
Abstract
Although the role of the cerebellum in motor sequences learning is widely established, the specific function of its gamma oscillatory activity still remains unclear. In the present study, gamma (50 Hz)—or delta (1 Hz)—transcranial alternating current stimulation (tACS) was applied to the right cerebellar cortex while participants performed an implicit serial reaction time task (SRTT) with their right hand. The task required the execution of motor sequences simultaneously with the presentation of a series of visual stimuli. The same sequence was repeated across multiple task blocks (from blocks 2 to 5 and from blocks 7 to 8), whereas in other blocks, new/pseudorandom sequences were reproduced (blocks 1 and 6). Task performance was examined before and during tACS. To test possible after-effects of cerebellar tACS on the contralateral primary motor cortex (M1), corticospinal excitability was assessed by examining the amplitude of motor potentials (MEP) evoked by single-pulse transcranial magnetic stimulation (TMS). Compared with delta stimulation, gamma-tACS applied during the SRTT impaired participants’ performance in blocks where the same motor sequence was repeated but not in blocks where the new pseudorandom sequences were presented. Noteworthy, the later assessed corticospinal excitability was not affected. These results suggest that cerebellar gamma oscillations mediate the implicit acquisition of motor sequences but do not affect task execution itself. Overall, this study provides evidence of a specific role of cerebellar gamma oscillatory activity in implicit motor learning.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Implicit motor learning refers to the acquisition of motor skills following repetition and without conscious awareness [1, 2]. Several studies report that a wide network of regions operates during motor skill learning, including the cerebellum, the prefrontal and primary motor cortex (M1), and the basal-ganglia [3]. Within this network, each region plays a unique role in the formation of new skills. In particular, the cerebellum has a key role in the acquisition of new motor skills as well as in the timing of motor sequences [4,5,6]. Indeed, cerebellar lesions impair the acquisition of sequences of movements [7, 8]. Likewise, repetitive transcranial magnetic stimulation (rTMS) and anodal transcranial direct current stimulation (tDCS) can interfere with cerebellar activity and affect motor-learning. Specifically, low-frequency cerebellar TMS, immediately before the execution of a serial reaction time task (SRTT), is able to disrupt implicit motor sequences learning (i.e., increasing reaction times) whereas anodal cerebellar tDCS can improve the performance on a similar task (i.e., reducing reaction times) [9, 10].
Although the role of the cerebellum is well established, the oscillatory dynamics mediating the acquisition of motor skills remain still to be clarified. For instance, 50 Hz transcranial alternating current stimulation (tACS) applied over the cerebellum improves the performance in a visuomotor task. Furthermore, the 50 Hz tACS induced a post-stimulation increase of M1 excitability [11] suggesting that cerebellum and M1 may communicate via gamma oscillations. Likewise, a weakening of cerebellar brain inhibition (CBI) was found. Indeed, the cerebellum exerts an inhibitory tone on the primary motor cortex (M1) so that applying magnetic or electric currents over the cerebellum induces secondary changes in motor cortex excitability levels [12, 13].
In line with these findings, high gamma frequency tACS (i.e., 70 Hz) delivered through electrodes placed simultaneously over the left cerebellar hemisphere and the right M1 has shown to improve motor performance in a force task requiring to track the movement of a target on a screen with the index finger [14]. The authors suggested that this improvement may reflect the strengthening of the synchronization between cerebellum and M1.
In a previous study, we found that M1 gamma-tACS (50 Hz) modulates the retrieval, but not the acquisition of a previously learned motor sequence in the SRTT. In addition, we found a reduction of M1 excitability after tACS [15]. An unexplored question, though, is whether cerebellar gamma activity also mediates implicit motor sequence learning. In the present study, we wanted to disentangle the role of M1 and cerebellum within the learning of a sequence of movements. We, therefore, applied a gamma-tACS (50 Hz) over the cerebellum while participants executed a SRTT. To control for frequency-specific effects and avoid entrainment of gamma harmonics and subharmonics, a delta (1 Hz) stimulation was applied as control condition [15, 16]. As both the stimulation frequencies may potentially induce an effect, to avoid misinterpretation of the results, we additionally compared performances during gamma and delta tACS with the performance of a group of participants that underwent sham tACS in a previous study conducted in our lab, with identical task and procedure.
Moreover, long-range after-effects on M1 were assessed by measuring MEP following cerebellar tACS. We hypothesized that if cerebellar gamma oscillations mediated implicit motor sequences learning [6], then we would expect an effect on task performance when the repetition of the same motor sequence is required. Moreover, if cerebellar tACS induced long-term effects on M1 activity, then we would also observe a modulation of corticospinal excitability, as indexed by MEP amplitude.
