
Abstract
Purpose
Distal radius fractures are the most common upper limb fractures in adults (up to 18% of all fractures in the Emergency Department). Conservative management is possible for the majority, the preferred surgical technique being volar plate fixation. Dorsal bridge plating (DBP) is an alternative method of treatment for complex fractures. DBP acts as an internal fixator and can be used in patients needing early rehabilitation. This systematic review assesses the demographics, functional and radiological outcomes and complications of using DBP in patients with distal radius fractures compared to volar plate fixation.
Methods
A literature search of PubMed, Cochrane, EMBASE and Google Scholar was performed according to PRISMA guidelines. Seven hundred and sixty-one articles were found; 11 articles met the inclusion criteria. Cadaveric studies and case studies of less than five patients were excluded. Primary outcome measures were functional and radiological outcomes. Complications were recorded as secondary outcomes.
Results
Three hundred and ninety-four patients were included in the study with an average age of 54.8 years (53.9% male and 46.1% female). Weighted mean follow-up was 55.2 weeks; the mean time to plate removal was 17.3 weeks with a mean DASH score of 25.7. The weighted range of movement was 46.9° flexion, 48.8° extension, 68.4° pronation and 67.5° supination. The radiological parameters show satisfactory outcomes with a mean radial height of 10mm, volar tilt of 3.1°, ulnar variance of 0.5mm and radial inclination of 18.8°. The complication rate was 11.4%. Digital stiffness was the most common complication but improved if tenolysis was performed at plate removal.
Conclusions
DBP is a good alternative to volar plating for complex distal radius fractures. The functional outcomes showed a slight loss of range of movement, whereas the radiological outcomes were within recommended limits. A significant disadvantage of the plate is the need for further surgical removal.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Distal radius fractures are the most common upper limb fractures and account for 17–18% of all adult fractures in the Emergency Department [1,2,3,4]. Operative techniques used to manage distal radius fractures include closed reduction, percutaneous K-wiring and internal/external fixation; of which, Volar locking plates have become the operative technique of choice [5].
This said, stability can be a concern when volar locking plates are used to manage patients with highly comminuted intra-articular fractures, additional radiocarpal ligamentous injuries, dorsal shearing fractures and those with poor bone quality [1, 5,6,7]. As a result, stabilisation of these fractures using an external fixator has traditionally been used for such complex injuries. This allows soft tissues to recover from the trauma and gives time for further imaging and planning, whilst reducing pain for the patient. However, these constructs are heavy, do not allow easy use of the arm perioperatively and are often complicated with pin site infections, stiffness and have the potential for fracture mal-reduction due to the pins being able to be accessed externally and knocked.
The dorsal bridge plate (DBP) was first described in 1998 [8]. The DBP has been proposed for use in polytrauma patients requiring damage control surgery or those needing to ambulate early in the post-operative period as it gives enough stability for weight bearing, irrespective of fracture configuration [9, 10]. In this way, a DBP is considered by many to be preferential to an external fixator, giving the same fracture stabilisation without the complication profile [2, 3, 8]. The plate can be left in for longer than an external fixator; however, the plate requires surgical removal after 12–16 weeks [3, 11].
There remains variation in practice amongst clinicians treating DRFs suitable for either treatment due to the limited literature available. Previous reviews have analysed functional and radiological outcomes in isolation [2]. The aim of this study is combine such studies to give a more powerful representation of the radiological and functional outcomes of DBPs. The study will also report on the complications associated with DBP in distal radius fractures compared to volar plate fixation and summarise findings in an effort to further inform and standardise clinical practice.
Method
Protocol and registration
The review was registered on PROSPERO prior to starting.
Literature search and selection of studies
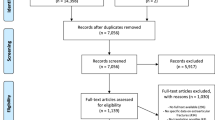
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, EMBASE, PubMed, Cochrane and Google Scholar and were all searched using (((Distract*) AND (Plat*)) OR ((Bridg*) AND (Plat*))) AND (distal radius) on 1st May 2021. There was no date restriction. Bibliographies of all identified papers were reviewed to ascertain if any listed were suitable for inclusion (n = 761).
