
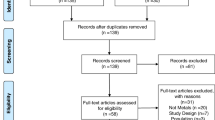
Abstract
About nine million Artisanal and Small-scale Gold Mining (ASGM) workers in Africa and people living near ASGM activities are highly exposed to geogenic and anthropogenic potentially toxic elements (PTEs). Despite the hazards and risks posed by ASGM being well characterized, coordinated multidisciplinary environmental characterization with combined public health studies are limited, with often piecemeal and snapshot studies reported, as highlighted by this review. Furthermore, studies are often not connected with efforts to minimize hazards holistically. Given this, we systematically reviewed the scientific literature on human health hazards associated with ASGM in Africa through Google Scholar, Science Direct, and Pubmed databases. One hundred and seventy-three peer-reviewed papers published between 1996 and June 2023 from 30 African countries were identified. Toxicological environmental hazards were reported in 102 peer-reviewed papers, notably As, Cd, CN, Cr, Hg, Pb, respirable SiO2-laden dust, and radionuclides. Exposure to PTEs in human biomonitoring matrices and associated health impacts were documented in 71 papers. Hg was the most reported hazard. Gaps in research robustness, regulation and policy framework, technology, risk detection, surveillance, and management were found. Despite international and in-country mitigation efforts, ASGM-related hazards in Africa are worsening. This review paper highlights the need for coordinated action and multidisciplinary collaborative research to connect dispersed isolated studies to better characterize the associated disease burden associated with ASGM in Africa and sustainably maximize the wider benefits of ASGM whilst protecting public health and the environment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Artisanal and small-scale gold mining (ASGM) presents serious but preventable hazards (Landrigan et al. 2022; WHO 2016). It occurs in over 80 low- and middle-income countries (LMICs), accounts for 20–25% of gold production, and employs 15–20 million people (WGC 2022). The ASGM communities often work without pollution and safety controls and live in heavily polluted environments (Allan-Blitz et al. 2022; Bugmann et al. 2022; Schwartz et al. 2021; Singo et al. 2022a, b; WGC 2022). Africa produced 677–740 metric tons of gold annually between 2017 and 2021 (Sasu 2023). Burkina-Faso, Democratic Republic of Congo, Ghana, Madagascar, South Africa, Sudan, and Tanzania accounted for the most significant production, with 25–100% attributed to ASGM (Jennings 1999; Schwartz et al. 2021; Seccatore et al. 2014; Uganda-NEMA 2019). Across Africa, surface mining, hard rock mining, mechanized cyanidation and hydrometallurgy are the primary techniques used in ASGM depending on the location and value of gold deposits (Table 1). Generally, unsafe working conditions, crude technology, unskilled labour, and poor waste management are significant challenges in ASGM (Basu et al. 2015; Stemn et al. 2021) (Fig. 1) and promoting safer and more sustainable ASGM practices is critical continent wide. The sector has contributed to economic growth and employment in many African nations. For instance, in Ghana, the gold mining industry contributed 7% of the national gross domestic product (GDP) in 2019, with ASGM accounting for 35% (Afrifa et al. 2019; Bakia 2014; Macdonald et al. 2014; Spiegel and Viega 2006; Taux et al. 2022). In Uganda, 7.1 t per year, equating to 90% of the annual gold production, comes from ASGM (Uganda-NEMA 2019). However, limited regulation, inappropriate ASGM technologies, and long gold value chains have resulted in limited economic benefits (WGC 2022) and significant environmental damage and health burdens at the local level (Basu et al. 2015, 2011; Dooyema et al. 2012a; Landrigan et al. 2022; Plumlee et al. 2013; Rajaee et al. 2015a; Ralph et al. 2018) as ASGM activities rapidly expand (WHO 2016).

Summary of ASGM processes across Africa
Detrimental environmental effects, injury, disease, and premature deaths in ASGM are significant issues in Africa (Bose-O’Reilly et al. 2008a; Dooyema et al. 2012b; Gibb and O’Leary 2014; Ismawati 2016; Nyanza et al. 2019; Steckling et al. 2011), a continent severely affected by climate change and strained health infrastructure (Landrigan et al. 2022). The key but neglected hazards to human health in ASGM are potentially toxic elements (PTEs) and physical hazards, most notably airborne dust, gaseous emissions, overexertion, physical injuries and related deaths, excessive noise, excessive heat, and poor ventilation inside the mines. Additional hazards include violence, prescription drugs, alcohol, illicit drug addiction, and a higher risk of infectious diseases, including HIV/AIDS and respiratory ailments (Basu et al. 2015; Singo et al. 2022a, b; WHO 2016; Mbuya et al. 2023). Over nine million workers still directly engage in hazardous ASGM activities in Africa (WGC 2022), putting their lives and those of others at risk. Regulations in the sector are lacking, evolving, or not enforced continent wide (Fritz et al. 2018b; Mallo 2012; Plumlee et al. 2013; Rajaee et al. 2015a; Schwartz et al. 2021; Wireko-Gyebi et al. 2022), leading to unabated degradation of land, waterways, food sources, and air, leading to human exposure to multiple toxic hazards (Bose-O’Reilly et al. 2020; Dooyema et al. 2012b; Keita et al. 2018; Nyanza et al. 2019; Plumlee et al. 2013; WHO 2016).
Multiple toxic hazards, primarily PTEs such as As (arsenic), CN (cyanide), Cr (chromium), Cd (cadmium), Hg (mercury), and Pb (lead); silica (SiO2); and physical hazards, mainly airborne dust, radionuclides, accidents, and the high risk of infectious diseases are of great public health concern in ASGM across the African continent. They affect both ASGM workers and residents living in exposed areas (Basu et al. 2015; Dooyema et al. 2012a; Ismawati 2016; Mambrey et al. 2020; Mtetwa and Shava 2003; Rajaee et al. 2015b; Rakete et al. 2022; Sako and Nimi 2018). Therefore, this review aims to provide a coordinated assessment of environmental and public health studies associated with ASGM in Africa, with the following objectives: (1) Evaluate the documented literature on toxic environmental hazards, related human exposure and health impacts; (2) Characterize the toxic health risks; and (3) Identify continent-wide strategies for mitigating hazards that improve the sustainability of ASGM by reducing the impact on environmental quality and human health.
Methods
The Google Scholar, Science Direct, and Pubmed databases were used with the following predefined search terms: Africa; artisanal small-scale gold mining; artisanal gold mining; environmental pollution; heavy metals; human exposure; health impacts; and names of African countries where ASGM is known to occur. One hundred seventy-three articles that reported multiple toxic environmental hazards in ASGM, most notably PTEs, like As, Cd, CN, Cr, Hg, Ni, and Pb, amongst others; respirable SiO2-laden dust and radionuclides; related human exposures; associated health effects; and biomarkers and biomonitors of toxic exposures amongst people working and living in ASGM areas in Africa were included. Seventy-seven articles that documented malaria, cholera, and hepatitis; malnutrition; heat stroke; and traumatic hazards, including cave-ins, burns, animal attacks, falls, and weapon-inflicted wounds, were excluded (Moher et al. 2009).
The following variables were extracted from articles and reports that met the inclusion criteria: date of the publication; study area and country; report on toxic hazards in the environment (soil, water, sediment, air, plants, food); report on the toxic hazards identified by human biomonitoring matrices (blood, hair, nails, urine, breast milk, saliva); the number of samples; report on study participants/population; report on interventions or treatment provided and outcomes; particular toxic hazard or risk; and documented health effects.
Results and Discussion
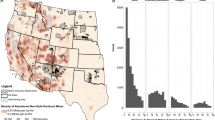
One hundred seventy-three studies published from 1996 through June 2023 (Supplementary Tables 1–5) across 30 different African countries, as presented in Fig. 2, were evaluated. The ASGM activities reported in these publications are spatially concentrated in West, South, East, and Central Africa (Fig. 2). One hundred and two evaluated studies reported toxic environmental hazards (Supplementary Tables 1–3). The human biomonitoring matrices data evaluated in 71 studies present both occupationally (n = 3,749 subjects) and inadvertently (n = 3,815 subjects) exposed subjects and associated documented health effects (Table 4; Supplementary Tables 4 and 5). Most residents, non-ASGM workers, farmers, and fishermen were classified as non-occupationally or inadvertently exposed. In contrast, most occupationally exposed subjects were miners, ore processors, and gold traders, who were anticipated to become increasingly exposed due to the nature of their work. Concentrations of PTEs in the blood (n = 2418 samples), breastmilk (n = 120 samples), hair (n = 1,599 samples), nails (n = 329 samples), and urine (n = 2,948 samples) were used to estimate exposure. More commonly, environmental concentrations of PTEs in soils, food, water, and air are used to estimate human exposure through predictive models and the associated hazards to health, including cancer risk.

Map of sampling sites of studies on toxic environmental hazards in artisanal and small-scale gold mining, related human exposure, and health impacts in Africa. (Map produced using Arc Map 10.4.1, Esri, 2016, using data from the reviewed studies)
Toxic Environmental Pollution in Artisanal and Small-Scale Gold Mining in Africa
Artisanal and small-scale gold mining negatively impacts the environment during ore exploration and mining, ore processing, gold recovery and purification, and waste dumping (Basu et al. 2015; Haidula et al. 2011; Ngole-Jeme and Fantke 2017; Plumlee et al. 2013). One hundred and two studies reported multiple toxic environmental hazards in ASGM in 30 countries, as presented in Supplementary Tables 1, 2, and 3 whilst summarized in Table 2 for selected PTEs. Exceedance of threshold concentrations of multiple toxic hazards, most notably, potentially toxic metals, As, CN, SiO2, and radionuclides are given for African examples for soils, sediments, surface and ground waters, fish, food crops and wild plants, and air (Black et al. 2017; Gyamfi et al. 2020).
Before ASGM activities commence, trees and vegetation cover are cleared, and large portions of agricultural land are often destroyed (Pancrace et al. 2022; Rajaee et al. 2015a). Miners typically use traditional methods, primarily indigenous knowledge, to explore gold deposits and break ores into smaller pieces. The ores are ground using locally fabricated ball mills to a fine powder, dispersing dust onto nearby vegetation, food crops, soils, houses, and surface waters. Ground ore is wetted and sluiced to concentrate gold particles. Sluice cloths are then washed in water buckets to remove concentrated gold. Panning separates gold-associated sediment particles, to which liquid Hg is added and kneaded to amalgamate gold in order to separate it from the sediment matrix. Continued panning and amalgamation may result in loss of Hg into discharged water or sediments. However, the Hg–Au amalgam is burnt to vaporize Hg and obtain pure gold, creating a highly mobile and toxic route of Hg exposure (Fig. 1). Sometimes, the Hg is added to the mined ore before or during crushing, a process called complete ore or whole ore amalgamation (Fig. 1) (Afrifa et al. 2019; Lassen et al. 2016).
Arsenic and Pb mainly occur in gold-sulphide deposits as minerals arsenopyrite (FeAsS) and galena (PbS). Other PTEs, most notably Ag (silver), Be (beryllium), Bi (bismuth), Cd, Co (cobalt), Cr, Cu, Fe, Hg, Ni, Mn (manganese), Os (osmium), Pd (palladium), Pt (platinum), Re (rhenium), SiO2, Sn (tin), and Zn, also occur naturally with gold ores (Doyi et al. 2016; Khafouri et al. 2021; Netshitungulwana 2011; Ondayo et al. 2023; Plumlee et al. 2013; Thiombane et al. 2023). These minerals are relatively stable under natural conditions, but mining and other ASGM activities expose them to oxygen and water, which dissolve and oxidize the metals to less stable and more reactive species (Kaninga et al. 2019; Ogola et al. 2002; Plumlee et al. 2013). Elemental Hg and CN are introduced during ore processing (Clifford 2017; Kristensen et al. 2014; Nyanza et al. 2014a, b; Ogola et al. 2002). Mercury released during amalgam burning can be inhaled or dispersed more widely into the environment. Surface run-offs and wind are important migration routes for Hg and other PTEs from the ASGM process into nearby waters and soils (Nyanza et al. 2014a; Veiga and Hinton 2002; Veiga and Baker 2004). Microorganisms biotransform elemental and inorganic Hg into methyl mercury (MeHg) in waterways. This neurotoxin (MeHg) bioaccumulates in fish and other aquatic animals and often biomagnifies in higher trophic food chain levels, posing risks to fish-consuming communities and persons consuming other contaminated animals and animal products, such as milk, eggs, and meat (Abdelaal et al. 2023; Adimado and Baah 2002; Gerson et al. 2018b; Niane et al. 2015; Telmer and Veiga 2009).
Potentially toxic metals (n = 102 studies) are the most studied environmental hazard in ASGM, with few studies reporting radionuclides (n = 5) (Ebongue and Njock 2018; Kamunda 2017; Kamunda et al. 2016; Klubi et al. 2020; Rwiza et al. 2022; Wanyama et al. 2020), silica (n = 3) (Bråtveit et al. 2003; Gottesfeld et al. 2015; Moyo et al. 2021), airborne Hg vapours (n = 2) (Black et al. 2017; Gyamfi et al. 2020), and CN (n = 4) (Knoblauch et al. 2020; Obiri et al. 2006; Porgo and Gokyay 2017; Razanamahandry et al. 2018). Subsequently, Hg is the most documented metal pollutant associated with ASGM (Further detail in Supplementary Tables 1–3).
Across the continent, hazardous wastes generated by ASGM processes are often poorly managed. Tailings with residual Hg and other PTEs; exhausted wastes from cyanidation plants; dust laden with SiO2 and other PTEs from ore crushers, inside mine shafts and tunnels; and wastewater and gases, including volatile Hg, are often released into the atmosphere, soils, water systems, and food sources untreated (Black et al. 2017; Ngole-Jeme and Fantke 2017; Omara et al. 2019a, b; Podolský et al. 2015; Talla and Moandjim-Me-Bock 2018; Tibane and Mamba 2022). For instance, there are increasing concerns about the extensive drinking water contamination and soil pollution caused by leaching from waste heaps and spillages from tailings storage areas and solution ponds (Basu et al. 2015; Bitala et al. 2009; Hilson and Monhemius 2006; Khafouri et al. 2021; Pascal et al. 2020). Additionally, occuptional exposure through use of CN and its complexes present severe hazards CN for workers and nearby communities (Knoblauch et al. 2020; Porgo and Gokyay 2017). Whilst CN degrades naturally in the environment, high concentrations of CN are acutely injurious to the environment and human health (Razanamahandry et al. 2018). Chemical properties and toxicity of CN depend on various factors, including exposure to light, air, and other metals. In ASGM, Hg-CN complexes formed when Hg-contaminated tailings are reprocessed with CN pose more significant health risks exponentially as Hg becomes readily methylated and more bioavailable (Hilson and Monhemius 2006; Veiga et al. 2009). Thus, the Minamata Convention on Mercury bans the application of CN to Hg-containing tailings and recommends the legal use of CN in gold mining by organized and trained miners in compliance with chemical management protocols (Minamata-Convention-on-Mercury 2021b; Stapper et al. 2021).
