
Abstract
The study aimed to determine the sociodemographic and psychological profiles of drivers with a history of motor vehicle crashes (MVCs), following the contextual-mediated model of crash involvement, and trying to define similarities and differences with drivers without MVCs. Although road trauma prevention has become a central public health issue, the study of psychological determinants of MVCs does not have consistent results due to methodological and theoretical weaknesses. Three-hundred and forty-five active drivers (20% females) completed an extensive office-based fitness-to-drive evaluation including measures of cognition, personality, self-reported driving-related behaviors, attitudes, as well as computerized measures of driving performance. The Classification and Regression Tree method (CART) was used to identify discriminant predictors. The classification identified several relevant predictors; the personality trait of Discostraint (as a distal context variable; cut-point: 50 T points) and motor speed (as a proximal context variable; cut-point: 64 percentile ranks). The global classification model increased approximately 3 times the probability of identifying people with a history of MVC involvement, starting from an estimated prevalence of being involved in an MVC in a period of five years in the population of active drivers. Consistent with the ‘contextual-mediated model of traffic accident involvement’, the results of the present study suggest that road trauma analysis should focus on both distal and proximal driver-related factors by paying attention to their association in determining MVCs. These results represent a valuable source of knowledge for researchers and practitioners for preventing road trauma.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Around the world, approximately 1.3 million people die each year from injuries resulting from motor vehicle crashes (MVCs) (WHO, 2018). Therefore, MVCs constitute a significant public health problem in many countries (Gicquel et al., 2017). The issue, attracting significant research interest and prompting authorities to identify the cause of these events (Javadi et al., 2015), remains an important research topic as MVCs, considered ‘rare’ events (Theofilatos et al., 2016), still account for one of the most common causes of death and/or serious injuries worldwide. Several factors, acting in isolation or in combination, determine MVC involvement, including vehicle factors, road environment, and human factors (Eboli & Forciniti, 2020). Vehicle-related factors include vehicle type and manufacturer, as well as vehicle maintenance and its actual performance which are associated with MVC (Mohamed et al., 2023). Environmental factors, such as increased motorization and traffic density, have been found to be positively associated with increased injuries and deaths (La Torre et al., 2007; Yasmeen, 2019). However, human factors have been identified as the leading factor, directly or indirectly, contributing to more than 90% of MVCs (Evans, 1991; NHTSA, 2019). For this reason, most studies exploring the causes of MVCs have focused on driver-related variables such as individual characteristics (e.g., social, and demographic factors), driving style and behaviors, intoxicated driving, cognitive functioning, risk perception, disability, personality traits, distraction, drowsiness, and fatigue (Wang et al., 2005; Javadi et al., 2015). Moreover, social and cultural factors have also been considered because of their influence on driving behavior. For example, illegality, social needs as well as a feeling of religious and national identity have been demonstrated to be associated with MVCs in a sample of Iranian drivers (Javadi et al., 2015), while observation and interpretation errors as well as inattention were found among main causes of MVCs in the European context (i.e., Germany, Finland, Italy, The Netherlands, Sweden, and United Kingdom; Thomas et al., 2013).
Early studies on psychological variables influencing MVC involvement have proposed a framework of crash-related factors including those that are extrinsic (but related) to driving (i.e., demographic variables, cultural features, cognition, personality, habits, values, etc.), which are different to those that are intrinsic to driving (i.e., driving behavior/performance, driving skills/style; Evans, 1991; Elander et al., 1993). Sümer (2003) replicated and extended this framework from the point of view of the ‘driving context’ by developing and testing the ‘contextual-mediated model of traffic accidents involvement’. According to this model, variables of the distal context (i.e., demographics, personality, etc.) influence the likelihood of being involved in MVCs both directly and indirectly, through the mediation of variables of the proximal context (i.e., driving behaviors and driving skills).
The present study focuses on the socio-demographic and psychological determinants of MVCs. The following section describes main findings of studies on human-related predictors of MVCs including drivers’ sociodemographic characteristics, cognitive functioning, personality traits as well as measures of driving-related behavior, attitudes, and performance.
Driver-related factors associated with MVCs
Sociodemographic characteristics
A recent review has focused on sociodemographic factors associated with MVC deaths and reported that most studies have found negative associations between education level and these events (Saeednejad et al., 2020). The authors also found that MVC deaths were positively associated with rural settlement and marital status, with higher MVC-related deaths for divorced, single, and widowed persons than for those who were married (Spoerri et al., 2011; Saeednejad et al., 2020). In the study of Meles et al. (2021), involving a population of Ethiopian drivers, being an experienced driver predicted the level of MVC-related injury severity. On the other hand, the authors found that being in a private vehicle, owning the vehicle, driving a heavy truck or cross-country bus, and types of MVCs involving pedestrians were associated with a reduced severity of MVC-related injuries. In addition, there is evidence from diverse global sources which indicates that individual differences in age and sex are the main demographic determinants of MVCs, with younger and male drivers being identified as having the highest MVC risk (Noland & Quddus, 2004; Ma et al., 2021; Saeed et al., 2023). These differences have been attributed to various psychological factors, such as personality profiles, cognitive and motor functioning, as well as driving-related behaviors and attitudes that influence the actual driving performance. The results of the studies of Begg and Langley (2001), Clarke et al. (2006), and Curry et al. (2012), which were conducted with samples of drivers from New Zealand, England, and the United States, respectively, showed that young male drivers are at a higher risk of MVC involvement due to engaging in risky behaviors, such as speeding and driving under the influence of drugs or alcohol, compared to young female drivers.