Material and Methods
Participants
Eighteen healthy right-handed volunteers (7 male, mean age 25.2 ± 4.1 years) took part in the experiment, after giving written informed consent. All participants were right-handed according to the Edinburgh handedness inventory [17] and naïve to the experimental hypotheses. Exclusion criteria were brain injury, neurological or psychiatric disorder, not-corrected vision deficits, intracranial metallic plates, cardiac pacemakers, pregnancy, family, or personal history of epilepsy. The study was approved by the ethical committee of the University Hospital “Paolo Giaccone” of Palermo and was conducted according to the declaration of Helsinki.
Procedure
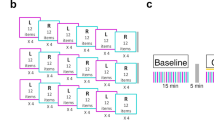
Participants took part in two experimental sessions, one for each stimulation frequency (1 Hz or 50 Hz), performed at least 48 h apart in a counterbalanced order. During the first session, participants familiarized with the experimental environment, underwent a brief interview about their medical history, and filled out the handedness inventory questionnaire [17]. During the experimental session, participants sat on a comfortable chair in front of a computer screen. Participants first executed the SRTT (pre-tACS phase). Soon after, the stimulation site and the motor threshold (MT) were identified, and 50 baseline MEP were collected through the input-output procedure. Afterward, participants executed a new version of the SRTT and simultaneously received tACS (online-tACS phase). Immediately after tACS (post-tACS phase), the TMS input-output procedure was replicated to test long-term changes in MEP amplitude (Fig. 1).

The figure shows the experimental procedure (left side) and the task’s structure (right side). In the pre-tACS phase, participants first performed the serial reaction time task (SRTT), followed by the assessment of the SI-1 mV (i.e., the lowest stimulus intensity needed to elicit MEP of 1 mV peak-to-peak) and of the input-output curve. In the online-tACS phase, stimulation was delivered during the execution of the SRTT (5 min). The electrodes were placed over the right cerebellum and the ipsilateral buccinator muscle. In the post-tACS phase, SI 1mV and the input-output procedure were again assessed. The panel on the right side shows the SRTT. The asterisk appeared in one of four possible positions marked by low dashes and corresponding to a key on a keyboard (V, B, N, M). Subjects responded to each asterisk by pressing with their right hand (index, middle, ring, pinkie) the key on the keyboard. Five hundred milliseconds after each response, the asterisk appeared at a new location. The task counted eight blocks, the same sequence was repeated in each block with the exception of blocks 1 and 6 were asterisks’ locations were randomly distributed
Serial Reaction Time Task (SRTT)
SRTT is one of the most common methods used to assess implicit learning of motor sequences [18, 19]. In the present study, we used the same version as in Giustiniani et al. [15]. The task lasts 5 min and consisted of a motor cue (an asterisk of 1.2 cm diameter) appearing on a grey screen (17 inch, 1280 × 1024 pixel resolution) in one of four horizontally centred positions, marked by a low dash. Participants were instructed to press the key on a keyboard corresponding to the asterisk position as soon and as fast as they could by using one of the four fingers of the right hand (index, middle, ring, pinkie). The asterisk would remain on the screen until a response was given, then disappear and appear to the following position (Fig. 1). The inter-stimulus interval (the blank between asterisks) was fixed at 500 ms [20]. The task counted 8 blocks, interleaved with a self-paced break (few seconds to relax the hand). Participants were instructed to press any key to restart the task from the break. Each block, with the exclusion of blocks 1 and 6, included 6 repetitions of the same 12 motor cues/movement sequences. Blocks 1 and 6 presented, instead, a series of items in a pseudorandom order. Participants were unaware of the structure of task’s sequences. Four parallel versions of the SRTT were implemented, each with a different sequence. The interchangeability of these versions was verified in a pilot study. Each participant performed all the versions across the four time points (1 Hz pre-/post-tACS, 50 Hz pre-/post-tACS). Furthermore, during the first session, before the pre-tACS phase, two pseudorandom sequences of 12 stimuli each were administered for practice.
At the end of the experiment, participants were debriefed to make sure they were not aware of the repeating sequences. The qualitative debriefing consisted of a series of questions by which they were asked to report their perceived task difficulty and any other impression about the task, without mentioning the sequencing rules. None of the participant reported the sensation of a repeating sequence.
Transcranial Alternating Current Stimulation (tACS)
TACS was delivered for the whole duration of the SRTT (online-tACS phase) through a BrainStim battery-driven electric stimulator (E.M.S., Bologna, Italy), connected with two conductive-rubber electrodes (5×5 cm2) placed in saline-soaked sponges. The centre of the active electrode was placed over the right cerebellar hemisphere (1 cm under and 3 cm right to the inion). The centre of the return electrode was placed over the ipsilateral buccinator muscle [21, 22], the impedance was kept below 10 kΩ. Stimulation intensity was set at 2 mA peak-to-peak corresponding to 0.08 mA/cm2 current density under each electrode, with a ramp up/down time of 30 s. Both participants and experimenters were blinded with respect to the stimulation frequency. At the end of each session, participants were asked about their perceived sensations during the stimulation using a structured questionnaire about tES-related sensations and discomforts [23]. We checked for the following sensations: itching, pain, burning, metallic/iron taste, warmth/ heat, fatigue, alertness, and others. Response options were none, mild, moderate, and strong. Most of the responses for all the sensations were either “none” or “mild” for both 1 and 50 Hz stimulation. None of the participants perceived phosphenes during the stimulation. Moreover, participants were not able to distinguish between the two stimulation frequencies. During the 1-Hz stimulation, two participants reported sensations of metallic taste and dizziness. For these participants, the stimulation was immediately interrupted, and they were excluded from the study and replaced by two additional participants (final n = 18).
