
Abstract
Acute myeloid leukemia (AML) is a genetic disorder of hematopoietic stem cells (HSCs) followed by clonal selection and uncontrolled proliferation leading to malignant neoplasm. Inappropriate regulation of apoptosis contributes to many human disorders including cancer. Caspase 9 (CASP9) is associated with the intrinsic pathway of apoptosis. Functional single-nucleotide polymorphisms (SNPs) in CASP9 might influence gene expression leading to altered apoptosis and increased AML risk. Previously, two CASP9 promoter polymorphisms (CASP9 1263 rs4645978A > G and CASP9 712 rs4645981C > T) were shown to be associated with increased risk of developing AML and inferior AML survival in South Indian subjects. This study was to evaluate these polymorphisms in an independent cohort of AML patients and controls in Egypt. PCR–RFLP for CASP9 1263 rs4645978 A > G and CASP9 712 rs4645981 C > T genotypes were done in 60 de novo AML cases and 40 healthy control subjects. Our study showed that CASP9 712 rs4645981 C > T gene polymorphism is associated with increased risk of developing AML and poor disease outcome (p value = 0.006, < 0.001; OR = 3.644, 26; and 95% CI = 1.39–9.528, 6.5–103.5, respectively). In contrast, CASP9 1263 rs4645978 A > G showed no significant difference between AML patients and the controls regarding the risk of developing AML or disease outcome (p value = 0.301, 0.573, respectively). CASP9 712 rs4645981 C > T could be involved in the pathophysiology and development of AML in Egypt and may be useful as a predictive molecular markers for inferior prognosis in AML. Notably, risk was highest and outcomes worst in patients with both the 712C > T and 1263A > G alleles.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acute myeloid leukemia (AML) is a genetically heterogeneous disease with accumulation of acquired genetic alterations in hematopoietic progenitor cells that disturb normal mechanisms of cell growth, proliferation, and differentiation [1]. AML is a complex disease with a wide range of clinical, morphologic, biologic, cytogenetic, molecular, and immunophenotypic features [2]. In Egypt, AML represents 1.8% of all cancer diagnoses by the National Cancer Institute (NCI) [3].
Cell proliferation and apoptosis are the result of a balanced interaction among multiple regulators such as oncogenes, oncosuppressor genes, and cell cycle associated proteins [4]. Caspase 9 (CASP9) belongs to a family of intracellular cysteine-aspartic proteases (caspases) and is located on chromosome l at 1p36.21. The CASP9 protein product functions in the intrinsic pathway of apoptosis which is cellular suicide required for the maintenance of cell homeostasis [5]. CASP9 is responsible for the first proteolytic events mediated by BCL-2 associated X protein (Bax)/BCL-2 homologous antagonist killer (Bak) insertion into mitochondrial membrane and subsequent release of cytochrome c from the mitochondrial inter-membrane space into the cytosol [1].
Single-nucleotide polymorphisms (SNPs) in the coding and regulatory regions of genes controlling apoptosis can impair the constitutive capacity of the host cells in dealing with DNA lesions which potentially alter the individual’s susceptibility to specific malignancies or sensitivity to chemo and radiotherapy. Several studies have confirmed the strong influence of genetic polymorphisms in genes controlling apoptosis on AML susceptibility [6].
Polymorphic variants of human CASP9 gene have been found. These human genetic polymorphisms can play critical roles in various diseases and malignancies including leukemia. Two polymorphisms, 1263 A > G and 712 C > T, have been identified in the CASP9 gene; both are located in the promotor region. A previous study of south Indian AML patients suggested that these polymorphisms may be associated with increased AML risk, possibly due to altered gene expression of CASP9 [1]. However, these results have not been replicated in an independent cohort or extrapolated to additional populations.
The present work aimed to study the influence of genetic polymorphisms of CASP9 on the risk of developing AML in Egypt. The chosen SNPs were CASP9 1263 rs4645978 A > G, and 712 rs4645981 C > T, using PCR–RFLP, and we correlated the genetic profile of AML patients regarding these genes with various clinical and laboratory findings as well as prognosis.
