
Abstract
Introduction
Sodium glucose co-transporter 2 inhibitors decrease hemoglobin A1c (HbA1c) and blood pressure (BP) and slightly increase low-density lipoprotein cholesterol (LDL-C) in patients with type 2 diabetes mellitus (T2DM). The effects of baseline BP and LDL-C on the safety and efficacy of canagliflozin in patients were analyzed post hoc in a phase III study.
Methods
Japanese patients with T2DM were classified by baseline systolic BP (SBP) of <130 or ≥130 mmHg, diastolic BP (DBP) of <80 or ≥80 mmHg, and LDL-C of <120 or ≥120 mg/dL. Canagliflozin was administered daily to patients for 52 weeks at doses of either 100 mg (n = 584) or 200 mg (n = 715). The effects of canagliflozin on the incidence of adverse events (AEs), BP, and LDL-C were evaluated.
Results
No clear differences were observed in overall safety among the subgroups classified by baseline SBP, DBP, or LDL-C, except for a slight imbalance in AEs associated with volume depletion with 200 mg of canagliflozin. The decrease in mean SBP and DBP was evident in subgroups with baseline SBP ≥130 mmHg and DBP ≥80 mmHg. Mean LDL-C was decreased in subgroups with baseline LDL-C ≥120 mg/dL at both canagliflozin doses, and they were slightly increased, but did not exceed 120 mg/dL in subgroups with baseline LDL-C <120 mg/dL. The changes in HbA1c and body weight from those observed at baseline were not different between subgroups classified by SBP, DBP, and LDL-C at either dose.
Conclusion
The present post hoc analysis indicates that canagliflozin is well tolerated irrespective of baseline BP and LDL-C in patients with T2DM.
Trial registration
ClinicalTrials.gov identifier, NCT01387737.
Funding
Mitsubishi Tanabe Pharma Corporation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Patients with type 2 diabetes mellitus (T2DM) often have comorbid hypertension and hypercholesterolemia. Comorbidities of these diseases synergistically increase the incidence rates of cerebrovascular and coronary heart diseases [1–4]. Integrated control of body weight, blood pressure (BP), and serum lipids in addition to blood glucose is essential for the treatment of diabetic patients to decrease the risk of cardiovascular (CV) events [5–7], because the goal of diabetes treatment is to improve quality of life and life span of diabetic patients to the same level as those of non-diabetics [8]. Sodium glucose co-transporter 2 (SGLT2) inhibitors are anti-diabetic agents that correct hyperglycemia by promoting urinary glucose excretion through the inhibition of glucose reabsorption in proximal tubules irrespective of the patient’s insulin secretory capacity or insulin resistance. Because this underlying pharmacological mechanism is novel and clearly different from that of existing drugs, SGLT2 inhibitors may present a new treatment option for T2DM.
In various clinical trials in patients with T2DM, administration of SGLT2 inhibitors, including canagliflozin, resulted in a sustained decrease in hemoglobin A1c (HbA1c), body weights, and BP for long periods [9–14]. Recently, in the EMPA-REG OUTCOME trial (ClinicalTrials.gov identifier, NCT01131676), empagliflozin significantly reduced the rate of primary composite CV outcome and of death from any cause in patients with T2DM at high CV risk [15]. It was the first evidence to assess the effects of SGLT2 inhibitor on CV outcome. The mechanisms behind the CV benefits of empagliflozin are multidimensional and involve established changes, such as decreasing HbA1c, losing body weight and lowering BP. On the other hand, BP-lowering effects of SGLT2 inhibitors may be mediated at least partly by its diuretic effect, and there is a concern of the risk of dehydration and hypotension. It has been reported that SGLT2 inhibitors increase low-density lipoprotein cholesterol (LDL-C) as a class effect [16, 17]. Although small increase in high-density lipoprotein cholesterol (HDL-C) was also observed in patients with T2DM, increase in LDL-C raises concerns of a CV risk [10].
