
Abstract
Direct oral anticoagulants (DOACs) are recommended by several scientific societies as first-line therapy for the prevention of stroke and systemic embolism in patients with atrial fibrillation. However, there is uncertainty regarding the organisation of anticoagulation care, with various caregivers being involved. Patients and caregivers are often confronted by uncertainty about the coordination of treatment. With the functional resonance analysis method we visualised the process of anticoagulation care in daily practice in the Maastricht region. This resulted in recommendations on how to improve the organisation of anticoagulation care for DOAC patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Current situation regarding anticoagulation care in the Netherlands
Anticoagulation therapy is effective for patients with an increased risk of thromboembolic events. Direct oral anticoagulants (DOACs) are replacing vitamin K antagonists (VKAs), primarily driven by new guidelines, in which DOACs are preferred to VKAs [1,2,3,4,5,6,7,8,9,10,11]. This change has major consequences for the anticoagulant care landscape. In the Netherlands, VKA patients are actively monitored and supervised by the anticoagulation clinic (AC). Patients that start on a DOAC are no longer under regular surveillance by the AC, as their service is exclusively funded by insurance companies, based on INR performance and dosing advice, linked to VKAs. Monitoring of DOAC patients was initially predominantly provided by medical specialists, nowadays increasingly by general practitioners (GPs). Optimal anticoagulant treatment should preferably involve personalised medicine, which in an era of switching from VKAs to DOACs will take time to be implemented [11, 12]. The Dutch National Standard for Integrated Care (LSKA 2.0) states that care must be organised for all patients on (any form of) antithrombotic medication. One major issue in care for DOAC patients is the lack of a structured follow-up. The LSKA 2.0 recommends an at least annual evaluation of all aspects of anticoagulation, including laboratory tests for liver and kidney functions. In addition, adherence to medication should be verified, and complications and side-effects must be recorded, as recommended by national (LTA 2019, in preparation) and international guidelines [11, 13]. All these aspects are clinically relevant, as both non-adherence and prescription of too low doses of DOAC are frequently observed in real-life studies [14, 15]. The upcoming Dutch guideline (LTA 2019) is in agreement with this, and states that the responsibility in DOAC treatment and follow-up should be shared between patient, pharmacist and medical specialist.
Analysing the current situation with the functional resonance analysis method
Many causes of failure to comply with guidelines and of lack of adherence to medication have been considered [16]. In addition to the search for guideline non-adherence and root causes of complications (the Safety‑I approach), a promising new perspective has become available, with insight into what can be learned from daily practice, providing the basis for improvement initiatives [17]. This Safety-II perspective tries to understand how processes usually go right and how this relates to predefined procedures, such as protocols [18]. A useful tool for this purpose is the functional resonance analysis method (FRAM), which has been endorsed by safety experts, as a promising way to improve safety in complex systems such as healthcare [19].
FRAM is a method to visualise processes as they are carried out in everyday practice (‘work-as-done’). Based on this information, good practices in the process can be identified, but also points for improvement and possible risks. As described previously [20, 21], the findings of a FRAM analysis help to initiate practically feasible improvement initiatives. This may contribute to quality and safety management, optimisation of work processes, prospective risk analysis, analysis of incidents and development and implementation of protocols [19, 22, 23].
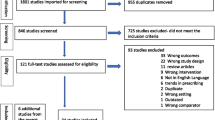
All essential activities that build up a process are described in models. In these models, activities are depicted as hexagons with six different labels (Fig. 1). Information on these activities can be obtained from various sources, including interviews and documentation. For detailed information on FRAM, we refer to practical instruction guides and previous publications [19,20,21,22,23].

The functional resonance analysis method (FRAM) function with all aspects. (To do X can represent any activity). I Input: what the activity starts or changes, O Output: the result of the activity, P Condition: a condition that must be present before the activity can be performed, R Source: material required to perform the activity, or used during the performance of the activity, C Control: how the activity is monitored, guidelines, T Time: time aspects that influence the activity

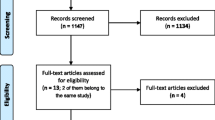
Work-as-done FRAM model of the organisation of care for patients using direct oral anticoagulants (DOACs), beginning in the left part of the figure with prescription of a DOAC by a medical specialist or GP (1, 2). Then the patient goes to the pharmacy to pick up the DOAC (3, 4). Thereafter, the patient starts taking the DOAC (5), and monitoring is done by various healthcare providers in primary or secondary care (6–9). (HCP healthcare professionals)
We used FRAM to gain insight into how care for patients on DOAC is arranged in daily practice, from the moment of prescription in the hospital setting, up to and including the follow-up (Fig. 2). This was based on semi-structured interviews with the following stakeholders: general practitioners (2), home care nurse (1), coordinator of home care for patients with ischaemic cerebral events (1), dentist (1), pharmacists (2), cardiologists (2), gastroenterologist (1), neurologist (1), internist (1). We questioned them about their role in the process and their collaboration with other professionals. One patient was also interviewed.