Patients and methods
Patients
Bone marrow and blood samples were collected from 60 newly diagnosed consecutive AML patients who sought care at the medical hematology-oncology clinics of the National Cancer Institute, Cairo University, Egypt, from January until December 2018, as well as blood samples from 40 age- and gender-matched healthy control subjects of the same geographic origin and ethnic background. The controls represented blood donors at the National Cancer Institute who consented to participate in research studies. The diagnosis of AML was established on the basis of the 2008 and revised 2016 World Health Organization classification criteria [7, 8] and confirmed by performing CBC, bone marrow study, immunophenotyping, cytochemistry, molecular, and cytogenetics studies. While most patients had greater than 20% blasts, one patient with a lower blast percentage met criteria for AML diagnosis by having a defining cytogenetic abnormality t [8, 9].
This study was approved by the ethical committee review board of Kasr Al-Ainy School of Medicine and National Cancer Institute, Cairo University, Cairo, Egypt, in accordance with the Helsinki guidelines for the protection of human subjects. Written informed consent was obtained from all participants.
Methods
A flow cytometric evaluation of the immunophenotype was analyzed in all 60 AML patients’ diagnostic samples using multicolor flow cytometry (Coulter Epics XL, Navios; Beckman Coulter, Danvers, MA, USA) using acute leukemia panel. Navios software was applied for analysis.
Karyotyping (G banding) was performed in all samples. Inter-phase fluorescence in situ hybridization (FISH) analysis to confirm changes and detect other changes was performed with locus-specific probes, double-color single fusion (Vysis, Downers Grove, IL, USA). FISH was considered positive when 3% or more of blasts were positive.
Genotyping: DNA was extracted from patients and controls’ leucocytes by QIAamp DNA Blood Mini Extraction Kit (Qiagen, Hilden, Germany) followed by polymerase chain reaction (PCR) and amplification of the extracted DNA by using specific primers for CASP9 1263 A > G (rs 4,645,978) and CASP9 712 C > T (rs 4,645,981) polymorphsims. Then, enzymatic digestion by specific restriction enzyme (Thermo Fisher Scientific, Massachusetts, USA) for each gene of the amplified PCR products using polymerase chain reaction-restriction fragment length polymorphism (PCR–RFLP) assay [1], followed by detection of the amplified gene by gel electrophoresis (Figs. 1 and 2), and genotyping for SNPs are all discussed in Table 1.

PCR–RFLP analysis of caspase 9 1263 rs4645978 A > G polymorphism in AML patients and the control group. Upper (U) panel, AML patients; lower (L) panel, control subjects. Lane 1, 50–1000 bps DNA molecular weight marker; lanes 2, 6, and 7 (U) and lanes 3, 4, 7, and 8 (L), AA genotype (29, 205 bp); lanes 3 and 9 (U) and lane 11 (L), GG genotype (234 bp); lanes 4, 5, 8, 10, and 11 (U) and lanes 2, 5, 6, 9, and 10 (L), AG genotype (29, 205, 234 bp)

PCR–RFLP analysis of caspase 9 712 rs4645981 C > T polymorphism in AML patients and the control group. Upper (U) panel, AML patients; lower (L) panel, control subjects. Lane 1, 50–1000 bps DNA molecular weight marker; lanes 5, 6, 7, 8, and 10 (U) and lanes 2, 3, 4, 6, 7, 8, and 11 (L), CC genotype (18, 176 bp); lane 2 (U) and lane 5 (L): = , TT genotype (194 bp); lanes 3, 4, 9, and 11 (U) and lanes 9 and 10 (L), CT genotype (18, 176, 194 bp)
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences, Version 23 (SPSS, Inc., Chicago, III., USA) for Windows. Numerical data were expressed as mean and standard deviation or median and range, as appropriate. Qualitative data were expressed as frequency and percentage. Chi-square test (Fisher’s exact test) was used to examine the relation between qualitative variables. For non-normally distributed quantitative data, comparison between 2 groups was done by the Mann–Whitney test (nonparametric t test). The multivariate analysis of variance test was used to compare more than 2 quantitative groups. A p value of < 0.05 was considered significant.
Results
This study included 60 patients diagnosed to have de novo AML prior to chemotherapy and followed up for 2 years. Forty age- and gender-matched normal healthy volunteers were also included as a control group. The controls consisted of 26 males (65%) and 14 females (35%), and their age ranged between 19 and 67 years with a mean age of 34 years. Full characterization of the patients regarding age, gender, hematologic findings, basic immunophenotypic acute leukemia panel, molecular study, karyotyping, and FISH is presented in Table 2.