Therefore, we investigated the influence of different baseline BPs and LDL-C (as CV risk factors) on the safety and efficacy of canagliflozin by post hoc analysis of data in a 52-week phase III study [13] in Japanese patients with T2DM.
Methods
Study Design and Patient Population
The present post hoc subgroup analyses were conducted using the data obtained in a phase III study of canagliflozin in Japanese patients with T2DM (multicenter, open-label, and long-term administration) [13]. In this clinical study, canagliflozin was administered once daily for 52 weeks at 100 or 200 mg as monotherapy or as add-on therapy to other oral antihyperglycemic drugs (sulfonylurea, glinide, α-glucosidase inhibitor, biguanide, thiazolidinedione, or dipeptidylpeptidase-4 inhibitor). The study was conducted in patients with T2DM whose blood glucose was inadequately controlled with diet/exercise therapy alone or in combination with an oral antihyperglycemic drug for more than 12 weeks before screening. The complete inclusion and exclusion criteria are described in the original report [13]. The main inclusion criteria were (1) patients ≥20 years of age, (2) diagnosis of T2DM at least 3 months before the screening, and (3) HbA1c of ≥7.0% and ≤10.0% in monotherapy and of ≥7.0% and ≤10.6% in combination therapy. The main exclusion criteria were (1) systolic BP (SBP) of ≥160 mmHg and diastolic BP (DBP) of ≥100 mmHg during the run-in period, (2) estimated glomerular filtration rate (eGFR) of <50 mL/min/1.73 m2 at the beginning of the run-in period, (3) urinary albumin-to-creatinine ratios of ≥300 mg/g creatinine, and (4) triglyceride of ≥600 mg/dL on the screening day.
This clinical study was conducted in compliance with Guideline for Good Clinical Practice and the Pharmaceutical Affairs Law in Japan. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all patients for being included in the study. This study is registered on ClinicalTrials.gov, identifier NCT01387737.
In the present analyses, patients were classified into subgroups according to their baseline BP or LDL-C: patients with baseline SBP <130 mmHg (S < 130) and SBP ≥130 mmHg (S ≥ 130), patients with DBP <80 mmHg (D < 80) and DBP ≥80 mmHg (D ≥ 80), and patients with LDL-C <120 mg/dL (L < 120) and LDL-C ≥120 mg/dL (L ≥ 120). SBP <130 mmHg, DBP <80 mmHg, and LDL-C <120 mg/dL are the control target levels for SBP, DBP, and LDL-C in Evidence-based Practice Guideline for the Treatment for Diabetes in Japan 2013 [8].
Assessments
Safety
Adverse events (AEs) were recorded throughout the study, as described in the original report [13], and the results for each subgroup are presented in this report. AEs were classified according to the System Organ Class and preferred term of MedDRA/J version 15.1 (Japanese Maintenance Organization, Tokyo, Japan). Drug-related AEs were defined as AEs in which a causal relationship with canagliflozin was not denied. We also evaluated the change of laboratory variables from baseline to week 52 (hemoglobin, hematocrit, aspartate transaminase (AST), alanine transaminase (ALT), γ-glutamyltranspeptidase (γGTP), blood urea nitrogen (BUN), Na, K, Cl, Ca, Mg, and inorganic phosphate; eGFR; and heart rate) in each subgroup.
Efficacy
Changes in HbA1c, fasting plasma glucose (FPG), and body weight from baseline to week 52 were assessed in each subgroup. The changes in SBP or DBP over the treatment period with the study drug and the change from baseline at week 52 were evaluated in each subgroup according to SBP or DBP categories. In addition, the proportion of patients whose SBP decreased to <130 mmHg and those in whom DBP decreased to <80 mmHg were determined in original S ≥ 130 and D ≥ 80 groups, respectively.
The changes in lipid parameters such as LDL-C, triglyceride, HDL-C, and LDL-C/HDL-C from baseline to week 52 and the changes in LDL-C over the treatment period with the study drug were assessed in each LDL-C subgroup. LDL-C was quantified using the direct method.