Duplicate studies identified were removed (n = 534). The articles were assessed by two people. First, the titles and abstracts were screened against the inclusion criteria as shown in Table 1 for their relevance (n = 534). Full articles were then analysed according to the inclusion and exclusion criteria. A modified PRISMA flowchart is used to display the methodology of this search in graphic form (Fig. 1).

The modified PRISMA flowchart for included and excluded studies
Data extraction and outcomes
A pilot study was performed in order to create a proforma. The data collected included: study designs, demographics of the population included in the study, sample size, outcomes and complications. All the data were collated on Microsoft Excel.
The primary outcomes:
-
Demographic data
-
Mechanism of injury
-
Functional outcomes including disabilities of the arm, shoulder and hand (DASH) scores and range of movement (ROM) including grip strength, flexion, extension, pronation, supination, ulnar deviation and radial deviation. DASH scoring system quantifies the disability with a range between 0 (no disability) and 100 (maximum disability).
-
Radiological outcomes including radial height, volar tilt, ulnar variance and radial inclination
Secondary outcomes:
-
Complications including infection, need for further operations, pain, tendon injuries and mal-or non-unions.
The primary and secondary outcomes were analysed in a quantitative manner. Weighted averages were calculated depending on the studies that analysed that particular outcomes. The outcomes were presented as a collective as seen in the results. Heterogeneity was evaluated to see if quantitative assessment with meta-analysis was possible.
Data analysis
Individual studies were assessed for risk of bias using the Risk of Bias In Non-Randomised Studies of Intervention (ROBINS-I) tool. The leads to the studies being labelled ‘low risk’, ‘moderate risk’, ‘high risk’ or ‘critical risk’ based on seven different criteria.
Results
The initial search found 761 studies, and 11 were eligible for inclusion [1, 4, 5, 12,13,14,15,16,17,18,19]. Of these, nine were retrospective [1, 4, 5, 12, 14, 15, 17,18,19], one was observational [16] and one was a case study of more than five participants [13]. This accounted for 394 patients.
Of those that were excluded 227 studies were duplicates, 16 were cadaveric, 14 were case reports of less than five participants, two were not in English and the remainder were not relevant. Due to the heterogeneity of data collection methods and methodology between studies, a meta-analysis was not possible. Therefore, results are presented of a quantitive nature.
Demographics
Table 2 describes the demographics from the included studies. The weighted mean age was 52.1 with a range from 41 to 72 years. The follow-up of patients was between 19.5 and 150.8 weeks (weighted mean 55.2 weeks). The weighted mean time to plate removal was 17.3 weeks. 58.9% of the participants were male. The majority of mechanisms of injuries were high-energy falls and road traffic accidents as shown in Table 3.
The majority of the papers subclassified the fracture pattern into AO classification. Of those that subclassified, 86% were C-type fractures, 4% were B-type and 10% were A-type. Only five studies documented if any of the fractures were open, of these, the rate of open fractures was 13.6%. A further breakdown of the fracture classification can be seen in Table 4.
Functional outcomes
The functional outcomes are summarised in Table 5. The ROM for extension and flexion (95.7°), pronation and supination (135.9°) and ulnar and radial deviation (28.8°). Grip strength was only documented in three studies and the weighted mean was 71.6% compared to the contralateral side. The weighted mean DASH score averaged 28.6 and the QuickDASH score 19.8.
Radiological outcomes
Table 6 shows the accumulated radiological outcomes. The articular step-off was recorded as < 2 mm in all papers, except one patient in Huish et al. [12].
Complications
Table 7 is a summary of the different complicate rates. The most common complications were digital stiffness, pain and hardware failure. Overall, the complication rate was 11.4%.
Risk of bias
The risk of bias for each article can be seen in Table 8. All studies had an overall risk of bias of moderate or high. This was mainly due to the confounding factors throughout each of the articles. In addition, due to all studies being retrospective, there was a moderate risk of bias in participation selection and classification of interventions.
