
Abstract
Background
Captopril is well tolerated in most patients. There is no report of acute deterioration in renal function after administration of captopril in neonates with congestive heart failure secondary to congenital heart defects with large left-to-right shunts.
Methods
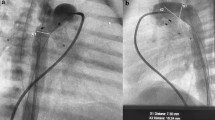
We report a premature neonate with double outlet right ventricle and congestive heart failure who developed acute renal failure after administration of captopril at a low dose of 0.1 mg/kg per 8 hours.
Results
On the third day after captopril therapy, the levels of serum creatinine and blood urea nitrogen increased to 2.6 mg/dl and 73 mg/dl respectively, and hyperkalemia appeared. Captopril was discontinued immediately. On the fourth day, the infant developed oliguria which persisted for 24 hours and resolved on the fifth day when the serum potassium normalized to 4.5 mmol/L. The level of serum creatinine peaked at 3.9 mg/dL on the sixth day and gradually decreased to normal on the ninth day after administration of captopril. The captopril-induced acute renal failure resolved completely after cessation of the drug.
Conclusions
Attention should be given to captopril therapy in premature neonates with congestive heart failure secondary to congenital heart disease with large left-to-right shunts. Routine hemodynamic examination and biochemical monitoring are suggested before and during captopril therapy.
Similar content being viewed by others

References
Hoch M, Netz H. Heart failure in pediatric patients. Thorac Cardiovasc Surg 2005;53(Suppl):S129–134.
Wood EG, Bunchman TE, Lynch RE. Captopril-induced reversible acute renal failure in an infant with coarctation of the aorta. Pediatrics 1991;88:816–818.
Yared A, Ichikawa I. Postnatal development of glomerular filtration. In: Polin RA, Fox WW, eds. Fetal and neonatal physiology. Philadelphia: Saunders, 1998:1588–1592.
Tufro-McReddie A, Gomez RA. Ontogeny of the reninangiotensin system. Semin Nephrol 1993;13:519–530.
Scammell AM, Arnold R. The effect of the first dose of captopril on blood pressure in infants in heart failure. Int J Cardiol 1989;22:377–379.
Al Shohaib S, Raweily E. Acute tubular necrosis due to captopril. Am J Nephrol 2000;20:149–152.
Blythe WB. Captopril and renal autoregulation. N Engl J Med 1983;308:390–391.
Smith WR, Neill J, Cushman WC, Butkus DE. Captopril-associated acute interstitial nephritis. Am J Nephrol 1989;9:230–235.
Hoitsma AJ, Wetzels JF, Koene RA. Drug-induced nephrotoxicity. Aetiology, clinical features and management. Drug Saf 1991;6:131–147.
Brion LP, Satlin LM, Edelmann CM Jr. Renal disease. In: Avery GB, Fletcher MA, MacDonald MG, eds. Neonatology: pathophysiology and management of the newborn. Philadelphia: Lippincott Co, 1999:887–973.
Packer M, Lee WH, Medina N, Yushak M, Kessler PD. Functional renal insufficiency during long-term therapy with captopril and enalapril in severe chronic heart failure. Ann Intern Med 1987;106:346–354.
Harrison AM, Davis S, Eggleston S, Cunningham R, Mee RB, Bokesch PM. Serum creatinine and estimated creatinine clearance do not predict perioperatively measured creatinine clearance in neonates undergoing congenital heart surgery. Pediatr Crit Care Med 2003;4:55–59.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tan, LH., Du, LZ., Carr, M.R. et al. Captopril induced reversible acute renal failure in a premature neonate with double outlet right ventricle and congestive heart failure. World J Pediatr 7, 89–91 (2011). https://doi.org/10.1007/s12519-011-0252-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12519-011-0252-1