
Abstract
Introduction
Daily burden of patients with chronic kidney disease (CKD) who have not received maintenance dialysis or renal transplantation has not been well reported compared with patients receiving dialysis. We conducted a patient survey and an advisory board in Japan to investigate the experience and perception of CKD and its treatments from the patient’s perspective.
Methods
An anonymous web survey (n = 342) was conducted in October and November 2020. Participants, who were recruited through multiple panels, aged 20 years or older, diagnosed with any stage of CKD, and who had neither received nor planned maintenance dialysis or renal transplantation were included. A questionnaire prepared under the medical advisor’s guidance was used to collect the background information, burden of disease and treatments, and needs and expectations for future treatments. An advisory board with five patients nominated from a patient group was conducted in December 2020. Additional insights to interpret the results of the preceding survey were collected using pre-identified discussion topics.
Results
Establishing a diagnosis of CKD generally took a long time; approximately 20% of the patients waited more than 5 years before diagnosis. In daily life, patients were burdened with CKD-related symptoms (e.g., tinnitus, leg cramps) and behavioral restrictions, including diet. They also felt psychological burdens, such as concerns about possible future dialysis and/or renal transplantation, lack of awareness and understanding of disease among the other people in their lives, and financial burdens related to medical expenses. Furthermore, they felt a lack of communication in daily interactions with health care professionals and others around them, and they desired interaction with patients with CKD.
Conclusion
Understanding the burdens and the thoughts of patients with CKD could inform discussions about the ways to improve communication with patients in daily practice, the role of the patient community, and new therapeutic options to address patients’ expectations.
Trial Registration
UMIN000042300.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Why carry out this study? |
Patients with chronic kidney disease (CKD) who have not received maintenance dialysis or renal transplantation find it challenging to continue comprehensive treatment and lifestyle management, such as dietary restrictions and exercise. However, compared with patients receiving dialysis, little is known about the burden of patients who have not received dialysis. |
We explored patients’ perceptions and needs captured in a survey (quantitative data), followed by a patient advisory board (qualitative data) to supplement the distinctive trends captured in the preceding survey. |
What was learned from the study? |
This study showed that diagnosis of CKD can take a long time, the patients were bothered by psychological burdens, such as concerns about possible future dialysis and/or renal transplantation, the lack of sufficient understanding of their disease by people around them, and they were stressed by restraints on behavior, including dietary restrictions. |
The participants in this study indicated that improvement of communication in daily interactions with health care professionals and people around them and more opportunities for patient-to-patient communication would reduce patients’ burden and improve patients’ quality of life. |
Digital Features
This article is published with a Japanese translation, to facilitate understanding of the article. To view digital features for this article go to https://doi.org/10.6084/m9.figshare.21603603.
Introduction
Chronic kidney disease (CKD) is characterized by persisting renal impairment and gradual loss of renal function. Approximately 13.3 million people, or 1 in 8 adults, are estimated to have CKD in Japan [1]. CKD can advance to end-stage renal failure, for which dialysis and renal transplantation are usually required [1]. In addition, CKD is a strong risk factor for death and cardiovascular (CV) diseases, such as myocardial infarction, stroke, and heart failure, and the CV risk increases once glomerular filtration rate (GFR) declines [2]. Studies in Japanese patients have also suggested that the risk of developing cardiovascular diseases increases when CKD is complicated with hypertension and heart failure [3].
Treatment of CKD aims to suppress the decline of renal function, delay progression to end-stage renal failure, and prevent the development of cardiovascular diseases [4]. Patients with CKD require comprehensive treatment and management, such as lifestyle modifications; dietary restrictions on calories, salt, and protein intake; and pharmacotherapy for the primary disease, such as hypertension and diabetes [1, 4, 5]. Furthermore, with progressive decline of renal function, treatment of complications, such as anemia and hyperkalemia, is needed, which adds to the burden associated with CKD treatment. Previous reports have shown that CKD reduces patients’ quality of life and imposes financial burdens associated with treatment or improvement of lifestyle [6, 7]. However, to date, the burden and difficulties faced by patients with CKD who are not receiving maintenance dialysis or renal transplantation are not well reported.