Transcranial Magnetic Stimulation (TMS)
Single-pulse TMS was delivered over the left M1 using a MagStim Super Rapid 2 biphasic magnetic stimulator (Magstim Company, Whiteland, Wales, UK) through a 70-mm figure-eight coil. MEP were recorded with surface Ag/AgCl electrodes placed over the first dorsal interosseous (FDI) muscle of the right hand, arranged in a belly-tendon montage, and connected to a stimulator-integrated EMG amplifier. Raw EMG signals were band-pass filtered (2 Hz to 10 kHz). The coil was placed tangentially to the scalp with the handle pointing in antero-medial orientation, 45° from the interhemispheric line of the participant’s head, so that the current flowed in a posterior to anterior direction inducing the strongest tissue current in the reversal phase of the pulse [24]. To define stimulation location, we first delivered TMS pulses over C3 (as in 10-20 EEG system) and surrounding sites, until we found the optimal site to elicit the largest evoked potential in the FDI muscle at rest. Coil position was then fixed and recorded through an optic tracking system (SoftTaxic Neuronavigator system; E.M.S., Bologna, Italy), which allowed the monitoring of the coil position throughout the whole session. TMS intensity was set relative to the lowest stimulus intensity (% maximum stimulator output) needed to elicit MEP of 1 mV peak-to-peak amplitude (SI-1mV) in at least three out of five pulses. Participants’ corticospinal excitability was assessed by using the input-output curve procedure. Namely, 50 peak-to-peak MEP were acquired at each stimulus intensity ranging from 100 to 140% of the SI-1mV, in steps of 10% (10 single pulses for each intensity delivered every 8–10 s), immediately before and after tACS [25, 26].
Data Analysis
SRTT
We measured tACS modulatory effects on the SRTT by using participants’ response times (RTs). Inferential statistics were not computed for error rates because the task typically shows very high percentage of accurate responses [15]. RTs of incorrect responses and shorter than 100 ms were removed before the analysis (overall 3.6% of trials). To improve the normality distribution of RTs, a log-transformation was applied to raw RTs data (Kolmogorov-Smirnov test on raw RTs: D = 0.11, p < .001, skewness = 2.24; K-S test on log-RT: D = 0.04, p < .001, skewness = 0.58) [27]. Then, RTs were modelled by a multiple linear regression model. Namely, the following model (in R notation) was fitted by means of the lme4 package [28]: RT ~ Stimulation frequency × Time × Block + (1 | ID), including stimulation frequency (delta vs. gamma stimulation), time (pre- vs. online-tACS phase), and block (1–8) as predictors. Delta stimulation, pre-tACS, and block 1 was entered as reference levels (set to 0). Block number was considered as a factor as blocks qualitatively differed: the same motor sequence was repeated across blocks 2, 3, 4, 5, 7, and 8, whereas new/pseudorandom sequences were presented in blocks 1 and 6. Motor performance was expected to improve across the blocks containing the repeated sequence (i.e., blocks 2–5, 7–8) and to worsen in the block containing pseudorandom sequences (i.e., block 6). Participant number (ID) was entered as random factor. To make sure participants learned the given sequence, in a separate regression model, we contrasted RTs in block 5, i.e., where the motor sequence was presented the maximal number of times, and thus, the amount of learning should be maximal, to RTs in block 6, i.e., containing a new/pseudorandom motor sequence, and thus, interrupting the learned sequence (RTsBlock5 vs RTsBlock6). This contrast represents an index of implicit learning [29]. The plotted residual values of all the models were normally distributed around zero (from max 0.5 to min -0.5).
Input-output curve
The tACS after-effect on corticospinal excitability was assessed by analysing the MEP input-output curve. Data were fitted with the following regression model: MEP amplitude ~ Stimulation frequency × Time × Pulse intensity + (1 | ID). Pulse intensity has five levels: 100, 110%, 120, 130, and 140%.
In all the regression models, p-values were estimated by means of the lmerTest package; the Satterthwaite’s approximation was applied for computing the degrees of freedom [30].