Multiple studies had incomplete datasets resulting in moderate attrition bias, whilst Lauder et al. [4] had a participation rate of 18% making the attrition bias high risk. The detection bias was low throughout, whereas there was some reporting bias due to gaps in the reported outcomes.
Discussion
This systematic review evaluates the radiological, functional outcomes and complications associated with DBP fixation of DRFs. Previous systematic reviews have looked at individual outcomes [2, 6], but none looked at a combination of radiological and functional outcomes as well as complications. The literature reveals that radiological outcomes following a DBP are satisfactory, with a complication rate of 11.4%.
Dorsal bridge plates are considered for complex and unstable distal radius fractures. Therefore, these are patients who are expected to have poor outcomes. This review shows that the radiological and functional outcomes are satisfactory for these fracture patterns.
Radiological outcomes
One concern regarding DBP is the possibility of less satisfactory radiological outcomes compared to volar locking plate fixation, potentially resulting in poorer overall outcomes. However, our review indicates that DBP yields radiological results comparable to those achieved with volar locking plate fixation in AO C2/3 distal radius fractures [20].
Standard radiological parameters such as volar tilt, radial inclination and radial height typically fall within the ranges of 7–15°, 15–25° and 8–14 mm, respectively, with acceptable ranges of < 5° dorsal angulation, > 15 degrees and > 8 mm. In this review, the DBP consistently achieved satisfactory radiological outcomes, within these acceptable ranges (3.1° for volar tilt, 18.8° for radial inclination and 10 mm for radial height). In contrast, fixation with volar locking plate failed to meet the acceptable standard for radial inclination (14.2°), although it did meet requirements for volar tilt (12.5°) and radial height (10.5 mm). Additionally, we observed acceptable articular step-off which was within the range of < 2 mm.
Comparison between DBP and volar locking plate fixation revealed that DBP consistently achieved acceptable radiological outcomes across all parameters. However, whilst volar plate fixation in AO C2/3 fractures met the criteria for volar tilt and radial height, it did not achieve acceptable degrees of radial inclination.
This review suggests that DBP offers a viable option for achieving satisfactory radiological outcomes in complex DRFs, potentially reducing the incidence of malunions. However, it is worth noting that DBP necessitates a second operation for plate removal. Furthermore, it is important to acknowledge that radiological outcomes may not necessarily correlate with functional outcomes, which ultimately determine the patient’s quality of life [6].
Functional outcomes
As highlighted in Fares et al. [2], the concerns regarding DBP are that prolonged immobilisation leads to a reduced ROM. However, this analysis demonstrates that functional ROM with DBP is significantly improved compared with the use of external fixators, an alternative mode of fixation for these complex fractures, and is comparable to that achieved with volar locking plates.
In this review, the average ROM values for flexion, extension, pronation and supination in patients treated with DBP were 46.9°, 48.8°, 68.4° and 67.5°, respectively. In comparison, Oner et al. reported improved flexion, extension and supination (79.5°, 62.8° and 71.7°, respectively) in the use of volar locking plates in AO C2/3 fractures; however, there was a reduction in pronation (64.4°). Despite this, the results indicate that a functional arc of 95.7° can be achieved with DBP fixation, which exceeds the range for most activities of daily living.
Regarding patient-reported outcomes, the DASH score at final follow-up was 25.1, measured between 19.5- and 150.8-week post procedure. However, it is important to note that Ruch et al. [19] reported a decrease in DASH score from 33.8 at 6 months to 11.5 at 2 years, suggesting that our DASH score may not fully capture the long-term outcomes of DBP [19]. In contrast, Oner et al. [20] reported a Quick DASH score of 4.94 at 1-year post-volar locking plate fixation [20]. Similarly, the grip strength with a volar plate was found to have a 10.4% loss compared to a 28.4% loss with DBP.
In summary, whilst DBP demonstrates acceptable functional outcomes, they are still inferior to volar locking plates.