The purpose of this study was to understand the experiences and perceptions of the disease and its treatment in patients with any stage of CKD who have not received maintenance dialysis or renal transplantation. We took a sequential two-stage approach in this study; quantitative data were initially collected using a survey to assess patient perception and needs, after which patient insight and real-life wisdom (qualitative data) were generated through a patient advisory board to supplement the distinctive trends captured in the preceding survey.
Methods
Study Design and Study Method
This is a cross-sectional study using quantitative research (survey) and qualitative research (advisory board). It was conducted in accordance with ethical principles based on the Declaration of Helsinki and in compliance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects (dated December 22, 2014, partially revised on February 28, 2017). Prior to implementation of the study, the study protocol was approved by the Clinical Research Ethics Committee of Medical Corporation Kyosokai AMC Nishi-Umeda Clinic. The study is registered in the UMIN Clinical Trials Registry (UMIN000042300).
Survey
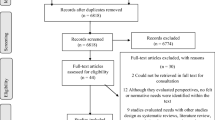
The survey was an anonymous web-based questionnaire administered by QLife, Inc. (Tokyo, Japan), a medical market research company, on behalf of Nippon Boehringer Ingelheim. The survey was conducted on a limited number of days (October 30 to November 6, 2020 and November 25 to 26, 2020) to eliminate the possibility of duplicate responses from a single survey participant accessing the survey from multiple panels. The participants were recruited through multiple panels, including Rakuten Insight, Jinlab (a patient community run by a patient group), Motto-Oishii-Jinzobyosyoku (a website that provides information about renal disease diet), Volunteer Bank, and others (Fig. 1). Prior to the start of this study, the study information for participants was posted on the survey website. Participants could voluntarily consent to participate in this study after reading the study information.

Breakdown of survey participants. aOne patient did not meet two eligibility criteria (age [≥ 20 years] and diagnosis of CKD); bExcluded at the data cleaning stage for their responses indicating that they did not meet the eligibility criteria; cRakuten Insight: an internet research company with a large panel (https://insight.rakuten.co.jp/). The questionnaire was delivered to 615 people who responded as having CKD in the attribute survey that was independently conducted by Rakuten Insight in January 2020 for their panel members; dJinlab: a web-based patient community (https://www.jinlab.jp/) that publishes information about kidney diseases and dialysis. The URL for the questionnaire was posted on the official website of Jinlab (approximately 2500 followers) and on the Twitter account of Mr. Takeshi Shukunobe (approximately 2000 followers), who is a representative of PPeCC, Inc. (which operates Jinlab) and a dialysis patient; eMotto-Oishii-Jinzobyosyoku: a medical media website that regularly posts articles on how to eat and enjoy kidney disease diets (https://www.kidney-journey.com/). An article announcing the survey and the URL of the questionnaire was posted on the website. The URL of the aforementioned article was posted on the Twitter account of the operator of Motto-Oishii-Jinzobyosyoku (approximately 900 followers) and a patient with CKD; fVolunteer Bank (currently QLife Clinical Research Monitor operated by QLife, Inc.; https://join.qlife.jp/): a clinical trial volunteer site with 580,000 registered users. Approximately 10% of the members have provided their attribute information, and the questionnaire was distributed to 3210 members whose attributes were listed as “diabetes mellitus” (related to CKD) in the attribute information; gOther: answered the web questionnaire from other than above. Details are unknown but includes participants who saw the retweet of Jinlab’s post on Twitter and participants who were referred by acquaintances with CKD. CKD chronic kidney disease, IgA immunoglobulin A
Survey participants were those aged 20 years or older with a self-reported diagnosis of CKD of any stage who had not received maintenance dialysis (hemodialysis or peritoneal dialysis) or renal transplantation (not scheduled). The eligibility criteria were confirmed on the basis of the information reported by the patient on the website (Fig. 1).
In the survey, 32 questions were formulated under the guidance of a medical advisor to quantitatively assess patients’ backgrounds, experiences and awareness of the disease and treatment, daily burdens, and future treatment needs and expectations (Table S1 in the electronic supplementary material). Of the survey participants who did not have Rakuten membership, 100 participants were chosen through a raffle to receive an Amazon gift certificate equivalent to 1000 yen (approximately US $9.62). In addition, all participants who completed the survey through the Rakuten Insight panel received Rakuten points equivalent to 50 yen (approximately US $0.48) if they spent 1 min or longer on the survey site and entered a valid answer.