After written consent, interviews were audio recorded and summarised immediately afterwards. Interviews were guided by a topic list, with minor adjustments made per specific discipline [21] and were conducted until data saturation was reached [24]. Afterwards, a discussion meeting was organised to present the final model to the stakeholders and other authors as a means of validation, and to elaborate on potential clinical implications and recommendations. The analysis was done under the auspices of the Thrombosis Committee of the Maastricht University Medical Centre.
We identified the most important points for improvement in the process and structured the findings of our FRAM analysis based on four perspectives: task division and role clarity, multidisciplinary collaboration, efficiency, and guidance and support [23].
Task division and role clarity
Our study showed that there is no agreement on follow-up responsibilities, with both GPs and medical specialists not knowing who is responsible. Primary care stakeholders indicated that for them it is often unclear which medical specialist is responsible. This is due to the fact that the main responsibility is dependent on the situation rather than structural. For example, if a patient is treated by a cardiologist, renal function is checked during the periodic visit. However, the frequency of visits differs per patient. The internist pointed out that even if renal function is checked, no action is taken when changes in clearance are observed. Because of this lack in clarity about the role that each professional has within the anticoagulation chain, assumptions are made about each other’s role.
Multidisciplinary collaboration
Multidisciplinary collaboration between peripheral pharmacy and GPs is good because their electronic systems are linked. However, the way information between transmural pharmacy, GP and medical specialists is shared, is less structured. The national database (Landelijk Schakel Punt, LSP) used by the pharmacy is hardly used by GPs or medical specialists. Apart from the LSP, there is no standard communication method between medical specialists and GPs. In particular, the transfer of renal function monitoring is highly variable. The letter of discharge from the hospital or outpatient clinic sent to the GP sometimes includes the advice to check renal function, but this information is often lacking. There is also no check on whether this advice has been followed by the GP. Furthermore, structural transmission of information to home care nurses is lacking. Especially the actual medication overview (AMO), a document that lists all medication that is currently taken by the patient, is often missing or incomplete. Medical specialists indicated that, overall, they assume that the pharmacy ‘will know’ about the medication. However, home care nurses are dependent on the AMO to be able to administer the correct medication to the patient.
Efficiency
If the AMO is missing, it takes home care a lot of extra time to retrieve the data from the doctor/pharmacy or the patient. Although there is a policy regarding the provision of AMOs, adherence to this policy is still poor.
Guidance and support
Overall, the information at the start of DOAC treatment is adequate. Most professionals prefer DOACs, mainly for convenience reasons, but according to their perspective this could also be a pitfall. Healthcare providers are not always aware of the risks of the DOAC. Also, the lack of routine as well as knowledge gaps might have an impact. Furthermore, the convenience aspect may lead to incautious behaviour on the part of patients.
The ‘peripheral’ pharmacy has some insight into therapy compliance; their system provides a signal when patients should come to collect their follow-up DOAC prescription. This means that the pharmacy checks compliance at least once every 3 months. This is in contrast to the in-hospital pharmacy, which has very limited insight into therapy compliance. Although it is mandatory to consider renal function when prescribing a DOAC, this is not always done or checked. At the pharmacy, renal function is considered when filling the first prescription but not for repeat prescriptions.
How to improve anticoagulation care
This FRAM analysis provided insight into the process of care for DOAC patients in daily practice. Based on this analysis, we recommend the following to improve the organisation of anticoagulation care for DOAC patients.
First of all, it is necessary to clarify roles and responsibilities for medical specialists involved in the monitoring of DOAC patients. Who does what and how frequently? It is important that everyone is aware of these agreements, so that no incorrect assumptions are made. Therapy compliance and dosage are currently not structurally monitored and should be incorporated in patient follow-up. It will be helpful to structure follow-up, for example with automated signals, doctor alerts for renal function or, if needed, by organising care within a specialised DOAC clinical care pathway or clinic.
