand WE, Mosca RS, et al. Superior outcomes for repair in infants and neonates with tetralogy of Fallot with absent pulmonary valve syndrome. J Thorac Cardiovasc Surg. 2006;132:1099–104.
Nørgaard MA, Alphonso N, Newcomb AE, Brizard CP, Cochrane AD. Absent pulmonary valve syndrome. Surgical and clinical outcome with long-term follow-up. Eur J Cardiothorac Surg. 2006;29:682–7.
Lee C, Lee CH, Kwak JG, Kim SH, Shim WS, Lee SY, et al. Factors associated with right ventricular dilatation and dysfunction in patients with chronic pulmonary regurgitation after repair of tetralogy of Fallot: analysis of magnetic resonance imaging data from 218 patients. J Thorac Cardiovasc Surg. 2014;148:2589–95.
Breymann T, Blanz U, Wojtalik MA, Daenen W, Hetzer R, Sarris G, et al. European Contegra multicentre study: 7-year results after 165 valved bovine jugular vein graft implantations. Thorac Cardiovasc Surg. 2009;57:257–69.
Uzark K, Griffin L, Rodriguez R, Zamberlan M, Murphy P, Nasman C, et al. Quality of life in pediatric heart transplant recipients: a comparison with children with and without heart disease. J Heart Lung Transplant. 2012;31:571–8.
Funding
The study was supported by the National Natural Science Foundation of China (81400242 and 81525002) from ESW and HZ, and Program for Distinguished Professor in PUMC from HZ.
Author information
Authors and Affiliations
Contributions
ESW contributed to the conception and design, data collection, analysis, and interpretation, statistical analysis, writing of the article, and participated in the critical revision of the article and the language correction. XSF contributed to the conception and design, data collection, analysis, and interpretation. ESW and XSF contributed equally to this article. LX participated in data interpretation. SJL contributed to the critical revision of the article and the statistical analysis. HZ contributed to the conception and design, data analysis, critical revision of the article, and language correction. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
The protocol of this study was carried out according to the principles of the Declaration of Helsinki and approved by the Medical Ethics Committee of Cardiovascular Institute and Fuwai Hospital. Written informed consent was obtained from all the participants before enrolment.
Conflict of interest
No financial or nonfinancial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Wang, ES., Fan, XS., Xiang, L. et al. Surgical outcome after complete repair of tetralogy of Fallot with absent pulmonary valve: comparison between bovine jugular vein-valved conduit and monocusp-valve patch. World J Pediatr 14, 510–519 (2018). https://doi.org/10.1007/s12519-018-0169-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12519-018-0169-z