Statistical Analysis
All the analyses were conducted for both doses of canagliflozin. Safety analyses were performed in the safety analysis set (N = 1299), which comprised all patients excluding those who did not receive a dose of canagliflozin or who lacked safety data after starting the study drug. AEs were summarized as the number and percentage of patients with AEs. Laboratory variables were shown as the mean ± standard deviation (SD) for the change from the baseline to week 52. Only patients with data at both baseline and week 52 or the relevant visit were included in the analyses of safety variables. Statistical analyses were not performed on the safety and laboratory variables between the subgroups.
Efficacy analyses were performed in the full analysis set (N = 1297), which comprised all allocated patients, excluding those without T2DM, those not receiving a dose of the study drug, or those for whom efficacy data after starting the study drug administration was absent. The last observation carried forward method was used to impute missing data at week 52. The changes in HbA1c, FPG, body weight, SBP, DBP, LDL-C, triglyceride, HDL-C, and LDL-C/HDL-C from baseline to week 52 were analyzed using the one-sample t test. All statistical tests were performed two-sided at a 5% significance level. For all statistical analysis, SAS ver. 9.2 (SAS Institute Inc., Cary, NC, USA) was used.
Results
Analysis in Subgroups Classified by Baseline BP
Patient characteristics of subgroups classified by baseline BP are shown in Table 1. In patients treated with 100 or 200 mg canagliflozin, the number of patients in the S < 130 subgroup was almost the same as that in the S ≥ 130 subgroup and the number of patients in the D < 80 subgroup was slightly larger than that of the D ≥ 80 subgroup.
Table 2 summarizes the incidence rates of AEs. We have focused on AEs with ≥2 times difference in the incidence rate between subgroups. No clear difference was observed in the incidence rate of total AEs between subgroups classified by baseline SBP and DBP at both doses of canagliflozin. There were no clear differences in the incidence rates of serious AEs (SAEs) between subgroups in the 100 mg treated group. Whereas a higher incidence rate of SAEs was observed in S ≥ 130 subgroup at the 200 mg dose, the frequency of drug-related SAEs was low and similar between S ≥ 130 and S < 130 subgroups [see Table S1 in the electronic supplementary material (ESM)]. The frequency of AEs leading to study discontinuation was low among subgroups. There was a difference in the incidence rates of urinary tract infection between the subgroups at 200 mg canagliflozin dose. The frequencies of urinary tract infection-related AEs were 4.0% and 0.3% in S < 130 and S ≥ 130 subgroups, respectively, and 3.5% and 0.6% in D < 80 and D ≥ 80 subgroups, respectively.
The incidence rate of volume depletion-related AEs was similar across subgroups at the 100 mg dose. In contrast, there was an imbalance in the AE incidences between subgroups classified by SBP and DBP at the 200 mg dose. The frequency of AEs was 2.9% and 1.2% in S < 130 and S ≥ 130 subgroups, respectively, and 2.8% and 1.3% in D < 80 and D ≥ 80 subgroups, respectively.
Volume depletion-related AEs occurred in 15 patients receiving the 200 mg dose. Of these, eight had mild postural dizziness: seven patients with postural dizziness were in the S < 130 and D < 80 subgroups. Four had mild or moderate dehydration: two patients were with S < 130 and D < 80 and two patients were with S ≥ 130 or D ≥ 80 subgroups (data not shown).
The incidence of other AEs including hypoglycemia (including both symptomatic and asymptomatic hypoglycemia), genital infections, osmotic diuresis, and skin and subcutaneous tissue disorders was similar across subgroups. The incidence rate of CV-related AEs was also similar between subgroups at both doses, and moderate lacunar infarction and mild increase of creatine phosphokinase occurred in one event each at 100 and 200 mg, respectively, and were classified as drug-related CV events.
Changes in laboratory variables from baseline to week 52 were similar across subgroups (see Table S2 in the ESM). Hematocrit and BUN increased across subgroups. No changes from baseline in electrolytes (Na, K, Cl, Ca, Mg, and inorganic phosphate) and heart rate were observed in any subgroups at both canagliflozin doses.