Advisory Board
The advisory board was conducted online using Zoom (December 6, 2020 [4 h]). Advisory board participants were selected on the basis of a recommendation from a patient group (PPeCC) among the survey participants who were also part of the CKD patient community (Jinlab) run by PPeCC. The sponsor of this study, Nippon Boehringer Ingelheim Co., Ltd., explained the study and obtained informed consent from all participants.
The advisory board was attended by patient participants, a moderator and transcriptionist (both from the market research company Rakuten Insight, Inc.), and two representatives from the study sponsor, Nippon Boehringer Ingelheim Co., Ltd., as observers. Interviews were conducted in Japanese by an experienced third-party moderator. Information necessary to supplement and interpret the results of the survey on pre-specified topics (diagnosis of CKD, current treatment, treatment goals, and obtaining disease information) was collected (Table S2 in the electronic supplementary material).
The interviews were audio-recorded with the consent of the participants, and a transcription was prepared at a later date. Participants in the advisory board were paid 10,000 yen (approximately US $96.15) per hour (4 h) for their attendance.
Analysis Methods
The participants who met the eligibility criteria for the study and whose responses to the questionnaire were valid were included in the survey count. The survey was analyzed by QLife, Inc., and the participants’ backgrounds and the frequency distribution of response data for each question were tabulated using Microsoft Excel.
Information obtained from the advisory board was analyzed qualitatively to interpret the detail of the survey results. Information about participants in the study was identified only by participant ID, and personal information was excluded from the analysis.
The target number of participants was 300 in the survey and six in the advisory board based on recruitment feasibility. No formal statistical approach was adopted in designing this study.
Results
Participant Disposition and Background
Of the 532 participants who accessed the web questionnaire, 342 participants were included in the survey, after exclusion of 190 participants: 184 participants who did not meet the eligibility criteria at screening or at data cleaning and six participants who met the eligibility criteria but did not complete the survey before answering each question (Fig. 1). Most participants were male (67.4%, 196/291 participants) and in their 50s (28.5%, 83/291 participants), followed by those in their 60s (23.7%, 69/291 participants) (Table 1).
Most advisory board participants (4/5 participants) were female (Table 2). The participants’ GFR [4] indicative of CKD stage ranged from G2 (normal or mild decrease, GFR 60–89 mL/min/1.73 m2) to G4 (severe decrease, GFR 15–29 mL/min/1.73 m2) (Table 2).
Diagnosis
Course of Diagnosis
Survey: Approximately 80% of the participants were diagnosed with CKD at the time of routine health check-up or treatment for other disease. Approximately 60% of the participants were diagnosed with CKD by a nephrologist and approximately 20% by general internists. Although more than half of the participants were diagnosed with CKD within 1 year of the first visit to a physician with symptoms, approximately 20% of the participants waited more than 5 years before they were diagnosed (Table 1). The relatively common pre-existing conditions prior to CKD diagnosis were abnormal renal function (11.4%, 39/341 participants), hypertension (36.2%, 123/340 participants), dyslipidemia (12.1%, 41/340 participants), and diabetes mellitus/impaired glucose tolerance (9.7%, 33/340 participants).
Advisory board: The course leading to the diagnosis of CKD varied; two of the participants had a diagnosis of an intractable disease designated by Ministry of Health, Labour and Welfare (IgA nephropathy and not reported [one patient each]), whereas three patients were diagnosed with CKD as a result of a routine health check-up. Renal biopsy, which is required to clarify the definite underlying cause of CKD, was not performed or was postponed for various reasons, including having only one functioning kidney from birth and a lack of time and resources for the patient to undergo the procedure. In one patient, renal biopsy was repeatedly performed before definitive diagnosis with CKD nearly 14 years after the initial diagnosis.
Emotional Response at the Time of Diagnosis
Survey: At the time of diagnosis of CKD, 70% of the participants felt worried about the future, whereas the remaining 30% did not feel anything in particular or accepted the diagnosis with resignation because it had been expected (Fig. 2).

Emotional response at the time of diagnosis: What did you think when you were diagnosed with chronic kidney disease? IgA immunoglobulin A
Advisory board: Participant perception of the diagnosis varied depending on the participant’s disease course. The following points were raised: the diagnosis was upsetting even if the patient had known that they had a kidney disease; one patient was shocked to know that they were diagnosed with CKD of a variation designated as an intractable disease by the health authority; and one patient felt worried and hopeless thinking about the possible future course of the disease leading to dialysis. In addition, some participants missed the chance to prepare for the disease because they had long remained undiagnosed (Fig. 2).
