
Abstract
Introduction
In the event-driven FREEDOM-EV trial, oral treprostinil delayed clinical worsening in patients with pulmonary arterial hypertension (PAH). Open-label extension studies offer additional data about tolerability, efficacy, and survival, especially for those initially assigned placebo. The aim of the current study was to determine if oral treprostinil changed survival when considering the parent and extension study, if treprostinil provides functional benefits for participants initially assigned to placebo, and if the benefits observed for those treated with treprostinil were durable.
Methods
Both active and placebo participants from FREEDOM-EV could enroll in the FREEDOM-EV open-label extension (OLE) study after experiencing an investigator-assessed clinical worsening event or after parent study closure. All participants in the OLE were offered open-label oral treprostinil. Previously assigned placebo participants titrated to maximally tolerated doses; previously assigned treprostinil participants continued dose titration. We repeated assessments including functional class and 6-min walk distance (6MWD) at 12-week intervals and measured N-terminal pro-brain natriuretic peptide (NT-proBNP) at week 48. Survival was estimated by Kaplan–Meier analysis, and we estimated hazard ratio (HR) using Cox proportional hazards.
Results
Of 690 FREEDOM-EV participants, 470 enrolled in the OLE; vital status was available for 89% of initial Freedom-EV participants. When considering the combined parent and open-label data, initial assignment to oral treprostinil reduced mortality (HR 0.64, 95% confidence interval 0.46–0.91, p = 0.013); absolute risk reduction was 9%. Participants randomized to placebo who initiated oral treprostinil after clinical worsening and tolerated treatment through week 48 demonstrated favorable shifts in functional class (p < 0.0001), 6MWD improvements of + 84 m (p < 0.0001), and a reduction in NT-proBNP of − 778 pg/mL (p = 0.02), compared to OLE baseline. Modest trends toward benefit were measured for those initially assigned placebo who did not have clinical worsening, and 132/144 (92%) of treprostinil assigned participants without clinical worsening remained on drug at week 48 in the OLE study. Adverse events were consistent with FREEDOM-EV.
Conclusion
Initial treprostinil assignment improved survival in the entire data set; those who began treprostinil after a clinical worsening in the placebo arm and tolerated drug to week 48 enjoyed substantial functional gains.
Clinical Trial Registration
ClinicalTrials.gov identifier NCT01560637.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The original FREEDOM-EV study demonstrated statistically significant reduction in mortality for those randomly allocated to active therapy. Here, we report the results of three additional years of open-label observation after the close of the placebo-controlled, event-driven study. |
In FREEDOM-EV OLE the survival curves separate at 2 years and absolute risk reduction for death is 9%. |
This study reports notable functional benefits (6MWD improvement, NT-proBNP reduction, and functional class shift) for those who began active therapy after initial assignment to placebo. |
This data provided the opportunity to “look back” and see that the participants who suffered clinical worsening events during the original Freedom-EV study were substantially different at baseline than those who did not. |
Introduction
Pulmonary arterial hypertension (PAH) is a rare but progressive and often fatal lung vascular disease, and while therapy options have greatly expanded, evidence to guide clinicians in choosing specific drugs remains sparse [1]. Historically, data from open-label extensions supplemented the primary efficacy data [2,3,4], assessing durability for those initially assigned active and any benefit for those initially assigned placebo (PBO). Three times daily oral treprostinil (TRE) was shown to reduce the risk of clinical worsening in the FREEDOM-EV study [5]. Those who had a clinical worsening event (CWE) were immediately eligible for open-label treatment; those who completed the study without clinical worsening (CW) were eligible at the close of the primary study. We interrogated this data in three ways: (1) to assess the survival benefit over a longer period of observation (especially for those randomized late in the study); (2) to assess any benefits in placebo participants starting treprostinil; (3) to evaluate durability of functional benefits for treprostinil participants in the parent study.
Methods
Study Design
Many details about the methods are included in the Supplementary Material; briefly, the FREEDOM-EV trial was a randomized, double-blind, placebo-controlled, event-driven study conducted between June 2012 and June 2018. Both active (oral TRE) and placebo participants from FREEDOM-EV could enroll in the open-label extension (OLE) after experiencing an investigator-assessed CWE (or after parent study closure) [5]. Patients were excluded from the OLE study if they had discontinued participation in FREEDOM-EV for any reason other than a CWE or if they had received treatment with infused or inhaled prostacyclin for 29 days or more. The OLE closed in July 2021, and 121 individuals who did not have access to commercial drug are still taking treprostinil through the sponsor. Data were collected and analyzed according to a prespecified statistical analysis plan, and all authors had access to the source-verified data and attest to the accuracy and completeness of this report. The study was conducted in accordance with the tenets of the Declaration of Helsinki and Good Clinical Practice. Written informed consent was obtained from all participants. The protocol and all study-related documents were approved by the institutional review board or independent ethics committee for each site (Supplementary Materials).