Migration Pathways and Routes of Exposure to Multiple Toxic Hazards Amongst ASGM Workers and Nearby Populations
The review found that ASGM is a source of constant high-dose exposure to multiple toxic hazards amongst workers and populations living nearby. The human biomonitoring studies evaluated (n = 71) reported significant body burdens of PTEs above thresholds in the blood (n = 27 studies), breast milk (n = 2 studies), nails (n = 9 studies), hair (n = 28 studies), urine (n = 30 studies), and inhaled air drawn from ASGM workers and nearby populations across Africa as fully detailed in Supplementary Table 4 and summarized in Table 3. Urine, hair, and blood are the most widely used biomonitors, whilst Hg is the most studied hazard amongst ASGM workers and local communities, followed by Pb.
Several critical migration routes and pathways of human exposure to PTEs in ASGM exist. Firstly, there is a common occurrence of incidental ingestion of soils, especially by young children and pregnant women that exhibit pica (Dooyema et al. 2012b; Gottesfeld et al. 2015; Moyo et al. 2021; Nyanza et al. 2014b; Plumlee et al. 2013). For instance, high incidences of geophagy were found in 203 out of 340 pregnant women aged 15–49 years in ASGM areas in Tanzania. The consumed soil was heavily contaminated with various PTEs, including As, Cd, Cr, Hg, Mn, and Ni, posing a severe risk to foetuses (Supplementary Table 3) (Nyanza et al. 2014b). Secondly, inhalation of airborne pollutants, most notably metallic Hg vapours during amalgam burning and respirable crystalline dust containing silica and other PTEs (Afrifa et al. 2017; Black et al. 2017; Gyamfi et al. 2020; Moyo et al. 2021; Tayrab 2017), is a significant pathway in ASGM. The third major exposure route is the ingestion of contaminated water, fish, and other foods (Addai-Arhin et al. 2022; Asante et al. 2007; Niane et al. 2015; Nyanza et al. 2019, 2014a; Rakete et al. 2022; Rakotondrabe et al. 2018; Wanyama et al. 2020). Fourth, in addition to utero exposures, children can be further exposed by consuming PTE-contaminated breast milk from their exposed mothers (Bose-O’Reilly et al. 2008a, 2008b, 2020; Nyanza et al. 2019). For example, in a study, young mothers (15–42 years) living and working in ASGM were found to expose their children to Hg and MeHg through breastfeeding (Bose-O’Reilly et al. 2008b, 2020). Therefore, pregnant women, new mothers, and women who might become pregnant should be particularly aware of the potential dangers of exposure from ASGM and take precautions by halting their participation in ASGM, avoiding geophagy, and seeking medical advice (Bose-O’Reilly et al. 2020; Nyanza et al. 2019). Fifth is the direct contact with PTEs, notably Hg, CN, and contaminated ores and wastes from ASGM processes, including tailings and Au–Hg amalgam washing pond waters (Chetty et al. 2021; Duncan 2020; Laker 2023; Ngole-Jeme and Fantke 2017; Talla and Moandjim-Me-Bock 2018). Detailed investigations linking specific migration routes and pathways of human exposure to particular toxic hazards in ASGM are still limited throughout the African continent.
Human exposure in ASGM varies depending on factors, such as occupation, Personal Protective Equipment (PPE) use, gold extraction technologies, geography, geological characteristics, personal behaviour, and individual biological characteristics, such as age, sex, immunity, and genetic makeup amongst others (Abebil et al. 2023; Afrifa et al. 2017; Bose-O’Reilly et al. 2010; Dooyema et al. 2012b; Godebo et al. 2019; Gottesfeld et al. 2015; Gottesfeld et al. 2019; Tomicic et al. 2011). A relatively high proportion of African women (50–60% of the workforce) engage in ASGM compared to the global average for ASGM (10%). In terms of gender, a high proportion of women are often responsible for ore processing (ore crushing, grinding, transport, sluicing, panning, and amalgam burning), whilst men traditionally explore, prospect, excavate gold ores, and distribute the income from the sale of gold. Women also have a role in supplying mine workers with food, drinks, apparatus, and equipment onsite (Hinton et al. 2003; Wall 2010) and are indirectly exposed to ASGM activities. In some ASGM sites, children are involved in all hazardous ASGM stages: ore extraction, milling, sluicing, amalgamation, and Hg–Au amalgam burning without personal protective equipment (PPE) (Bose-O’Reilly et al. 2007). The reviewed studies reported over 3,000 children (0–17.9 years) that were both occupationally and inadvertently exposed to As, Cd, Hg, and Pb in ASGM (Afrifa et al. 2017; 2019; Bose-O’Reilly et al. 2007; Nyanza et al. 2019; Ralph et al. 2018).
The ASGM activities are often not physically segregated from the communities but rather occur near housing units and other social and economic activities. Thus, even residents of ASGM areas that do not participate in the activities are exposed to similarly significant concentrations of PTEs as the ASGM workers (Astolfi et al. 2020; Bose-O’Reilly et al. 2008b; Bose-O’Reilly et al. 2020; Dooyema et al. 2012b; Niane et al. 2015; Nyanza et al. 2019; Rabiu et al. 2019; Rakete et al. 2022). This is of particular concern since it is estimated that for every active ASGM worker, there are likely to be upwards of ten non-mining family and community members at risk of exposure to PTEs (Harada et al. 1999; Kamunda 2017; Ralph et al. 2018; Steckling et al. 2014b; Tayrab 2017; Tomicic et al. 2011). For example, there were generally no significant differences between recorded exposures for miners and non-miners in a study comparing Hg in urine drawn from miners (mean 3.6 μg/L; range 0.5–9.4 μg/L) and non-miners (mean 4.3 μg/L; range 1.1–12 μg/L) living in Takwa-Ghana and non-miners (mean 3.1 μg/L; range 1.4–5.5 μg/L) residing in Accra. Likewise, in Dunkwa-on-Offin in Ghana, reported mean Hg concentrations in hair drawn from small-scale gold miners (2.1 mg/kg) and non-small-scale miners (2.4 mg/kg) did not significantly vary (Kwaansa-Ansah et al. 2010).
Human Health Impacts of Artisanal and Small-Scale Gold Mining in Africa
Forty-nine studies across Africa have linked premature mortalities and non-communicable diseases. For example, neurological and behavioural disorders, asthma, congenital disabilities, liver, lung, heart, and kidney diseases, blood disorders, skeletal disorders, suppressed immunity, stroke, and cancers in children and adults working or living in ASGM areas. Exposure to toxic hazards, most notably heavy metals, As, CN, and respirable crystalline silica, could be both acute and chronic, as fully detailed for health implications in Supplementary Table 5 and summarized in Table 4. Health effects associated with heavy metal exposure are the most widely studied (n = 39 studies) continent wide.
Overall under-studied toxic hazards in ASGM, including radionuclides (Kamunda 2017), respirable SiO2 (Moyo et al. 2021; Ross et al. 2010; Steen et al. 1997), airborne Hg vapours (Black et al. 2017; Gyamfi et al. 2020), and CN (Knoblauch et al. 2020; Obiri et al. 2006; Porgo and Gokyay 2017) pose significant risks to human health. For instance, a study found that amalgam burners were exposed to higher airborne Hg (702,676,857 mg/m3) compared to bystanders (141,272,870 mg/m3) and the 100-mg/m3 Permissible Exposure Limit (PEL). The 8-h time-weighted average (TWA) readings for 82% of amalgam burners exceeded the PEL, with 11% having TWA values that exceeded the Immediately Dangerous to Life and Health (IDLH) level of 10,000 mg/m3. In addition, the TWA in 86% of ASGM workers at the burn points and 59% of control workers exceeded the recommended exposure limit. The detectable peak air Hg concentration was from 0 to 19, 999 mg/m3 (Black et al. 2017). Besides, the risk of silicosis, lung cancer, tuberculosis, autoimmune diseases, and deaths is increasing amongst ASGM workers and local community members exposed to respirable crystalline SiO2-ladden dust in Botswana, Ghana, Malawi, South Africa, Tanzania, and Zimbabwe (Abeid et al. 2022; Moyo et al. 2021; Ohene et al. 2021; Rambiki et al. 2020; Ross et al. 2010). However, the data collected do not accurately reflect the actual burden of the disease since diseases persist or manifest even after workers quit ASGM (Steen et al. 1997). Furthermore, predispositions and positive associations between dust exposure and incidences of cancer and infectious diseases such as COVID-19, HIV, and tuberculosis (TB) have been established in ASGM. Silicosis and HIV infection additively increase the risk of TB infection more than fifteen times (Moyo et al. 2021; Ross et al. 2010) (Supplementary Tables 5).
Once PTEs reach human bodies, their toxicities and subsequent health effects depend on the elemental oxidation state, chemical species, dosage consumed, length and frequency of exposure, age, and behavioural and biological characteristics of the recipient, amongst others. Through various mechanisms of action in exposed subjects’ cells, tissues, and organs, PTEs can induce carcinogenicity, cardiovascular toxicity, genotoxicity, hepatotoxicity, immunotoxicity, nephrotoxicity, neurotoxicity, reproductive and developmental, and skin toxicities (Mitra et al. 2022). Health effects occur even at low quantities, acute, and chronic PTE exposures and are either reversible or largely irreversible, ranging from subtle, subclinical changes in function to symptomatic and life-threatening intoxication in the human body. Generally, susceptible sub-populations that need to be aware of health protection measures in ASGM areas are those that are more sensitive to the toxic effects of PTEs (like the foetus, the newborn, children, and sick individuals) and persons exposed to higher PTEs concentrations (like the Hg–Au amalgam burners and ore millers) (Abadin et al. 2007; Chou and Harper 2007; Dooyema et al. 2012a; Fashola et al. 2016; Mitra et al. 2022; Risher 1999; Tayrab 2017). As explicitly discussed in this review, the relative scales of the short- and long-term effects of various toxic hazards in ASGM have not been wholly clarified in Africa.
Neurological Health Effects
Studies (n = 14) in ASGM across Africa document neurological effects associated with As, CN, Hg, MeHg, and Pb exposures (Table 4; Supplementary Table 5). Arsenic is known for cognitive impairment of the central nervous system as detailed in Table 5 (Thakur et al. 2021). Studies documented As exposure levels that are potentially detrimental to ASGM workers and residents’ health in Ghana (Abrefah et al. 2011; Asante et al. 2007; Basu et al. 2011; Mensah et al. 2020), Kenya (Ondayo et al. 2023), and Tanzania (Ikingura and Akagi 1996; Nyanza et al. 2019, 2014b) (Tables 2 and 3; Supplementary Tables 1–4). Similarly, a few (n = 4) studies found Cd concentrations that can potentially have adverse health effects (Adewumi et al. 2019; Asante et al. 2007; Basu et al. 2011; Rakete et al. 2022). No reported studies investigated shorter- and longer-term neurotoxic health effects or As and Cd biomarker effects in ASGM in Africa, contrary to available global evidence (Table 5).
Though limited (n = 2), findings of studies on the neurological health effects of CN use in ASGM in Africa (Knoblauch et al. 2020; Porgo and Gokyay 2017) complement the existing broader literature on neurological health effects of CN (Table 5) (Isom and Borowitz 2015). Neurological health effects due to Hg (n = 25 studies) and Pb exposure (n = 14 studies) are the most widely studied in Africa (Table 4; Supplementary Tables 4 and 5). Mercury (Hg) is known to damage the brain and the nervous systems as described in Table 5 (Zhu et al. 2022). The Hg exposures reported amongst ASGM workers and residents in Burkina Faso (Tomicic et al. 2011), Ghana (Mensah et al. 2016), Tanzania (Bose-O’Reilly et al. 2010; Harada et al. 1999), Uganda (Wanyana et al. 2020), and Zimbabwe (Bose-O’Reilly et al. 2008a; Steckling et al. 2014b) were statistically significantly associated with the neuro-psychological symptoms notably ataxia, dizziness, headaches, excessive salivation, numbness, thoracic pain, Minamata disease, and mortalities (Supplementary Table 5; Table 4), corroborating existing literature.
Besides, poisoning Pb clinically manifests as seizures, encephalopathy, headaches, cerebral palsy, and confusion and can be fatal as Pb exposure increases (Table 5) (Axelrad et al. 2022; Ortega et al. 2021), as reported amongst children in Zamafara, Nigeria (Dooyema et al. 2012b). Existing global literature also links Cu, Cr, Fe, Mn, and Zn to neurological complications, but these health effects are not documented in the reviewed ASGM studies across Africa (Mitra et al. 2022; Tinkov et al. 2021).
Cancer Effects
Clinically Established Carcinogenic Effects
As widely established in the literature (Basu et al. 2015; Landrigan et al. 2022), various cancers are linked to exposure to As (skin, bladder, lung, liver, and kidney cancers); Cd (lung, kidney, and prostate cancers); Ni (lung and nasal cancers); SiO2 (lungs and upper respiratory cancers); hexavalent Cr (lungs and upper respiratory cancers); and Pb (lung, stomach, and urinary bladder cancers) (Table 5) (IARC 2021). In the reviewed studies, As, Cd, Ni, and Pb had the most data available using reliable biomarkers (Supplementary Tables 4 and 5). Further research is critical to establishing if reported exposures may be causing cancer in ASGM communities since, to our knowledge, no clinical data exist on cancer rates in ASGM settings in Africa (Supplementary Tables 1–5).
Overall Risk Assessments of Cancer Hazards and Non-cancer Health Effects
Studies (n = 10) conducted health risk assessments for cancer and non-cancer hazard indices as results of ASGM operations amongst ASGM workers and local communities (Cobbina et al. 2011, 2013; Gyamfi et al. 2021; Kamunda 2017) (Supplementary Table 5). The cancer risk is generally increasing amongst children from ASGM communities based on the concentrations of toxic hazards detected, most notably heavy metals, As, CN, and radionuclides. For example, a hazard assessment of environmental radionuclides and heavy metals in the Westwits ASGM area in Gauteng, South Africa, found elevated heavy metal concentrations and radionuclides in soils, edible plants, and drinking water. Significant mean activity concentrations (Bq/kg) for radioactive uranium (238U), thorium (232Th), and potassium (40 K) in soil (238U 574 ± 39.5; 232 Th 49.4 ± 8.5; and 40 K 425 ± 129), plants (238U 17.4 ± 3.1, 19.7 ± 1.6; and 232Th 147 ± 9.2), and water (238U 0.7 ± 0.03, 232Th 0.56 ± 0.03, and 40 K 7.4 ± 0.6) were recorded. It was estimated that the heavy metals and the radionuclides posed an increased cancer risk to communities in the ASGM area (Kamunda 2017). Furthermore, a study evaluated human health risks from using CN in gold extraction amongst children and adults in Bogoso, Ghana and attributed most unexplained deaths experienced in the communities to accidental ingestion and dermal contact with CN water (Obiri et al. 2006). From the findings, about 230 and 43 resident adults were likely to suffer diseases related to CN intoxication via ingestion and dermal routes, respectively (Obiri et al. 2006). Findings of a study in western Kenya revealed an increased risk of non-cancer health effects (97) and cancer in adults (4.93 × 10−2) and children (1.75 × 10−1) potentially exposed to As, Cd, Cr, Ni, and Pb in 19 ASGM villages in Kakamega and Vihiga counties, Kenya (Ondayo et al. 2023).