Further, the information transfer between professionals needs to be optimised. It is desirable that transfer takes place in a more timely, consistent, accurate and systematic way. This requires clear agreements and adequate action by the professionals involved. Ideally, using a single, generally accessible information system would greatly improve information transfer.
It is also recommended that knowledge about DOACs be increased among professionals. Not every professional is aware of the potential risks of DOACs; in particular, primary care professionals (home care, GP and dentist) lack knowledge and routine.
Limitations
This FRAM analysis was performed in the Maastricht area. It can be expected that a FRAM analysis performed in other regions of the Netherlands might have differed to some extent. However, knowledge of internal and external variability was considered when the model was analysed. Knowledge of how care for patients using DOACs is organised in different regions of the Netherlands led us to conclude that this FRAM analysis is representative of the overall situation in the Netherlands.
References
Connolly SJ, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139–51.
Granger CB, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981–92.
Patel MR, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883–91.
Giugliano RP, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093–104.
Schulman S, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361(24):2342–52.
EINSTEIN Investigators, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363(26):2499–510.
EINSTEIN–PE Investigators, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366(14):1287–97.
Agnelli G, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799–808.
Hokusai-VTE Investigators, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. 2013;369(15):1406–15.
Torbicki A, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008;29(18):2276–315.
Kirchhof P, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893–962.
Hendriks JM, Heidbuchel H. The management of atrial fibrillation: An integrated team approach—Insights of the 2016 European Society of Cardiology guidelines for the management of atrial fibrillation for nurses and allied health professionals. Eur J Cardiovasc Nurs. 2019;18(2):88–95.
January CT, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in collaboration with the Society of Thoracic Surgeons. Circulation. 2019;140(2):e125–e51.
Manzoor BS, et al. Real-world adherence and persistence with direct oral anticoagulants in adults with atrial fibrillation. Pharmacotherapy. 2017;37(10):1221–30.
Barra ME, et al. Evaluation of dose-reduced direct oral anticoagulant therapy. Am J Med. 2016;129(11):1198–204.
Seelig J, Hemels MEW. Adherence to anticoagulation: an ongoing challenge. Neth Heart J. 2019;27(12):594–5.
Hollnagel E. Safety I and Safety II. The past and future of safety management. Farnham: Ashgate; 2014.
Hollnagel E, Braithwaite J, Wears RI. Resilient health care. Farnham: Ashgate; 2015.
Raben DC, Bogh SB, Viskum B. Learn from what goes right: a demonstration of a new systematic method for identification of leading indicators in healthcare. Reliab Eng Syst Saf. 2018;169:187–98.
Damen NL, et al. Preoperative anticoagulation management in everyday clinical practice: an international comparative analysis of work-as-done using the functional resonance analysis method. J Patient Saf. 2018; https://doi.org/10.1097/PTS.0000000000000515.
Hollnagel E, Hounsgaard J. FRAM—The functional analysis method—a handbook for practical use of the method. Middelfart, Denmark. 2014. http://functionalresonance.com/onewebmedia/FRAM_handbook_web-2.pdf. Access date 14 january 2020.
Clay-Williams R, Hounsgaard J, Hollnagel E. Where the rubber meets the road: using FRAM to align work-as-imagined with work-as-done when implementing clinical guidelines. Implement Sci. 2015;10:125.
Damen NL, de Vos MS. Experiences with FRAM in Dutch hospitals: lessons from our resilient journey. Resilient Health Care. 2020;6:. Muddling through with purpose (in press).
Mason M. Sample size and saturation in PhD studies using qualitative interviews. 2010. http://www.qualitative-research.net/index.php/fqs/article/view/1428. Accessed 25-10-2019.
Acknowledgements
We acknowledge the substantial, voluntary input from the different stakeholders that provided the data for this paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
H. ten Cate is Chair of the Federation of Dutch Anticoagulation Clinics (FNT). He received research support from Bayer and Pfizer and consultancy fees from Bayer, Pfizer, LEO and Alveron. A.J.W. Gulpen, J.K. van Dijk, N.L. Damen, S. Schalla and A.J. ten Cate-Hoek declare that they have no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gulpen, A.J.W., van Dijk, J.K., Damen, N.L. et al. Organisation of care for patients using direct oral anticoagulants. Neth Heart J 28, 452–456 (2020). https://doi.org/10.1007/s12471-020-01436-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12471-020-01436-8