Treatment
Treatment Characteristics
Survey: Pharmacotherapy and dietary management were the main treatments for CKD before and after the diagnosis. The proportions of participants on these therapies increased post-diagnosis compared with pre-diagnosis (pharmacotherapy, 76.1% [258/339 participants] vs 46.0% [156/339 participants]; dietary management, 46.3% [157/339 participants] vs 18.3% [62/339 participants]). Dietary management was cited by the majority of participants (84.8%, 284/335 participants) as a focal point of self-directed efforts to slow the progression of CKD.
Advisory board: All participants were on some sort of dietary restriction, mainly controlling salt and protein intake. No participant was advised by their physician to limit fluid intake, and nor were they practicing it (Table 2). For exercise therapy, two participants were undertaking “renal rehabilitation” created by Tohoku University [8, 9].
Treatment Satisfaction
Survey: In response to the question asking about satisfaction with current treatment, 44.8% (152/339 participants) and 18.0% (61/339 participants) answered in the positive and negative, respectively. The remaining 37.2% (126/339 participants) felt neither satisfied nor unsatisfied.
Advisory board: The reasons for perceived treatment satisfaction were that CKD was not progressing and that relevant biomarkers (e.g., blood pressure and creatinine level) were stable. Reduced financial burden owing to medical expense subsidy for the designated intractable disease was also raised as a factor contributing to satisfaction. The reasons for perceived dissatisfaction with current treatment included a lack of long-term efficacy with some CKD pharmacotherapy, and limited pharmacotherapy options to treat other diseases owing to impaired renal function.
Treatment Goals
Survey: At the start of treatment for CKD, only 14.3% (48/335) of participants were given treatment goals (Fig. 3).

Treatment goals: Are there any treatment goals shared by your physician to start treatment for chronic kidney disease?
Advisory board: Advisory board participants each had varying levels of motivation for receiving CKD treatment. Their perceived treatment goals were also diverse. One thing the participants had in common was that none of them were provided with clear treatment goals for CKD by their attending physicians beyond quantitative laboratory value targets.
Knowledge and Awareness of the Disease and Treatment
Understanding of the Disease
Survey: Approximately two-thirds (65.7%, 224/341) of participants did not know of CKD until they were diagnosed. Most participants gained new information by the diagnosis, primarily about the disease, diet, and treatment (Fig. 4).

Post-diagnosis learning: Have you gotten any new information about chronic kidney disease since you were diagnosed with it? (left); What information have you gotten about chronic kidney disease since you were diagnosed with it? (right; n = 292; multiple answers allowed)
Advisory board: None of the advisory board participants knew about CKD until they were diagnosed. They emphasized that the understanding of CKD is limited and that it is confused with diabetes, which was more recognized.
“People recommended something good for health, but those things are mostly good for diabetic patients or healthy people and are rather bad for kidney disease.”
“I look healthy.... I haven’t told people... about my disease. If I do so, for example, they would worry about me.”
Information About the Disease
Survey: More than half of the survey participants agreed that they have enough information about CKD. The attending physician (76.2%, 260/341 participants) was the most common source of the disease information; the internet (70.1%, 239/341 participants), books (37.5%, 128/341 participants), nurses and nutritionists (19.6%, 67/341 participants), and journals (15.8%, 54/341 participants) followed. However, nearly half of participants thought that they did not have enough information, and many of them wanted to know more about their illness, diet, and treatment (Fig. 5). Approximately 30% of participants wanted more information about medical expenses (Fig. 5).

Disease information: Do you think you have enough information about chronic kidney disease? (left); What information would you like to know about chronic kidney disease? (right; n = 156; multiple answers allowed)
Advisory board: Participants listed physicians, registered dieticians, books and textbooks, patient websites and brochures issued by patient groups, and patient stories (e.g., social networking services [SNS] and video distribution sites) as their daily sources of information on the disease. Participants noted that they carefully examined website content, for example, by consulting a physician. Information that they wanted to know but had not yet obtained included familiar experiences from other patients (e.g., how to engage with work and hospitals, daily living, diet, complications) and clinical symptoms for which appropriate information was not obtained from the attending physician (leg cramps). It was noted that some patients with CKD did not have a positive attitude toward treatment, and for such patients, personalized care must be considered not just with provision of information but, for example, with support of a professional mental counselor or the family, depending on the patient’s background.