Respiratory Problems
Few studies which were limited in range and scope reported respiratory problems linked with exposure to As, Cd, CN, and Pb (n = 2 studies), Hg (n = 6 studies), and SiO2 dust in ASGM in Africa (n = 6 studies) (Supplementary Table 5). High amounts of SiO2-laden dust common in hard rock ASGM mines and SiO2 exposure are risk factors for silicosis, lung cancer, Chronic Obstructive Pulmonary Disease (COPD), asthma, and death. Silica particles in the lung may trigger tuberculous infection (Patrick et al. 2023; Rupani 2023), as detailed in Table 5. Studies (n = 6) reported a high burden of silicosis, pneumonoconiosis, and tuberculosis among ASGM workers despite generally short exposure and latent durations (Supplementary Table 5) (Armah et al. 2021; Mbuya et al. 2023; Moyo et al. 2022; Ohene et al. 2021; Ross et al. 2010), augmenting existing literature (Table 5). Additionally, existing literature strongly and exhaustively links various respiratory problems to Al, Be, Cr, Cu, Fe, Mn, Ni, Ti, and Zn exposure (Nemery 1990; Zhou et al. 2022) (Table 5), which are not widely documented in ASGM contexts in Africa.
Other Health Effects
Studies found skin and wound infections amongst populations exposed to As and CN (Table 4; Supplementary Table 5). Skin and wound infections associated with Cr and Hg exposure (Mitra et al. 2022) have not been studied in African ASGM settings (Supplementary Table 5).
Limited studies that documented kidney damage due to exposure to Hg, Cd, and CN in ASGM continent-wide (Afrifa et al. 2017; Bose-O’Reilly et al. 2008a, 2010, 2017) (Supplementary Table 5). They are consistent with the broader existing literature summarized in Table 5. Health effects of Cr, Lithium, and Thallium on the kidneys are not documented in ASGM across Africa (Markowitz et al. 2000; Mitra et al. 2022).
Tayrab (2017) studied the impact of Hg exposure on thyroid function in African ASGM workers, augmenting existing literature (Table 5), although limited to defining an outcome for thyroid function. These health effects require further comprehensive evidence to define possible links to Hg or ASGM activities.
Findings on Hg and Pb and hypertension in ASGM Africa (Ralph et al. 2018) augment existing literature on health effects of Pb and Hg (Table 5). However, cardiovascular health effects associated with Cd, CN, and Co (Mitra et al. 2022; Simões et al. 2021; Zhang et al. 2022; Zhu et al. 2022) are not reported in ASGM in Africa.
Reproductive and developmental health effects are strongly linked with Ag, Al, As, Cd, Co, Cr, Hg, Pb, U, and V (vanadium) in the broader global literature (Table 5) (Clarkson et al. 1985; Goutam Mukherjee et al. 2022; Mitra et al. 2022). These are not widely studied in ASGM in Africa, except for a few studies (n = 10) that reported neurodevelopmental effects of PTEs in ASGM (Supplementary Table 5). The burden of reproductive and developmental health effects associated with toxic exposure in ASGM, notably in Africa, is not documented.
The broader global literature documents the immune-suppressing effects of Pb and Hg (Table 5) (Mitra et al. 2022; Pollard et al. 2019; Zhu et al. 2022), not widely and exhaustively studied in ASGM in Africa. A study reported frequent autoimmune rhinitis in 125 out of 174 Pb- and Hg-exposed miners in Batouri Gold District, Cameroon. However, rhinitis prevalence was not statistically significantly linked to Pb and Hg exposure (Ralph et al. 2018) (Supplementary Table 5).
Documented silica dust and inhaled respirable crystalline silica in ASGM in Africa (Armah et al. 2021; Gottesfeld et al. 2015) point to the potential risk of associated autoimmune diseases, notably scleroderma, rheumatoid arthritis, systemic lupus erythematosus, and some of the small vessel vasculitides with renal involvement (Carneiro et al. 2022; Hoy et al. 2022; Parks et al. 1999) although there are no studies to evidence this link. Even though studies on immune suppression effects are limited in ASGM in Africa, the prevalence of HIV (average 2%) amongst ASGM workers diagnosed with silicosis and increased tuberculosis (TB) (6766 per 100,000 cases) with the severity of SiO2 dust exposure in Zimbabwe suggested immune suppression (Moyo et al. 2022, 2021). Similar to adverse immune-suppressing effects of Cr, Be, Cd, and Au (Mitra et al. 2022), links between high-dose exposure to respirable silica dust and chronic inflammation, and fibrosis in the lung and other body organs (Carneiro et al. 2022) (Table 5) have not been explored in ASGM in Africa. Any further study would require a comprehensive inclusion of dietary and nutritional status alongside lifestyle and work activities.
Only a few studies (n = 4) in ASGM in Africa established musculoskeletal effects, notably low back pains, body pains, myalgia, severe fatigue, and hernias amongst ASGM workers and residents exposed to Hg and Pb (Afrifa et al. 2017; Mensah et al. 2016; Ralph et al. 2018; Tayrab et al. 2016) (Supplementary Table 5).
Risks Characterization of ASGM in Africa
The ASGM risks in Africa are complex and influenced by scale, techniques, regulatory environment, and PPE usage (Afrifa et al. 2017; Landrigan et al. 2022). Thus, risks should be characterized based on context. Reviewed data revealed similar dynamics of potentially toxic metals, As, CN, radionuclides, and SiO2 contamination in soil, dust, sediment, water, food, and air, with identical migration routes in ASGM across Africa (Table 2; Supplementary Tables 1–3). The ASGM workers and community members were exposed to significant concentrations of PTEs in the reviewed countries (Table 3; Supplementary Table 4). Most studies documented Hg, Pb, and As exposures and related health effects at low to moderate concentrations. The health effects generally included cell, tissue, system and organ damage, and metabolic disorders amongst exposed individuals and populations (Table 4; Supplementary Table 5). Exposures and risks to human health from under-studied respirable crystalline SiO2 dust, radionuclides, inhalation of airborne Hg vapours, CN, and other critical heavy metals in ASGM in Africa were underreported (Supplementary Tables 1–5). In order to reduce ASGM-related exposures, wet ore crushing, and milling, mechanization, extended sluice channels, and non-toxic alternatives, like borax and retorts, amongst others, have been developed and deployed in some African countries (Appel and Jonsson 2010; Aslam et al. 2022; Barasa et al. 2016; Mitchell et al. 2021; Steckling et al. 2014a; Stoffersen et al. 2019). However, adoption rates of these alternatives for ASGM in the field is low throughout the continent. This is attributed to technical issues, such as development process and complexity, know-how transfer, and adaptability of new technologies in changing environments; ASGM workers’ level of organization, responsiveness to ASGM workers’ varying needs; and the extent of supply chain collaboration (Keane et al. 2023).
This review highlights gaps in African literature compared to global evidence.
Gaps in the Representativeness of Exposure and Health Effects Research in ASGM and Inclusion of Vulnerable Groups
Less focus is put on exposure and health effects research in ASGM in Africa (n = 173 studies reviewed across 30 countries). Furthermore, limited studies represented foetus (n = 3) and children between 0 and 7 years (n = 10) who are most vulnerable to the toxic effects of various toxic hazards. The reviewed studies cover other vulnerable groups, notably young women and highly exposed ASGM workers (Supplementary Tables 4 and 5). Ethical boards, national and local environmental and health authorities, and all relevant stakeholders, including ASGM communities, should be involved in early development and all other research processes and decision-making phases. Uncertainties around involving vulnerable groups should be resolved (von Stackelberg et al. 2022; World-Bank 2020).
Data Availability, Transparency, and Quality Gaps
Similar to past efforts to build secondary data sources (Steckling et al. 2014b), this review faced data availability, transparency, and quality challenges across the African continent. A defined continent-wide research agenda in the ASGM context is critical in line with existing global initiatives, notably the Global Mercury Partnership (Minamata-Convention-on-Mercury 2021a) and the World Bank’s agenda, recognizing the ‘big global data gap’ (Keane et al. 2023; World-Bank 2020). Contrary to Europe (Apel et al. 2017; Černá et al. 2017; Schmidtkunz et al. 2019) and North America (Control and Prevention 2015; Haines et al. 2017; Saravanabhavan et al. 2017), amongst other developing countries, human biomonitoring (HBM) at a national level that includes PTEs outside of an occupational exposure environment is uncommon in Africa (Watts et al. 2021). As there are few or no reference values and biological equivalents for evaluating toxic exposure data in the context of human health in the African population, it was challenging to interpret biomonitoring data in recent studies (Nakaona et al. 2019; Ondayo et al. 2023). Future efforts should be focused on developing these in Africa. There is also a need to practically assess and update existing environmental and biomonitoring limits in order to consider low-level, chronic toxic exposures in Africa since most PTEs, for example, Pb, have been shown to have profound effects even in low to moderate concentrations (Axelrad et al. 2022).
Gaps in Assessing Toxic Hazards and Exposures, Methods Used, and Study Robustness
Highly diverse exposure assessment approaches notably sampling and analysing up to 58 PTEs in environmental (Table 2; Supplementary Table 1–3) and human (Table 3; Supplementary Table 4) media; use of risk indices; and in limited studies, use of biomarkers of effects (Abebil et al. 2023; Afrifa et al. 2017; Bose-O’Reilly et al. 2008a, 2010, 2017; Knoblauch et al. 2020; Tomicic et al. 2011). There is considerable interest in highlighting Hg pollution and its health effects in the reviewed studies. This can be explained by adopting the Minamata Convention on Mercury in 2013 (Minamata-Convention-on-Mercury 2021a). From the reviewed data, it is evident that Hg use in ASGM could be overshadowing other significant toxic exposures and health concerns in ASGM, notably other potentially toxic metals other than Hg, such as As, Cd, Co, Cr, Cu, Mn, Ni, and Zn, amongst others; CN; SiO2 dust; and radionuclides (Supplementary Table 5). Whilst international literature reports mobility, bioavailability, and toxicities of various toxic hazards (Zhang et al. 2022; Zhu et al. 2022), 90% of ASGM studies in Africa focused on quantifying total PTEs concentrations in various matrices. Few studies focused on elemental Hg vapour from amalgam burning and MeHg in fish, soils, and rice (Black et al. 2017; Gerson et al. 2018a; Gyamfi et al. 2020; Harada et al. 1999; Odukoya et al. 2022) and As speciation in soils (Mensah et al. 2020; Ondayo et al. 2023). It is crucial for future research to explore speciation as it reveals the mobility, bioavailability, and toxicity of elements, ions, and compounds, affecting their reactions and adverse health effects. For example, metallic elements are generally inert, but their ionic salts and chelates have significant bioavailability and toxicity, for example, the carcinogenic potential of various As, Cr, and Ni species (Mitra et al. 2022; Watts et al. 2008; Zhu et al. 2022). The conversion of metallic elements to organic forms makes them more lipophilic, enabling them cross-the-blood–brain barrier, like the case of organic Hg (Zhu et al. 2022).
Studies identifying the contributing role of each PTE from the myriad of other stressors in ASGM are lacking in Africa and globally. A few studies investigated exposures to multiple toxic hazards and linked them to various health effects in ASGM in Africa, but used basic scientific approaches, like hazard indices (HI) (Kamunda 2017; Olujimi et al. 2015; Ondayo et al. 2023; Rabiu et al. 2019; Ralph et al. 2018). However, toxicity mechanisms of multiple elements in a particular human or environmental media can be antagonistic, additive, synergistic, or potentiating (Zhang et al. 2022; Zhu et al. 2022). Thus, the combined health effects of a given mixture depend on individual components, the potencies, and proportions in the mixture. This is a vast knowledge gap both in Africa and globally and enhancing methods and tools for assessing human health risks from combined exposure to multiple toxic hazards, as in the case of most ASGM settings, is critical (Nikolopoulou et al. 2023). Furthermore, dermal exposure to PTEs is an essential pathway in ASGM but has not been studied (Supplementary Table 4).
Gaps in the Health Conditions Investigated, Surveillance, and Associated Burden of Disease in ASGM in Africa
Overall in ASGM in Africa, only one study calculated the burden of disease in 2004, whereby ASGM workers in Zimbabwe experienced 72% chronic Hg intoxication, causing 95,400 Disability-adjusted Life Years (DALYs) in the whole Zimbabwean population (Steckling et al. 2014b). One DALY represents the loss of one year of total health due to premature mortality and prevalent disease cases in a population (WHO 2020). Critical health impacts of toxic exposures, notably genotoxic, hepatotoxic, hepatic, and reproductive effects (Mitra et al. 2022), are not documented in ASGM in Africa (Table 4; Supplementary Table 5). Besides, respective studies did not holistically look at all potential effects of investigated toxic hazards on health (Table 4; Supplementary Table 5). Future research should, therefore, focus on the public health relevance of multiple toxic hazards shown to co-occur in ASGM (Tables 3 and 4; Supplementary Tables 1–5) (Gottesfeld et al. 2015; Kamunda 2017; Knoblauch et al. 2020; Moyo et al. 2022; Ondayo et al. 2023). Few studies (n = 3 articles) reported communicable diseases, notably malaria, water-borne diseases, tuberculosis, and HIV, amongst other sexually transmitted infections, which are more likely to be prevalent in ASGM given their remote contexts with poor local health systems (Moyo et al. 2022, 2021). Future research should cover associated infections (Moyo et al. 2022, 2021) as these potentially contribute to the systematic health data gap in the ASGM sector at local, national, and regional levels. Furthermore, it leads to insufficient knowledge about the relationship between ASGM activities and the effect of other toxic exposures on human health. Broader international literature shows long-term PTE exposure, chronic disease risks, and spillovers from unmanaged conditions (Allan-Blitz et al. 2022; Landrigan et al. 2022; von Stackelberg et al. 2022; WGC 2022). Mostly in ASGM in Africa, ad hoc surveys reported cancers and other health outcomes amongst ASGM workers, children, and women with no evidence of genetic risks and developmental effects (Supplementary Table 5). Additionally, an evidence gap exists on specific long-term health risks and consequences of each respective toxic hazard, including associated fatality levels in ASGM across Africa.
Gaps in Regional Regulation of ASGM in Africa
The widely informal ASGM sector across Africa operates autonomously without government support (Chupezi et al. 2009), with 70–80% of the sector being illegal (Achina-Obeng and Aram 2022). The remaining 20–30% are legal (Mensah et al. 2022) but often improperly overseen, monitored, and evaluated (Hilson et al. 2018; Keane et al. 2023; World-Bank 2020). For instance, Kenya’s Mining Act of 2016 legalizes ASGM nationwide (Fritz et al. 2018b; GoK 2016) but lacks regulations for health, safety, environmental surveillance, and cost–benefit evaluation of ASGM. Considering the evidence of exposures and health effects (Tables 2–4; Supplementary Tables 1–5) in Africa, preventive measures are needed to reduce and eliminate exposures. In contrast, Africa’s regional ASGM policies and regulations are critical but lacking (Hilson et al. 2018; Keane et al. 2023; World-Bank 2020). Besides, most ASGM workers and communities are unaware of exposure risks and compensation for risks from ASGM. African countries lack updated compensation criteria for ASGM risks and morbidities. For example, the Medical Bureau and Compensation Commission delayed compensating 200,000 and 700,000 eligible ex-miners in South Africa (World-Bank 2015).