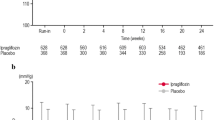
HbA1c, FPG and body weight were significantly decreased from baseline to week 52 of treatment with canagliflozin in all subgroups (Table 3). The decreases in mean SBP and DBP from the baseline at 52 weeks were larger in S ≥ 130 and D ≥ 80 subgroups than those in S < 130 and D < 80 subgroups, respectively (Table 3). The decreases in mean SBP and DBP in S ≥ 130 and D ≥ 80 subgroups were sustained from 4 to 52 weeks after administration of canagliflozin at both doses (Fig. 1; Table 3). In S ≥ 130 subgroups, the proportions of patients whose SBP decreased to <130 mmHg were 43.6% and 57.1% after the 52-week administration at 100 mg and 200 mg doses, respectively. In D ≥ 80 subgroups, the proportions of patients whose DBP decreased to <80 mmHg were also 42.0% and 47.3% at 100 and 200 mg doses, respectively. The BP-lowering effect of canagliflozin was not affected by combined treatment of antihypertensive agents at baseline (data not shown).

Changes in SBP (a) and DBP (b) over time in subgroups classified by BP. Each point and bar represent mean and standard deviation, respectively. BP blood pressure, DBP diastolic blood pressure, SBP systolic blood pressure
Analysis in Subgroups Classified by Baseline LDL-C
Patient characteristics of subgroups classified by baseline LDL-C are shown in Table 4. The number of patients was almost the same in each subgroup.
Table 2 summarizes the AEs in each subgroup. No differences were observed in the incidence rate of total AEs and SAEs in both subgroups at either dose of canagliflozin. No differences were observed in the incidence rate of AEs resulting in study discontinuation. The frequency of female genital infection in AEs was 7.0% and 15.1% in L < 120 subgroup and L ≥ 120 subgroup at the 200 mg dose, respectively, whereas it was similar between L < 120 and L ≥ 120 subgroups at the 100 mg dose (Table 2).
Of 15 patients with volume depletion-related AEs at the 200 mg dose, 12 and 3 were in L < 120 and L ≥ 120 subgroups, respectively. Of the 12 volume depletion-related AEs in the L < 120 subgroup, 7 had mild postural dizziness and 4 had dehydration (data not shown).
No clear differences were observed in the incidence rates of other AEs and drug-related AEs between the subgroups classified by baseline LDL-C (Table 2 and Table S1). Changes of laboratory variables from baseline to week 52 were similar between subgroups at both doses of canagliflozin (see Table S3 in the ESM).
HbA1c, FPG, and body weight significantly decreased from baseline to week 52 of treatment with canagliflozin in both subgroups (Table 5). In L <120 subgroup, LDL-C slightly increased but did not exceed 120 mg/dL after a 52-week administration of either dose (Table 5; Fig. 2). This LDL-C increase was maintained until week 52. On the other hand, LDL-C in L ≥ 120 subgroup slightly decreased from baseline after administrations of canagliflozin at both doses (Table 5). Triglyceride decreased from baseline to week 52, except for L < 120 subgroup at the 100 mg dose. HDL-C increased after the 52-week administration to a similar extent in these subgroups. LDL-C/HDL-C was unchanged in L < 120 subgroup, but it slightly decreased in L ≥ 120 subgroup at both canagliflozin doses.