Personality
Concerning measures of personality and mental health, irritability and anger have been identified in many studies as significant contributors to MVCs (Giquel et al., 2017). The findings of Zhang et al. (2019) suggest that individuals with high levels of impulsivity and low levels of self-control were more likely to engage in risky driving behaviors and thus, more likely to be involved in MVCs. Similarly, a study by Ünal, (2006) found that individuals with higher levels of sensation-seeking and lower levels of self-control had a higher likelihood of being involved in an MVC. Specifically, the authors reported that males showed greater inclination towards sensation seeking, resulting in more self-reported MVCs, and driving violations compared to females. On the other hand, females displayed higher levels of sensitivity to punishment, which has been identified as a protective factor against engaging in risky driving behaviors (Costantinou et al., 2011). In their study, Eduardo and Ildefonso (2020) found a significant correlation between personality and MVCs among males, whereas this relationship was not significant among females. Considering young drivers, previous research has highlighted that sensation-seeking, together with trait anxiety and anger, are predictors of aberrant driving behaviors and MVCs (Javadi et al., 2015; Zicat et al., 2018). Conversely, the association between personality attributes and MVCs in older drivers is less evident, since reckless driving tends to be attenuated in this age cohort (Alavi et al., 2017). However, studies have shown that anxiety, extraversion, conscientiousness, and type A personality are associated to risky driving and driving errors in older drivers (Lucidi et al., 2019; Adrian et al., 2011). Beside personality traits, and interacting with them, cognitive and mobility functioning play a crucial role influencing the fitness-to-drive and, in turn, the involvement in MVCs (Kwok et al., 2015; Ledger et al., 2019a, 2019b; Tinella et al., 2020, 2021a, 2021b).
Cognition
Driving a motor-vehicle requires an interaction of multiple cognitive abilities including attention, psychomotor and perceptual skills, executive functions, visuospatial skills, and memory (Anstey et al., 2005). Previous research has demonstrated that a driver’s cognitive and decision-making abilities significantly affects their risk of MVCs (Wang et al., 2021). In addition, previous research has demonstrated that incomplete maturation of cognitive functioning in young drivers, as well as initial cognitive decline in older drivers, may contribute to a higher rate of MVCs in these age groups (Svetina, 2016; Ledger et al., 2019a; Tinella et al., 2020). This is due to the inverted U-shaped relationship between age and cognitive functioning (Salthouse, 2000, 2009). Therefore, the relationship between cognition and driving performance shows similar patterns in both young and older drivers (Ledger et al., 2019b). In particular, the performance in tests of visual attention, visual memory, and mental status have shown to similarly predict speeding and lane deviation in younger and older drivers. Since driving is mainly a visuospatial task (Sommer et al., 2010), numerous studies have considered measures of this cognitive domain attempting to predict driving behavior and MVCs. Indeed, visual acuity, visual attention, motion detection, visuo-constructive abilities, and immediate visuo-spatial memory have been identified as significant predictors of real-world driving, especially for older drivers (Anstey et al., 2005; Mathias & Lucas, 2009). Other studies have shown that specific strategies of spatial orientation affect driving behaviors (Nori et al., 2020) and that visuospatial representation and transformation skills are involved in driving performance (Kunishige et al., 2019; Teranishi et al., 2019; Tinella et al., 2020, 2021a, 2021b). Considering the above, older drivers’ errors may be affected by age-related declines in visual, cognitive, and mobility functioning (Janke, 1991; Rolison et al., 2018). Furthermore, poor visual functioning and cognitive abilities are both considered risk factors for older drivers’ MVC involvement (Ball et al., 2006, 2010; Owsley et al., 1991, 1998). Taken together, all the above-mentioned psychological factors contribute to shape and influence more specific driving-related constructs such as driving attitudes, driving behaviors, and driving performance.
Behaviors, attitudes, and performance
Young drivers have significantly more road rule violations than older drivers (Kweon & Kockelman, 2003; Williams & Shabanovab, 2003), and this propensity to engage in risky driving may be affected by careless attitudes toward traffic safety (Zicat et al., 2018). Positive attitudes toward speeding have been found to predict at-fault MVCs in young drivers (Hassan & Abdel-Aty, 2013). Compared with older drivers, younger are more likely to engage in speeding behaviors and reckless driving, loss of control, failure to detect another vehicle, and higher levels of speed deviatation (Doroudgar et al., 2017; Ledger et al., 2019a, 2019b; Braitman et al., 2008). In contrast, the MVCs of older drivers are more likely to be affected both by driver errors and lapses. Common causes of MVCs in older drivers include: failure to yield right of way, non-compliance with signs and signals, difficulty seeing objects, making improper turns and lane changes, driving error at intersections and when making turns (Hakamies-Blomqvist, 1993; McGwin & Brown, 1999; Langford & Koppel, 2006). The evidence reported above suggests that the driver’s demographic characteristics interacts with their cognitive and personality profile by determining specific patterns of driving behaviors and attitudes towards safety which in turn affect risk of MCV involvement.
The present study
According to the ‘contextual mediated model of traffic accident involvement’ (Sumer, 2003), variables referred to the distal context of driving affect the involvement in MVCs both directly and indirectly, through the mediation of variables included in the proximal context. Despite this model being highly referenced in driving behavior research, to the best of our knowledge, no previous study has sought to classify psychological determinants of MVCs by directly investigating main effects and interrelationships between variables in a classification model. In addition, research on contributing factors affecting MVCs historically present theoretical and methodological deficiencies. For example, Af Wåhlberg (2003) identified three main issues characterizing (psychological) research on predictors of MVCs including: (a) information on the time period for MVCs used as a dependent variable, (b) the reliability of variables used as predictors, and (c) the driver’s culpability for MVCs. These limitations still characterize part of research on MVC predictors making results often tentative and with scarce replicability and/or generalizability. On the other hand, obtaining and analysing data in forensic clinical settings can be challenging, particularly for MVCs. The validity of the data may be affected by various factors such as retrospective analysis (archive data), non-standardized assessment procedures, and the risk of bias due to impression management by respondents (Bosco et al., 2020; Martino et al., 2016). These limitations can undermine the validity of the data at the acquisition phase.