Risk Monitoring and Management Measures in ASGM in Africa
Toxic exposures in ASGM lead to significant health burden-related costs, including reduced work performance, intellectual capacity, behavioural and psychosocial loss, and healthcare costs (Table 4; Supplementary Table 5). These are transferred to future generations, negatively impacting individuals, families, societies, and national, regional, and global economies (Landrigan and Fuller 2015). Regional and global multidisciplinary, multi-sector and multi-stakeholder interventions are crucial for combating Africa’s ASGM-related environmental and health risks. Global efforts, including Ramazzini, Minamata Convention, and Intergovernmental Forum on Mining, Minerals, Metals and Sustainable Development (IGF) and Collegium Ramazzini, aim to address these and ensure sustainable development. The Minamata Convention urges governments to promote Hg-free gold processing to protect vulnerable populations (Hilson et al. 2018). The IGF supports sustainable mining in 60 countries with minimal adverse environmental, economic, social, and health impacts (Fritz et al. 2018a; Keane et al. 2023). Collegium Ramazzini promotes environmental and occupational hazard reduction in small-scale artisanal mining (Landrigan et al. 2022). Despite all these global efforts, there is still the need for respective in-country, inter-country, and regional multi-sectoral multi-stakeholder interdisciplinary policies and preventive interventions to minimize and eliminate ASGM-related hazards in Africa. In the future, as a region, this paper recommends the following essential action areas:
Research and Systematic Monitoring
Established gaps in toxic hazards and health effects studies between African and broader literature require investment in scientific research and practice improvement across the continent. This is crucial in ensuring an accurate understanding of the environmental and health burdens and risks of ASGM by researchers, regulators, and policy-makers. Updated literature and data will aid in developing comprehensive policies and interventions. Research should focus on critical areas, notably investigating the migration routes and pathways of occupational and non-occupational exposures in ASGM; toxicological studies, including investigations on multiple exposures, biomonitoring of PTEs, and regular medical checks for known associated risks amongst ASGM workers and community members, especially women and children including foetuses and preventing them from harm. Additionally, implementing surveillance systems for ASGM workers, ex-workers, and communities is crucial for best practices (Keane et al. 2023; Landrigan et al. 2022; von Stackelberg et al. 2022; WHO 2016; Wireko-Gyebi et al. 2022; World-Bank 2020).
Improving and Strengthening Legislation, Regulation, and Policy
Governments should acknowledge and provide appropriate support to ASGM. Developing consistent policies addressing poverty alleviation, sustainable rural development, environmental and health impact reduction, productive business environment, and government revenue stability is crucial. These should be consistent for artisanal, small-scale, and large-scale mechanized gold mining (Fritz et al. 2018a; WGC 2022; WHO 2016; World-Bank 2020). Establishing appropriate in-country and regional transparent, non-discriminatory legal and regulatory frameworks for ASGM workers are crucial whilst improving government enforcement and compliance, such as mandatory PPE use and banning child labour, Hg, and other toxic chemical use in ASGM. Governments should also offer regularization incentives. For instance, tax allowances, equipment exemptions, finance, and export assistance for ASGM enterprises (Fritz et al. 2018a; Keane et al. 2023; WGC 2022; WHO 2016; World-Bank 2020). To fully control the ASGM sector, governments must address ASGM workers’ legal, organisational, technical, health and safety needs, including cooperatives formation, exposure standards, monitoring, coherent administration, and collaboration with NGOs, donors, and industry (WGC 2022; World-Bank 2020).
Technology Development and Improvement
The ASGM sector is widely informal and unorganized with minimum support or intervention from their governments (Chupezi et al. 2009). Regional multi-sectoral and multidisciplinary cooperation is needed for investment, improvement, and adoption of affordable, cleaner, safer, and efficient alternative ASGM techniques (Appel and Jonsson 2010; Aslam et al. 2022; Keane et al. 2023; Mitchell et al. 2021; Steckling et al. 2014a; Stoffersen et al. 2019). This includes research and exploration of affordable, cleaner, and more efficient gold recovery alternatives for Hg and NaCN, like the use of borax and retorts; putting in place engineering and mechanical controls to reduce/eliminate occupational and non-occupational dust exposures; and updated technologies for hazard controls, management of wastes in ASGM, medical surveillance and remediation. Further improvements should include increasing access to geological information, adequate management tools, capacity building, and increasing access to finances and appropriate technologies by ASGM workers (Keane et al. 2023; WGC 2022; Zhuwarara 2023). For instance, collective cash and equipment loan schemes aimed at encouraging the formation of groups and the use of required technology in ASGM have been met with little success in Congo, Kenya, Namibia, Zambia, and South Africa (IGF 2017; PlanetGOLD 2020; WGC 2022).
Risk Reduction and Subsequent Elimination
Investing in adequate and proper management of the identified risks is necessary. The first step is identifying and managing risks at the source (Landrigan et al. 2022). This can, for instance, include eliminating PTEs sources in ASGM by substituting Hg, NaCN, and other toxic chemicals used in gold ore processing with less toxic options such as borax and upgrading ASGM technologies used in most countries by adopting the use of retorts and wet milling machines to reduce dust emissions and Hg losses and safe leaching (Appel and Jonsson 2010; Aslam et al. 2022; Mitchell et al. 2021; Steckling et al. 2014a; Stoffersen et al. 2019). Additionally, addressing the low adoption of safer, cleaner ASGM technologies is critical (Keane et al. 2023). The second step is in identifying and managing hazards and risks along the migration pathways (Landrigan et al. 2022; WHO 2016; World-Bank 2020). For example, eliminating the various migration routes and exposure pathways of PTEs through personal protective equipment, traceable mine waste management, and extensive awareness engagement and education amongst ASGM workers and local communities. Informing miners, ore processors, and the community on ASGM policies, PTEs exposures and health risks are also vital. Governments should implement mitigation measures to prevent adverse impacts on public spaces, schools, hospitals, and markets. For example, by resettling communities, relocating schools, remediating contaminated soils, monitoring, and involving ASGM workers and local communities in risk assessments (Smith et al. 2016). Thirdly, identifying and managing risks in ASGM by improving research practice and enhancing legal procedures are critical. Ensuring compliance with occupational, health and safety guidelines, adherence to the recommended limits for respective PTEs exposures, and systematic monitoring of ASGM workers and local community members have significantly reduced and subsequently eliminated risks in developed countries (Allan-Blitz et al. 2022; Smith et al. 2016; WGC 2022).
Detection, Surveillance, and Management of Health Outcomes in ASGM in Africa
African countries should invest in diagnostic capabilities, training, and early disease screening to manage ASGM health burdens effectively. Enhancing healthcare access for ASGM workers, ex-workers, and communities; enhancing surveillance infrastructure; and regionally coordinated health risk collaborations and data exchanges, including malnutrition, mined gold, and illegal transport and purchase of toxic chemicals, like Hg, amongst others, are critical (Smith et al. 2016; WHO 2016; World-Bank 2020; Zhuwarara 2023).
Limitations and Strengths of the Review
Whilst a substantive body of literature was found in the search, this review had limitations; primarily, literature in English was included. This might under-represent some Lusophone (Angola, Equatorial Guinea, Guinea-Bissau, and Mozambique) and Francophone (Burundi, Djibouti, and Togo) countries. Grey literature, which is not available online, was not incorporated. Studies were of variable quality, sometimes old and concentrated in a few countries where established gold deposits were more likely to have been reported widely. The available data in other studies limited our review. Whereas very few studies provided complete datasets to summarize measures of central tendency adequately, most studies lacked information on the distribution and spread of PTEs concentrations or information on the number of samples and subsamples collected and the median. Few studies provided adequate information on data collection and quality assurance checks to provide research transparency and confidence in the study design and sample analyses. Besides, the lack of standard terms for investigated adverse health conditions, such as symptoms of Hg intoxication and Pb intoxication in included studies (Table 4; Supplementary Table 5), may have caused duplication.
However, this review explores environmental and health research in African ASGM communities, offering insights into practices and literature. Additionally, the scientific evidence found for the African continent was adequate to identify and characterize significant ASGM-related toxic hazards to the environment, human exposures, and health risks and allow for comparison with the broader global evidence.
Conclusion
The review reveals extensive ASGM in 30 African countries. The ASGM sector presents major and complex challenges as it is a significant source of widespread environmental pollution and human exposure to toxic hazards, which have detrimental health effects on the ASGM workers and local community members, including fatalities. Thus, there are no quick solutions, as explained in this review. Essentially, there is a continued need for a collective cost–benefit analysis of ASGM in Africa using DALYs calculation and review of legislation, policies, stringent oversight of ASGM operations in the field, and tangible actions to eliminate environmental degradation and human exposure to toxic hazards in ASGM.
In contrast, the overall disease burden of ASGM in Africa remains unknown. This review petitions for country-specific efforts and properly coordinated collaborative continent-wide efforts amongst all countries where ASGM is practised, the World Health Organization, World Bank, the United Nations agencies (UNEP, UNDP, and UNIDO) and Non-Governmental Organizations, academia, and the private sector to identify, design, and implement sustainable solutions for the ASGM sector in individual countries and regionally. The activities are well-documented measures for identifying, assessing, and managing occupational and non-occupational hazards and risks arising from ASGM at the source, along the migration routes and pathways and at the receiving environments, individual human beings and populations as summarized in this review. Similarly, considering the regional magnitude of ASGM practice in Africa, the number of health-related studies in ASGM appears low, with several specific contexts not adequately represented in the existing literature. For instance, twenty African countries have developed National Action Plans for ASGM, focusing on eliminating Hg use and use of CN to reprocess Hg-contaminated tailings. However, apart from Hg and Hg-CN complexes, other toxic hazards of significant public health importance, notably potentially toxic metals, As, crystalline respirable SiO2 dust exist in ASGM. With concrete holistic actions, addressing the highlighted research and “big data gaps” in ASGM contexts in Africa is possible.
Data availability
Enquiries about data availability should be directed to the authors.
References
Abadin H, Ashizawa A, Llados F, Stevens Y-W (2007) Toxicological profile for lead. https://stacks.cdc.gov/view/cdc/37676/cdc_37676_DS1.pdf
Abdelaal A, Sultan M, Abotalib AZ, Bedair M, Krishnamurthy R, Elhebiry M (2023) Emerging mercury and methylmercury contamination from new artisanal and small-scale gold mining along the Nile Valley, Egypt. Environ Sci Pollut Res 30(18):52514–52534. https://doi.org/10.1016/j.scitotenv.2020.141654
Abebil F, Tefera Y, Tefera W, Kumie A, Mulugeta H, Kassie G (2023) Nonfatal occupational injuries among artisanal and small-scale gold mining workers in Ethiopia. Environ Health Insights 17:11786302231171808. https://doi.org/10.1177/1178630223117
Abeid R, Mergenthaler C, Muzuka V, Goodluck A, Nkwabi T, Bigio J, Vasquez NA, Pande T, Haraka F, Creswell J, Rahman T, Straetemans M (2022) Increasing TB/HIV case notification through an active case-finding approach among rural and mining communities in northwest Tanzania. J Trop Med 2022:1–11. https://doi.org/10.1155/2022/4716151
Abrefah RG, Adotey DK, Ampomah-Amoako E, Opata NS (2011) Biomonitoring of occupational exposure to total arsenic and total mercury in urine of goldmine workers in southwestern Ghana. Environ Res Eng Manag 56(2):43–48
Achina-Obeng R, Aram SA (2022) Informal artisanal and small-scale gold mining (Asgm) in Ghana: assessing environmental impacts, reasons for engagement, and mitigation strategies. Resour Policy 78:102907. https://doi.org/10.1016/j.resourpol.2022.102907
Addai-Arhin S, Novirsa R, Jeong HH, Phan QD, Hirota N, Ishibashi Y, Shiratsuchi H, Arizono K (2022) The human health risks assessment of mercury in soils and plantains from farms in selected artisanal and small-scale gold mining communities around Obuasi, Ghana. J Appl Toxicol 42(2):258–273. https://doi.org/10.1002/jat.4209
Adewumi AJ, Laniyan TA, Xiao T, Liu Y, Ning Z (2019) Exposure of children to heavy metals from artisanal gold mining in Nigeria: evidences from bio-monitoring of hairs and nails. Acta Geochimica. https://doi.org/10.1007/s11631-019-00371-9