Change in LDL-C over time in subgroups classified by LDL-C. Each point and bar represent mean and standard deviation, respectively. LDL-C low-density lipoprotein cholesterol
Discussion
Hypertension and hypercholesterolemia are common comorbid conditions in many patients with T2DM [18], and canagliflozin affects BP and lipid parameters. Therefore, in this report, we examined the safety and efficacy of canagliflozin in post hoc subgroup analyses in which patients were classified subgroups of different baseline of BP and LDL-C using data from a 52-week randomized open-label study in Japanese patients with T2DM [13]. In the present subgroup analyses, the total incidence of AEs and drug-related AEs was not generally different between BP and LDL-C subgroups. There were some imbalances in incidence rates of AEs between the subgroups according to SBP, DBP, or LDL-C at the 200 mg dose. The incidence rate of urinary tract infections or volume depletion-related AEs was frequent in S < 130 and D < 80 subgroups at 200 mg dose. In the LDL-C subgroup analysis, occurrence of volume depletion-related or female genital infection-related AEs was frequent in the L < 120 or L ≥ 120 subgroups, respectively, at the 200 mg dose. However, AEs related to urinary tract infections, volume depletion, or female genital infections occurred with other SGLT2 inhibitors at an incidence rate of approximately 0–7.4%, 0–4.4%, or 0–22.2%, respectively [19–25]. Therefore, the incident rates of canagliflozin-associated AEs in this study were within the expected range for SGLT2 inhibitors. The reasons for the difference in the incidence of urinary infections or female genital infection-related AEs between subgroups at 200 mg doses are unknown, and there is no evidence which have shown the association between urinary tract infections and BP, or between female genital infections and LDL-C.
The incidence of volume depletion-related AEs was evident at 200 mg, particularly in the S < 130, D < 80, and L < 120 subgroups. Baseline characteristics of 15 patients with volume depletion-related AEs were age of 38–72 years old and eGFR of 62–104 mL/min/1.73 m2. No patients received loop diuretics and the time to the first AEs varied over the study period. Eight of 15 patients were with SBP <130 mmHg and LDL-C <120 mg/dL and 8 patients were with DBP <80 mmHg and LDL-C <120 mg/dL. On the other hand, volume depletion-related AEs did not occur in patients with SBP ≥130 mmHg and LDL-C ≥120 mg/dL. The reason for the high frequency of volume depletion-related AEs in the patients in the lower BP or LDL-C subgroups at 200 mg dose is unclear. With regard to BP, it is possible that the patients with volume depletion-related AEs in the lower BP subgroups might be susceptible to the diuretic effects of canagliflozin; however, there were insufficient data to discuss this. A previous study has shown that canagliflozin increased the incidence rate of volume depletion in elderly patients (>75 years old), patients with eGFR <60 mL/min/1.73 m2, and those on diuretic therapy [26], which do not correspond to the baseline characteristics of the patients with volume depletion-related AEs in the present study. Although volume depletion should be carefully considered in elderly patients, patients with renal impairment, and those receiving loop diuretic therapies, the severity of the volume depletion-related AEs was mild in the patients in the present study.
Efficacy was similar in the overall group and subgroups, except for BP in the SBP and DBP subgroups and lipid profiles in the LDL-C subgroups. In overall patients, canagliflozin slightly reduced SBP and DBP from baseline. The changes in SBP and DBP from baseline were evident in the S ≥ 130 subgroups after starting treatment with canagliflozin at the 100 mg and 200 mg doses. These results are consistent with a report of more evident decreases in mean BP with SBP ≥140 mmHg than in the overall population after a 26-week administration of canagliflozin [27]. In the S ≥ 130 and D ≥ 80 subgroups at both doses, >40% of patients achieved SBP <130 mmHg and DBP <80 mmHg at 52 weeks. In addition, the BP-lowering effect of canagliflozin was independent of combined treatment with antihypertensive agents at baseline. According to the guidelines for treatment of T2DM, the target level of BP control is SBP <130 mmHg and DBP <80 mmHg in patients with diabetes [8]. Therefore, the results indicate that canagliflozin is beneficial in the treatment of patients with T2DM with hypertension.