The present study sought to address some of the above-mentioned gaps by investigating sociodemographic and psychological predictors of MVCs following the ‘contextual-mediated model of traffic accident involvement’ (Sümer, 2003). The aim of this study was to analyze both sociodemographic and psychological characteristics of drivers who have been involved in MVCs, trying to establish relationships and differences with those who have not. The study utilized rigorous machine learning techniques such as classification trees, which have been employed in previous research studies (Abbasi et al., 2021; Portela-Pino et al., 2021; Faílde-Garrido et al., 2022; Zamzuri and Qi, 2022). Unlike previous studies, the current study interpreted the results of the Classification And Regression Trees (CART) models through a Bayesian factor and conditional probabilities based on frequencies emerged by models’ outputs. Additionally, the association between the obtained model of classification with the participants’ belonging to different groups of drunk drivers (i.e., caught for drunken driving), systemic drivers (i.e., with a diagnosed systemic illness), and controls (healthy drivers) was also explored. Following the above-mentioned theoretical model, predictors belonging to both the distal and the proximal context were expected to significantly discriminate participants with and without MVC involvement.
Methods
Participants
A total sample of 345 drivers participated in the study (Female, 22%). One-hundred and eighty-seven participants were recruited from the community-dwelling (Females, 34.2%; Age: M ± sd = 38.3 ± 17.8; years of education: M ± sd = 12.2 ± 2.3), while one-hundred and fifty-eight drunk and systemic drivers (Females, 7.7%; Age: M ± sd = 50.6 ± 20.4; years of education: M ± sd = 11.4 ± 3.7) were recruited with the help of the local healthcare authority. The group of drunk drivers included 90 drivers caught for drunken driving (i.e., BAC level between 0.8 and 1.5 g/l) while the group of systemic drivers included 68 participants with a diagnosed systemic and/or multi-systemic illness limiting their driving license (i.e., cardiovascular, metabolic, pulmonary, rheumatic diseases). All participants were required to: have Italian as their mother tongue; hold a valid current driver’s license (provisional or above); have normal or corrected to normal vision; have driven more than one time within the last month; and not currently (or previously) be a professional driver (e.g., taxi driver, truck driver, transporter on delivery, etc.). Considering the ratio between independent predictors and number of observations, the sample size of the present study was consistent with those of previous studies using CART in the field of road safety (Faílde-Garrido et al., 2022), and greater than the smallest sample used for CART simulations in epidemiological studies (i.e., 150–200 observations; Venkatasubramaniam et al., 2017; Wilcox & Hripcsak, 1999; Chapman & Haug, 1999). However, the sample size of the present study also satisfies the general rule of thumb of 10–20 observations for each independent variable (Jerkins & Quintana-Ascencio, 2020). All participants were able to perform all the tasks included in the assessment at the time of data collection and provided informed consent prior to the enrolment in the present study. The Ethical Committee of the Department of Education, Psychology, and Communication approved the study protocol (approval code: ET-20-17), and the study was conducted following the Helsinki Declaration and its later amendments.
Materials and procedures
Participants in the community-dwelling group were recruited via proxy informants, generally undergraduate and graduate students, trainees, and employers of the Department. Both drunk drivers and systemic drivers were recruited via the local health authority (Commissione Medica Locale). All participants were enrolled and completed the evaluation protocol between October 2019 and February 2021. Participants were asked to report if they have been involved in an MVC(s) during the previous five years, and if so, to provide a detailed description of the event (i.e., the more recent MVC if more than one was reported). An independent panel of experts (i.e., a coroner and a forensic psychologist), blind to the study aims, was established to determine driver’s culpability in the reported MVC, rating each event as “at-fault” or “not-at-fault” based on a chart review and following the existing scientific literature. The assessment protocol included questions related to participants’ socio-demographic and driving characteristics, a brief clinical anamnesis, questionnaires on driving behaviors, attitudes, and personality as well as cognitive tests and a computerized driving task. Detailed descriptions of these measures are reported below. All participants were assessed individually in a quiet and well-lit room without disturbances. Both the drunk and systemic groups of drivers were assessed at the mobility center of the city, while participants within the community-dwelling group were assessed in the Department of Psychology of the University using the same apparatus. Each assessment session was conducted by trained research assistants and lasted 120–150 min, with breaks provided as requested by participants.
Cognitive measures
Global cognitive functioning was evaluated using the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005; Bosco et al., 2020). This test showed good reliability (Cronbach’s α = 0.83) measuring different cognitive domains such as visuospatial-executive, naming, memory, attention, orientation, and language. The best cut-off used in an Italian sample for discriminating participants with probable cognitive impairment was demonstrated elsewhere and it was 17 (Bosco et al., 2017).
To evaluate participants’ object-based spatial transformation, the Mental Rotation Test (MRT) has been administered (Vandemberg & Kuse, 1978). The MRT is a paper-and-pencil assessment consisting of 20 items, each of which presents a two-dimensional representation of a three-dimensional figure made up of cubes. For each item, there is a criterion figure and four response options, including two correct and two distractors. The correct options are structurally identical to the criterion but are displayed in a rotated form. Participants are required to identify the two figures out of the four response options that match the criterion figure in terms of their rotation. The MRT is divided into two parts, and participants are given three minutes to complete each part. The entire procedure takes approximately 10 min. This test showed good reliability (Cronbach’s α = 0.81).
To measure self-based spatial transformation, the Object Perspective-Taking Test was administered (OPT; Hegarty & Waller, 2004). This paper-and-pencil test consisted of 12 items, featuring a configuration of seven objects on the top half of the page. Participants were instructed to imagine standing at one object, facing another, and identifying the direction to a third object (the target). They drew an arrow from the center of a circle at the bottom of the page, which represented their imagined standing point, towards the target direction. The item score was based on the absolute directional error, in degrees, between the participant’s answer and the correct target direction. The total score was the average deviation across items, with a higher score indicating lower OPT ability. The test had a time limit of five minutes and took around 10 min to complete. This test showed good reliability (Cronbach’s α = 0.79).