Adimado A, Baah D (2002) Mercury in Human blood, urine, hair, nail, and fish from the Ankobra and Tano river basins in southwestern Ghana. Bull Environ Contam Toxicol 68(3):339–346. https://doi.org/10.1007/s00128-001-0259-8
Adounkpe JG, Azon N, Dégila HW, Hounkpe P, Amoussou R (2021) Assessment of the temporal and spatial variation of the mercury content of lake Nokoué in Southern Benin Republic (West Africa). Sci World J. https://doi.org/10.1155/2021/5412785
Afrifa J, Essien-Baidoo S, Ephraim RK, Nkrumah D, Dankyira DO (2017) Reduced Egfr, elevated urine protein and low level of personal protective equipment compliance among artisanal small scale gold miners at Bibiani-Ghana: a cross-sectional study. BMC Public Health 17(1):601. https://doi.org/10.1186/s12889-017-4517-z
Afrifa J, Opoku YK, Gyamerah EO, Ashiagbor G, Sorkpor RD (2019) The clinical importance of the mercury problem in artisanal small-scale gold mining. Front Public Health. https://doi.org/10.3389/fpubh.2019.00131
Agaba EF, Sakimpi DK, Kamese G, Mukasa V, Nkonge D, Ssempebwa JC (2018) Assessment of Occupational, Environment and Other Impacts from Use Of Mercury in Artisanal Small – Scale Gold Mining (ASGM) In Uganda: 2017 – 2018 (Research Paper, Issue). Accessed on June 2022 from https://nape.or.ug/publications/chemical-management/83-assesment-of-environmental-health-occupational-and-other-impacts-of-use-of-mercury-inasgm-sector-in-uganda/file
Ali M, Elhagwa A, Elfaki J, Sulieman M (2017) Influence of the artisanal gold mining on soil contamination with heavy metals: A case study from Dar-Mali locality, North of Atbara, River Nile State. Sudan. Eurasian Journal of Soil Science 6(1):28–36. doi: https://doi.org/10.18393/ejss.284261
Allan-Blitz L-T, Goldfine C, Erickson TB (2022) Environmental and health risks posed to children by artisanal gold mining: a systematic review. SAGE Open Med 10:20503121221076936
Antabe R, Atuoye KN, Kuuire VZ, Sano Y, Arku G, Luginaah I (2017) Community health impacts of surface mining in the upper west region of ghana: the roles of mining odors and dust. Hum Ecol Risk Assess Int J 23(4):798–813. https://doi.org/10.1080/10807039.2017.1285691
Apel P, Angerer J, Wilhelm M, Kolossa-Gehring M (2017) New Hbm values for emerging substances, inventory of reference and Hbm values in force, and working principles of the german human biomonitoring commission. Int J Hyg Environ Health 220(2):152–166. https://doi.org/10.1016/j.ijheh.2016.09.007
Appel P, Jonsson JB (2010) Borax–an alternative to mercury for gold extraction by small-scale miners: introducing the method in Tanzania. Geol Survey Denmark Greenland Bull 20:87–90
Armah EK, Adedeji JA, Boafo BB, Opoku AA (2021) Underground gold miner exposure to noise diesel particulate matter and crystalline silica dust. J Health Pollut. https://doi.org/10.5696/2156-9614-11.29.210301
Arthur-Holmes F (2021) Gendered division of labour and “sympathy” in artisanal and small-scale gold mining in Prestea-Huni valley municipality, Ghana. J Rural Stud 81:358–362. https://doi.org/10.1016/j.jrurstud.2020.11.001
Asante KA, Agusa T, Subramanian A, Ansa-Asare OD, Biney CA, Tanabe S (2007) Contamination status of arsenic and other trace elements in drinking water and residents from Tarkwa, a historic mining township in Ghana. Chemosphere 66(8):1513–1522. https://doi.org/10.1016/j.chemosphere.2006.08.022
Aslam IN, Orcon N, Klein B, Alam PN (2022) Optimizing gold recovery of artisanal mining: a lesson learned from Kenya. J. Rekayasa Kim. Lingkung. 17(1):9. https://doi.org/10.23955/rkl.v17i1.23223
Astolfi ML, Protano C, Marconi E, Massimi L, Piamonti D, Brunori M, Vitali M, Canepari S (2020) Biomonitoring of mercury in hair among a group of eritreans (Africa). Int J Environ Res Public Health 17(6):1911. https://doi.org/10.3390/ijerph17061911
Axelrad DA, Coffman E, Kirrane EF, Klemick H (2022) The relationship between childhood blood lead levels below 5 µg/Dl and childhood intelligence quotient (Iq): protocol for a systematic review and meta-analysis. Environ Int 169:107475. https://doi.org/10.1016/j.envint.2022.107475
Babut M, Sekyi R, Rambaud A, Potin-Gautier M, Tellier S, Bannerman W, Beinhoff C (2003) Improving the environmental management of small-scale gold mining in ghana: a case study of Dumasi. J Clean Prod 11(2):215–221. https://doi.org/10.1016/S0959-6526(02)00042-2
Bakia M (2014) East cameroon’s artisanal and small-scale mining bonanza: how long will it last? Futures 62:40–50. https://doi.org/10.1016/j.futures.2013.10.022
Barasa B, Kakembo V, Karl T (2016) Characterization of artisanal gold mining activities in the tropics and their impact on sediment loading and stream flow in the okame river catchment, Eastern Uganda. Environ Earth Sci 75(14):1076. https://doi.org/10.1007/s12665-016-5876-y
Basu N, Nam D-H, Kwansaa-Ansah E, Renne EP, Nriagu JO (2011) Multiple metals exposure in a small-scale artisanal gold mining community. Environ Res 111(3):463–467. https://doi.org/10.1016/j.envres.2011.02.006
Basu N, Clarke E, Green A, Calys-Tagoe B, Chan L, Dzodzomenyo M, Fobil J, Long RN, Neitzel RL, Obiri S (2015) Integrated assessment of artisanal and small-scale gold mining in Ghana—part 1: human health review. Int J Environ Res Public Health 12(5):5143–5176. https://doi.org/10.3390/ijerph120505143
Bitala MF, Kweyunga C, Manoko M (2009) Levels of heavy metals and cyanide in soil, sediment and water from the vicinity of North Mara Gold Mine in Tarime District, Tanzania: A report presented to the Christian Council of Tanzania, Dodoma. https://www.olca.cl/oca/tanzania/north_mara_pollution_report.pdf
Black P, Richard M, Rossin R, Telmer K (2017) Assessing occupational mercury exposures and behaviours of artisanal and small-scale gold miners in Burkina Faso using passive mercury vapour badges. Environ Res 152:462–469. https://doi.org/10.1016/j.envres.2016.06.004
Bose-O’Reilly S, Lettmeier B, Cao TL, Siebert U, Tesha A, Pronczuk J, Beinhoff C, Drasch G (2007) Health and environmental training in mercury-contaminated areas. Int J Environ Health 1(4):621–637. https://doi.org/10.1504/IJENVH.2007.018580
Bose-O’Reilly S, Lettmeier B, Gothe RM, Beinhoff C, Siebert U, Drasch G (2008a) Mercury as a serious health hazard for children in gold mining areas. Environ Res 107(1):89–97. https://doi.org/10.1016/j.envres.2008.01.009
Bose-O’Reilly S, Lettmeier B, Roider G, Siebert U, Drasch G (2008b) Mercury in breast milk–a health hazard for infants in gold mining areas? Int J Hyg Environ Health 211(5–6):615–623. https://doi.org/10.1016/j.ijheh.2007.09.015
Bose-O’Reilly S, Drasch G, Beinhoff C, Tesha A, Drasch K, Roider G, Taylor H, Appleton D, Siebert U (2010) Health assessment of artisanal gold miners in Tanzania. Sci Total Environ 408(4):796–805. https://doi.org/10.1016/j.scitotenv.2009.10.051
Bose-O’Reilly S, Bernaudat L, Siebert U, Roider G, Nowak D, Drasch G (2017) Signs and symptoms of mercury-exposed gold miners. Int J Occup Med Environ Health 30(2):249–269. https://doi.org/10.13075/ijomeh.1896.00715
Bose-O’Reilly S, Lettmeier B, Shoko D, Roider G, Drasch G, Siebert U (2020) Infants and mothers levels of mercury in breast milk, urine and hair, data from an artisanal and small-scale gold mining area in Kadoma/Zimbabwe. Environ Res 184:109266. https://doi.org/10.1016/j.envres.2020.109266
Bråtveit M, Moen BE, Mashalla YJ, Maalim H (2003) Dust exposure during small-scale mining in Tanzania: a pilot study. Ann Occup Hyg 47(3):235–240. https://doi.org/10.1093/annhyg/meg027
Bugmann A, Brugger F, Zongo T, van der Merwe A (2022) “Doing Asgm without mercury is like trying to make omelets without eggs”. understanding the persistence of mercury use among artisanal gold miners in Burkina Faso. Environ Sci Policy 133:87–97. https://doi.org/10.1016/j.envsci.2022.03.009
Carneiro A, Teixeira VdS, Silveira A, Araújo S, Algranti E (2022) Non-malignant silica-related diseases in a specialized outpatient clinic. Occup Med 72(6):394–402. https://doi.org/10.1093/occmed/kqac034
Černá M, Puklová V, Hanzlíková L, Sochorová L, Kubínová R (2017) 25 years of Hbm in the Czech Republic. Int J Hyg Environ Health 220(2):3–5. https://doi.org/10.1016/j.ijheh.2016.08.004
Chetty S, Pillay L, Humphries MS (2021) Gold mining’s toxic legacy: pollutant transport and accumulation in the Klip River catchment, Johannesburg. S Afr J Sci 117(7–8):1–11. https://doi.org/10.17159/sajs.2021/8668
Chou C-H, Harper C (2007) Toxicological profile for arsenic. agency for toxic substances & disease registry. https://www.atsdr.cdc.gov/toxprofiles/tp2-p.pdf
Chupezi TJ, Ingram V, Schure J (2009) Study on impacts of artisanal gold and diamond mining on livelihoods and the environment in the Sagha Tri-National Park (TNS) landscape, Congo Basin. Yaounde. https://pure.uva.nl/ws/files/893516/78180_ingram02.pdf
Clarkson TW, Nordberg GF, Sager PR (1985) Reproductive and developmental toxicity of metals. Scand J Work Environ Health 11:145–154. https://doi.org/10.5271/sjweh.2239
Clifford MJ (2017) The extractive industries and society assessing releases of mercury from small-scale gold mining sites in Ghana. Extractive Ind Soc. https://doi.org/10.1016/j.exis.2017.05.007
Cobbina SJ, Dagben JZ, Obiri S, Tom-Dery D (2011) Assessment of non-cancerous health risk from exposure to Hg, as and Cd by resident children and adults in Nangodi in the upper east region, Ghana. Water Qual Exposure Health 3(3–4):225–232. https://doi.org/10.1007/s12403-012-0059-x
Cobbina SJ, Nkuah D, Tom-Dery D, Obiri S (2013) Noncancer risk assessment from exposure to mercury (Hg), cadmium (Cd), arsenic (as), copper (Cu) and lead (Pb) in boreholes and surface water in Tinga, in the Bole-Bamboi district. J Toxicol Environ Health Sci 5(2):29–36. https://doi.org/10.5897/JTEHS12.0253
Control CfD, Prevention (2015) Fourth national report on human exposure to environmental chemicals, updated tables, February 2015. Atlanta: US Department of Health and Human Services, pp. 91–105. https://stacks.cdc.gov/view/cdc/75822
Dooyema CA, Neri A, Lo Y-C, Durant J, Dargan PI, Swarthout T (2012a) Outbreak of fatal childhood lead poisoning related to artisanal gold. Environ Health Perspect 120(4):601–607
Dooyema CA, Neri A, Lo Y-C, Durant J, Dargan PI, Swarthout T, Biya O, Gidado SO, Haladu S, Sani-Gwarzo N (2012b) Outbreak of fatal childhood lead poisoning related to artisanal gold mining in northwestern Nigeria. Environ Health Perspect 120(4):601–607. https://doi.org/10.1289/ehp.1103965
Doyi I, Essumang D, Nyarku M, Gbeddy G, Ackah M (2016) Multielemental analysis of gold ore samples from underground artisanal gold mines in tongo, upper east region of Ghana: implications of occupational exposure. J Environ Anal Toxicol 6(350):2161–0525.1000350. https://doi.org/10.4172/2161-0525.1000350
Duker AA, Stein A, Hale M (2006) A statistical model for spatial patterns of buruli ulcer in the Amansie west district, Ghana. Int J Appl Earth Obs Geoinf 8(2):126–136. https://doi.org/10.1016/j.jag.2005.06.013
Duncan AE (2020) The dangerous couple: illegal mining and water pollution—a case study in Fena River in the Ashanti region of Ghana. J Chem 2020:1–9. https://doi.org/10.1155/2020/2378560
Ebongue AN, Njock MK (2018) Assessment of natural radioactivity levels and the associated radiological hazards in some building materials from Mayo-Kebbi region. Chad. https://doi.org/10.1051/radiopro/2018030
ELAW (2010) Guidebook for evaluating mining project eias: overview of mining and its impacts. environmental law alliance worldwide. https://www.elaw.org/files/mining-eia-guidebook/Chapter1.pdf
Fashola MO, Ngole-Jeme VM, Babalola OO (2016) Heavy metal pollution from gold mines: environmental effects and bacterial strategies for resistance. Int J Environ Res Public Health 13(11):1047. https://doi.org/10.3390/ijerph13111047
Fritz M, McQuilken J, Collins N, Weldegiorgis F (2018a) Global trends in artisanal and small-scale mining (Asm): a review of key numbers and issues. Hal Working Papers (Hal-02547257). https://www.iisd.org/system/files/publications/igf-asm-global-trends.pdf
Fritz MM, McQuilken J, Collins N, Weldegiorgis F (2018b) Global trends in artisanal and small-scale mining (Asm): a review of key numbers and issues. HAL Working Papers (Hal-02547257).
Gerson JR, Driscoll CT, Hsu-Kim H, Bernhardt ES (2018) Senegalese artisanal gold mining leads to elevated total mercury and methylmercury concentrations in soils, sediments, and rivers. Elem Sci Anth. https://doi.org/10.1525/elementa.274
Getaneh W, Alemayehu T (2006) Metal contamination of the environment by placer and primary gold mining in the adola region of Southern Ethiopia. Environ Geol 50(3):339–352. https://doi.org/10.1007/s00254-006-0213-5
Gibb H, O’Leary KG (2014) Mercury exposure and health impacts among Individuals in the artisanal and small-scale gold mining community: a comprehensive review. Environ Health Perspect 122(7):667–672. https://doi.org/10.1289/ehp.1307864
Godebo TR, Paul CJ, Jeuland MA, Tekle-Haimanot R (2019) Biomonitoring of metals and trace elements in urine of central ethiopian populations. Int J Hyg Environ Health 222(3):410–418. https://doi.org/10.1016/j.ijheh.2018.12.007
GoK (2016) Mining act, no. 12 of 2016, laws of Kenya. http://kenyalaw.org/kl/fileadmin/pdfdownloads/Acts/MiningAct_No12of2016.pdf
Gonçalves JF, Dressler VL, Assmann CE, Morsch VMM, Schetinger MRC (2021) Cadmium neurotoxicity: from its analytical aspects to neuronal impairment. Advances in neurotoxicology, vol 5. Elsevier, pp 81–113
Gonick HC (2008) Nephrotoxicity of cadmium & lead. Indian J Med Res 128(4):335–352
Gottesfeld P, Andrew D, Dalhoff J (2015) Silica exposures in artisanal small-scale gold mining in tanzania and implications for tuberculosis prevention. J Occup Environ Hyg 12(9):647–653. https://doi.org/10.1080/15459624.2015.1029617
Gottesfeld P, Meltzer G, Costello S, Greig J, Thurtle N, Bil K, Mwangombe BJ, Nota MM (2019) Declining blood lead levels among small-scale miners participating in a safer mining pilot programme in Nigeria. Occup Environ Med 76(11):849–853. https://doi.org/10.1136/oemed-2019-105830
Goutam Mukherjee A, Ramesh Wanjari U, Renu K, Vellingiri B, Valsala Gopalakrishnan A (2022) Heavy metal and metalloid—induced reproductive toxicity. Environ Toxicol Pharmacol 92:103859. https://doi.org/10.1016/j.etap.2022.103859