Selection of Participants
Participants were 18–75 years of age, met the 2013 consensus definition of group 1 PAH [6], and had a 6-minute walk distance (6MWD) ≥ 150 m at the screening visit for the FREEDOM-EV study. Any participant alive after a CWE was eligible for open-label treprostinil, including those who had a CWE while on active therapy.
Trial Procedures
After the sponsor’s acceptance of a complete CWE report and the site’s confirmation of enrollment in the OLE, the interactive voice response system issued unblinded information to guide dosing in the OLE. Participants who were already using treprostinil continued at the previous dose and were able to titrate further without limitation (identified as TRE → TRE). Those initially assigned placebo were instructed to begin oral treprostinil 0.125 mg three times daily (spaced carefully every 6 to 8 h with food, identified as PBO → TRE) and no maximum dose was specified.
Outcome Measures
Study participants were assessed at OLE enrollment (baseline OLE), week 6, and every 12 weeks thereafter. Efficacy assessments included 6MWD, Borg dyspnea score, and World Health Organization (WHO) functional class; plasma N-terminal pro-brain natriuretic peptide (NT-proBNP) was collected at week 48 only. Before the final statistical analysis plan was submitted to the US Food and Drug Administration (FDA), we planned an a priori risk analysis using three noninvasive variables as previously proposed [7] and validated [8] (i.e., 6MWD, NT-proBNP, and WHO functional class); for the current report, we supplemented the French noninvasive risk analysis with the COMPERA 2.0 score [9] and the REVEAL Lite 2 score [10]. Safety assessments included evaluation of adverse events (AEs) and clinical laboratory parameters.
Results
Participants
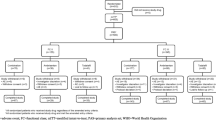
Of the 690 initial FREEDOM-EV participants, 470 (68%) enrolled in the OLE (Fig. 1). Table 1 shows the demographic and clinical characteristics of participants, divided by their initial treatment assignment in the parent study. Participants were predominantly female; 57% had WHO functional class I or II symptoms, and 74% were taking a phosphodiesterase 5 (PDE5) inhibitor or soluble guanine cyclase (sGC) stimulator.

CONSORT diagram for the open-label extension of the FREEDOM-EV study showing reasons for discontinuation until the week 48 timepoint when the key clinical assessments were made. Thirty participants initially assigned to placebo and 27 participants initially assigned to treprostinil completed FREEDOM-EV and were eligible to enroll but did not (i.e., they had not had a disqualifying, drug related adverse event but decided for some other reason not to enroll). CWE clinical worsening event, No CWE no clinical worsening event, OLE open-label extension, PBO placebo, TRE oral treprostinil
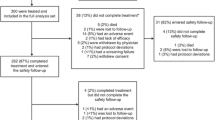
Figure 1 shows the overall disposition of participants in the parent FREEDOM-EV study as they entered into the OLE as well as the reasons for discontinuation before the week 48 timepoint when we made the key efficacy observation during open-label experience. We separated participants into four groups, categorized by original treatment assignment and CWE status from the parent study. Of note, discontinuations for AEs by week 48 for previous treprostinil participants was low (7%) compared to 11% of previous placebo participants (who were exposed to treprostinil for the first time; most discontinuations due to adverse effect occur early). Of the 144 treprostinil participants who entered OLE without a CWE, 132 (92%) continued to week 48.
Survival
Initial treprostinil assignment resulted in a 9% absolute risk reduction for death compared to those initially assigned placebo, acknowledging 11% missing data overall. An unadjusted Kaplan–Meier analysis is shown in Fig. 2a. Most (75%) of the placebo-assigned participants from FREEDOM-EV enrolled in the open-label study and began oral TRE with a median treatment delay of 55 weeks (placebo exposure of 55 weeks). Even among the low-risk group that was initially assigned placebo and completed the parent study without a CWE, there were five deaths before week 48 (as compared to zero among treprostinil assigned participants who completed the open label without CWE, Fig. 1). With the additional deaths, which accumulated disproportionately among former placebo participants during the open-label study, the survival curves now separate at 2 years. There was a 36% reduction in risk of death for participants initially assigned oral TRE compared to placebo; the hazard ratio (HR) was 0.64 (95% CI 0.46–0.91, p = 0.013). Figure 2b shows the complete set of hazard ratios as deaths were recorded in the parent FREEDOM-EV, OLE, and Vital Status Subtudy. Finally, with regard to the missing data, a “tipping point” analysis indicates that the result is robust; even if we assumed eight excess deaths among treprostinil participants for this group of 74 whose vital status is unknown, the mortality benefit would remain statistically significant (theoretical Fisher’s exact in that case, p = 0.049).