Personality measures
The Personality Psychopathology Five (PSY-5) traits were measurred using the Minnesota Multiphasic Personality Inventory-2 (MMPI-2; Butcher et al., 1989), a 567-item questionnaire that measures personality profiles through true-or-false answers. T-scores are used to report personality scale scores. In the Italian validation of MMPI-2, a T-score of 65 or higher is considered clinically significant. The PSY-5 scale comprises traits of aggressiveness (AGGR), psychoticism (PSYC), constraint (DISC), negative emotionality/neuroticism (NEGE), and introversion (INTR). These traits are deemed important in daily life and can impact clinical issues according to the Personality Psychopathology Five model. The “Gough dissimulation index” (F-K) has been calculated by subtracting the raw scores of validity scales F and K. All these scales showed moderate reliability coefficients: AGGR (α = 0.67), PSYC (α = 0.69), DISC (α = 0.64), NEGE (α = 0.73), INTR (α = 0.71).
Driving behaviors and attitudes
The Driving Behavior Questionnaire (DBQ; Reason et al., 1990) was used to measure aberrant driving behaviors. The questionnaire consists of 28 items that measure three types of driving behaviors: violations, lapses, and errors. Participants rated how frequently they engage in each behavior on a 6-point Likert scale ranging from “never” (0) to “always” (5). Higher scores indicate more frequent abnormal driving behaviors. The total score was used in the current analyses. The questionnaire showed good reliability (Violations: α = 0.73; Lapses: α = 0.79; Errors: α = 0.69).
The Attitudes Toward Traffic Safety Scale (ATTSS), consisting of 16 items, was developed by Iversen and Rundmo (2004) and translated into Italian by Lucidi et al. (2010). Participants rated their level of agreement on a 5-point scale ranging from “strongly disagree” (1) to “strongly agree” (5). A high score indicated a positive attitude towards traffic safety regulations. The reliability of the instrument was strong, as demonstrated by the high internal consistency of its five subscales: Drink (α = 0.86), Speed (α = 0.75), Rule (α = 0.80), Care of others (α = 0.73), and Risk (α = 0.89).
Fitness-to-drive screening
The cognitive prerequisites for fitness-to-drive were assessed using the Drivesc package of the Vienna Test System (Schuhfried GmbH, 2016). The test is computerized and consists of three subtasks that evaluate the resilience of attention (Determination Test; DT), reaction times (Reaction Speed: RS and Motor Speed: MS), and perceptual speed (Adaptive Tachistoscopic Traffic Perception Test (ATAVT). The apparatus includes an ergonomic response panel, foot pedals, a standard audio output device (headset), and a video screen. The experimental screening took approximately 25 min. The DT is a measure of the resilience of attention. Participants must react as quickly and accurately as possible to changing acoustic and visual stimuli that differ in frequency and color, respectively. The software varies the speed of stimulus presentation through a computer adaptive system based on the respondent’s ongoing performance in terms of accuracy (i.e., hits, omissions, and false alarms) and response delay (i.e., milliseconds), providing a unique score. The RT measures the ability to respond as quickly and accurately as possible to specific auditory and visual stimuli. It provides two distinct measures: Reaction speed (i.e., the time taken to initiate the physical movement) and Motor speed (i.e., the time between the moment in which the participant’s finger leaves the rest button and the moment in which the reaction button is pressed). Times are recorded in milliseconds. A short reaction time (i.e., high visual and motor reaction speed) corresponds to a higher ability to quickly respond. The ATAVT measures the ability to quickly gain an overview of the traffic scenario. This subtask was administered in the right-hand traffic form according to Italian Traffic Laws. Pictures of traffic scenarios were presented briefly after an acoustic cue. After each picture, participants must select which one or more objects out of a provided list of five (i.e., motorcycles/bicycles, automobiles, traffic signs, traffic lights, and pedestrians) they have perceived. The total score is the number of correct responses (omissions and false alarms are also recorded). The total scores of the three subtasks were reported as percentile ranks, with higher scores indicating higher / better performance. The test showed moderate to good reliability in its domains (DT: α = 0.89; RS: α = 0.91; MS: α = 0.93; ATAVT = 0.70).
Study design
This is a descriptive study using cross-sectional assessment, in which the independent variables included demographic characteristics (i.e., age, gender, and level of education), cognitive measures (i.e., MoCA, MRT, and OPT), personality traits (i.e., AGGR, PSYC, DISC, NEGE, INTR, and the dissimulation index), driving behaviors (i.e., violations, errors, lapses) and attitudes (i.e., towards: rules, risk, speed, drunken driving, and care of other), and prerequisites of fitness-to-drive (i.e., DT, RS, MS, ATAVT). On the other hand, the presence/absence of an MVC(s) was the dependent variable.
Statistical analyses
The data were analyzed using SPSS 21.0 (IBM Corp., 2012) and Jamovi 1.0.7 (The Jamovi Project, 2022) statistical software. After data cleaning and codification, two steps of analysis were performed: (a) preliminary descriptive and bivariate comparisons, and (b) CART.
Descriptive statistics were performed to analyse the characteristics of the sample. Normality and homoscedasticity were also assessed. Normality of the sample distribution was assessed using Shapiro-Wilk’s test, while the homoscedasticity/heteroscedasticity was examined using Levene’s test for equality of variances, as well as using bivariate scatter plots. A one-way ANOVA was conducted to test for differences in study measures across the driver groups, with the Welch’s/Games-Howell’s statistical indices considered. Chi-Square Tests were performed to investigate the independence of nominal predictors (i.e., gender and fault) across driver groups. Correlation analysess were performed using Pearson’s coefficients.