Green CS, Lewis PJ, Wozniak JR, Drevnick PE, Thies ML (2019) A comparison of factors affecting the small-scale distribution of mercury from artisanal small-scale gold mining in a Zimbabwean stream system. Science of the Total Environment 647:400–410. https://doi.org/10.1016/j.scitotenv.2018.07.418
Gyamfi O, Sorenson PB, Darko G, Ansah E, Bak JL (2020) Human health risk assessment of exposure to indoor mercury vapour in a ghanaian artisanal small-scale gold mining community. Chemosphere 241:125014. https://doi.org/10.1016/j.chemosphere.2019.125014
Gyamfi O, Sørensen PB, Darko G, Ansah E, Vorkamp K, Bak JL (2021) Contamination, exposure and risk assessment of mercury in the soils of an artisanal gold mining community in Ghana. Chemosphere 267:128910. https://doi.org/10.1016/j.chemosphere.2020.128910
Hagos G, Sisay W, Alem Z, Niguse G, Mekonen A (2016) Participation on traditional gold mining and its impact on natural resources, the case of Asgede Tsimbla, Tigray, Northern Ethiopia. J Earth Sci Geotech Eng 6(1):89–97
Haidula AF, Ellmies R, Kayumba F (2011) Environmental monitoring of small-scale mining areas in Rwanda. https://docs.igihe.com/IMG/pdf/rwanda_environment_asm_report_2011-09-20x.pdf
Haines DA, Saravanabhavan G, Werry K, Khoury C (2017) An overview of human biomonitoring of environmental chemicals in the canadian health measures survey: 2007–2019. Int J Hyg Environ Health 220(2):13–28. https://doi.org/10.1016/j.ijheh.2016.08.002
Harada M, Nakachi S, Cheu T, Hamada H, Ono Y, Tsuda T, Yanagida K, Kizaki T, Ohno H (1999) Monitoring of mercury pollution in Tanzania: relation between head hair mercury and health. Sci Total Environ 227(2–3):249–256. https://doi.org/10.1016/S0048-9697(99)00031-5
Hays SM, Nordberg M, Yager JW, Aylward LL (2008) Biomonitoring equivalents (Be) dossier for cadmium (Cd)(Cas No 7440-43-9). Regulat Toxicol Pharmacol 51(3):S49–S56. https://doi.org/10.1016/j.yrtph.2008.05.008
Hays SM, Aylward LL, Gagné M, Nong A, Krishnan K (2010) Biomonitoring equivalents for inorganic arsenic. Regul Toxicol Pharmacol 58(1):1–9. https://doi.org/10.1016/j.yrtph.2010.06.002
Hilson G, Monhemius A (2006) Alternatives to cyanide in the gold mining industry: what prospects for the future? J Clean Prod 14(12–13):1158–1167. https://doi.org/10.1016/j.jclepro.2004.09.005
Hilson G, Zolnikov TR, Ortiz DR, Kumah C (2018) Formalizing artisanal gold mining under the minamata convention: previewing the challenge in sub-saharan Africa. Environ Sci Policy 85:123–131. https://doi.org/10.1016/j.envsci.2018.03.026
Hinton J, Veiga MM, Beinhoff C (2003) Women and artisanal mining: gender roles and the road ahead: the socio-economic impacts of artisanal and small-scale mining in developing countries, pp. 149–188. https://prod-edxapp.edx-cdn.org/assets/courseware/v1/6913dd84795c217cc1c8c05358d8e782/asset-v1:SDGAcademyX+NR001+2T2019+type@asset+block/Women_and_artisanal_mining_-_gender_roles_and_the_road_ahead.pdf
Hoy RF, Jeebhay MF, Cavalin C, Chen W, Cohen RA, Fireman E, Go LH, León-Jiménez A, Menéndez-Navarro A, Ribeiro M (2022) Current global perspectives on silicosis—convergence of old and newly emergent hazards. Respirology 27(6):387–398. https://doi.org/10.1111/resp.14242
IARC (2021) Agents classified by the IARC monographs, vol 1–133. International Agency for Research on Cancer. World Health Organization. https://monographs.iarc.who.int/agents-classified-by-the-iarc/
Idris IM, Younis YME, Elbeshir AM (2018a) Assessment of drinking water quality status of butana mining sites, eastern sudan via determination of physicochemical parameters and heavy metal concentration levels (I). https://www.eijst.org.uk/images/frontImages/articles/Vol.7No.1/1.Drinking_Water_Quality_Status_of_Butana_Mining_Sites.pdf
Idris IM, Younis YME, Elbashir AA (2018b) Monitoring the anthropogenic and geochemical environment surrounding the butana drinking water sources via the determination of heavy metals composition of the soil, streams sediments and gold mining tailings (Ii). https://www.eijst.org.uk/images/frontImages/articles/Vol.7No.3/6.51-64.pdf
IGF (2017) Igf Guidance for government managing artisanal and small-scale mining: the international institute for sustainable development. https://www.iisd.org/system/files/publications/igf-guidance-for-governments-asm_0.pdf
Ikingura JR, Akagi H (1996) Monitoring of fish and human exposure to mercury due to gold mining in the lake victoria goldfields. Tanzania Sci Total Environ 191(1–2):59–68. https://doi.org/10.1016/0048-9697(96)05178-9
Ismawati Y (2016) Children’s exposures to mercury in artisanal and small-scale gold mining areas in indonesia and in more than 70 countries. (August), pp. 1–7. https://www.ohchr.org/sites/default/files/Documents/HRBodies/CRC/Discussions/2016/YuyunIsmawati.pdf
Isom GE, Borowitz JL (2015) Biochemical mechanisms of cyanide toxicity. Toxicology of cyanides and cyanogens: experimental, applied and clinical aspects. Wiley, pp 70–81
Jennings N (1999) Social and labour issues in small-scale mines: report for discussion at the tripartite meeting on social and labour issues in small-scale mines. Geneva: International Labour Organization. https://www.ilo.org/wcmsp5/groups/public/---ed_dialogue/---sector/documents/meetingdocument/wcms_714371.pdf
Kamunda C, Mathuthu M, Madhuku M (2016) Health risk assessment of heavy metals in soils from witwatersrand gold mining basin, South Africa. Int J Environ Res Public Health 13(7):663. https://doi.org/10.3390/ijerph13070663
Kamunda C (2017) Human health risk assessment of environmental radionuclides and heavy metals around a gold mining area in Gauteng Province, South Africa. North-West University (South Africa) Mafikeng Campus. https://repository.nwu.ac.za/bitstream/handle/10394/25382/Kamunda_C.pdf?sequence=1&isAllowed=y
Kaninga BK, Chishala BH, Maseka KK, Sakala GM, Lark MR, Tye A, Watts MJ (2019) Mine tailings in an African tropical environment—mechanisms for the bioavailability of heavy metals in soils. Environ Geochem Health. https://doi.org/10.1007/s10653-019-00326-2
Keane S, Bernaudat L, Davis KJ, Stylo M, Mutemeri N, Singo P, Twala P, Mutemeri I, Nakafeero A, Etui ID (2023) Mercury and artisanal and small-scale gold mining: review of global use estimates and considerations for promoting mercury-free alternatives. Ambio 52(5):833–852. https://doi.org/10.1007/s13280-023-01843-2
Keita MM, Ogendi GM, Owuor O, Nyamao WN (2018) Impacts of artisanal gold mining on water quality: a case study of Tangandougou Commune in Sikasso Region. Mali J Environ Health Sustain Dev. https://doi.org/10.18502/jehsd.v3i4.228
Khafouri A, Talbi EH, Abdelouas A (2021) Assessment of heavy metal contamination of the environment in the mining site of Ouixane (North East Morocco). Water Air Soil Pollut 232:1–27. https://doi.org/10.4172/2381-8719.1000237
Kirman C, Belknap A, Webster A, Hays S (2018) Biomonitoring equivalents for cyanide. Regul Toxicol Pharmacol 97:71–81. https://doi.org/10.1016/j.yrtph.2018.06.006
Klubi E, Abril JM, Mantero J, García-Tenorio R, Nyarko E (2020) Environmental radioactivity and trace metals in surficial sediments from estuarine systems in Ghana (equatorial Africa), impacted by artisanal gold-mining. J Environ Radioact 218:106260. https://doi.org/10.1016/j.jenvrad.2020.106260
Knoblauch AM, Farnham A, Ouoba J, Zanetti J, Müller S, Jean-Richard V, Utzinger J, Wehrli B, Brugger F, Diagbouga S (2020) Potential health effects of cyanide use in artisanal and small-scale gold mining in Burkina Faso. J Clean Prod 252:119689. https://doi.org/10.1016/j.jclepro.2019.119689
Kortei NK, Heymann ME, Essuman EK, Kpodo FM, Akonor PT, Lokpo SY, Boadi NO, Ayim-Akonor M, Tettey C (2020) Health risk assessment and levels of toxic metals in fishes (Oreochromis Noliticus and Clarias Anguillaris) from Ankobrah and Pra Basins: impact of illegal mining activities on food safety. Toxicol Rep 7:360–369. https://doi.org/10.1016/j.toxrep.2020.02.011
Kpan J, Opoku B, Gloria A (2014) Heavy Metal Pollution in Soil and Water in Some Selected Towns in Dunkwa-on-Offin District in the Central Region of Ghana as a Result of Small Scale Gold Mining. Journal of Agricultural Chemistry and Environment 3:40–47. https://doi.org/10.4236/jacen.2014.32006
Kristensen BKA, Thomsen F, Mikkelsen S (2014) A review of mercury exposure among artisanal small-scale gold miners in developing countries. Int Arch Occup Environ Health 87(6):579–590. https://doi.org/10.1007/s00420-013-0902-9
Kwaansa-Ansah E, Basu N, Nriagu J (2010) Environmental and occupational exposures to mercury among indigenous people in Dunkwa-on-Offin, a small scale gold mining area in the south-west of Ghana. Bull Environ Contam Toxicol 85(5):476–480. https://doi.org/10.1007/s00128-010-0141-7
Kwaansa-Ansah EE, Armah EK, Opoku F (2019) Assessment of total mercury in hair, urine and fingernails of small-scale gold miners in the Amansie west district, Ghana. J Health Pollut 9(21):190306. https://doi.org/10.5696/2156-9614-9.21.190306
Laker MC (2023) Environmental impacts of gold mining—with special reference to South Africa. Mining 3(2):205–220. https://doi.org/10.3390/mining3020012
Landrigan PJ, Fuller R (2015) Global health and environmental pollution. Int J Public Health 60(7):761–762. https://doi.org/10.1007/s00038-015-0706-7
Landrigan P, Bose-O’Reilly S, Elbel J, Nordberg G, Lucchini R, Bartrem C, Grandjean P, Mergler D, Moyo D, Nemery B (2022) Reducing disease and death from artisanal and small-scale mining (Asm)-the urgent need for responsible mining in the context of growing global demand for minerals and metals for climate change mitigation. Environ Health 21(1):78. https://doi.org/10.1186/s12940-022-00877-5
Lassen C, Maag J, Jønsson J, Sarunday C (2016) Country reports on mercury trade and use for artisanal and small-scale gold mining: appendix to the report “mercury trade and use for artisanal and small-scale gold mining in sub-saharan Africa” draft final report World Bank, Washington, DC. https://www.unep.org/globalmercurypartnership/resources/report/mercury-trade-and-use-artisanal-and-small-scale-gold-mining-sub-saharan-africa
Lusilao-Makiese J, Cukrowska E, Tessier E, Amouroux D, Weiersbye I (2013) The impact of post gold mining on mercury pollution in the West Rand region, Gauteng, South Africa. Journal of Geochemical Exploration 134:111–119. https://doi.org/10.1016/j.gexplo.2013.08.010
Macdonald KF, Lund MA, Blanchette ML, Mccullough CD (2014) Regulation of artisanal small scale gold mining (Asgm) in Ghana and Indonesia as currently implemented fails to adequately protect aquatic ecosystems. https://ro.ecu.edu.au/cgi/viewcontent.cgi?referer=https://scholar.google.com/&httpsredir=1&article=1864&context=ecuworkspost2013
Magodi R (2017) Assessment and management of environmental and socio-economic impacts of small-scale gold mining at Giyani greenstone belt. Dissertation—Magodi, r.-.pdf (univen.ac.za). Accessed 6 July 2023.
Mallo SJ (2012) Mitigating the activities of artisanal and small-scale miners in Africa: challenges for engineering and technological institutions. Int J Modern Eng Res 2(6):4714–4725
Mambrey V, Rakete S, Tobollik M, Shoko D, Moyo D, Schutzmeier P, Steckling-Muschack N, Muteti-Fana S, Bose-O’Reilly S (2020) Artisanal and small-scale gold mining: a cross-sectional assessment of occupational mercury exposure and exposure risk factors in Kadoma and Shurugwi, Zimbabwe. Environ Res 184:109379. https://doi.org/10.1016/j.envres.2020.109379
Markowitz GS, Radhakrishnan J, Kambham N, Valeri AM, Hines WH, Dagati VD (2000) Lithium nephrotoxicity: a progressive combined glomerular and tubulointerstitial nephropathy. J Am Soc Nephrol 11(8):1439–1448. https://doi.org/10.1681/asn.V1181439
Marriott A, Osano O, Coffey T, Humphrey O, Ongore C, Watts M, Aura C (2023) Considerations for environmental biogeochemistry and food security for aquaculture around lake Victoria, Kenya. Environ Geochem Health 2:1–26. https://doi.org/10.1007/s10653-023-01585-w
Mbuya AW, Mboya IB, Semvua HH et al (2023) Prevalence and factors associated with tuberculosis among the mining communities in Mererani, Tanzania. PLoS ONE 18(3):e0280396. https://doi.org/10.1371/journal.pone.0280396
Meck M, Love D, Mapani B (2006) Zimbabwean mine dumps and their impacts on river water quality—a reconnaissance study. Phys Chem Earth, Parts a/b/c 31(15–16):797–803. https://doi.org/10.1016/j.pce.2006.08.029
Mengistu HA, Demlie MB, Abiye TA, Xu Y, Kanyerere T (2019) Conceptual hydrogeological and numerical groundwater flow modelling around the Moab Khutsong deep gold mine, South Africa. Groundwater Sustain Dev 9:100266. https://doi.org/10.1016/j.gsd.2019.100266
Mensah EK, Afari E, Wurapa F, Sackey S, Quainoo A, Kenu E, Nyarko KM (2016) Exposure of small-scale gold miners in Prestea to Mercury, Ghana, 2012. Pan Afr Med J 25:12. https://doi.org/10.11604/pamj.supp.2016.25.1.6171
Mensah AK, Marschner B, Shaheen SM, Wang J, Wang S-L, Rinklebe J (2020) Arsenic contamination in abandoned and active gold mine spoils in ghana: geochemical fractionation, speciation, and assessment of the potential human health risk. Environ Pollut 261:114116. https://doi.org/10.1016/j.envpol.2020.114116
Mensah SK, Siabi EK, Donkor P, Kurantin N (2022) Assessing the safety and health practices in the artisanal and small-scale gold mining sector of ghana: a case of Ntotroso. Environ Challenges 6:100443. https://doi.org/10.1016/j.envc.2022.100443
Minamata Convention (2021a) Minamata covention on mercury. https://mercuryconvention.org/en/parties. Accessed 10 Jan 2023
Minamata-Convention-on-mercury guidance document on the management of artisanal and small scale gold mining tailings. In: Conference of the parties to the minamata convention on mercury fourth meeting, Online, 1–5 Nov 2021 (2021b). Minamata Covention on Mercury. https://mercuryconvention.org/sites/default/files/documents/information_document/4_INF6_ASGM_Guidance.English.docx
Mitchell C, Bide T, Odhiambo C (2021) Recovering lost gold with improved efficiency, productivity and environmental impacts in Kenya. https://delvedatabase.org/resources/recovering-lost-gold-with-improved-efficiency-productivity-and-environmental-impacts-in-kenya
Mitra S, Chakraborty AJ, Tareq AM, Emran TB, Nainu F, Khusro A, Idris AM, Khandaker MU, Osman H, Alhumaydhi FA (2022) Impact of heavy metals on the environment and human health: novel therapeutic insights to counter the toxicity. J King Saud Univ Sci 34:101865. https://doi.org/10.1016/j.jksus.2022.101865
Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D, Antes G, Atkins D, Barbour V, Barrowman N, Berlin JA (2009) Preferred reporting items for systematic reviews and meta-analyses: the prisma statement (Chinese edition). J Chinese Integr Med 7(9):889–896. https://doi.org/10.7326/0003-4819-151-4-200908180-00135
Moyo D, Zishiri C, Ncube R, Madziva G, Sandy C, Mhene R, Siziba N, Kavenga F, Moyo F, Muzvidziwa O (2021) Tuberculosis and silicosis burden in artisanal and small-scale gold miners in a large occupational health outreach programme in Zimbabwe. Int J Environ Res Public Health 18(21):11031. https://doi.org/10.3390/ijerph182111031
Moyo D, Ncube R, Kavenga F, Chikwava L, Mapuranga T, Chiboyiwa N, Chimunhu C, Mudzingwa F, Muzvidziwa O, Ncube P (2022) The triple burden of tuberculosis, human immunodeficiency virus and silicosis among artisanal and small-scale miners in Zimbabwe. Int J Environ Res Public Health 19(21):13822. https://doi.org/10.3390/ijerph192113822
Mtetwa C, Shava S (2003) A sociological survey of small-scale artisanal gold mining in the Kadoma-Chakari area. Report to the United Nations Industrial Development Organization, Vienna. https://www.researchgate.net/publication/237390281_Sociological_survey_of_small-scale_artisanal_gold_mining_in_the_Kadoma-Chakari_area. Accessed 6 July 2023
Naicker K, Cukrowska E, McCarthy T (2003) Acid mine drainage arising from gold mining activity in Johannesburg, South Africa and environs. Environ Pollut 122(1):29–40. https://doi.org/10.1016/S0269-7491(02)00281-6
Nakaona L, Maseka KK, Hamilton EM, Watts MJ (2019) Using human hair and nails as biomarkers to assess exposure of potentially harmful elements to populations living near mine waste dumps. Environ Geochem Health 42:1197–1209. https://doi.org/10.1007/s10653-019-00376-6
Nemery B (1990) Metal toxicity and the respiratory tract. Eur Respir J 3(2):202–219. https://doi.org/10.1183/09031936.93.03020202
Netshitungulwana R (2011) An investigation of the trace element compositions of gold from Zimbabwe and South Africa: implications for tracing the source of archeological gold artefacts. University of the Free State. https://scholar.ufs.ac.za/handle/11660/6145. Accessed 6 July 2023
Ngole-Jeme VM, Fantke P (2017) Ecological and human health risks associated with abandoned gold mine tailings contaminated soil. PLoS ONE 12(2):e0172517. https://doi.org/10.1371/journal.pone.0172517
Ngure V, Davies T, Kinuthia G, Sitati N, Shisia S, Oyoo-Okoth E (2014) Concentration levels of potentially harmful elements from gold mining in Lake Victoria region, Kenya: environmental and health implications. J Geochem Explor 144:511–516. https://doi.org/10.1016/j.gexplo.2014.04.004
Niane B, Guédron S, Moritz R, Cosio C, Ngom PM, Deverajan N, Pfeifer HR, Poté J (2015) Human exposure to mercury in artisanal small-scale gold mining areas of Kedougou region, senegal, as a function of occupational activity and fish consumption. Environ Sci Pollut Res 22(9):7101–7111. https://doi.org/10.1007/s11356-014-3913-5
Nikolopoulou D, Ntzani E, Kyriakopoulou K, Anagnostopoulos C, Machera K (2023) Priorities and challenges in methodology for human health risk assessment from combined exposure to multiple chemicals. Toxics 11(5):401
Nsambu M, Musibono E, Mputu K (2020) Contribution to the evaluation of the level of mercury pollution of the soils of gold mining sites in the territory of fizi, eastern of democratic Republic of Congo. J Mater Environ Sci 11(1):85–100
Nyanza EC, Dewey D, Thomas DSK, Davey M, Ngallaba S (2014a) Spatial distribution of mercury and arsenic levels in water, soil and cassava plants in a community with long history of gold mining in Tanzania. Bull Environ Contam Toxicol 93(6):716–721. https://doi.org/10.1007/s00128-014-1315-5
Nyanza EC, Joseph M, Premji SS, Thomas DS, Mannion C (2014b) Geophagy practices and the content of chemical elements in the soil eaten by pregnant women in artisanal and small scale gold mining communities in Tanzania. BioMedCentral Pregnancy Childbirth 14(1):144. https://doi.org/10.1186/1471-2393-14-144
Nyanza EC, Bernier FP, Manyama M, Hatfield J, Martin JW, Dewey D (2019) Maternal exposure to arsenic and mercury in small-scale gold mining areas of northern Tanzania. Environ Res 173:432–442. https://doi.org/10.1016/j.envres.2019.03.031
Obiri S, Dodoo D, Okai-Sam F, Essumang D (2006) Non-cancer health risk assessment from exposure to cyanide by resident adults from the mining operations of bogoso gold limited in Ghana. Environ Monit Assess 118(1–3):51. https://doi.org/10.1007/s10661-006-0773-6
Odukoya AM, Uruowhe B, Watts MJ, Hamilton EM, Marriott AL, Alo B, Anene NC (2022) Assessment of bioaccessibility and health risk of mercury within soil of artisanal gold mine sites, Niger, north-central part of Nigeria. Environ Geochem Health 44(3):893–909. https://doi.org/10.1007/s10653-021-00991-2
Odumo O, Mustapha A, Patel J, Angeyo H (2011) Multielemental analysis of Migori (Southwest, Kenya) artisanal gold mine ores and sediments by Edx-ray fluorescence technique: implications of occupational exposure and environmental impact. Bull Environ Contam Toxicol 86:484–489. https://doi.org/10.1007/s00128-011-0242-y
Odumo B, Antonio J, Martin R, Carbonell G (2014) Impact of gold mining associated with mercury contamination in soil biota sediments and tailings in Kenya. Environ Sci Pollut Res 21:12426–12435. https://doi.org/10.1007/s11356-014-3190-3
Odumo BO, Nanos N, Carbonell G, Torrijos M, Patel JP, Rodríguez Martín JA (2018) Artisanal gold-mining in a rural environment: land degradation in Kenya. Land Degrad Dev 29(10):3285–3293. https://doi.org/10.1002/ldr.3078
Ogola JS, Mitullah WV, Omulo MA (2002) Impact of gold mining on the environment and human health: a case study in the migori gold belt, Kenya. Environ Geochem Health 24(2):141–157. https://doi.org/10.1023/A:1014207832471
Ohene S-A, Bonsu F, Adusi-Poku Y, Dzata F, Bakker M (2021) Case finding of tuberculosis among mining communities in Ghana. PLoS ONE. https://doi.org/10.1371/journal.pone.0248718
Olujimi OO, Oputu O, Fatoki O, Opatoyinbo OE, Aroyewun OA, Baruani J (2015) Heavy metals speciation and human health risk assessment at an illegal gold mining site in Igun, Osun State, Nigeria. J Health Pollut 5(8):19–32. https://doi.org/10.5696/i2156-9614-5-8.19
Omara T, Karungi S, Kalukusu R, Nakabuye B, Kagoya S, Musau B (2019a) Mercuric pollution of surface water, superficial sediments, Nile Tilapia (Oreochromis Nilotica Linnaeus 1758 [Cichlidae]) and Yams (Dioscorea Alata) in Auriferous areas of Namukombe stream, Syanyonja, Busia. Uganda Peerj 7:e7919. https://doi.org/10.7717/peerj.7919
Omara T, Karungi S, Ssebulime S, Kiplagat KM, Bongomin O, Ogwang R, Akaganyira S (2019b) Artisanal and small-scale gold mining in syanyonja, busia gold district, South Eastern Uganda: impacts on the mining population and the environment. https://doi.org/10.20944/preprints201910.0298.v1
Ondayo MA, Watts MJ, Hamilton EM, Mitchell C, Mankelow J, Osano O (2023) Artisanal gold mining in Kakamega and Vihiga counties, Kenya: potential human exposure and health risk. Environ Geochem Health. https://doi.org/10.1007/s10653-023-01647-z
Oosthuizen, M, John J, Somerset V (2010) Mercury exposure in a low-income community in South Africa. South African Med J 100(6). https://doi.org/10.7196/SAMJ.4325
Ortega DR, Esquivel DFG, Ayala TB, Pineda B, Manzo SG, Quino JM, Mora PC, de la Cruz VP (2021) Cognitive impairment induced by lead exposure during lifespan: mechanisms of lead neurotoxicity. Toxics 9(2):23. https://doi.org/10.3390/toxics9020023
Pancrace P, Salanga R, Lalika M (2022) Vegetation cover changes due to artisanal and small-scale gold mining in Bukombe-Mbogwe forest reserve in Geita region, Tanzania. Tanzania J Forestry Nat Conserv 91(2):66–82
Parks CG, Conrad K, Cooper GS (1999) Occupational exposure to crystalline silica and autoimmune disease. Environ Health Perspect 107(suppl 5):793–802. https://doi.org/10.1289/ehp.99107s5793
Paruchuri Y, Siuniak A, Johnson N, Levin E, Mitchell K, Goodrich JM, Renne EP, Basu N (2010) Occupational and environmental mercury exposure among small-scale gold miners in the talensi-nabdam district of Ghana’s upper east region. Sci Total Environ 408(24):6079–6085. https://doi.org/10.1016/j.scitotenv.2010.08.022
Pascal NM, Dieudonné MEA, Jean-Noël MK (2020) Evaluation of the level of mercury pollution in the sediments of the rivers draining the gold panning sites in the territory of fizi, eastern Democratic Republic of Congo. J Geosci Environ Protect 8(02):97. https://doi.org/10.4236/gep.2020.82007
Patrick H, Hader M, Bibie S, Alexander M, Onn Min K, Stellah George M, Johanna F (2023) Silicosis, tuberculosis and silica exposure among artisanal and small-scale miners: a systematic review and modelling paper. medRxiv:2023.2005.2031.23290725. https://doi.org/10.1101/2023.05.31.23290725
PlanetGOLD (2020) Improving access to formal finance in artisanal and small-scale gold mining. https://www.planetgold.org/sites/default/files/2020-08/Improving_Access_to_Formal_Finance_in_ASGM-planetGOLD_Issue_Brief.pdf
Plumlee GS, Durant JT, Morman SA, Neri A, Wolf RE, Dooyema CA, Hageman PL, Lowers HA, Fernette GL, Meeker GP (2013) Linking Geological and health sciences to assess childhood lead poisoning from artisanal gold mining in Nigeria. Environ Health Perspect 121(6):744–750. https://doi.org/10.1289/ehp.1206051
Poddalgoda D, Macey K, Hancock S (2019) Derivation of biomonitoring equivalents (be values) for zinc. Regul Toxicol Pharmacol 106:178–186. https://doi.org/10.1016/j.yrtph.2019.04.018
Podolský F, Ettler V, Šebek O, Ježek J, Mihaljevič M, Kříbek B, Sracek O, Vaněk A, Penížek V, Majer V, Mapani B, Kamona F, Nyambe I (2015) Mercury in soil profiles from metal mining and smelting areas in Namibia and Zambia: distribution and potential sources. J Soils Sediments 15(3):648–658. https://doi.org/10.1007/s11368-014-1035-9
Pollard KM, Cauvi DM, Toomey CB, Hultman P, Kono DH (2019) Mercury-induced inflammation and autoimmunity. Biochim Biophys Acta (BBA)–gen Subj 12:129299. https://doi.org/10.1016/j.bbagen.2019.02.001
Porgo M, Gokyay O (2017) Environmental impacts of gold mining in Essakane site of Burkina Faso. Hum Ecol Risk Assess Int J 23(3):641–654. https://doi.org/10.1080/10807039.2016.1263930
Rabiu S, Abubakar M, Sahabi D, Makusidi M, Dandare A (2019) Co-exposure to lead and mercury among artisanal gold miners. Asian J Environ Ecol 12:1–8. https://doi.org/10.9734/ajee/2019/v11i330140
Rajaee M, Obiri S, Green A, Long R, Cobbina SJ, Nartey V, Buck D, Antwi E, Basu N (2015a) Integrated assessment of artisanal and small-scale gold mining in Ghana—part 2: natural sciences review. Int J Environ Res Public Health 12(8):8971–9011. https://doi.org/10.3390/ijerph120808971
Rajaee M, Obiri S, Green A, Long R, Cobbina SJ, Nartey V, Buck D, Antwi E, Basu N (2015b) Integrated assessment of artisanal and small-scale gold mining in Ghana—part 2: natural sciences review. Int J Environ Res Public Health 12:8971–9011. https://doi.org/10.3390/ijerph120808971
Rakete S, Moonga G, Wahl A-M, Mambrey V, Shoko D, Moyo D, Muteti-Fana S, Tobollik M, Steckling-Muschack N, Bose-O’Reilly S (2022) Biomonitoring of arsenic, cadmium and lead in two artisanal and small-scale gold mining areas in Zimbabwe. Environ Sci Pollut Res 29:4762–4768. https://doi.org/10.1007/s11356-021-15940-w
Rakotondrabe F, Ngoupayou JRN, Mfonka Z, Rasolomanana EH, Abolo AJN, Ako AA (2018) Water quality assessment in the Bétaré-Oya gold mining area (East-Cameroon): multivariate statistical analysis approach. Sci Total Environ 610:831–844. https://doi.org/10.1016/j.scitotenv.2017.08.080
Ralph O, Gilles N, Fon N, Luma H, Greg N (2018) Impact of artisanal gold mining on human health and the environment in the batouri gold district, east cameroon. Acad J Interdisc Stud 7(1):25–44. https://doi.org/10.2478/ajis-2018-0003
Rambiki E, Dimba A, Ng’ambi W, Banda K, Girma B, Shight B, Lwanda L, Dambe I, Tripathy JP, Chola M, -Kapata PC, Mpunga J, Kathyola D (2020) The prevalence of pulmonary tuberculosis among miners from the Karonga, Rumphi, Kasungu and Lilongwe Districts of Malawi in 2019. Malawi Medical J. https://www.ajol.info/index.php/mmj/article/view/202960
Razanamahandry L, Andrianisa H, Karoui H, Yacouba H, Manikandan E, Maaza M (2018) Cyanide dynamics in catchment areas affected by artisanal gold mining in Burkina Faso. In: Artisanal small mining conference. https://www.researchgate.net/profile/Harinaivo-Andrianisa/publication/327655887_Cyanide_dynamics_in_catchment_areas_affected_by_artisanal_gold_mining_in_Burkina_Faso/links/5b9c0abba6fdccd3cb579cd1/Cyanide-dynamics-in-catchment-areas-affected-by-artisanal-gold-mining-in-Burkina-Faso.pdf
Reyes-Hinojosa D, Lozada-Pérez C, Cuevas YZ, López-Reyes A, Martínez-Nava G, Fernández-Torres J, Olivos-Meza A, Landa-Solis C, Gutiérrez-Ruiz M, Del Castillo ER (2019) Toxicity of cadmium in musculoskeletal diseases. Environ Toxicol Pharmacol 72:103219. https://doi.org/10.1016/j.etap.2019.103219
Risher J (1999) Toxicological profile for mercury. https://www.atsdr.cdc.gov/toxprofiles/tp.asp?id=115&tid=24
Rodríguez J, Mandalunis PM (2018) A review of metal exposure and its effects on bone health. J Toxicol 2018:4854152. https://doi.org/10.1155/2018/4854152
Ross J, Ehrlich R, Hnizdo E, White N, Churchyard G (2010) Excess lung function decline in gold miners following pulmonary tuberculosis. Thorax 65(11):1010–1015. https://doi.org/10.1136/thx.2009.129999
Rupani MP (2023) A mixed-methods study on impact of silicosis on tuberculosis treatment outcomes and need for TB-silicosis collaborative activities in India. Sci Rep. https://doi.org/10.1038/s41598-023-30012-4
Rwiza M, Mohammed N, Banzi F (2022). The Influence of Gold Mining on Radioactivity of Mining Sites Soil in Tanzania. https://doi.org/10.6092/issn.2281-4485/13288
Sako A, Nimi M (2018) Environmental geochemistry and ecological risk assessment of potentially harmful elements in tropical semi-arid soils around the Bagassi south artisanal gold mining site, Burkina Faso. Cogent Environ Sci 4(1):1543565. https://doi.org/10.1080/23311843.2018.1543565