A Oral treprostinil reduced mortality even after initial placebo participants crossed over to active treatement with oral TRE. A total of 346 participants were initially assigned oral treprostinil and 344 matching placebo; for 74 participants (11%), vital status was unknown. In July 2021 at final database closure, hazard ratio for death among those initially assigned treprostinil was 0.64 (95% CI 0.46–0.91, p = 0.013). In the main EV study, participants were censored at time of study withdrawal, but most participants continued to be followed in a “vital status substudy” which involved phone confirmation of vital status every 6 months until October 2018. Participation in OLE was high for those who completed the EV study; 258 of 288 eligible placebo-assigned participants enrolled (30 declined to continue participating even though eligible) and 212 of 239 eligible treprostinil-assigned participants enrolled (27 declined to continue). In OLE, participants were censored as soon as they withdrew without further attempts to determine vital status. B Tabular summary of all-cause deaths in FREEDOM-EV, FREEDOM-EV OLE, and the Vital Status Substudy. CI confidence interval, DC discontinued, HR hazard ratio, OLE open-label extension, PBO placebo, TRE oral treprostinil
Dosing and Exposure
Figure 3 provides dosing information for the four groups after enrollment in the OLE. Over the first 24 weeks of the OLE, the PBO → TRE participants steadily titrated oral TRE to doses comparable to actively treated participants in FREEDOM-EV at week 24 [5]. Interestingly, the PBO → TRE participants with clinical worsening (CWE) reached 5.7 mg TID at week 48, while the PBO → TRE participants without clinical worsening (no CWE) did not titrate as rapidly or achieve doses as high. In the safety analysis, the median exposure to oral TRE for those originally randomized to PBO was 113 weeks (IQR 47, 159) and 223 weeks (IQR 152, 290) for those randomized to oral TRE (inclusive of exposure in FREEDOM-EV and OLE.)

Dosing increased steadily for initial placebo participants as they entered open label, and doses at week 24 (approx. 3.5 mg TID) were very similar to the actively treated group in the parent EV study. CWE clinical worsening event, NO CWE no clinical worsening event, OLE open-label extension, PBO placebo, SD standard deviation, TID three times daily, TRE oral treprostinil
Baseline Characteristics of Groups with CWE
Not surprisingly, the groups (both placebo-assigned and treprostinil-assigned) that had CWE had a high average risk profile at the time of entry into OLE (Table 2, top) as compared to those who did not have CWE. Perhaps more interesting, looking back to baseline characteristics at enrollment in the parent study, the CWE groups also looked markedly different than the groups that did not have a CWE (Table 2, bottom). The two sets of participants who had CWE had much higher NT-proBNP, significantly lower 6MWD, and a more severe functional class profile at baseline in the parent study, yielding a substantially higher risk score/classification whether calculated by REVEAL Lite 2 or COMPERA 2.0.
Previous Placebo Participants with CWE
Of the 108 placebo-assigned participants who had CWE and entered OLE, there were 11 deaths (10%) in this high-risk group during the first 48 weeks, and 16 (15%) did not tolerate drug, similar to the AE dropout rate in the parent trial (Fig. 1). Sixty-nine (64%) completed assessments at week 48, and 58 had a recorded 6MWD which increased on average 84 m (Fig. 4a, p < 0.0001 compared to open-label baseline). Forty-nine had an NT-proBNP which fell (Fig. 4b, p < 0.03), and 65 had a WHO functional class assessment at week 48 (with improvement in 43%, Fig. 4c, p < 0.0001). We added a post hoc analysis of the open-label data, using the more recently described COMPERA 2.0 and REVEAL Lite 2 risk scores instead of the French noninvasive (the score we had selected a priori for the analyses in the parent FREEDOM-EV study). Most (58%) of these participants were intermediate-high risk at baseline in the OLE (this group had all experienced CWE), and a substantial minority were high risk (Fig. 4d). For the 51 with a score at week 48, more than half of the group improved with 51% now intermediate-low risk (Fig. 4d, p = 0.0004). Similarly, REVEAL Lite 2 assessed this to be a very high-risk group at open-label baseline, and because REVEAL Lite 2 is less sensitive to missing data, 64 of the 69 who completed week 48 had a score (Fig. 4e). When considering the categorical low/intermediate/high strata, 35% shifted favorably, and 36% had dropped to low risk (Fig. 4e, p = 0.001). REVEAL Lite 2 produces an integer score, and on average, the score dropped by 1.2 ± 1.9 (p < 0.0001); a drop of at least 1 in this continuous, quantitative scoring system is prognostically significant [11], and most, 39/64 participants, dropped by at least 1 (p < 0.0001). Tabular data at week 48 is presented as Supplementary Material Table 1.