Results
SRTT
Overall, a mean accuracy of 97% (SD = 18) in both the pre- and online 1 Hz sessions and a mean accuracy of 97% (SD = 16) in both the pre- and online 50 Hz sessions was obtained. The mean RTs across blocks and tACS sessions are plotted in Fig. 2. A main effect of time and a main effect of block were found. Namely, participants were overall significantly faster in the online-tACS phase relative to the pre-tACS phase (t = −6.78, p < .001), and in all blocks relative to block 1 (blocks 2–5, 7–8: ts < −4.64, ps < .001), but block 6 (t = 3.21, p = .001). No main effect of Stimulation frequency was found (t = -.34, p = .734). Importantly, the Stimulation frequency × Time × Block interaction revealed that the RTs change from pre- to online-tACS phase was smaller when gamma stimulation was applied relative to delta stimulation, in blocks 3, 4, 5, 7, and 8 (ts > 2.02, ps ≤ .05; Fig. 3). In other words, participants became significantly faster during the delta stimulation compared with the gamma stimulation. On the other hand, RTs on block 6 were not affected by Stimulation frequency × Time (t = 0.12, p = 0.9).

Mean response times (RTs) expressed in milliseconds (ms) across task blocks and stimulation frequency (Delta, 1 Hz vs. Gamma, 50 Hz), before (pre) or during (online) tACS. The repeating sequence was presented from block 2 to block 5 and in blocks 7 and 8, respectively. A random sequence was embedded in blocks 1 and 6. Error bars represent standard deviation of mean RT

Difference between mean response times (RTs) in the pre-tACS phase and mean RTs in the online-tACS phase across task blocks and stimulation types (Delta, 1 Hz vs. Gamma, 50 Hz). Error bars represent standard error of mean RTs difference. Here, RTs are expressed in milliseconds (ms) whereas statistical analyses were performed on log-transformed data, baseline corrected to block 1
When we contrasted the RTs in block 5 to RTs in block 6 (learning index) in the online tACS phase, a significant Stimulation frequency × Time interaction emerged (t = -2.29, p = .022), which showed that the difference between RTs in block 5 and RTs in block 6 was larger during the delta stimulation relative to the gamma stimulation.
The effect on the learning index was similar to that previously observed during the sham tACS in a previous study of our lab with identical task and design ([15], Table 4S and Fig. 1S). Although this comparison should be taken cautiously since the data refer to an independent study, we merged the data of the two experiments and statistically tested the effects of Stimulation frequency (1 Hz vs. 50 Hz vs. Sham), Time (pre vs. online), and block (5 vs. 6) on RTs. The analysis confirmed the presence of a three-way interaction, that is, the RT difference between block 6 and block 5 in the online-tACS phase relative to the pre-tACS phase was smaller in the 50 Hz condition compared with the Sham (t = −2.88, p = .004), but it did not differ between the 1 Hz and the Sham session (t = −.7, p = .485).
To check for carry-over effects and differences at baseline (pre-tACS), we assessed the effect of the stimulation order using the following model: RT ~ Stimulation frequency × session + (1 | ID). The statistical analysis revealed no differences between the pre-tACS in the two stimulation conditions (ts < .043, ps > .372).
Input-output curve
Figure 4 depicts the mean MEP amplitude evoked by single-pulse TMS at varying intensities after tACS. As expected, MEPs amplitude significantly increased with increasing TMS intensities (t = 18.7, p < .001). However, neither the effect of Stimulation frequency (t = -0.17, p = .867) nor the Time (t = -0.6, p = .55) and the interactions (ts < 0.75, ps > 0.454) were significant.

Mean amplitude of motor-evoked potential (MEP) in pre- and post-tACS phases of the two stimulation frequencies (Delta, 1 Hz vs. Gamma, 50 Hz) across transcranial magnetic stimulation (TMS) pulse intensities (from 100 to 140% of the TMS intensity that elicited a 1 mV peak-to-peak MEP, SI-1mV). Error bars represent standard error of mean MEP amplitude
All the complete regression models are reported in the Supplementary materials.
Discussion
The aim of the present study was to assess the role of cerebellar gamma oscillations in motor sequences learning. To this aim, during the execution of an implicit motor learning task (SRTT), we delivered either gamma—or delta—tACS over the cerebellar hemisphere ipsilateral to the performing hand. Compared with delta tACS, we found that, during the gamma-tACS, participants did not show an increased performance in blocks where the same motor sequence was repeated over time and the motor performance was expected to maximally improve. Interestingly, no differences between the two stimulation frequencies emerged during the execution of the new/pseudorandom motor sequence. This finding was confirmed by a reduced difference between the block where we expected the sequence being maximally learned due to repetition (i.e., block 5) and the block where the new/pseudorandom sequence was presented and learning was interfered (i.e., block 6) during gamma—compared with delta—tACS.
The role of the cerebellum is principally to create predictions and internal models of the external stimuli [31]. These models are used to fast detect future regularities and deviances (errors) so that learning can take place and motor responses can be optimized. Therefore, implicit motor learning, such as the one we observed during the execution of SRTT, is indexed by a progressive reduction of RTs when stimuli/movements follow a fixed predictable order (regular motor sequences) [32]. In the present study, during the gamma stimulation, the progressive RTs reduction that usually emerges over time during learning of fixed sequences was missing, so that the performance reflected a flattened learning curve across blocks (see Fig. 3). We speculate that this result was due to interference caused by cerebellar gamma-tACS on the formation of internal models, which, in turn, resulted in a disrupted learning of the motor sequence [33, 34].