Saravanabhavan G, Werry K, Walker M, Haines D, Malowany M, Khoury C (2017) Human biomonitoring reference values for metals and trace elements in blood and urine derived from the Canadian health measures survey 2007–2013. Int J Hyg Environ Health 220(2):189–200. https://doi.org/10.1016/j.ijheh.2016.10.006
Sasu, DD (2023) Africa: gold mine production 2021. https://www.statista.com/statistics/508145/african-gold-mine-production. Accessed 27th June 2023
Schmidtkunz C, Gries W, Weber T, Leng G, Kolossa-Gehring M (2019) Internal exposure of young german adults to Di (2-Propylheptyl) phthalate (Dphp): trends in 24-H urine samples from the German environmental specimen bank 1999–2017. Int J Hyg Environ Health 222(3):419–424. https://doi.org/10.1016/j.ijheh.2018.12.008
Schwartz FW, Lee S, Darrah TH (2021) A review of the scope of artisanal and small-scale mining worldwide, poverty, and the associated health impacts. GeoHealth. https://doi.org/10.1029/2020GH000325
Seccatore J, Veiga M, Origliasso C, Marin T, De Tomi G (2014) An estimation of the artisanal small-scale production of gold in the world. Sci Total Environ 496:662–667. https://doi.org/10.1016/j.scitotenv.2014.05.003
Serge GK, Séraphin KK, Lazare KK, Alexis BL, Félix KK, Dongui BK (2019) Evaluation of pollution due to gold mining at ity-floleu area in sub-prefecture of Zouan-Hounien, Western Côte D’ivoire. J Geosci Environ Protect 7(12):20–41. https://doi.org/10.4236/gep.2019.712002
Simões MR, Azevedo BF, Alonso MJ, Salaices M, Vassallo DV (2021) Chronic low-level lead exposure increases mesenteric vascular reactivity: role of cyclooxygenase-2-derived prostanoids. Front Physiol. https://doi.org/10.3389/fphys.2020.590308
Singo J, Isunju JB, Moyo D, Steckling-Muschack N, Bose-O’Reilly S, Mamuse A (2022a) Hazards and control measures among artisanal and small-scale gold miners in Zimbabwe. Ann Glob Health 88(1):21. https://doi.org/10.5334/aogh.3621
Singo J, Moyo D, Isunju JB, Bose-O’Reilly S, Steckling-Muschack N, Becker J, Mamuse A (2022b) Health and safety risk mitigation among artisanal and small-scale gold miners in Zimbabwe. Int J Environ Res Public Health 19(21):14352. https://doi.org/10.3390/ijerph192114352
Smith NM, Ali S, Bofinger C, Collins N (2016) Human health and safety in artisanal and small-scale mining: an integrated approach to risk mitigation. J Clean Prod 129:43–52. https://doi.org/10.1016/j.jclepro.2016.04.124
So SCA, Tsoi MF, Cheung AJ, Cheung TT, Cheung BM (2021) Blood and urine inorganic and organic mercury levels in the United States from 1999 to 2016. Am J Med 134(1):e20–e30. https://doi.org/10.1016/j.amjmed.2020.06.023
Spiegel S, Viega M (2006) Global impacts of mercury supply and demand in small-scale gold mining: report to the unep governing council meeting. UNEP Governing Council: Nairobi, Kenya. www.globalmercuryproject.org. Accessed 6 July 2023
Ssenku JE, Naziriwo B, Kutesakwe J, Mustafa AS, Kayeera D, Tebandeke E (2023) Mercury accumulation in food crops and phytoremediation potential of wild plants thriving in artisanal and small-scale gold mining areas in Uganda. Pollutants 3(2):181–196. https://doi.org/10.3390/pollutants3020014
Stapper D, Dales K, Velasquez P, Keane S (2021) Best management practices for cyanide use in the smallscale gold mining sector. PlanetGOLD programme. https://www.planetgold.org/sites/default/files/CN%20Best%20Practices%20in%20ASGM_Final_Dec%2016%202021_0.pdf
Steckling N, Boese-O’Reilly S, Gradel C, Gutschmidt K, Shinee E, Altangerel E, Badrakh B, Bonduush I, Surenjav U, Ferstl P (2011) Mercury exposure in female artisanal small-scale gold miners (Asgm) in Mongolia: an analysis of human biomonitoring (Hbm) Data from 2008. Sci Total Environ 409(5):994–1000. https://doi.org/10.1016/j.scitotenv.2010.11.029
Steckling N, Bose-O’Reilly S, Shoko D, Muschack S, Schierl R (2014a) Testing local conditions for the introduction of a mercury-free gold extraction method using borax in Zimbabwe. J Health Pollut 4(7):54–61. https://doi.org/10.5696/2156-9614-4-7.54
Steckling N, Bose-O’Reilly S, Pinheiro P, Plass D, Shoko D, Drasch G, Bernaudat L, Siebert U, Hornberg C (2014b) The burden of chronic mercury intoxication in artisanal small-scale gold mining in Zimbabwe: data availability and preliminary estimates. Environ Health 13(1):111. https://doi.org/10.1186/1476-069X-13-111
Steen T, Gyi K, White N, Gabosianelwe T, Ludick S, Mazonde G, Mabongo N, Ncube M, Monare N, Ehrlich R (1997) Prevalence of occupational lung disease among botswana men formerly employed in the south african mining industry. Occup Environ Med 54(1):19–26
Stemn E, Amoh PO, Joe-Asare T (2021) Analysis of artisanal and small-scale gold mining accidents and fatalities in Ghana. Resour Policy 74:102295. https://doi.org/10.1016/j.resourpol.2021.102295
Stoffersen B, Køster-Rasmussen R, Cardeño JIC, Appel PW, Smidth M, Na-Oy LD, Lardizabal DL, Onos RW (2019) Comparison of gold yield with traditional amalgamation and direct smelting in artisanal small-scale gold mining in Uganda. J Health Pollut 9(24):191205. https://doi.org/10.5696/2156-9614-9.24.191205
Talla A, Moandjim-Me-Bock C (2018) The impact of wastewater from artisanal mining on the pollution of contaminated sites: a case study of Betare-Oya in East Cameroon. Adv Res 16:1–12. https://doi.org/10.9734/AIR/2018/43351
Taux K, Kraus T, Kaifie A (2022) Mercury exposure and its health effects in workers in the artisanal and small-scale gold mining (Asgm) sector—a systematic review. Int J Environ Res Public Health 19(4):2081. https://doi.org/10.3390/ijerph19042081
Tayrab E (2017) Thyroid function in Sudanese gold miners with chronic mercury exposure. Eur J Pharm Med Res 30:28.21–25.39
Tayrab E, Abd Elrahim MA, Elameen MEA, Yassin A, Kodi A (2016) Human mercury exposure associated with artisanal gold miners in Sudan. Int J Earth Environ Sci. https://doi.org/10.15344/2456-351X/2016/118
Telmer KH, Veiga MM (2009) World emissions of mercury from artisanal and small scale gold mining. Mercury fate and transport in the global atmosphere. Springer, pp 131–172
Thakur M, Rachamalla M, Niyogi S, Datusalia AK, Flora SJS (2021) Molecular mechanism of arsenic-induced neurotoxicity including neuronal dysfunctions. Int J Mol Sci 22(18):10077. https://doi.org/10.3390/ijms221810077
Thiombane M, De Vivo B, Niane B, Watts MJ, Marriott AL, Di Bonito M (2023) A new hazard assessment workflow to assess soil contamination from large and artisinal scale gold mining. Environ Geochem Health. https://doi.org/10.1007/s10653-023-01552-5
Tibane LV, Mamba D (2022) Dataset on enrichment of selected trace metals in the soil from designated abandoned historical gold mine solid waste dump sites near residential areas, Witwatersrand basin, South Africa. Data Brief 41:107895. https://doi.org/10.1016/j.dib.2022.107895
Tinkov AA, Paoliello MM, Mazilina AN, Skalny AV, Martins AC, Voskresenskaya ON, Aaseth J, Santamaria A, Notova SV, Tsatsakis A (2021) Molecular Targets of manganese-induced neurotoxicity: a five-year update. Int J Mol Sci 22(9):4646. https://doi.org/10.3390/ijms22094646
Tomicic C, Vernez D, Belem T, Berode M (2011) Human mercury exposure associated with small-scale gold mining in Burkina Faso. Int Arch Occup Environ Health 84(5):539–546. https://doi.org/10.1007/s00420-011-0615-x
Uganda-NEMA (2019) The national action plan for artisanal and small scale gold mining in Uganda, in accordance with the minamata convention on mercury. National Environment Management Authority (NEMA), Uganda. https://mercuryconvention.org/sites/default/files/documents/national_action_plan/Uganda-NAP-2019.pdf
Uriah L, Kenneth T, Gusikit R, Ayuba M (2013) Lead and mercury contamination associated with artisanal gold mining in Anka, Zamfara State, North Western Nigeria: the continued unabated Zamfara lead poisoning. http://hdl.handle.net/123456789/431. Accessed 6 July 2023
Veiga MM, Fadina O (2020) A review of the failed attempts to curb mercury use at artisanal gold mines and a proposed solution. Extractive Ind Soc 7(3):1135–1146. https://doi.org/10.1016/j.exis.2020.06.023
Veiga MM, Nunes D, Klein B, Shandro JA, Velasquez PC, Sousa RN (2009) Mill leaching: a viable substitute for mercury amalgamation in the artisanal gold mining sector? J Clean Prod 17(15):1373–1381. https://doi.org/10.1016/j.jclepro.2009.03.012
Veiga MM, Baker RF (2004) Protocols for environmental and health assessment of mercury released by artisanal and small-scale gold miners. United Nations Publications, Vienna, Austria: GEF/UNDP/UNIDO. http://web.unep.org/globalmercurypartnership/protocols-environmental-and-health-assessment-mercury-released-artisanal-and-small-scale-gold-miners. Accessed 6 July 2023
Veiga M, Hinton JJ (2022) Abandoned artisanal gold mines in the Brazilian Amazon: a legacy of mercury pollution. In: Natural resources forum. vol 1. Wiley Online Library, pp 15–26. https://onlinelibrary.wiley.com/doi/abs/https://doi.org/10.1111/1477-8947.00003
Verbrugge B, Lanzano C, Libassi M (2021) The cyanide revolution: efficiency gains and exclusion in artisanal-and small-scale gold mining. Geoforum 126:267–276. https://doi.org/10.1016/j.geoforum.2021.07.030
von Stackelberg K, Williams PR, Sánchez-Triana E (2022) Artisanal small-scale gold mining: a framework for collecting site-specific sampling and survey data to support health-impact analyses. World Bank Pub. https://doi.org/10.1596/978-1-4648-1819-6
Wall E (2010) Working together: how large-scale mining can engage with artisanal and small-scale miners. International council on mining and metals (ICMM), London, Washington, DC: Oil, Gas and Mining Sustainable Community Development Fund (IFC CommDev). https://commdev.org/wp-content/uploads/pdf/publications/Working-together-How-large-scale-mining-can-engage-with-artisanal-and-small-scale-miners.pdf
Wanyama CK, Makokha JW, Masinde FW, Waswa MN (2020) Natural radioactivity and external dose rates in tailing samples from rosterman gold mine, Kakamega County, Kenya. ITEGAM-JETIA 6(26):73–77. https://doi.org/10.5935/jetia.v6i26.718
Wanyana MW, Agaba FE, Sekimpi DK, Mukasa VN, Kamese GN, Douglas N, Ssempebwa JC (2020) Mercury exposure among artisanal and small-scale gold miners in four regions in Uganda. J Health Pollut 10(26):200613. https://doi.org/10.5696/2156-9614-10.26.200613
Watts MJ, Button M, Brewer TS, Jenkin GRT, Harrington CF (2008) Quantitative arsenic speciation in two species of earthworms from a former mine site. J Environ Monit 10(6):753–759. https://doi.org/10.1039/B800567B
Watts MJ, Menya D, Humphrey OS, Middleton DS, Hamilton E, Marriott A, McCormack V, Osano O (2021) Human urinary biomonitoring in western Kenya for micronutrients and potentially harmful elements. Int J Hyg Environ Health 238:113854. https://doi.org/10.1016/j.ijheh.2021.113854
Weleabzgi B, Alemayehu T, Estifanos S (2021) Assessing the environmental impact of artisanal gold mining activities on the waters and sediments around meli, northwestern Tigray, Ethiopia. Momona Ethiopian J Sci 13(2):281–299. https://doi.org/10.4314/mejs.v13i2.6
WGC (2022) Lessons learned on managing the interface between large-scale and artisanal and small-scale gold mining. https://www.gold.org/download/file/17063/ASGM-Report-2022-English.pdf
WHO (2016) Environmental and occupational health hazards associated with artisanal and small-scale gold mining. World Health Organization Technical Paper #1. https://apps.who.int/iris/bitstream/handle/10665/247195/9789241510271-eng.pdf
WHO (2020) Who methods and data sources for life tables 1990–2019. World Health Organization: Geneva. https://www.who.int/docs/default-source/gho-documents/global-health-estimates/ghe2019_life-table-methods.pdf
Wilson ST, Wang H, Kabenge M, Qi X (2017) The mining sector of Liberia: current practices and environmental challenges. Environ Sci Pollut Res 24(23):18711–18720. https://doi.org/10.1007/s11356-017-9647-4
Wireko-Gyebi RS, Asibey MO, Baah-Ennumh TY (2022) Planning for the effective and sustainable management of ghana’s artisanal small-scale gold mining industry. Resour Policy 76:102576. https://doi.org/10.1016/j.resourpol.2022.102576
World-Bank (2015) Mining together: large-scale mining meets artisanal mining. https://documents1.worldbank.org/curated/en/148081468163163514/pdf/686190ESW0P1120ng0Together0HD0final.pdf
World-Bank (2020) 2020 state of the artisanal and small scale mining sector. https://delvedatabase.org/resources/2020-state-of-the-artisanal-and-small-scale-mining-sector
Zhang F, Wang Z, Peijnenburg WJGM, Vijver MG (2022) Review and prospects on the ecotoxicity of mixtures of nanoparticles and hybrid nanomaterials. Environ Sci Technol 56(22):15238–15250. https://doi.org/10.1021/acs.est.2c03333
Zhou S, Wang Y, Yu C, Ding C, He J, Liu Y, Wang H, Ni C (2022) Metal Exposure-Related Welder’s Pneumoconiosis and Lung Function: A Cross-Sectional Study in a Container Factory of China. Int J Environ Res Public Health 19(24):16809. https://doi.org/10.3390/ijerph192416809
Zhu Y, El-Demerdash FM, Li X, Machado MM, Boye A (2022). Toxicity Mechanisms, Exposure, Toxicokinetic and Risk Assessment Aspects of Metals, Toxic for Animals and Humans. https://doi.org/10.3389/978-2-88974-640-8
Zhuwarara SK (2023) The potential of digitisation in enhancing regulation and sustainability in the artisanal and small-scale mining (Asm) sector in Zambia, Nigeria, and Ghana. Mining Law Govern Afr 111:525–528. https://doi.org/10.4324/9781003284437-11
Funding
Inorganic Geochemistry Facility at British Geological Survey and British Geological Survey University Funding Initiative (BUFI) [BGS Contract Number: GA/19S/020]. Additional support was provided by the British Academy Early Career Researchers Writing Skills Workshop (WW21100104); BGS East Africa Official Development Assistance (ODA) platform (NE/R00069/1); and NERC National Capability Science international award (NE/X006255/1).
Author information
Authors and Affiliations
Contributions
This manuscript was designed, written, and reviewed by MAO, MJW, and OO and reviewed and edited by CM, DCPK, and SBO.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ondayo, M.A., Watts, M.J., Mitchell, C.J. et al. Review: Artisanal Gold Mining in Africa—Environmental Pollution and Human Health Implications. Expo Health 16, 1067–1095 (2024). https://doi.org/10.1007/s12403-023-00611-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-023-00611-7