Placebo-assigned participants who had clinical worsening, began oral treprostinil, and had week 48 assessments demonstrated functional improvements. A 6MWD increased 84 m (paired-t, p < 0.0001 compared to baseline); the baseline 6MWD in the OLE was similar between the overall 106 and the 58 who had a baseline and week 48 test (i.e., those for whom paired-t statistic could be performed). B NT-proBNP dropped (paired t test against log-transformed data); for this group of n = 49 with baseline and week 48 values, the median and upper IQR were not as high as the n = 96 with baseline values, but the statistic reported is for the group with both values. Median (IQR) = line (bar). Geometric mean = dot. C WHO functional class shifted favorably (McNemar’s test p < 0.0001). D Participants (n = 51) with complete data were statistically different at week 48 using the 4-strata COMPERA 2.0 risk tool (McNemar’s test, p = 0.0004). E REVEAL Lite 2 is less sensitive to missing data and n = 64 participants were statistically different at week 48 (McNemar’s test, p = 0.001). COMPERA 2.0 Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension Version 2.0, EV OLE FREEDOM-EV open-label extension, FC functional class, IQR interquartile range, m meter, mL milliliter, NT-proBNP plasma N-terminal pro-brain natriuretic peptide, pg picogram, REVEAL Lite 2 Registry to Evaluate Early and Long-term PAH Disease Management Version 2, WHO FC World Health Organization Functional Class, 6MWD 6-minute walk distance
Previous Placebo Participants Without CWE
The placebo-assigned participants who enrolled in OLE at the close of the parent study (no CWE, n = 150) were a low-risk group (Table 2, Fig. 5d; mean REVEAL Lite 2 = 4.5). By week 48 of open-label experience, 13 participants (9%) had stopped the drug because of adverse effects (lower than the parent study), and 5 (3%) had died. For the 125 (83%) who had a week 48 assessment, exposure to oral treprostinil produced favorable trends including a significant reduction in NT-proBNP. The mean 6MWD at baseline in OLE was 450 m, and 58% had a 6MWD distance ≥ 440 m; the median walk increased numerically by 6 m (Fig. 5a, p = 0.19). Similarly, the median NT-proBNP was 270 pg/mL, and 52% had an NT-proBNP < 300 pg/mL. Even so, there appeared to be a favorable effect of treprostinil as the mean reduction in NT-proBNP was 140 pg/mL, and Fig. 5b shows that the upper bound of the IQR dropped visually (p = 0.03). A similar trend was also observed for WHO functional class with 12% improving (Fig. 5c, p = 0.07). Integrating these observations into the COMPERA 2.0 score, we observed that 90% of these participants began open-label experience with either low or intermediate-low status, and nonetheless, we observed a trend with 14% improved by one stratum (Fig. 5d, p = 0.10). REVEAL Lite 2 made a similar estimate with 85% being intermediate or low risk at baseline but the three-strata model was less sensitive to improvement (Fig. 5e). The quantitative REVEAL Lite 2 score did not change, but started quite low with a mean of 4.5.