In a previous study [15], we applied a gamma-tACS over M1 during the execution of the same motor sequence task, and observed a disruption of participants’ performance only in the two last task blocks (blocks 7 and 8). We interpreted this result as due to gamma-tACS impairing participants’ ability to retrieve the previously learned motor sequence. By comparing these findings to the present results, we may speculate that while gamma-tACS over the cerebellum interferes with the acquisition phase of a motor sequence (blocks 3–5) and, consequently, with its retrieval at later stages (blocks 7–8), gamma-tACS over M1 interferes with retrieval of previously learned sequential movements (blocks 7–8 only), without affecting the initial acquisition of motor traces. The present findings are consistent with previous imaging studies demonstrating the cerebellum having a key role on the formation of implicit motor skills [3, 35], and M1 playing a role during relatively later stages, such as the retention phase [3, 33,34,35]. Furthermore, these findings are in line with a previous tDCS study that dissociated the contribution of cerebellum in the acquisition and of M1 in the retention of motor memories [36].
To the best of our knowledge, this is the first evidence showing a causal role of cerebellar gamma oscillations in the acquisition of implicit motor sequences. A recent study investigated the role of higher gamma frequency band in motor memory showing that 70 Hz tACS enhances retention in a task requiring to explicitly memorize fingers’ movements, needed to track a visual target on a screen [15]. Indeed, a performance’s improvement was observed 1 day after stimulation. Conversely, no changes in performance were found during tACS. Remarkably, in this study, the authors compared two different tACS montages (cerebellum only vs. cerebellum and M1) reporting no effects when tACS electrodes were placed over the cerebellum only. Overall, the authors conclude that synchronizing the activity of cortical and cerebellar areas in the gamma frequency band affects explicit motor learning over a wide intervals of time (i.e., 1 day after learning). In a more recent study, 50 Hz left cerebellar tACS did not affect performance in an explicit motor learning task requiring the execution of a grip force to move a cursor [37]. The difference in montage and hand between this study (left cerebellum and non-dominant hand) and our study (right cerebellum and right hand) might account for the divergent results and suggests that the effects depend on the stimulated hemisphere. Moreover, the divergent results might depend on the specific effect of 50 Hz gamma on implicit (our study) rather than explicit (Wessel’s and Miyaguchy’s studies) motor learning.
At a first glance, the impaired rather than the improved performance induced by gamma-tACS may appear inconsistent with the evidence of gamma synchronization in a wide network of brain regions during motor tasks [38]. However, one should consider that motor learning processes relative to cerebellar activity depend on the combined activity of Purkinje cells and parallel fibers [39]. Together they are responsible of cerebellar long-term depression (LTD) plasticity, which, we know, occurs during motor sequence learning [40]. Due to the low intensity of the stimulation, we may speculate that alternating currents reached the more external layer of cerebellum where Purkinje cells have their bodies [41]. By modulating the activity of these cells in the cerebellar cortex, gamma-tACS might have prevented the LTD processes needed for the formation of internal models and consequently for sequence learning [42, 43]. Indeed, inducing gamma oscillations might have led to long-term potentiation (LTP) [44].
On the other hand, as Purkinje cells exhibit activity at 50 Hz [44], we cannot exclude that the observed interference reflected an U-shape dose-effect [45]. Indeed, when an optimal level of oscillatory activity is reached, an increase of the power of that specific brain rhythm would deteriorate performance [46, 47]. In this case, endogenous cerebellar gamma oscillations could have reached high levels of power during the task. Therefore, externally applying gamma oscillatory currents could have perturbed cells activity by inducing homeostatic plasticity and prevented cells’ normal functioning during the formation of the motor sequence.
Finally, another possible explanation for the disruptive effect is that suboptimal components of the gamma frequency band have been entrained here. Indeed, Purkinje cell’s simple spikes are distributed in a wider range of frequencies, including the higher gamma band [48].
We did not find changes in corticospinal excitability measured after the end of the stimulation; therefore we might conclude that gamma-tACS specifically impaired cerebellar functioning and procedural learning components, probably without affecting M1 excitability. However, one might argue that some changes could have occurred on M1 excitability during tACS (online effect), which did not survive beyond the end of stimulation (after effect). Furthermore, input-output curve is a measure of cortical excitability; thus, we cannot exclude that some changes occurred in terms of cortical inhibition and that other methods (i.e., short or long intracortical inhibition) might have been more sensitive in detecting these changes. Our results are in contrast with a previous study of Naro et al. [11] reporting changes in cortical excitability (i.e., MEP amplitude) after 50 Hz cerebellar tACS. Nevertheless, methodological differences might account for this difference, such as the tACS duration (1 min in the Naro’s study vs. the whole task duration in the present study), the procedure used to test corticospinal excitability (TMS-MEP vs. TMS input-output curve), and the brain state during tACS (resting vs. task execution). Further studies are needed to explore the effect of cerebellar tACS on corticospinal excitability, taking into account the ongoing brain state (state dependency effect). A limitation of the study that we should acknowledge is that assessing paired-pulse cerebellar inhibition might have been a more sensitive measure to evaluate the impact of tACS on the cerebello-M1 tract. Additionally, throughout the input-output procedure, we collected only 10 MEP for each stimulation intensity, assessing MEP amplitude in 20–30 trials might have ensured a more stable and reliable measure of M1 excitability [49].With respect to tACS, another limitation of the study is the poor focality of stimulation. Indeed, given the montage and the electrodes’ size, we cannot exclude a spread of the current over other cortical areas [50]. The future use of high-density montages would elucidate this issue.