Although there were no changes in LDL-C in the overall patients, LDL-C over those observed at baseline increased in the L < 120 subgroups and decreased in the L ≥ 120 subgroup at both 100 and 200 mg canagliflozin. The present study, baseline LDL-C in the L < 120 subgroups at both 100 and 200 mg canagliflozin were 97.5 and 99.1 mg/dL, respectively, was consistent with previous reports: dapagliflozin or empagliflozin increased LDL-C in patients with baseline LDL-C between 90 and 110 mg/dL [16]. The change in LDL-C was observed at 4 weeks of initiation of treatment although the mean LDL-C did not reach 120 mg/dL throughout the treatment period. HDL-C in the overall, L < 120, and L ≥ 120 subgroups similarly increased. The triglyceride were decreased in the overall and L ≥ 120 subgroup at the 100 mg dose and the overall, L ≥ 120, and L < 120 subgroups at the 200 mg dose. The effects of canagliflozin on lipid metabolism may be mediated through urinary caloric loss by SGLT2 inhibition. Although further investigation is necessary to clarify the mechanism on lipid metabolism, it should be stressed that canagliflozin did not increase the risk of LDL-C elevation in L ≥ 120 subgroup. Indeed, empagliflozin was associated with small increases in LDL-C in the EMPA-REG OUTCOME trial; however, CV risk was reduced in the empagliflozin treated group, as compared with placebo group [15].
The limitations of the study are described as follows: (1) this 52-week study was conducted in an open-label manner and the present results are derived from post hoc sub-analyses of the original data and (2) the study scale and treatment period were insufficient to evaluate risks of CV events for antidiabetic agents. To assess the effect of canagliflozin on the CV risk, the CANVAS (CANagliflozin cardioVascular Assessment Study; ClincalTrials.gov identifier, NCT01032629) clinical trial is now in progress in patients with high risk of heart diseases [28]. The effects of SGLT2 inhibitors on the risk of CV events should be further evaluated.
Conclusions
This post hoc analysis indicates that canagliflozin at 100 and 200 mg reduces HbA1c, FPG, body weight, and triglyceride, and increases HDL-C across subgroups classified according to baseline SBP, DBP, and LDL-C in a 52-week phase III study in Japanese patients with T2DM. Reduction in BP was evident in S ≥ 130 and D ≥ 80 subgroups. LDL-C was decreased in the L ≥ 120 subgroup and was slightly increased but did not exceed 120 mg/dL in the L < 120 subgroup. No clear differences were observed in overall safety among the subgroups except for a slight difference in AEs associated with volume depletion, mainly postural dizziness, with 200 mg of canagliflozin. Therefore, canagliflozin is well tolerated irrespective of baseline BP and LDL-C in patients with T2DM.
References
Stamler J, Vaccaro O, Neaton JD, Wentworth D. Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the Multiple Risk Factor Intervention Trial. Diabetes Care. 1993;16:434–44.
Sone H, Katagiri A, Ishibashi S, et al. Effects of lifestyle modifications on patients with type 2 diabetes: the Japan Diabetes Complications Study (JDCS) study design, baseline analysis and three year-interim report. Horm Metab Res. 2002;34:509–15.
Oikawa S, Kita T, Mabuchi H, et al. Risk of coronary events in Japanese patients with both hypercholesterolemia and type 2 diabetes mellitus on low-dose simvastatin therapy: implication from Japan Lipid Intervention Trial (J-LIT). Atherosclerosis. 2007;191:440–6.
American Diabetes Association. Role of cardiovascular risk factors in prevention and treatment of macrovascular disease in diabetes. Diabetes Care. 1989;12:573–9.
Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358:580–91.
UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ. 1998;317:703–13.
American Diabetes Association. Standards of medical care in diabetes—2015: summary of revisions. Diabetes Care. 2015;38:S4.
The Japan Diabetes Society. Evidence-based Practice Guideline for the Treatment for Diabetes in Japan. http://www.jds.or.jp/modules/en/index.php?content_id=44. 2013. Accessed 30 Oct 2015.
Stenlof K, Cefalu WT, Kim KA, et al. Efficacy and safety of canagliflozin monotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise. Diabetes Obes Metab. 2013;15:372–82.
Cefalu WT, Leiter LA, Yoon KH, et al. Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial. Lancet. 2013;382:941–50.