Placebo-assigned participants who did not have clinical worsening and began oral treprostinil were stable at week 48 assessments. A 6MWD was an average 6 m higher (paired-t, p = 0.19 compared to baseline); most of these participants already had 6MWD > 440 m. B NT-proBNP dropped (paired t test against log-transformed data); for this group of n = 114 with baseline and week 48 values, the median and upper IQR were not as high as the n = 147 with baseline values, but the statistic reported is for the group with both values. Median (IQR) = line (bar). Geometric mean = dot. C WHO functional class was preserved (McNemar’s test p = 0.07). D Consistent with previous reports, 4-strata COMPERA 2.0 was relatively sensitive to improvements and overall risk trended lower at week 48 (McNemar’s test, p = 0.10). E REVEAL Lite 2 was not different at week 48 (McNemar’s test, p = 0.56). COMPERA 2.0 Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension Version 2.0, EV OLE FREEDOM-EV open-label extension, FC functional class, IQR interquartile range, m meter, mL milliliter, NT-proBNP plasma N-terminal pro-brain natriuretic peptide, pg picogram, REVEAL Lite 2 Registry to Evaluate Early and Long-term PAH Disease Management Version 2, WHO FC World Health Organization Functional Class, 6MWD 6-minute walk distance
Previous Treprostinil Participants Starting OLE
For the low-risk group assigned to treprostinil who completed the parent study without CWE (n = 144), we observed stability over the first 48 weeks of open-label experience. There were no deaths, although ten participants (7%) stopped the drug because of AEs. For 126 participants who had a 6MWD at week 48, it was similar to baseline (Fig. 6a); for 122 participants who had NT-proBNP, it was again steady with median baseline and week 48 values below 300 pg/mL (Fig. 6b). Functional class was likewise stable with an equally small number of patients improving and declining (Fig. 6c). The distribution of COMPERA 2.0 scores at baseline was 94% low or intermediate-low risk, and again, the results were largely stable with an equally small number of participants improving and declining (Fig. 6d). REVEAL Lite 2 had a few more observations than COMPERA 2.0 (less sensitive to missing data) and suggested the possibility that more patients (16%) deteriorated than improved (9%), but overall, these scores were also stable (Fig. 6e, p = 0.08). Quantitatively, the REVEAL Lite 2 score started at 4.3 ± 2.1 (extremely low risk) and increased by 0.4 ± 1.6 at week 48 OLE. The inclusion of more labile variables (heart rate, blood pressure) into REVEAL Lite 2 may make it more prone to noise in therapeutic trials.

Treprostinil-assigned participants who did not have clinical worsening and continued oral treprostinil were stable at week 48 assessments. A 6MWD was an average 7 m lower (paired-t, p = 0.12 compared to baseline); most of these participants already had 6MWD > 440 m. B NT-proBNP (paired t test against log-transformed data) started and finished with a median under the low-risk threshold of 300 pg/mL. Median (IQR) = line (bar). Geometric mean = dot. C WHO functional class was preserved (McNemar’s test p = 0.56). D COMPERA 2.0 risk started and finished favorably (McNemar’s test, p = 0.53). E REVEAL Lite 2, which includes more labile values like heart rate and blood pressure, trended worse at week 48 (McNemar’s test, p = 0.08). COMPERA 2.0 Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension Version 2.0, EV OLE FREEDOM-EV open-label extension, FC functional class, IQR interquartile range, m meter, mL milliliter, NT-proBNP plasma N-terminal pro-brain natriuretic peptide, pg picogram, REVEAL Lite 2 Registry to Evaluate Early and Long-term PAH Disease Management Version 2, WHO FC World Health Organization Functional Class, 6MWD 6-minute walk distance
A small group (n = 66) of treprostinil-assigned participants had a CWE in the parent study and yet still continued treprostinil in the OLE, which seemed an unusual decision for us as author-investigators. These participants were largely (70%) from regions of the world in which access to expert care and drugs may have influenced the decision to continue participating in a study that offered open-label therapy and access to the study team at regular intervals. Seven (11%) died by week 48; functional and risk outcomes are shown in Supplementary Material Fig. 1.
Safety
Nearly all (n = 238, 92%) prior placebo-assigned participants reported a treprostinil-attributable AE after beginning open-label treprostinil (Table 3), and 83 (32%) of these stopped the drug because of an AE by the end of the study. Forty-six (18%) reported that the treprostinil-attributable AE was severe in intensity (eight subsequently stopped the drug and are included in the aforementioned 83 who stopped because of an AE). Twenty-one participants (8%) had a serious AE attributable to treprostinil. AEs were typical for treprostinil and similar to those reported in the parent study; of note, it did not appear that AEs were more likely in the group of low risk, placebo-assigned patients who began treprostinil with no CWE (Table 3). If anything, AEs were numerically more likely in the high-risk group who had had a CWE.
Discussion
Survival
We initially reported a statistically significant survival benefit for three times daily treprostinil-assigned participants, but the group separation occurred late. With a longer period of observation, especially for those randomized relatively late in the conduct of the parent trial, the complete data set includes more deaths and now shows clear group separation at year 2 after randomization in the parent study. Absolute risk reduction was 9%, corresponding to a number needed to treat of 12 to prevent a death. Thus, our initial report of the first placebo-controlled trial in PAH to demonstrate a mortality benefit using the a priori statistical plan is even stronger now with the complete data set. While we acknowledge that the post hoc analysis of mortality from AMBITION [12] was robust and indicates a survival benefit for initial combination therapy, we propose that this new data might influence clinical practice in the choice of an oral drug from this class. Selexipag’s similarly designed event-driven study had numerically more deaths at the end of the placebo-controlled period in the active treatment arm, and although PAH-related deaths numerically favored active treatment at the trial close, the available data does not support a survival benefit for selexipag [13]. In fact, the efficacy of oral treprostinil in this regard is perhaps underscored because GRIPHON, FREEDOM-EV, and similar event-driven trials took great pains to avoid finding a mortality benefit by offering open-label drug immediately to the surviving placebo participants who had a CWE, thus biasing the studies against finding a survival advantage. Despite this bias, our study showed a mortality benefit.