The final stage of the analysis employed the CART models to achieve the study’s objectives. The calculations considered to draw conclusions include: (i) classification rules for observations, (ii) importance of the predictor in discriminating categories of the dependent variable, and (iii) the proportion of categorizing under one of such categories of the dependent variable. CART models were performed in an iterative manner, considering the groups of variables as described in the contextual-mediated model (i.e., distal and proximal contexts). The trees were built in steps, considering early distal predictors (step 1), and then incorporating proximal ones (step 2). To assess the stability of the model across the driver groups, this stage of the analysis was conducted for each subgroup of drivers as well as for the overall sample, resulting in a total of four classification models (i.e., drunken driver group – Model “a”, systemic group - Model “s”, and community-dwelling group – Model “c”, and total sample - Model “t”). Specifically, the driver groups were also analysed separately to assess whether the model provided informative results even when small, homogeneous samples are considered. To balance the depth of the trees across the driver groups (i.e., the number of levels or steps required to reach the terminal node starting from the root of the tree), different growth limits (i.e., minimum number of cases included in both the parent and the child nodes) were imposed to models depending by the subsamples size and producing the same ratio (2).
Moreover, since the CART model returns crosstabulations related to the association between each discriminant independent variable and the dependent variable, the data was further analysed by calculating the operational characteristics (i.e., sensitivity: proportion of participants who scored higher than the cut-off and belonging to the driver group with MVCs; specificity: proportion of participants who scored under or equal the cut-off and belonging to the driver group without MVCs; Fawcett, 2006) for each model step, following a sequential approach that considers distal and proximal variables, respectively. The associated likelihood ratios were also calculated for each step of the tree. This approach was adopted trying to limit the strongly data-driven nature of the CART technique in which decision trees are built based on the provided data (e.g., without considering theoretical assumptions), sometimes producing counterintuitive results compared to the theoretical model (Breiman et al., 1984; Hastie et al., 2009). For this reason, the models’ error rates have been discussed based on a diagnostical approach, for clinical purposes (i.e., false/true positives/negatives) instead of considering the global models’ error rates. Based on the model results, likelihood ratios have been identified as risk factors (i.e., positive likelihood ratio: calculated as sensitivity divided by one minus specificity) or protective factors (i.e., negative likelihood ratio: calculated as one minus sensitivity divided by specificity). At the end of the process, we gathered an a posteriori probability quantifying the increased of likelihood of belonging to one of the categories of the dependent variable starting from a priori probability, that is, an estimated probability of MVC involvement within the established interval of the previous five years (i.e., the ratio between the total number of police recorded MVCs and the number of active licensed drivers during the five years preceding data collection). As results, an approximate prevalence of 5‰ was estimated for MVC involvement within the referred population. Diagnostic characteristics (i.e., sensitivity, specificity, and positive/negative likelihood ratio) were calculated for each discriminating variable in each tree.
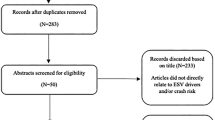
Finally, a Chi-square Test was performed to test the association between the obtained classification model and the belonging to different groups of drivers (i.e., drunk, systemic, community dwelling). Figure 1 shows a diagram of the performed analyses.

Diagram of the performed analyses
Results
Descriptive and influence statistics
Most variables were not normally distributed in the sample. However, none of the skewness and kurtosis values exceeded the critical thresholds (West et al., 1995). Consequently, all variables were included in the analysis. Additionally, some variables showed different variances across the driver groups. Therefore, various indices were considered in the preliminary statistics. Significant intergroup differences were found in all considered variables except for driving frequency and psychoticism.
Considering sociodemographic variables, significant differences were found in age and education [Age: F(2, 342) = 83.42, p < .001; Years of education: F(2, 342) = 3.25, p < .05]; post-hoc analyses revealed that drivers with systemic illness are significantly older than the drivers in other groups (Drunk: MD = -28.8; p < .001; Community-dwelling: MD = -28.7; p < .001). Significant differences were found on self-reported aberrant driving behaviors [Violations: F(2, 342) = 52.16, p < .001; Lapses: F(2, 342) = 37.10, p < .001; Errors: F(2, 342) = 11.54, p < .001], with the drunk drivers and the community-dwelling groups showing higher violations than the systemic group (Community-dwelling: MD = 10.36; p < .001; Drunk drivers: MD = 3.86; p < .001) and the drunk driver group showing lower violations than community-dwelling (MD = -6.50; p < .001). Regarding lapses, drivers in the community-dwelling group reported higher scores than drunk drivers (MD = 3.62; p < .001) and systemic drivers (MD = 3.64; p < .001). Similarly, Community-dwelling reported higher driving errors than other two groups of drivers (drunk drivers: MD = 1.49; p = .002; systemic drivers: MD = 2.00; p < .001)]. Significant results emerged for intergroup differences in driving attitudes [Rule: F(2, 342) = 12.43, p < .001; Risk: F(2, 342) = 21.24, p < .001; Speed: F(2, 342) = 21.47, p < .001; Care of others: F(2, 342) = 5.18, p = .006; Drunk: F(2, 342) = 6.38, p = .002]; drivers in the community-dwelling group showed lower attitudes towards rules (Drunken: MD = -1.79; p < .001; Systemic: MD = -1.68; p = .001), risk (Drunk: MD = -2.48; p < .001; Systemic: MD = -1.91; p < .001), speed (Drunk: MD = -1.65; p < .001; Systemic: MD = -2.09; p < .001), care of others (Drunk: MD = − 0.919; p < .001), and drunk (Systemic: MD = -1.04; p < .001).