Burdens of Disease/Treatment and Support From Others
Burden of Daily Life
Survey: Dietary restriction was the most common burden in daily life, followed by medication/outpatient visit, fluid intake restriction, and exercise restriction (Fig. 6).

Impacts on daily life (burden or concern): What are the impacts of chronic kidney disease on your daily life? (multiple answers allowed)
Advisory board: All participants were on dietary restrictions, such as salt and protein restriction (Table 2). It was suggested that behavioral restrictions, including diet, renal conditions, and restrictions on medication for complications, affect their daily life. In addition to treatment and diet, psychological burdens, such as the following experiences, were noted:
-
Being seen by others as lazy or not trying things enough when it is difficult because of the disease
-
Concealing the fact of having the disease
-
Being expected to do a regular amount of work when it is difficult because of the disease
In addition, the symptoms that contributed to daily burden included tinnitus, leg cramps, hand stiffness, convulsions, sweating, fatigue, and difficulty breathing.
Treatment Support
Survey: Approximately half of the survey participants had no support from others. Among those who had others’ support, a person living with the participant (e.g., family member) was the most common provider of support (84.2%), followed by medical personnel (37.6%) (Fig. 7). More than 90% of participants were not in a patient group; only 6% of the patients participated in a patient group.

Support for treatment: Do you have anyone who helps you with your current treatment? (left); What is your relationship with those who help you with treatment? (right; n = 165; multiple answers allowed)
Advisory board: Most participants were supported by family members. They were involved in a patient community run by a patient group and interacted with other patients with CKD. It was suggested that patients actively interact with each other in a patient community setting, which presumably is accessible.
“I heard what it was like to live with dialysis from other patients and I got a very positive impression of the experience. Until then, I had thought that once I need dialysis, it’s over, but after I heard their stories, I could strongly feel that it’s not so and then I dared to give birth (it means that I decided I could give birth). Thus, I feel it very important to hear such real information, stories of those with actual experience of dialysis.”
“[At a gathering of intractable disease patients] I can get much advice.... Having someone to talk to gives me a kind of emotional support. I’m grateful for that.”
Concerns for the Future
Survey: Dialysis was the most common reason for concern for the future, followed by dietary restriction, financial burden, and renal transplantation (Fig. 8).

Concerns for the future: What are your concerns about chronic kidney disease in the future? (multiple answers allowed)
Advisory board: One advisory board participant stated that they were not so concerned (rather, they were practically minded about their situation) about the future course of the disease; other participants said that they would always be concerned. Despite their concerns being alleviated compared with the time of diagnosis, they were still worried about what would happen to them in the future. Four participants were concerned about when dialysis treatment would be required; all advisory board participants wanted to avoid dialysis mainly because of anticipated restrictions on behaviors and time constraints. They recognized kidney transplantation as an option.
Discussion
As part of recent developments in clinical research, efforts have been made to generate outcomes that are more relevant to patients. Patient and Public Involvement (PPI) is a growing initiative that aims to proactively involve patients and the general public in clinical research. In Europe and the USA, attempts have begun to systematically understand patients’ experiences and perceptions and to incorporate their needs and priorities into the medicines development plan (clinical study plan) and into the marketing authorization review and approval process by health authorities [10, 11]. In Japan, attempts at patient and public involvement have recently materialized with published resources, such as a PPI Guidebook from the Japan Agency for Medical Research and Development [12] and a white paper on patient-centric medicine development [13] from the Japan Pharmaceutical Manufacturers Association. Within the Pharmaceuticals and Medical Devices Agency, an internal guidance on patient engagement was developed in September 2021 [14], signaling the health authority-led exploration of patient participation in Japan. Based on this background, this study was conducted by the study sponsor, in collaboration with physicians and the patient community, and this article was developed with a patient author. The main findings of the study included diversity in CKD disease etiology, background, treatment, and perceived burden, and common unmet needs of patients with CKD for a proper understanding of the disease among others, increased support, and opportunities for patient-to-patient interaction to learn from experiences of those living with CKD.