Conclusions
The present study suggests that gamma-tACS on cerebellum perturbs the acquisition of motor sequences. This impairment of cerebellar activity during gamma-tACS does not induce long-lasting effects on corticospinal excitability measured with the input-output procedure. These results confirm previous studies showing the pivotal role of the cerebellum in procedural learning and add new evidence on the specific contribution of cerebellar gamma oscillations, encouraging future studies to explore the specific functional role of gamma cerebellar oscillatory activity in motor as well as in cognitive learning.
References
Mauk MD, Medina JF, Nores WL, Ohyama T. Cerebellar function: Coordination, learning or timing? Curr Biol. 2000;10:R522–5. https://doi.org/10.1016/S0960-9822(00)00584-4.
Doyon J, Gaudreau D, Laforce R Jr, Castonguay M, Bédard PJ, Bédard F, et al. Role of the Striatum, Cerebellum, and Frontal Lobes in the Learning of a Visuomotor Sequence. Brain Cogn. 1997;34:218–45. https://doi.org/10.1006/brcg.1997.0899.
Ungerleider L. Imaging Brain Plasticity during Motor Skill Learning. Neurobiol Learn Mem. 2002;78:553–64. https://doi.org/10.1006/nlme.2002.4091.
Nixon PD, Passingham RE. The cerebellum and cognition: cerebellar lesions impair sequence learning but not conditional visuomotor learning in monkeys. Neuropsychologia. 2000;38:1054–72. https://doi.org/10.1016/S0028-3932(99)00138-4.
Ivry RB, Keele SW. Timing Functions of The Cerebellum. J Cogn Neurosci. 1989;1:136–52. https://doi.org/10.1162/jocn.1989.1.2.136.
Doyon J, Song AW, Karni A, Lalonde F, Adams MM, Ungerleider LG. Experience-dependent changes in cerebellar contributions to motor sequence learning. Proc Natl Acad Sci. 2002;99:1017–22. https://doi.org/10.1073/pnas.022615199.
Torriero S, Oliveri M, Koch G, Lo Gerfo E, Salerno S, Petrosini L, et al. Cortical networks of procedural learning: Evidence from cerebellar damage. Neuropsychologia. 2007;45:1208–14. https://doi.org/10.1016/j.neuropsychologia.2006.10.007.
Molinari M, Leggio MG, Solida A, Ciorra R, Misciagna S, Silveri MC, et al. Cerebellum and procedural learning: Evidence from focal cerebellar lesions. Brain. 1997;120:1753–62. https://doi.org/10.1093/brain/120.10.1753.
Torriero S, Oliveri M, Koch G, Caltagirone C, Petrosini L. Interference of Left and Right Cerebellar rTMS with Procedural Learning. J Cogn Neurosci. 2004;16:1605–11. https://doi.org/10.1162/0898929042568488.
Ferrucci R, Brunoni AR, Parazzini M, Vergari M, Rossi E, Fumagalli M, et al. Modulating human procedural learning by cerebellar transcranial direct current stimulation. Cerebellum. 2013;12:485–92. https://doi.org/10.1007/s12311-012-0436-9.
Naro A, Bramanti A, Leo A, Manuli A, Sciarrone F, Russo M, et al. Effects of cerebellar transcranial alternating current stimulation on motor cortex excitability and motor function. Brain Struct Funct. 2017;222:2891–906. https://doi.org/10.1007/s00429-016-1355-1.
Oliveri M, Koch G, Torriero S, Caltagirone C. Increased facilitation of the primary motor cortex following 1 Hz repetitive transcranial magnetic stimulation of the contralateral cerebellum in normal humans. Neurosci Lett. 2005;376:188–93. https://doi.org/10.1016/j.neulet.2004.11.053.
Galea JM, Jayaram G, Ajagbe L, Celnik P. Modulation of Cerebellar Excitability by Polarity-Specific Noninvasive Direct Current Stimulation. J Neurosci. 2009;29:9115–22. https://doi.org/10.1523/JNEUROSCI.2184-09.2009.