Significant intergroup differences were also found for cognitive variables [MoCA: F(2, 342) = 14.62, p < .001; MRT: F(2, 342) = 13.05, p < .001; OPT: F(2, 342) = 7.30, p < .001], with drivers in the systemic illness group showing lower cognitive functioning scores (Drunk: MD = -2.25; p < .001; Controls: MD = -2.19; p < .001), mental rotation abilities (Drunk: MD = -4.09; p = .003; Controls: MD = -6.31; p < .001), and perspective taking performance (Drunk: MD = -22.8; p = .01; Controls: MD = -28.1; p = .001). Considering measures of fitness-to-drive, significant intergroup differences emerged in all considered variables [DT: F(2, 342) = 39.34, p < .001; RS: F(2, 342) = 17.57, p < .001; MS: F(2, 342) = 8.49, p < .001; ATAVT: F(2, 342) = 21.84, p < .001]; drivers with a systemic illness showed lower performances in DT (Drunk: MD = -26.6; p < .001; Controls: MD = -30; p < .001), RS (Drunk: MD = -14.9; p < .001; Controls: MD = -21.9; p < .001), MS (Drunk: MD = -16.7; p < .001; Controls: MD = -10.8; p = .001), and ATAVT (Drunk: MD = -24.8; p < .001; Controls: MD = -24.2; p < .001).
Considering personality traits, significant differences emerged among groups [F-K: F(2, 150) = 10.20, p < .001, AGGR: F(2, 342) = 3.39, p = .035; DISC: F(2, 342) = 16.28, p < .001; NEGE: F(2, 342) = 19.44, p < .001; INTR: F(2, 342) = 20.31, p < .001]. Drivers with a systemic illness reported lower aggression (Alcohol: MD = -4.22; p = .025; Controls: MD = -3.07; p = .043), drivers in the community-dwelling group scored a higher F-K index (Drunk: MD = 8.3; p < .001; Systemic: MD = 7.06; p = .028), while drivers in the community-dwelling group reported higher negative-emotionality (Drunk: MD = 7.6; p < .001; Systemic: MD = 5.10; p < .001), and introversion (Drunk: MD = 6.68; p < .001; Systemic: MD = 5.10; p < .001). Regarding disconstraint, drunk drivers showed higher scores than those included in the systemic group (MD = 9.96; p < .001) and in the community-dwelling group (MD = 4.96; p = .003), which in turn showed higher disconstraint than systemic drivers (MD = 5; p < .001). Finally, drivers in the community-dwelling group showed higher disconstraint than those with a systemic illness (MD = 4.96; p < .001). Table 1 shows means, standard deviations as well as significant and non-significant intergroup differences.
The proportion of culpability for individuals reporting MVCs was 45.2% in the group of drunk drivers, 37.8% in the community-dwelling group, and 0.0% in the group of systemic drivers. The results of the Chi-squared test indicated that the group variable was significantly associated with gender (χ2 = 35.9; p < .001) and the at-fault status for the MVC (χ2 = 22; p < .001). Age showed significant and negative associations with aberrant driving behaviors [Violations: r = − .365; p < .001; Lapses: r = − .170; p = 002], the performance in cognitive tests [MoCA: r = .395; p < .001; MRT: r = .429; p < .001; OPT: r = .398; p < .001], measures of fitness-to-drive [DT: r = − .697; p < .001; RS: r = − .437; p < .001; MS = r = − .392; p < .001; ATAVT: r = − .541; p < .001], and certain personality traits [AGGR: r = − .112; p < .037; DISC: r = − .307; p < .001], while positive associations with driving attitudes. Bivariate correlations for all variables are reported in Supplementary Table S1.
Classification and regression tree (CART)
After processing the data and performing influence analysis, classification trees were conducted. In all the considered models, we first included variables in the distal context and then incorporated proximal variables in a second step to observe their differential influence. For the sake of clarity, figures and tables have been reported only for those models that successfully extracted the probability to belong to the group of participants with MVCs. For the same reason, only configurations corresponding to the final step of the trees have been reported (trees corresponding to step 1 are available among Supplementary Figures). However, all the performed models are discussed in detail within the following sections.
Model “a”
The first model (Model “a”) was performed considering only the group of drunk drivers (i.e., caught for drunk driving). Results showed that variables related to the distal context (specifically sociodemographic variables; Supplementary Fig. 1) provided a unique contribution to the classification model. Once all the variables were entered in the analysis (step 2), the most relevant variable for classification was age (cut-off: 28 years; χ2 = 10.2; p < .05), representing the only level of the tree (Fig. 2). Following previous studies on drunk drivers (McKnight et al., 1995), younger age is a risk factor for negative driving outcomes. Thus, belonging to the younger age group was considered as the positive test in subsequent analysis.

Model “a”. Classification model for the group of drinker drivers (Step 2)
Age significantly discriminated participants in the sample identifying 19 true positives (i.e., number of drivers aged 28 years or younger) on the total of drivers with an MVC (42) as well as 41 true negatives (i.e., number of drivers older than 28 years) on the total of drivers without an MVC (48). Thus, sensitivity was equal to 0.45, while specificity was 0.85. The positive likelihood ratio was equal to 3.0; Drivers aged 28 years or younger have three times higher the probability of belonging to the group of participants with an MVC than the non-MVC group.
Model “c”
The second model (Model “c”) was performed considering only the community-dwelling group of drivers. Results showed that variables related to the distal context (specifically personality traits; Supplementary Fig. 2) provided a unique contribution to the classification model. Even in this case, the inclusion of proximal predictors did not change the model configuration. Once all the variables were entered in the analysis (step 2), the most relevant one for classification was disconstraint (cut-off: 50, T-points; χ2 = 10.9; p < .01) representing the only level of the tree (Fig. 3). Having obtained a score above the cut-off was considered as positive test in subsequent analysis.

Model “c”. Classification model for the community-dwelling group of drivers (Step 2)
Disconstraint significantly discriminated participants in the sample showing 27 true positives (scores above the cut-off) on 37 drivers with an MVC and 86 true negatives (scores below the cu-off) on 150 drivers without an MVC. Thus, sensitivity was equal to 0.73, while specificity was 0.57. The positive likelihood ratio was equal to 1.70; Drivers with a disconstraint score higher than the cut-off have approximately 1.7 times higher the probability of belonging to the group of drivers with an MVC then to the non-MVC group.