On the basis of insights gained from survey and advisory board participants, improving patient-to-health care professional (HCP) communication could be a potential driver of reducing the physical and psychological burden of people living with CKD. In the survey, 70% of participants expressed concerns for the future course of the disease when they received a confirmed diagnosis of CKD from their physicians. Some participants in the advisory board also shared their experiences of feeling pessimistic about the future after speaking to their physicians, who provided no evidence-based prognosis of the disease, and implied that the disease is incurable and may lead to dialysis. Other participants reflected upon the time of diagnosis and wished that there had been more optimistic messages on prognosis received from physicians. Miscommunication between a patient with CKD and a physician also existed before a confirmed diagnosis of CKD; although 30% of survey participants were diagnosed with CKD in the process of treating pre-existing non-CKD diseases, an advisory board participant reported having developed mistrust for a physician when their repeated expression of concern about the use of nephrotoxic medication to treat non-CKD diseases was left ignored for a long time.
Regarding treatment goals established through physician–patient communication and agreement, we acknowledge that technical issues in phrasing the question in the survey and advisory board may have caused inaccurate capturing of how goals were established, despite the fact that the questionnaire had been carefully developed with the supervision of a nephrologist who served as an external research advisor to this study. An advisory board participant felt that the term “(treatment) goal” was not appropriate in the context of CKD, given that the currently available CKD treatments aim to prevent the disease from progressing to the dialysis stage, not to cure it, while some participants felt resistance in regarding therapies they were receiving as “treatment” for the same reason. Using the term “treatment goal” may therefore have caused ambiguity on what was being asked among survey participants. Furthermore, the question asked whether a treatment goal was shared by an HCP, thus possibly giving participants the impression that cases where a goal was established through mutual agreement of patient and physician were out of scope. The feedback from the participants to the treatment goal question underscores the importance of the patient and their physician reaching an agreement as to what is meant by “goal” and “treatment” before discussing a specific target. It is also critical to have careful and repeated patient-to-physician communications about setting and updating targets, taking into consideration the patient’s lifestyle and preferences. This requires a two-way commitment—an effort on the physician’s part to improve communication skills with the support of other HCPs, as well as the patient’s willingness to openly discuss and convey their needs to HCPs.
Communication challenges and the needs of patients with CKD have been demonstrated not only with HCPs when patients receive treatment but also with other people in everyday interactions. Participants in the advisory board expressed hesitation in talking about their disease to their friends and people at work after a diagnosis of CKD. As a result, they experienced a situation in which others do not relate to their CKD-driven symptoms (e.g., fatigue) and disease-related dietary restrictions. It was also reported that when the patients talked about the disease, the disease was confused with the more widely recognized disease, diabetes, or that the patients were puzzled by advice from others on dietary management based on incorrect information.
At the root of the communication problem between patients with CKD and non-HCPs is the low awareness of CKD [15] and the lack of knowledge about CKD at the general public level. The survey revealed that just over 30% of the patients knew about CKD prior to diagnosis. After diagnosis, more than half of the patients felt that they obtained sufficient information about the disease via physicians or the internet. Nevertheless, more awareness and education about the disease should be delivered for the public in general, who may not seek information proactively.
Since 2020, a public interest incorporated foundation, the Kidney Foundation in Japan, has been conducting CKD awareness-raising activities through television commercials and posters in train stations [16]. Efforts have been made on a regular basis to increase communication to the general public unfamiliar with CKD. Several CKD disease awareness-raising websites are provided by local governments and pharmaceutical companies. Information provided by pharmaceutical companies should be balanced and from the patient viewpoint; for instance, information about medicines should be understandable to the general public and instructions for medication should consider diversity in lifestyle, as commented by advisory board participants.
The outcome of the survey and the advisory board regarding treatment support and disease information indicated that it was necessary and important for patients with CKD to be connected and communicating with each other. In the survey, approximately half the patients reported receiving no support from others during the course of CKD treatment, whereas the vast majority of the remaining participants were supported by their families. Some participants in the advisory board reported that they had the chance to be connected with other patients via SNS or at their workplace and continued sharing information about the disease and treatment courses with them. There was also an experience of dealing with concerns for the future by staying in contact with dialysis patients through the patient community (Jinlab: https://www.jinlab.jp/), which collaborated on this study, suggesting that the connection between patients plays a mental support role in the continuation of treatment. Helping each other through the patient community, so-called peer support, is not a substitute for treatment but it provides an opportunity to improve quality of life by receiving information on daily living, such as how to deal with diet, work, and regular visits to physicians, and to prevent isolation and continue treatment while learning and seeking advice from other patients with CKD.