Complications
In this review, the overall rate of complications associated with DBP was 11.4%, which is notably lower compared to reported complication rates of up to 23% for volar plating [21] and 63% for external fixation [22]. The most frequently encountered complications included digital stiffness, pain, hardware failure and infection.
An analysis by Hanel et al. [18] found that the complication rate was influenced by the duration the plate remained implanted. Patients who retained the plate for more than 16 weeks experienced a complication rate of 20.8%, whereas those who underwent plate removal earlier had a lower rate of 8.5% [18]. In this review, the mean time to plate removal in this review was 17.3 weeks.
Although the incidence of digital stiffness with DBP was relatively high at 18.2%, it was substantially lower than observed with external fixators [16]. Rates of digital stiffness improved when tenolysis was performed during plate removal [15].
Hardware failure was only observed in patients who retained the plate for longer than 6 months, after the fracture has healed [11, 15], indicating a need for plate removal. Additionally, the choice of plate for fixation plays a crucial role. Studies have shown that the 2.4-mm plate may not adequately support the axial weight bearing in polytrauma patients, potentially leading to early hardware failure. In cases where early weight bearing is needed, consideration should be given to using a 3.5-mm DBP [23].
The complications rates associated with DBP were significantly lower than those observed with volar plating in C-type fractures, as well as external fixators. Sharareh et al. [5] reported an overall complication rate of 11.3% for volar plates, with rates as high as 20% in C-type fractures. Whilst this review did not specifically analyse complication rates by fracture classification, these findings support the use of DBP in C-type fractures [5].
Limitations
This systematic review is limited by the number of papers and consequently the number of patients analysed. Currently, there is a sparsity of high-level studies in the literature, with only retrospective analyses and case studies available. These study types have inherent limitations such as: loss to follow-up, inconsistent evaluation of the functional and radiological outcomes and potential bias introduced by operating surgeons reporting the results during follow-up. In addition, the subjective interpretation of ROM further adds to the complexity of assessing outcomes [18].
The follow-up periods in the included studies were relatively short, with only two studies extending beyond 100 weeks [4, 19], while the remainder were less than 55 weeks. Consequently, the long-term effects, as well as the functional and radiological outcomes associated with DBP, remain uncertain. Additionally, the heterogeneity of outcomes in this review may have introduced interpretation bias.
The fact that five out of the 11 studies share authors suggest a limited pool of research available and raise concerns about potential bias. Previous systematic reviews have also included a study by Jain et al. who have since been retracted due to methodological flaws [24]. Furthermore, some of these reviews incorporated papers consisting of only one or two case studies, heightening the risk of bias.
To mitigate these limitations and provide more robust evidence, a randomised control trial comparing all three techniques (volar plating, DBP and external fixation) is warranted. Such a trial would not only help to minimise bias but also offer more reliable insights into the comparative effectiveness of these approaches.
Conclusion
Despite the small cohort of patients, this review has shown that DBP has been used with adequate outcomes, comparable in radiological and functional outcomes to current fixation methods and a significantly lower complication rate than external fixation. Further research with meta-analysis in the future is needed. The DBP should be considered by clinicians as an option for select patients and for patients with complex fractures.