SNP genotyping of the CASP9 polymorphism was performed using a previously described PCR-based RFLP assay [1]. Regarding CASP9 1263 rs4645978 A > G, there was no statistically significant difference in the frequency of the alternate G allele between AML patients and normal controls (p value = 0.301, OR = 1.556, 95% CI = 0.672–3.602). Specifically, 18 AML patients (30%) were of the AA genotype, while 42 (70%) were heterozygous or homozygous for the alternate allele (AG or GG). Similarly, in the control group, 16 (40%) individuals were of the AA genotype, and 24 (60%) were heterozygous or homozygous for the alternate allele. In contrast, a highly statistically significant association was identified between the CASP9 712 rs4645981 C > T alternate allele and AML risk (p value = 0.006, OR = 3.644, and 95% CI = 1.39–9.528. Specifically, 32 AML patients (53%) were of the CC genotype and 28 (47%) had alternate allele (CT/TT). While in the control group, 32 (80%) individuals were of the CC genotype and 8 (20%) had alternate allele (Table 3). This small study lacked power to identify a difference in odds ratio for CASP9 1263 and 712 heterozygotes versus homozygotes. Moreover, double combined CASP9 gene polymorphisms (CASP9 712 TT/CT compared to CASP9 1263 AA) were associated with a significant elevation of the risk of developing AML (p value = 0.005, OR = 7.41, and 95% CI = 1.58–34.71).
The relationship of the different genotypes of CASP9 1263 rs4645978 A > G and 712 rs4645981 C > T polymorphisms with the demographic, clinical, and laboratory parameters in AML patients was studied and shown in Table 4. There was no significant difference between the different groups as regards these clinical-pathological factors (p value > 0.05) except for an association of CASP9 alternate allele (G and T) having more frequent lymphadenopathy (p value = 0.027, 0.009) and higher TLC (p value = 0.023, 0.027), respectively, and an association of the CASP9 712 rs4645981 T allele with higher LDH level (p value < 0.001), and more frequent cytogenetic abnormalities with intermediate and adverse risk category (p value = 0.038, 0.011, respectively).
We evaluated the association between CASP9 gene polymorphisms and disease outcome following chemotherapy (Table 5). Prognosis and disease outcome in our study was classified into complete remission (CR), relapse, and death. CASP9 1263 A > G gene polymorphism had no significant impact on prognosis (p value = 0.573, OR = 7.3 and 95% CI = 0.24–2.21), while CASP9 712 T genotype was found to have a significant impact by increasing the risk of unfavorable outcome (p value < 0.001, OR = 26, and 95% CI = 6.5–103.5). Furthermore, combined CASP9 1263 G genotype and 712 T genotype were found to have a more significant impact on prognosis by increasing the risk of unfavorable outcome in AML patients than single gene polymorphism (p value = 0.004, OR = 7.1, and 95% CI = 1.7–29.4).
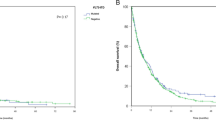
As regards overall survival in our AML patients, the mean survival time of individuals with the CASP9 1263 AA genotype was 16 months with 61% of AML patients surviving at 1 year (median survival not reached). Survival was similar in individuals with the alternate AG and GG genotypes, with a mean survival time of 18 months; 69% of patients were alive at 1 year (median survival not reached) (p value = 0.600) (Fig. 3). In contrast, the CASP9 712 CT and TT genotypes were associated with inferior survival (p value = 0.002). Specifically, the mean survival of AML patients homozygous for the CC allele was 21 months with 84% of individuals alive at 1 year (median survival not reached). In contrast, AML patients with CT/TT genotypes had mean survival of only 12 months with 46% alive at 1 year (median survival = 10 months) (Fig. 4).

Overall survival in caspase 9 1263 A > G gene polymorphism

Overall survival in caspase 9 712 C > T gene polymorphism
Discussion
The ability of cancer cells to evade apoptosis is a major characteristic that enables their uncontrolled growth. Deregulation of apoptosis disrupts the complex and delicate balance between cell proliferation, survival and death, and plays a major role in the development of diseases such as cancer, and particularly leukemia [4, 10].