We believe that this survival data underscores the urgency with which clinicians need to address PAH, even in COMPERA 2.0 intermediate-low and REVEAL Lite 2 ≤ 6. The participants in FREEDOM-EV were effectively “early combination therapy” (median time on monotherapy 6 months before randomization), and treatment delay (randomization to placebo) led to a clear increase in CWE and death over the median 55 weeks of careful, quarterly observation explicitly designed to prevent death. Our recent analysis of risk argued for fixed-duration “clinical improvement” studies to synthesize the goals of measuring durable treatment effects and functional benefits [11], and we believe that the mortality consequences of event-driven studies are another reason to avoid these in the future.
Participants with CWE were Higher Risk
Our demographic analysis looking “backward” at the baseline demographics for those who had CWE is a first for the previously reported event-driven studies in PAH. We think this analysis emphasizes the utility of integrated risk scores in patient selection for studies that are designed to find a difference in the occurrence of CWE (e.g., event-driven or, alternatively, primary endpoint as time-to-clinical-worsening during a defined period). Both placebo and treprostinil-assigned participants who had events had higher average REVEAL Lite 2 scores and a more advanced COMPERA 2.0 risk profile (Table 2). The currently enrolling event-driven study of sotatercept is only including participants with REVEAL Lite 2 ≥ 6, and our post hoc analysis strongly supports that as a sensible enrichment strategy.
In addition to the survival benefit, treprostinil proved effective in providing functional benefits, even for those who had suffered CWE while taking placebo. Functional improvements, measured as part of a multifaceted risk assessment, have been repeatedly associated with improved outcomes [7, 8, 14, 15]. Unlike the group of participants initially enrolled in FREEDOM-EV that were relatively lower risk at baseline, those assigned placebo who suffered a CWE and began open-label therapy were a relatively higher-risk population with a mean REVEAL Lite 2 score of 8.2. Sixty-nine individuals (64%) in this group titrated drug steadily to a mean of 5.7 ± 3.8 mg when they completed week 48, experiencing substantial benefits in NT-proBNP, functional class, and 6MWD. There were 11 deaths (10%) during that 48 weeks, and we are not advocating oral treprostinil for high-risk individuals; however, this data strengthens the overall efficacy profile of the drug.
For those who tolerated AEs and remained on drug, functional benefits were durable. This is most evident in the group of 138 participants who initially began oral treprostinil, had no CWE, and remained on drug in open label (Fig. 6). There were no deaths over those 48 weeks; this is very different than the similarly low-risk group of placebo-assigned participants who began oral treprostinil (without clinical worsening) and still had 5 deaths (3%) during the first 48 weeks of open label. Low risk does not mean no risk in PAH, and we believe that monotherapy is rarely adequate. In support of an early treatment strategy with oral treprostinil, the placebo participants who began treprostinil without previous CWE had a typical AE profile for this class of medication and 19% discontinued drug because of an AE (Table 3, similar to the blinded Freedom-EV parent study).
Limitations
Our study has important limitations. Adverse effects typical for prostacyclin class medications were common, and 126 (27%) participants in the OLE ultimately stopped the drug because of an AE during the at least 3 years of observation. The functional benefits recorded in the open-label phase were obviously only observed in those who survived and tolerated drug to week 48 (a “completers” analysis). The overall survival analysis, while increasingly robust at this point, is limited by 74 participants (11% of initially enrolled) whose vital status is unknown. Importantly, the baseline mortality risk for those with unknown vital status was similar between placebo- and treprostinil-assigned participants (unlike the overall study population), and the present analysis would remain significant even in the extreme case of eight excess treprostinil deaths in this group with unknown vital status.
Conclusions
Oral treprostinil three times daily improved survival in comparison to those assigned placebo over the entire period of observation in FREEDOM-EV and open label. For those who suffered CWE while assigned to placebo, a majority completed 48 weeks of open-label therapy and recorded impressive functional benefits despite having intermediate risk for mortality. A remarkable 92% of those initially assigned treprostinil who completed FREEDOM-EV without CWE maintained an average low-risk status during 48 weeks of open-label therapy.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the study sponsor on reasonable request.
References
Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2022;61:2200879.
Oudiz RJ, Galie N, Olschewski H, et al. Long-term ambrisentan therapy for the treatment of pulmonary arterial hypertension. J Am Coll Cardiol. 2009;54(21):1971–81.