Leiter LA, Yoon KH, Arias P, et al. Canagliflozin provides durable glycemic improvements and body weight reduction over 104 weeks versus glimepiride in patients with type 2 diabetes on metformin: a randomized, double-blind, phase 3 study. Diabetes Care. 2015;38:355–64.
Lavalle-Gonzalez FJ, Januszewicz A, Davidson J, et al. Efficacy and safety of canagliflozin compared with placebo and sitagliptin in patients with type 2 diabetes on background metformin monotherapy: a randomised trial. Diabetologia. 2013;56:2582–92.
Inagaki N, Kondo K, Yoshinari T, Kuki H. Efficacy and safety of canagliflozin alone or as add-on to other oral antihyperglycemic drugs in Japanese patients with type 2 diabetes: a 52-week open-label study. J Diabetes Investig. 2015;6:210–8.
Inagaki N, Kondo K, Yoshinari T, Takahashi N, Susuta Y, Kuki H. Efficacy and safety of canagliflozin monotherapy in Japanese patients with type 2 diabetes inadequately controlled with diet and exercise: a 24-week, randomized, double-blind, placebo-controlled, Phase III study. Expert Opin Pharmacother. 2014;15:1501–15.
Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;15:1501–15. doi:10.1056/NEJMoa1504720.
Halimi S, Verges B. Adverse effects and safety of SGLT-2 inhibitors. Diabetes Metab. 2014;40:S28–34.
Inzucchi SE, Zinman B, Wanner C, et al. SGLT-2 inhibitors and cardiovascular risk: proposed pathways and review of ongoing outcome trials. Diab Vasc Dis Res. 2015;12:90–100.
Center for Disaese Control and Prevention. National diabetes statics report. 2014. http://www.cdc.gov/diabetes/pubs/statsreport14/national-diabetes-report-web.pdf.
Kaku K, Maegawa H, Tanizawa Y, et al. Dapagliflozin as monotherapy or combination therapy in Japanese patients with type 2 diabetes: an open-label study. Diabetes Ther. 2014;5:415–33.
Araki E, Tanizawa Y, Tanaka Y, et al. Long-term treatment with empagliflozin as add-on to oral antidiabetes therapy in Japanese patients with type 2 diabetes mellitus. Diabetes Obes Metab. 2015;17:665–74.
Tanizawa Y, Kaku K, Araki E, et al. Long-term safety and efficacy of tofogliflozin, a selective inhibitor of sodium–glucose cotransporter 2, as monotherapy or in combination with other oral antidiabetic agents in Japanese patients with type 2 diabetes mellitus: multicenter, open-label, randomized controlled trials. Expert Opin Pharmacother. 2014;15:749–66.
Ikeda S, Takano Y, Cynshi O, et al. A novel and selective sodium–glucose cotransporter-2 inhibitor, tofogliflozin, improves glycaemic control and lowers body weight in patients with type 2 diabetes mellitus. Diabetes Obes Metab. 2015. doi:10.1111/dom.12538.
Seino Y, Kaku K, Inagaki N, et al. Fifty-two-week long-term clinical study of luseogliflozin as monotherapy in Japanese patients with type 2 diabetes mellitus inadequately controlled with diet and exercise. Endocr J. 2015;62:593–603.
Seino Y, Inagaki N, Haneda M, et al. Efficacy and safety of luseogliflozin added to various oral antidiabetic drugs in Japanese patients with type 2 diabetes mellitus. J Diabetes Investig. 2015;6:443–53.
Kadowaki T, Haneda M, Inagaki N, et al. Efficacy and safety of empagliflozin monotherapy for 52 weeks in Japanese patients with type 2 diabetes: a randomized, double-blind, parallel-group study. Adv Ther. 2015;32:306–18.
Mikhail N. Safety of canagliflozin in patients with type 2 diabetes. Curr Drug Saf. 2014;9:127–32.