Caspases (CASPs), one of the core components of apoptosis, are found in the cytosol as inactive zymogens. CASP9, a member of the caspase family of proteins, plays a central role in the mitochondrial apoptotic pathway [1]. Polymorphic variants of CASP9 were previously found to be associated with development of many types of cancers and resistance to chemotherapy [11]. But some CASP9 polymorphisms have more effect on malignancies than others as the mutations at the promoter alter the transcription of CASP9 more significantly and eliminate apoptosis, leading to increase proliferation of malignant cells and increased risk of many cancers [12].
In the present study, the G allele carrier (AG and GG) genotype frequencies were higher among AML patients than the controls; however, it was not significant regarding CASP9 1263 A > G gene polymorphism (p value = 0.174) with no association between this rs4645978 SNP genotype and AML risk in the studied Egyptian population (p value = 0.301, OR = 1.556, 95% CI = 0.672–3.602). Previously, Cingeetham et al. [1] described a borderline significant association between the CASP9 rs4645978 1263 A > G polymorphism and AML risk in a South Indian population (OR = 1.53; 95% CI = 0.99–2.36). In the present study of a distinct population of AML patients in Egypt, we did not confirm the association between this allele and AML risk. The discordance between our results and the prior study from South India might be attributed to genetic and/or environmental differences between these populations. In addition, our study is relatively small and may be underpowered for detection of small differences in risk. Alternatively, given the borderline P value in the prior study, it is possible that the previously reported result represents a spurious association. It will be important to investigate the relationship between this SNP and AML risk in additional populations and larger cohorts.
Various studies had shown that single-nucleotide polymorphisms in the CASP9 gene are associated with the pathogenesis of different cancers. These SNPs or their haplotypes might alter the expression and functions of the CASP9 resulting in increased risk for AML and cancer development [12,13,14]. On the other hand, CASP9 -1263 G allele had shown to be significantly associated with reduced risk of other cancers among different researchers [11, 15, 16]. A functional explanation may lie in the fact that the CASP9-1263 A-to-G transition leads to the creation of an additional transcription factor (TF)-binding site which might increase the CASP9 expression and elevate apoptosis, leading to the elimination of malignant cells and association with reduced risk of many cancers [15, 17]. However, this controversy between our study result and these different studies might be due to an altered effect of this putative TF-binding site depending on other binding factors present in different tissues [14].
Regarding CASP9 712 SNP (rs4645981), the mutant CT/TT genotypes were detected in 47% of AML patients, while they were detected in 20% of controls, and the mutant T allele was significantly higher in patients when compared to the controls, conferring a significant threefold increased risk of developing AML. This was in concordance with Cingeetham et al.[1] who reported that CASP9 712 C to T transition reduces promoter activity and eliminates Krox-20, NF-1 and ETF-binding sites. Thus, the CASP9 712 T allele may lower CASP9 expression, altering the efficiency of apoptosis and, in turn, increasing the risk of AML. Earlier work supports this mechanism [18], and these conclusions are further supported by a prior meta-analysis which revealed increased susceptibility of T allele carriers to cancer [14, 19, 20]. On the contrary, genome-wide association studies (GWAS) have not implicated the 1p36 region where CASP9 resides as being associated with AML risk. Lack of a 1p36 signal in GWAS studies may reflect differences in study populations, including distinct ethnic background and/or environmental influences [9, 21].
Knowing that the malignant phenotype is likely to result from the accumulation of many minor genotypes, in the present work we tried to assess whether there was an association between the combined presence of the 2 polymorphisms and increased risk of AML development. When we analyzed AML patients with respect to the two polymorphisms, a substantial increase in the risk of AML development of the disease was observed. Thus, a significant association was observed suggesting that the polymorphisms interact to increase the risk of AML by about sevenfold for combined CASP9 1263 G and 712 T gene polymorphisms. To our knowledge, only Cingeetham et al. [1] had studied the effect of the combined presence of the 2 polymorphisms on the risk of AML. They analyzed the haplotypes of these two polymorphisms and observed that the presence of two risk alleles at CASP9 1263 G and CASP9 712 T position in a haplotype group increases the risk of AML by 11-fold and even a presence of single allele G at CASP9 − 1263 position in haplotype also confers a two-fold risk.