Benza RL, Seeger W, McLaughlin VV, et al. Long-term effects of inhaled treprostinil in patients with pulmonary arterial hypertension: the Treprostinil Sodium Inhalation Used in the Management of Pulmonary Arterial Hypertension (TRIUMPH) study open-label extension. J Heart Lung Transplant. 2011;30(12):1327–33.
Oudiz RJ, Brundage BH, Galie N, et al. Tadalafil for the treatment of pulmonary arterial hypertension: a double-blind 52-week uncontrolled extension study. J Am Coll Cardiol. 2012;60(8):768–74.
White RJ, Jerjes-Sanchez C, Bohns Meyer GM, et al. Combination therapy with oral treprostinil for pulmonary arterial hypertension. A double-blind placebo-controlled clinical trial. Am J Respir Crit Care Med. 2020;201(6):707–17.
Galie N, Barbera JA, Frost AE, et al. Initial use of ambrisentan plus tadalafil in pulmonary arterial hypertension. N Engl J Med. 2015;373(9):834–44.
Boucly A, Weatherald J, Savale L, et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur Respir J. 2017;50(2):1700889–99.
Hoeper MM, Pittrow D, Opitz C, et al. Risk assessment in pulmonary arterial hypertension. Eur Respir J. 2018;51(3):1702606.
Hoeper MM, Pausch C, Olsson KM, et al. COMPERA 2.0: a refined four-strata risk assessment model for pulmonary arterial hypertension. Eur Respir J. 2022;60(1):2102311.
Benza RL, Kanwar MK, Raina A, et al. Development and validation of an abridged version of the REVEAL 2.0 risk score calculator, REVEAL Lite 2, for use in patients with pulmonary arterial hypertension. Chest. 2021;159(1):337–46.
Benza RL, Gomberg-Maitland M, Farber HW, et al. Contemporary risk scores predict clinical worsening in pulmonary arterial hypertension—an analysis of FREEDOM-EV. J Heart Lung Transplant. 2022;41(11):1572–80.
Hoeper MM, McLaughlin VV, Barbera JA, et al. Initial combination therapy with ambrisentan and tadalafil and mortality in patients with pulmonary arterial hypertension: a secondary analysis of the results from the randomised, controlled AMBITION study. Lancet Respir Med. 2016;4(11):894–901.
Sitbon O, Channick R, Chin KM, et al. Selexipag for the treatment of pulmonary arterial hypertension. N Engl J Med. 2015;373(26):2522–33.
Benza RL, Farber HW, Frost A, et al. REVEAL risk scores applied to riociguat-treated patients in PATENT-2: Impact of changes in risk score on survival. J Heart Lung Transplant. 2018;37(4):513–9.
Benza RL, Miller DP, Foreman AJ, et al. Prognostic implications of serial risk score assessments in patients with pulmonary arterial hypertension: a Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL) analysis. J Heart Lung Transplant. 2015;34(3):356–61.
Acknowledgements
The authors thank the patients who participated in this trial, their families, the investigators, and staff at all the clinical sites.
Funding
This work was sponsored by United Therapeutics Corporation (Research Triangle Park, NC) and United Therapeutics Corporation funded the journal’s rapid service fee.
Author information
Authors and Affiliations
Consortia
Contributions
R. James White is the Principal Investigator of the study and contributed substantially to the protocol, beginning with amendment 2, actively recruited and treated participants in the study, served as the academic lead for analysis and interpretation of the data, and wrote the initial manuscript draft. Rob Grover, Aliou Ousmanou, Scott Seaman, Chunqin Deng, and Meredith Broderick conceived and designed the study. Ekkehard Grünig, Franck Rahaghi, Jean Elwing, Carmine Dario Vizza, Joanna Pepke-Zaba, Jieyan Shen, Hua Yao, Antoine Hage, Stephan Rosenkranz, Madelon Vonk, Vijay Balasubramanian, Yang Yuanhua, Zaixin Yu, James Lordan, Linda Cadaret and R. James White were investigators in the study, actively recruited and treated participants in the study, obtained data and provided revisions to the manuscript. Rob Grover served as Medical Monitor for the study and provided critical input, data analysis and manuscript revision. Chunqin Deng managed the Study Database, performed and directed all the statistical analyses per the Statistical Analysis Plan, helped with interpretation of the statistics and their inclusion in the manuscript, supported additional analyses requested by the authors, and revised the manuscript throughout its development. All authors approve of the decision to submit the manuscript for publication and assume responsibility for the overall content and integrity of the article.