Model “s”
The third model (Model “s”) was performed considering only the group of drivers with a systemic illness. Results showed that variables related to the distal context (specifically personality traits and sociodemographic factors; Supplementary Fig. 3) provided a unique contribution to the classification model. Consistent with the previous models, the inclusion of proximal predictors did not significantly change the model configuration. Once all the variables were entered in the analysis (step 2), the most relevant ones were negative emotionality (cut-off: 66, T-score; χ2 = 11.2; p < .01) and age (cut-off-1: 67 years of age; cut-off-2: 72 years of age; χ2 = 17.6; p < .01) respectively representing the first and second level of classification (Fig. 4). Having obtained a score under or equal to the cut-off and being aged 67 years or younger were considered as negative tests in subsequent analysis.

Model “s”. Classification model for the group of drivers with a diagnosed systemic disease (Step 2)
Considering the first level of the tree, negative emotionality significantly discriminated participants in the sample showing 3 true positives (scores above the cut-off in negative-emotionality) on a total of 7 participants with an MVC and 58 true negatives (participants who scored equal or under the cut-off score) on a total of 61 participants without an MVC. Thus, sensitivity was equal to 0.42, while specificity was 0.95. The negative likelihood ratio was equal to 0.61.
Considering the second level of the tree, age significantly discriminated three subgroups of drivers who scored above the cut-off in negative emotionality (i.e., younger than/or aged 67 years; aged from 68 to 72 years; older than 72 years). Since no drivers with an MVC were included in the oldest group, the remaining participants (without an MVC) were included in the nearest age group defining a unique cut-off: ≤ 67 years. Considering the remaining groups, results showed 3 true positives on a total of 4 participants with an MVC and 29 true negatives on a total of 58 participants without an MVC. Thus, sensitivity was equal to 0.75, while specificity was 0.50. The negative likelihood ratio was 0.50; The probability of being involved in an MVC for drivers who scored below or equal to the cutoff in negative emotionality and who were also 68 years of age or older is reduced by approximately threefold.
Model “t”
Finally, the model “t” was performed considering the total sample of participants. The model showed that variables related to both the distal and proximal context (specifically personality traits and performance-based variables) provided contributions to the classification model. Once all variables were entered in the analysis (step 2), the most relevant ones for classification were disconstraint (cut-off: 50 T-points; χ2 = 25.8; p < .001) and motor speed (cut-off: 64 percentile ranks; χ2 = 7.9; p < .05) showing to be the first and second levels of the model (Fig. 5).

Model “t”. Classification model for the whole sample (Step 2)
Considering the inclusion of distal variables (step 1; Supplementary Fig. 4), disconstraint significantly discriminated drivers in the sample showing 81 true positives (scores above the cut-off) on a total of 86 drivers with an MVC and 157 (scores below the cut-off) true negatives on 259 drivers without an MVC. Therefore, the sensitivity is equal to 0.7. The specificity is equal to 0.6. In turn, the positive likelihood ratio is equal to 1.75; Drivers with a disconstraint score higher than the cut-off have the 1.75 times a higher probability of belonging to the group of drivers with an MVC than to the group of drivers without an MVC.
When incorporating proximal predictors, motor speed (cut-off: 64 percentile rank) showed to further improve the classification model in those participants who scored above the cut-off in disconstraint. Results showed that an obtained score above the cut-off (64 percentile ranks) significantly discriminated drivers included in such subsample (DISC score > 50) showing 30 true positives (scores above the cut-off) on 61 drivers with an MVC and 74 true negatives (scores below the cut-off) on 102 drivers without an MVC. Therefore, sensitivity was equal to 0.49 while the specificity to 0.72. Then, the positive likelihood ratio was again equal to 1.75. Considering drivers who scored above the cut-off in disconstraint score, those also showing a score above the cut-off in motor speed have 1.75 times a higher probability of belonging to the group of drivers with an MVC than the other group. The posterior probability of belonging to the group of drivers with an MVC considering the overall model was 15‰, three times the prior probability (5‰). The model error rate was 24.3%.
Associations between the model “t” and the driver groups
After performing the final classification model on the total sample (“model t”), a Chi-squared test of association was conducted among the obtained model and the participants’ driver groups. Therefore, participants in the sample were assigned to four different subgroups based on their obtained scores at those variables defining the nodes of the tree (disconstraint and motor speed) according to cut-off scores emerged in the model (Lower/Equal or Higher).
Results showed that the obtained model of classification was significantly associated to the participant’s belonging to the driver group (χ2 = 36.1; p < .001). The analysis of standardized residuals revealed that participants belonging to the drunk driver group were mainly characterized by high disconstraint and low motor speed, while those belonging to the systemic drivers group were mainly characterized by low disconstraint and low motor speed. Drunk drivers with high disconstraint and low motor speed showed a standardized residual = 1.83; systemic drivers with low disconstraint and motor speed: standardized residual = 3.32). Table 2 shows both observed and predicted frequencies as well as standardized residuals.
Discussion
This study aimed to ascertain psychological profiles of drivers with an history of MVCs, controlling for the contribution of sociodemographic variables. The investigation was focused on different driver populations, including drunk drivers (i.e., caught for drunk-driving), systemic drivers (i.e., with a diagnosed systemic/multisystemic illness), and community-dwelling drivers (without these violations/diagnosis in their history). The current analyses were conducted both separately for these groups as well as on the total sample following the contextual-mediated model (Sümer et al., 2003) of traffic accident involvement.