Miyaguchi S, Otsuru N, Kojima S, Saito K, Inukai Y, Masaki M, et al. Transcranial Alternating Current Stimulation With Gamma Oscillations Over the Primary Motor Cortex and Cerebellar Hemisphere Improved Visuomotor Performance. Front Behav Neurosci. 2018;12:132. https://doi.org/10.3389/fnbeh.2018.00132.
Giustiniani A, Tarantino V, Bonaventura RE, Smirni D, Turriziani P, Oliveri M. Effects of low-gamma tACS on primary motor cortex in implicit motor learning. Behav Brain Res. 2019;376:112170. https://doi.org/10.1016/j.bbr.2019.112170.
Ali MM, Sellers KK, Frohlich F. Transcranial Alternating Current Stimulation Modulates Large-Scale Cortical Network Activity by Network Resonance. J Neurosci. 2013;33:11262–75. https://doi.org/10.1523/jneurosci.5867-12.2013.
Oldfield RC. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia. 1971;9:97–113. https://doi.org/10.1016/0028-3932(71)90067-4.
Nissen MJ, Knopman DS, Schacter DL. Neurochemical dissociation of memory systems. Neurology. 1987. https://doi.org/10.1212/wnl.37.5.789.
Mutanen TP, Bracco M, Robertson EM. A Common Task Structure Links Together the Fate of Different Types of Memories. Curr Biol. 2020;30:2139–2145.e5. https://doi.org/10.1016/j.cub.2020.03.043.
Nitsche MA, Jakoubkova M, Thirugnanasambandam N, Schmalfuss L, Hullemann S, Sonka K, et al. Contribution of the premotor cortex to consolidation of motor sequence learning in humans during sleep. J Neurophysiol. 2010;104:2603–14. https://doi.org/10.1152/jn.00611.2010.
Naro A, Russo M, Leo A, Cannavò A, Manuli A, Bramanti A, et al. Cortical connectivity modulation induced by cerebellar oscillatory transcranial direct current stimulation in patients with chronic disorders of consciousness: A marker of covert cognition? Clin Neurophysiol. 2016;127:1845–54. https://doi.org/10.1016/j.clinph.2015.12.010.
Rezaee Z, Ruszala B, Dutta A, A computational pipeline to find lobule-specific electric field distribution during non-invasive cerebellar stimulation, in: IEEE Int. Conf. Rehabil. Robot., 2019. https://doi.org/10.1109/ICORR.2019.8779453.
Antal A, Alekseichuk I, Bikson M, Brockmöller J, Brunoni AR, Chen R, et al. Low intensity transcranial electric stimulation: Safety, ethical, legal regulatory and application guidelines. Clin Neurophysiol. 2017;128:1774–809. https://doi.org/10.1016/j.clinph.2017.06.001.
Groppa S, Oliviero A, Eisen A, Quartarone A, Cohen LG, Mall V, et al. A practical guide to diagnostic transcranial magnetic stimulation: Report of an IFCN committee. Clin Neurophysiol. 2012;123:858–82. https://doi.org/10.1016/j.clinph.2012.01.010.
Bracco M, Turriziani P, Smirni D, Mangano GR, Oliveri M (2017) Relationship between physiological excitatory and inhibitory measures of excitability in the left vs. right human motor cortex and peripheral electrodermal activity. Neurosci Lett 641:45–50. https://doi.org/10.1016/j.neulet.2017.01.027.
Bracco M, Mangano GR, Turriziani P, Smirni D, Oliveri M (2017) Combining tDCS with prismatic adaptation for non-invasive neuromodulation of the motor cortex. Neuropsychologia 101:30–8. https://doi.org/10.1016/j.neuropsychologia.2017.05.006Get
Wagenmakers EJ, Brown S. On the Linear Relation Between the Mean and the Standard Deviation of a Response Time Distribution. Psychol Rev. 2007;114:830–41. https://doi.org/10.1037/0033-295X.114.3.830.
Bates D, Mächler M, Bolker B, Walker S. Fitting Linear Mixed-Effects Models Using lme4. J Stat Softw. 2015. https://doi.org/10.18637/jss.v067.i01.
Ambrus GG, Chaieb L, Stilling R, Rothkegel H, Antal A, Paulus W. Monitoring transcranial direct current stimulation induced changes in cortical excitability during the serial reaction time task. Neurosci Lett. 2016;616:98–104. https://doi.org/10.1016/j.neulet.2016.01.039.
Luke SG. Evaluating significance in linear mixed-effects models in R. Behav Res Methods. 2017;49:1494–502. https://doi.org/10.3758/s13428-016-0809-y.
Penhune VB, Doyon J. Cerebellum and M1 interaction during early learning of timed motor sequences. Neuroimage. 2005;26:801–12. https://doi.org/10.1016/j.neuroimage.2005.02.041.
Robertson EM. The Serial Reaction Time Task: Implicit Motor Skill Learning? J Neurosci. 2007;27:10073–5. https://doi.org/10.1523/JNEUROSCI.2747-07.2007.