Corresponding author
Ethics declarations
Conflict of Interest
The following authors have declarations of support from organizations for the submitted work: Ekkehard Grünig, Franck Rahaghi, Jean Elwing, Carmine Dario Vizza, Joanna Pepke-Zaba, Jieyan Shen, Hua Yao, Antoine Hage, Stephan Rosenkranz, Madelon Vonk, Vijay Balasubramanian, Yang Yuanhua, Zaixin Yu, James Lordan, Linda Cadaret and R. James White received institutional funding from United Therapeutics in order to conduct the study at their respective institutions. Ekkehard Grünig, Franck Rahaghi, Jean Elwing, Carmine Dario Vizza, Joanna Pepke-Zaba, Stephan Rosenkranz, Madelon Vonk, Vijay Balasubramanian, and Linda Cadaret have received support for consultation, advisory and/or speaker bureau from United Therapeutics. Rob Grover, Aliou Ousmanou, Scott Seaman, Chunqin Deng, and Meredith Broderick are employees of United Therapeutics. Below, is a summary of each authors’ disclosures, related and unrelated to the submitted work. Ekkehard Grünig—Received fees for lectures and/or consultations from Actelion, Bayer/MSD, Ferrer, GEBRO, GSK, Janssen and OMT. Research grants to his institution have been received from Acceleron, Actelion, BayerHealthCare, MSD, Bellerophon, GossamerBio, GSK, Janssen, Novartis, OMT, Pfizer, REATE and United Therapeutics. Franck Rahaghi—received research support, serving on Advisory Board, Consultation and/or Speaker bureau for United Therapeutics; grants or contracts from Bayer, Janssen PH, and Acceleron. Jean Elwing—received grant/research support and/or serving on Advisory Boards for Janssen, United Therapeutics, Liquidia, Phase Bio, Gossamer Bio, Bayer, Acceleron/Merck, Altavant, Aerovate, Tenax, and Pharmosa. Carmine Dario Vizza—received grant/research support and/or serving on Advisory Boards or as a consultant for Ferrier, GSK, MSD, Bayer Actelion and United Therapeutics. Joanna Pepke-Zaba—received honoraria for lecturing and consulting from Bayer, Actelion, and GSK; on advisory boards for Actelion, Pfizer, Bayer, GSK, and United Therapeutics. Jieyan Shen—received institutional funding from United Therapeutics in order to conduct the study at their institution. Hua Yao—received institutional funding from United Therapeutics in order to conduct the study at their institution. Antoine Hage—received research grant/support from Actelion, Bayer, United Therapeutics, REATA and Arena. Stephan Rosenkranz—received research grants or contracts from Actelion, AstraZeneca, Bayer, Janssen, and Novartis; consulting fees from Abbott, Acceleron, Actelion, Bayer, Janssen, MSD, Novartis, Pfizer, United Therapeutics, and Vifor; and payment or honoraria from Actelion, Bayer, BMS, Ferrer, GSK, Janssen, MSD, Novartis, Pfizer, United Therapeutics, and Vifor. Madelon Vonk—Received research support, serving on Advisory Board, Consultation and/or Speaker bureau for Actelion, Boehringer Ingelheim, Ferrier, GSK, and Roche. Vijay Balasubramanian—received research support, serving on Advisory Board, Consultation and/or Speaker bureau for United Therapeutics, Bayer, and Boehringer Ingelheim. Yuanhua Yang—received institutional funding from United Therapeutics in order to conduct the study at their institution. Zaixin Yu—Received institutional funding from United Therapeutics in order to conduct the study at their institution. James Lordan—received institutional funding from United Therapeutics in order to conduct the study at their institution. Linda Cadaret—received grant/ research support and/or serving on Advisory Boards for United Therapeutics. Rob Grover—employee of the United Therapeutics—sponsor of the study. Aliou Ousmanou—employee of the United Therapeutics—sponsor of the study. Scott Seaman—employee of the United Therapeutics—sponsor of the study. Chunqin Deng—employee of the United Therapeutics—sponsor of the study. Meredith Broderick—employee of the United Therapeutics—sponsor of the study. R. James White—received research support (payment to institution only) from United Therapeutics.
Ethical approval
The protocol and all study-related documents were approved by the institutional review board or independent ethics committee for each site. The full list of institutional review board and independent ethic committee names, locations, and serial numbers can be found in the Supplementary Materials. The study was conducted in accordance with the tenets of the Declaration of Helsinki and Good Clinical Practice. Written informed consent was obtained from all participants.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Grünig, E., Rahaghi, F., Elwing, J. et al. Oral Treprostinil is Associated with Improved Survival in FREEDOM-EV and its Open-Label Extension. Adv Ther 41, 618–637 (2024). https://doi.org/10.1007/s12325-023-02711-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-023-02711-x