References
Richard MJ, Katolik LI, Hanel DP, Wartinbee DA, Ruch DS (2012) Distraction plating for the treatment of highly comminuted distal radius fractures in elderly patients. J Hand Surg Am 37(5):948–956
Fares AB, Childs BR, Polmear MM, Clark DM, Nesti LJ, Dunn JC (2021) Dorsal bridge plate for distal radius fractures: a systematic review. J Hand Surg Am 46:627e1
Wang WL, Ilyas AM (2020) Dorsal bridge plating versus external fixation for distal radius fractures. J Wrist Surg 9(2):177–184
Lauder A, Agnew S, Bakri K, Allan CH, Hanel DP, Huang JI (2015) Functional outcomes following bridge plate fixation for distal radius fractures. J Hand Surg Am 40(8):1554–1562
Sharareh B, Mitchell S (2020) Radiographic outcomes of dorsal spanning plate for treatment of comminuted distal radius fractures in non-elderly patients. J Hand Surg Global Online 2(2):94–101
Beeres FJP, van de Wall BJM, Hug U, Schep NWL, Babst R, Link BC, et al. (2021) Temporary spanning plate wrist fixation of complex distal radius fractures: a systematic review of 353 patients. Eur J Trauma Emerg Surg
Lam F, Jaysekera N, Karmani S, Jupiter JB (2006) What’s new in the treatment of distal radius fractures? Curr Orthop 20(3):208–211
Burke EF, Singer RM (1998) Treatment of comminuted distal radius with the use of an internal distraction plate. Tech Hand Up Extrem Surg 2(4):248–252
Lauder A, Hanel DP (2017) Spanning bridge plate fixation of distal radial fractures. JBJS Rev 5(2):e2
Papadonikolakis A, Ruch DS (2005) Internal distraction plating of distal radius fractures. Tech Hand Up Extrem Surg 9(1):2–6
Boateng HA, Payatakes AH (2015) Distal radius fractures: dorsal bridge plating. Oper Tech Orthop 25(4):282–287
Huish EG Jr, Coury JG, Ibrahim MA, Trzeciak MA (2018) Radiographic outcomes of dorsal distraction distal radius plating for fractures with dorsal marginal impaction. Hand (N Y) 13(3):346–349
Tinsley BA, Ilyas AM (2018) Distal radius fractures in a functional quadruped: spanning bridge plate fixation of the wrist. Hand Clin 34(1):113–120
Hanel DP, Lu TS, Weil WM (2006) Bridge plating of distal radius fractures: the Harborview method. Clin Orthop Relat Res 445:91–99
Dodds SD, Save AV, Yacob A (2013) Dorsal spanning plate fixation for distal radius fractures. Tech Hand Up Extrem Surg 17(4):192–198
Carula BC, Pereira MDS, Ferreira APB, Ayzemberg H, Steglich V, Stangarlin TS (2021) Analysis of the clinical and radiological results of bridge plate versus external fixation in comminuted distal radius fractures. Rev Bras Ortop (Sao Paulo) 56(1):61–68
Bouvet C, Beaulieu JY (2013) Treatment of highly comminuted distal radius fractures with temporary distraction plate: case reviews. Swiss Med Wkly 143:12S
Hanel DP, Ruhlman SD, Katolik LI, Allan CH (2010) Complications associated with distraction plate fixation of wrist fractures. Hand Clin 26(2):237–243
Ruch DS, Ginn TA, Yang CC, Smith BP, Rushing J, Hanel DP (2005) Use of a distraction plate for distal radial fractures with metaphyseal and diaphyseal comminution. J Bone Joint Surg Am 87(5):945–954
Öner K, Paksoy AE, Durusoy S (2021) Comparison of two surgical methods in the treatment of intra-articular distal radius fractures: volar locking plate and K-wire augmented bridging external fixator. Ulus Travma Acil Cerrahi Derg 27(6):684–689
Kwak JM, Jung GH (2018) Biologic plating of unstable distal radial fractures. BMC Musculoskelet Disord 19(1):117
Weber SC, Szabo RM (1986) Severely comminuted distal radial fracture as an unsolved problem: complications associated with external fixation and pins and plaster techniques. J Hand Surg Am 11(2):157–165
Huang JI, Peterson B, Bellevue K, Lee N, Smith S, Herfat S (2018) Biomechanical assessment of the dorsal spanning bridge plate in distal radius fracture fixation: implications for immediate weight-bearing. Hand (N Y) 13(3):336–340
Jain MJ, Mavani KJ (2016) A Comprehensive Study of Internal Distraction Plating an Alternative Method for Distal Radius Fractures. J Clin Diagn Res. https://doi.org/10.7860/JCDR/2016/21926.9036
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Drummond, I., Durand-Hill, M., Jones, N. et al. Systematic review: dorsal bridge plating in distal radius fractures. Musculoskelet Surg (2024). https://doi.org/10.1007/s12306-024-00822-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12306-024-00822-4