Jenkins I, Brooks D, Nixon P, Frackowiak R, Passingham R. Motor sequence learning: a study with positron emission tomography. J Neurosci. 1994;14:3775–90. https://doi.org/10.1523/JNEUROSCI.14-06-03775.1994.
Balleine BW, O’Doherty JP. Human and rodent homologies in action control: corticostriatal determinants of goal-directed and habitual action. Neuropsychopharmacology. 2010;35:48–69. https://doi.org/10.1038/npp.2009.131.
Shadmehr R. Neural Correlates of Motor Memory Consolidation. Science (80-). 1997;277:821–5. https://doi.org/10.1126/science.277.5327.821.
Galea JM, Vazquez A, Pasricha N, Orban de Xivry J-J, Celnik P. Dissociating the Roles of the Cerebellum and Motor Cortex during Adaptive Learning: The Motor Cortex Retains What the Cerebellum Learns. Cereb Cortex. 2011;21:1761–70. https://doi.org/10.1093/cercor/bhq246.
Wessel MJ, Draaisma LR, de Boer AFW, Park CH, Maceira-Elvira P, Durand-Ruel M, et al. Cerebellar transcranial alternating current stimulation in the gamma range applied during the acquisition of a novel motor skill. Sci Rep. 2020. https://doi.org/10.1038/s41598-020-68028-9.
Jerbi K, Ossandón T, Hamamé CM, Senova S, Dalal SS, Jung J, et al. Task-related gamma-band dynamics from an intracerebral perspective: Review and implications for surface EEG and MEG. Hum Brain Mapp. 2009;30:1758–71. https://doi.org/10.1002/hbm.20750.
Ito M. Internal model visualized. Nature. 2000. https://doi.org/10.1038/35003097.
Ito M. Cerebellar learning in the vestibulo–ocular reflex. Trends Cogn Sci. 1998;2:313–21. https://doi.org/10.1016/S1364-6613(98)01222-4.
Andersen P, Eccles JC, Voorhoeve PE. POSTSYNAPTIC INHIBITION OF CEREBELLAR PURKINJE CELLS. J Neurophysiol. 1964. https://doi.org/10.1152/jn.1964.27.6.1138.
Penhune VB, Steele CJ. Parallel contributions of cerebellar, striatal and M1 mechanisms to motor sequence learning. Behav Brain Res. 2012;226:579–91. https://doi.org/10.1016/j.bbr.2011.09.044.
Huang L, Yang X-J, Huang Y, Sun EY, Sun M. Ketamine Protects Gamma Oscillations by Inhibiting Hippocampal LTD. PLoS One. 2016;11:e0159192. https://doi.org/10.1371/journal.pone.0159192.
Middleton SJ, Racca C, Cunningham MO, Traub RD, Monyer H, Knöpfel T, et al. High-Frequency Network Oscillations in Cerebellar Cortex. Neuron. 2008;58:763–74. https://doi.org/10.1016/j.neuron.2008.03.030.
Ridding MC, Ziemann U. Determinants of the induction of cortical plasticity by non-invasive brain stimulation in healthy subjects. J Physiol. 2010;588:2291–304. https://doi.org/10.1113/jphysiol.2010.190314.
Rufener KS, Zaehle T, Oechslin MS, Meyer M. 40 Hz-Transcranial alternating current stimulation (tACS) selectively modulates speech perception. Int J Psychophysiol. 2016;101:18–24. https://doi.org/10.1016/j.ijpsycho.2016.01.002.
Karabanov A, Ziemann U, Hamada M, George MS, Quartarone A, Classen J, et al. Consensus paper: probing homeostatic plasticity of human cortex with non-invasive transcranial brain stimulation. Brain Stimul. 2015;8:993–1006.
Thach WT. Discharge of Purkinje and cerebellar nuclear neurons during rapidly alternating arm movements in the monkey. J Neurophysiol. 1968. https://doi.org/10.1152/jn.1968.31.5.785.
Goldsworthy MR, Hordacre B, Ridding MC. Minimum number of trials required for within- and between-session reliability of TMS measures of corticospinal excitability. Neuroscience. 2016. https://doi.org/10.1016/j.neuroscience.2016.02.012.
Sadleir RJ, Vannorsdall TD, Schretlen DJ, Gordon B. Transcranial direct current stimulation (tDCS) in a realistic head model. Neuroimage. 2010;51:1310–8. https://doi.org/10.1016/j.neuroimage.2010.03.052.
Acknowledgments
The current work was funded by A.I.R.Alzh Onlus-COOP Italia. We wish to thank Antonino Visalli for his guidance in the statistical analyses.
Funding
Open access funding provided by Università degli Studi di Palermo within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 152 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Giustiniani, A., Tarantino, V., Bracco, M. et al. Functional Role of Cerebellar Gamma Frequency in Motor Sequences Learning: a tACS Study. Cerebellum 20, 913–921 (2021). https://doi.org/10.1007/s12311-021-01255-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12311-021-01255-6