While suggesting the importance of interaction between patients, the survey found that only 6% of the patients ever participated in a CKD-related patient group, although the advisory board participants were involved in a patient community run by a patient group. This may be attributed to the absence of a patient group with a primary focus on pre-dialysis CKD. Considering that 70% of patients in this survey obtained information on CKD from the internet and that patients with pre-dialysis CKD are relatively young and have time constraints owing to work and household chores, the value of an online patient community, in which patients can readily participate, will be expected to increase. Concerns about both the credibility of information available on the internet and online slander were raised by advisory board participants who experienced online information gathering and social networking with other patients with CKD. To solve these problems, importantly, an online patient community should be organized on an easily manageable scale and range, with support from people with a variety of expertise.
Strengths and Limitations of the Study
The strength of this study is that a relatively large number of patients with CKD (n = 342) who had not undergone renal transplantation or dialysis completed the survey. The limitations of the study should be noted. First, participants were mainly in their 50s, followed by their 60s, with fewer elderly people aged 70 years or older (nearly 20% of the total). One of the reasons for the relatively low number of elderly participants may be an inherent limitation of web surveys. Second, the study recruited patient participants through specific patient panels. Although multiple patient panels were used, the high likelihood of selection bias has to be recognized. Third, survey responses and comments of advisory board participants about past events are not necessarily based on written records and thus may be affected by recall bias. Finally, it is important to note that the diagnosis of CKD was self-reported by the participants.
Conclusion
A survey for patients with CKD who were not receiving maintenance dialysis or renal transplantation and a group interview in the form of an advisory board that included patients were conducted. The characteristic findings captured in the survey (quantitative data) were complemented by specific examples from the advisory board (qualitative data). By interpreting the patient perspective, we were able to draw conclusions regarding patient perceptions and needs that are more aligned with reality. The results showed that it took time for patients to obtain a diagnosis of CKD, they were bothered by the lack of sufficient understanding by others, and they felt stressed by behavioral restrictions, including dietary restrictions, required for CKD. Patients indicated a lack of communication in daily interactions with HCPs and others around them, and they hoped for more opportunities to interact with other patients with CKD. We hope that understanding the burden and thoughts of patients with CKD, especially those at the pre-dialysis stage, will deepen the understanding of CKD, improve communications with patients in routine medical care, and illustrate the importance and role of patient communities, such as those on social media. In addition, we hope that this information will contribute to improved understanding of patient needs and expectations with new treatments, early diagnosis and treatment initiation, and treatment paths to improve prognosis.
References
The Japanese Society of Nephrology. Evidence-based CKD clinical practice guidelines 2018 [Japanese]. Tokyo: Tokyo Igakusha; 2018.
Matsushita K, van der Velde M, Astor BC, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375:2073–81.
Nakayama M, Sato T, Miyazaki M, et al. Increased risk of cardiovascular events and mortality among non-diabetic chronic kidney disease patients with hypertensive nephropathy: the Gonryo study. Hypertens Res. 2011;34:1106–10.
The Japanese Society of Nephrology. CKD clinical practice guide 2012 [Japanese]. Tokyo: Tokyo Igakusha; 2012.
Ikizler TA, Burrowes JD, Byham-Gray LD, et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am J Kidney Dis. 2020;76:S1–107.
Pergola PE, Pecoits-Filho R, Winkelmayer WC, et al. Economic burden and health-related quality of life associated with current treatments for anaemia in patients with CKD not on dialysis: a systematic review. Pharmacoecon Open. 2019;3:463–78.
Travers K, Martin A, Khankhel Z, Boye KS, Lee LJ. Burden and management of chronic kidney disease in Japan: systematic review of the literature. Int J Nephrol Renovasc Dis. 2013;6:1–13.
Kohzuki M. Kidney disease improves with exercise!: “Kidney Rehabilitation” Developed by Tohoku University [Japanese]. Tokyo: Makino Shuppan; 2019.