Studies investigating the effect of CASP9 1263A > G and 712C > T polymorphisms on outcomes and overall survival in AML are scarce. As a result, the current study tried to evaluate the association between these polymorphisms and prognosis, as well as overall survival. In our cohort, there was no impact of different CASP9 1263 genotypes on prognosis or overall survival (p value = 0.573 and 0.600, respectively), a finding in contrast to those previously reported by Anuradha [18] and Cingeetham et al. [1]. However, we did confirm an association between the CASP9 712C > T polymorphism and outcomes. Specifically, the presence of the CASP9 712 T allele was associated with a 26-fold increased risk of unfavorable outcomes (p value < 0.001), as well as decreased survival (p value = 0.002). This result confirms prior observations from Anuradha [18], who also reported reduced mean survival in AML patients with CASP9 712 CT and TT genotypes and further had poor survival outcomes. The rs4645981 T allele significantly reduces promotor activity, which may diminish CASP9 expression and its mediated apoptotic capacity to eliminate mutated or transformed cells, increasing the risk of cancer development and leading to poor survival outcome in patients [22].
Furthermore, the combined presence of CASP9 1263 G and 712 T alleles were found to have more significantly impact prognosis, increasing the risk of unfavorable outcome in AML by sevenfold compared to the CASP9 712 allele alone. This observation suggests that the inferior prognosis of the CASP 712 TT/CT genotypes may be dependent on the presence of a CASP 1263 alternative allele (GA or GG genotype).
There has been growing appreciation for the importance of germline variants in AML risk. Notably, much/most of the published literature to date has focused on rare germline alleles (in genes like CEBPA, RUNX1, DDX41) associated with highly penetrant risk of myeloid malignancy. In contrast, much less is known about the impact of common genetic variants with lower effect size, which may contribute collectively to polygenic risk.
The present study confirms prior observations suggesting that CASP9 promoter polymorphisms may represent one such example of common genetic variation impacting AML risk.
Conclusions
Here, we confirm an increased risk of AML in Egyptian individuals harboring the CASP9 712C > T promoter polymorphism. AML patients with this allele also had inferior outcomes in our cohort. Notably, risk was highest and outcomes worst in patients with both the 712C > T and 1263 A > G alleles, raising the possibility impacts may be greatest when these alleles are inherited as a haplotype. Thus, determining the CASP9 1263 A > G and 712 C > T gene polymorphisms is important for the prediction of both the risk of developing AML and the prognosis. This study is limited by the small sample size. Future larger studies with detailed treatment data to evaluate whether these polymorphisms specifically affect the outcome of drugs such as Venetoclax that target the apoptotic pathway and longer follow-up are warranted to validate the result of this study and make a firm conclusion.
References
Cingeetham A, Vuree S, Dunna NR, Gorre M, Nanchari SR, Edathara PM, Mekkaw P, Annamaneni S, Digumarthi RR, Sinha S, Satti V (2014) Association of caspase 9 promoter polymorphisms with the susceptibility of AML in south Indian subjects. Tumor Biol 35(9):8813–8822
Makhlouf MM (2011) Melanoma antigen encoding gene-A3 expression, its clinical significance, and its risk of developing acute myeloid leukemia. J Investig Med 59(7):1131–1136
Ibrahim AS, Khaled HM, Mikhail NNH, Baraka H, Kamel H (2014) Cancer incidence in Egypt: results of the national population-based cancer registry program. J Cancer Epidemiol 437971
Makhlouf MM (2016) Survivin and cyclin E2 genes expression in a cohort of Egyptian acute leukemia patients: clinical importance and future prospects. Cancer Biomark 16(1):181–189
Marques I, Teixeira AL, Ferreira M, Assis J, Lobo F, Mauricio J, Medeiros R (2013) Influence of survivin (BIRC5) and caspase 9 (CASP9) functional polymorphisms in renal cell carcinoma development: a study in a southern European population. Mol Biol Rep 40(8):4819–4826
El-Din MS, Raslan H, Abdel-Hamid S, Makhlouf M (2012) Detection of XRCC1 gene polymorphisms in Egyptian patients with acute myeloid leukemia. Comp Clin Pathol 21(5):505–513
Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz MJ, Porwit A, Harris NL, Le Beau MM, Hellström-Lindberg E, Tefferi A, Bloomfield CD (2009) The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood 114(5):937–951
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, Bloomfield CD, Cazzola M, Vardiman JW (2016) The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 127(20):2391–2405
Knight JA, Skol AD, Shinde A, Hastings D, Walgren RA, Shao J, Tennant TR, Banerjee M, Allan JM, Le Beau MM, Larson RA, Graubert TG, Cox NJ, Onel K (2009) Genome-wide association study to identify novel loci associated with therapy-related myeloid leukemia susceptibility. Blood 113(22):5575–5582
Makhlouf MM, Elwakil SG, Ibrahim NS (2017) Molecular and serological assessment of parvovirus B-19 infection in Egyptian children with sickle cell disease. J Microbiol Immunol Infect 50(5):565–569
Liamarkopoulos E, Gazouli M, Aravantinos G, Tzanakis N, Theodoropoulous G, Rizos S, Nikiteas N (2011) Caspase 8 and caspase 9 gene polymorphisms and susceptibility to gastric cancer. Gastric Cancer 14(4):317–321
Soung YH, Lee JW, Kim SY, Park WS, Nam SW, Lee JY, Yoo NJ, Lee SH (2006) Mutational analysis of proapoptotic caspase 9 gene in common human carcinomas. APMIS 114:292–297
Wang YX, Zhao L, Wang XY, Liu CM, Yu SG (2012) Role of Caspase 8, Caspase 9 and Bcl-2 polymorphisms in papillary thyroid carcinoma risk in Han Chinese population. Med Oncol 29(4):2445–2451
Theodoropoulos GE, Michalopoulos NV, Pantou MP, Kontogianni P, Gazouli M, Karantanos T, Lymperi M, Zografos GC (2012) Caspase 9 promoter polymorphisms confer increased susceptibility to breast cancer. Cancer Genet 205(10):508–512
Kesarwani P, Mandal RK, Maheshwari R, Mittal RD (2011) Influence of caspases 8 and 9 gene promoter polymorphism on prostate cancer susceptibility and early development of hormone refractory prostate cancer. BJUI 107(3):471–476
Gangwar R, Mandhani A, Mittal RD (2009) Caspase 9 and caspase 8 gene polymorphisms and susceptibility to bladder cancer in north Indian population. Ann Surg Oncol 16(7):2028–2034
Park JY, Park JM, Jang JS, Choi JE, Kim KM, Cha SI, Kim CH, Kang YM, Lee WK, Kam S, Park RW, Kim IS, Lee JT, Jung TH (2006) Caspase 9 promoter polymorphisms and risk of primary lung cancer. Hum Mol Genet 15(12):1963–1971
Anuradha C (2013) Analyses of MDM2 Gene expression and single nucleotide polymorphisms of DNA repair and intrinsic apoptotic pathways in the development of acute leukemia. http://shodhganga.inflibnet.ac.in
Luo G, Zeng Y, Zhu L, Zhang YX, Zhou LM (2009) Inhibition effect and its mechanism of nobiletin on proliferation of lung cancer cells. Sichuan Da Xue Xue Bao Yi Xue Ban 40(3):449–453
Xu W, Jiang S, Xu Y, Chen B, Li Y, Zong F, Zhao W, Wu J (2012) Meta-analysis of caspase 9 polymorphisms in promoter and exon sequence on cancer Susceptibility. PLoS ONE 7(5):e37443
Lv H, Zhang M, Shang Z, Li J, Zhang S, Lian D, Zhang R (2017) Genome-wide haplotype association study identify the FGFR2 gene as a risk gene for acute myeloid leukemia. Oncotarget 8(5):7891–7899
Edathara PM, Gorre M, Kagita S, Cingeetham A, Annamaneni S, Digumarti R, Satti V (2019) Influence of caspase 9 polymorphisms on the development of chronic myeloid leukemia- A case-control study. Gene-X 1:100002
Acknowledgements
The authors thank Kasr Al-Ainy School of Medicine and National Cancer Institute, Cairo University, Cairo, Egypt, for helping in performing this study and also the patients for their willing participation in this research.
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
The study was approved by the Ethical Committee of Kasr Al-Ainy School of Medicine, Cairo University, Egypt, and was conducted according to the ethics guidelines of the Declaration of Helsinki.
Informed consent
Written informed consents were taken from all participants in this study.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Makhlouf, M.M., Ayoub, M.A. & Mourad, D.F. The risk and prognostic influence of caspase 9 promotor polymorphisms in Egyptian patients with acute myeloid leukemia. J Hematopathol 15, 131–140 (2022). https://doi.org/10.1007/s12308-022-00508-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12308-022-00508-5