Weir MR, Januszewicz A, Gilbert RE, et al. Effect of canagliflozin on blood pressure and adverse events related to osmotic diuresis and reduced intravascular volume in patients with type 2 diabetes mellitus. J Clin Hypertens (Greenwich). 2014;16:875–82.
Neal B, Perkovic V, de Zeeuw D, et al. Rationale, design, and baseline characteristics of the Canagliflozin Cardiovascular Assessment Study (CANVAS)—a randomized placebo-controlled trial. Am Heart J. 2013;166:217–223.e211.
Acknowledgments
This study was funded by Mitsubishi Tanabe Pharma Corp. The article processing charges and open access fee for this publication were funded by Mitsubishi Tanabe Pharma Corp. The authors thank to Dr. A. Saito, of Tanabe R&D service Co., Ltd., for providing editorial support, which was funded by Mitsubishi Tanabe Pharma Corp. The authors thank Ms. K. Sasaki for insightful discussions. The authors thank all investigators, study team, and patients for participating in this study. Canagliflozin was developed by Mitsubishi Tanabe Pharma Corp. in collaboration with Janssen Research and Development, LLC. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Disclosures
N. Inagaki has received consulting fees and research support from Mitsubishi Tanabe Pharma Corp., and has served on speakers bureaus for Mitsubishi Tanabe Pharma Corp. He has also received consulting fees and/or research support from Astellas Pharma Inc., AstraZeneca K.K., Bristol-Myers K.K., Chugai Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., Eisai Co., Ltd., Eli Lilly Japan K.K., GlaxoSmithKline K.K., Japan Tobacco Inc., Kissei Pharmaceutical Co., Ltd., Kyowa Hakko Kirin Co., Ltd., MSD K.K., Nippon Boehringer Ingelheim Co., Ltd., Nipro Corporation, Novartis Pharma K.K., Novo Nordisk Pharma Ltd., Ono Pharmaceutical Co., Ltd., Pfizer Japan Inc., Roche Diagnostics K.K., Sanofi K.K., Sanwa Kagaku Kenkyusho Co., Ltd., Shionogi and Co., Ltd., Shiratori Pharmaceutical Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Taisho Pharmaceutical Co., Ltd., and Takeda Pharmaceutical Co., Ltd., Terumo Corporation, and Tsumura and Co.; and has served on speakers bureaus for ARKRAY, Inc., Astellas Pharma Inc., AstraZeneca K.K., Bayer Yakuhin, Ltd., Daiichi Sankyo Co., Ltd., Eisai Co., Ltd., Eli Lilly Japan K.K., Japan Tobacco Inc., Johnson and Johnson K.K., Kissei Pharmaceutical Co., Ltd., Kowa Pharmaceutical Co., Ltd., Kyowa Hakko Kirin Co., Ltd., Medtronic, Inc., MSD K.K., Nippon Boehringer Ingelheim Co., Ltd., Novartis Pharma K.K., Novo Nordisk Pharma Ltd., Ono Pharmaceutical Co., Ltd., Roche Diagnostics K.K., Sanofi K.K., Sanwa Kagaku Kenkyusho Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Taisho Toyama Pharmaceutical Co., Ltd., and Takeda Pharmaceutical Co., Ltd. and Tsumura and Co. M. Goda is an employee of Mitsubishi Tanabe Pharma Corporation. S. Yokota is an employee of Mitsubishi Tanabe Pharma Corporation. N. Maruyama is an employee of Mitsubishi Tanabe Pharma Corporation. H. Iijima is an employee of Mitsubishi Tanabe Pharma Corporation.
Compliance with ethics guidelines
All procedures followed were in accordance with the ethical standards of the relevant committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all patients for study participation.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Inagaki, N., Goda, M., Yokota, S. et al. Effects of Baseline Blood Pressure and Low-Density Lipoprotein Cholesterol on Safety and Efficacy of Canagliflozin in Japanese Patients with Type 2 Diabetes Mellitus. Adv Ther 32, 1085–1103 (2015). https://doi.org/10.1007/s12325-015-0255-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-015-0255-8