Kohzuki M. Renal rehabilitation: chronic kidney disease is a new target of rehabilitation [Japanese]. Jpn Rehabil Med. 2018;55:682–9.
U.S. Food & Drug Administration. FDA Patient-Focused Drug Development Guidance Series for Enhancing the Incorporation of the Patient’s Voice in Medical Product Development and Regulatory Decision Making. https://www.fda.gov/drugs/development-approval-process-drugs/fda-patient-focused-drug-development-guidance-series-enhancing-incorporation-patients-voice-medical. Accessed Jul 13, 2022.
European Medicines Agency. Patients and consumers. https://www.ema.europa.eu/en/partners-networks/patients-consumers. Accessed Jul 13, 2022.
Japan Agency for Medical Research and Development. PPI guidebook [Japanese]. 2019. https://www.amed.go.jp/ppi/guidebook.html. Accessed Jul 13, 2022.
Drug Evaluation Committee (Clinical Evaluation Expert Committee), Japan Pharmaceutical Manufacturers Association. Drug development reflecting the patient’s voice—patient centricity by pharmaceutical companies [Japanese]. 2018. https://www.jpma.or.jp/information/evaluation/results/allotment/lofurc0000005m95-att/patient_centricity.pdf. Accessed Jul 13, 2022.
Patient Involvement Working Group, Pharmaceuticals and Medical Devices Agency. PMDA Patient Involvement Guidance [Japanese]. 2021. https://www.pmda.go.jp/files/000242830.pdf. Accessed Jul 13, 2022.
Yanagisawa N, Miyazaki M, Sato H, Taguma Y, Ito S. Awareness about and educational intervention for chronic kidney disease in the general population: from a survey of participants at the CKD educational lecture in Miyagi prefecture [Japanese]. Jpn J Nephrol. 2014;56:131–7.
The Kidney Foundation Japan. CKD (Chronic Kidney Disease) Management business. http://www.jinzouzaidan.or.jp/jigyou/ckd.html. Accessed Jul 13, 2022.
Acknowledgements
We extend our appreciation for the patients and parties concerned who cooperated in the study. We would also like to extend our appreciation to Ms. Kimiko Mitani, of Nippon Boehringer Ingelheim Co., Ltd., who worked on the project management and drafting of this paper.
Funding
This study was conducted with funding from Nippon Boehringer Ingelheim Co., Ltd. The preparation of this article was supported by Nippon Boehringer Ingelheim Co., Ltd., who funded the cost of the submission and the Rapid Service and Open Access Fees.
Medical Writing, Editorial, and Other Assistance
The writing and submission of this paper was supported by Ms. Hiroko Ebina, of ProScribe KK (Envision Pharma Group), in accordance with Good Publication Practice (GPP3).
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Nobutaka Yagi, Seiichiro Nishimura, and Akira Mima were involved in the planning and design of the study. Nobutaka Yagi and Seiichiro Nishimura contributed to and/or supervised the acquisition and analysis of the data. All authors contributed to the interpretation of the data analysis, revised the manuscript for important intellectual content, and approved the final version for submission.
Disclosures
The authors, Nobutaka Yagi and Seiichiro Nishimura, are employees of Nippon Boehringer Ingelheim Co., Ltd. Akira Mima has received lecture fees and consulting fees from Nippon Boehringer Ingelheim Co., Ltd. PPeCC, Inc., a general incorporated association operated by Takeshi Shukunobe, has received consulting fees and grants for their patient advocacy initiatives from Nippon Boehringer Ingelheim Co., Ltd.
Compliance with Ethics Guidelines
This research was conducted in accordance with ethical principles based on the Declaration of Helsinki and is in compliance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects (dated December 22, 2014, partially revised on February 28, 2017). Prior to implementation of this study, the research plan was approved by the Clinical Research Ethics Committee of Medical Corporation Kyosokai AMC Nishi-Umeda Clinic.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding authors, Akira Mima and Nobutaka Yagi, on reasonable request.
Author information
Authors and Affiliations
Corresponding authors
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Yagi, N., Shukunobe, T., Nishimura, S. et al. Experience and Daily Burden of Patients with Chronic Kidney Disease Not Receiving Maintenance Dialysis or Renal Transplantation. Adv Ther 40, 853–868 (2023). https://doi.org/10.1007/s12325-022-02341-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-022-02341-9