Significant intergroup differences emerged in terms of measures of aberrant driving behavior and attitudes toward safety: (a) Systemic drivers exhibited the lowest mean scores for aberrant driving behaviors, while (b) drivers in the community-dwelling group showed the highest frequencies of errors and lapses and expressed the lowest attitudes toward safety compared to the other two groups. Considering the first point, it is known that driving frequency tends to decrease with age (Ang et al., 2019), and older drivers are generally less prone to engage in reckless driving behaviors (Youssef et al., 2023). They often prefer driving during daylight hours and in familiar, well-known environments, typically close to their homes (Ang et al., 2019; Tinella et al., 2023). In this study, participant belonging to the systemic group was composed mainly by mature-adult and older drivers. Consequently, the result likely emerged due to the intervening effect of age. Concerning the second point, instead, it should be noted that drivers in the community-dwelling group were recruited from the general population. Previous studies highlighted the occurrence of aberrant driving behaviors in non-clinical samples of non-professional drivers (Lucidi et al., 2014; Yang et al., 2013). Furthermore, this result potentially emerged because of the influence of impression management in these scales. It is worth noting that community-dwelling group participants were assessed at a different institution (the university department) compared to the other two groups (the mobility center of the city). This difference in assessment location may have introduced a degree of impression management in the self-reported driving measures of participants within both the drunk driver and systemic driver groups. This confirms the need for cautious consideration of these measures for relicensing and fitness-to-drive assessment purposes (Lajunen & Summala, 2003). Considering the analyses performed separately on drivers’ groups, the current results provided convergent evidence on the importance of distal predictors in discriminating participants with and without an MVC. Nonetheless, the further inclusion of proximal predictors did not significantly change the models’ structures. In line with the above-mentioned theoretical framework (Sümer, 2003), the results of the present study showed the importance of sociodemographic variables (i.e., driver’s age) as well as personality traits (i.e., disconstraint and negative emotionality) in classifying drivers who reported (or not) an MVC in the past five years. For example, to be aged 28 or younger was the most important factor for classifying drivers with an MVC in the subsample of participants caught for drunk driving. Similarly, negative emotionality, together with age, were two variables contributing to the classification model in the subsample of participants with a diagnosed systemic illness. Finally, disconstraint was the only significant factor contributing to the classification model performed on the community-dwelling group. However, significant predictors found in the last two models were not able to significantly improve the likelihood of correctly classifying drivers in the group of those reporting an MVC. This result likely emerged due to a significant imbalance between participants with and without an MVC in these two groups. Furthermore, it is possible that participants with and without an MVC in these groups exhibited high variability in the study measures. These limitations prevented the attainment of a reliable estimation model for the systemic and the community-dwelling groups of drivers.
Results presented here confirms those of previous studies suggesting that age is one of the most important human-related determinants of MVC involvement in the general driving population (Oster & Strong, 2013; Fraade-Blanar et al., 2018; Castellucci et al., 2020) and particularly for drunk drivers (McKnight et al., 1995; Jongen et al., 2016; Tinella et al., 2021b). On one hand, age was negatively correlated with aberrant driving behaviors; thus, the passing of years seemed to reduce the likelihood of the engagement in risky driving (Ledger et al., 2019a, 2019b). On the other hand, the driver’s age was highly correlated with their driving experience (Ucińska el al., 2021). Thus, it can be assumed that a greater driving experience may reduce the likelihood to engage in driving violations such as drunk driving (Liu et al., 2021) by mitigating the intention to drink and drive. In this study, the results showed that drunk drivers aged 28 years or younger have three times a higher probability of belonging to the group of participants with an MVC than the non-MVC group.
Considering the model performed on drivers with a diagnosed systemic illness, the results suggest that negative emotionality may be a contributing factor in the classification of MVC involvement. However, the whole model did not show any practical benefit in terms of clinical usefulness, as evidenced by its positive likelihood ratio lower than one for the probability of MVCs group belonging. Nevertheless, previous studies have demonstrated the effects of negative emotionality on driving measures highlighting positive associations with aberrant driving behaviors, negative driving outcomes (Hu et al., 2013), and MVCs (Taubman-Ben-Ari et al., 2004). Moreover, negative emotionality, defined as “the tendency to show various forms of negative affect” (Bhagat et al., 2016, pp.1), has been shown to have significant associations with distracted driving and, in turn, with aberrant driving behaviors (Tinella et al., 2022). Personality traits are significant factors for the prevention of MVC for vulnerable road users (Alavi et al., 2017), including those with a restricted driving licence for medical reasons (Graveling & Frier, 2015; Mikuls et al., 2023). It has been shown that negative emotionality is highly recurrent in people with diagnosed systemic diseases, including cardiovascular (Balog, 2018), neurological (Devins & Seland, 1987), rheumatic (Lu et al., 2022), and metabolic (Kalra et al., 2018). Despite this, the model provided unclear clinical indications that should be considered with caution by practitioners when treating drivers with diagnosed conditions.
Considering the model performed on the community-dwelling group, disconstraint was the only predictor contributing to the classification. Disconstraint can be defined as a lack of impulse control (Harkness et al., 2014) and higher scores in this scale have been previously found to be predictive of road violations, offending attitudes, and MVCs (Magallón-Neri et al., 2015; Veltri et al., 2014). Moreover, this personality trait has been found to be significantly and negatively associated with measures of fitness-to-drive in both clinical and non-clinical samples (Tinella et al., 2021b, 2021c). In this group, drivers showing disconstraint scores higher than the cut-off showed approximately 1.7 times more the probability of belonging to the group of drivers with an MVC than the non-MVC group.
Overall, the best and most stable results were identified in the analysis performed on the whole sample, with results showing the contribution of variables included in both the distal and the proximal context of driving, that is, disconstraint (as a personality trait, included in the distal context) and motor speed (as a driving skill, included in the proximal context) were identified to be significant predictors. Both these variables improved the classification accuracy. The most likely driver group to be involved in an MVC was represented by drivers with high disconstraint scores and high motor speed (i.e., above the corresponding cut-off scores). Similar results have been showed in previous studies highlighting both impulse control and motor reaction as crucial driver-related factors affecting behaviors and performance behind the wheel (Svetina, 2016). The result shows that, despite not attaining critical thresholds, a deficiency in impulse control can be viewed as a potential risk factor, even in subclinical cases. Therefore, the monitoring of such aspects is warranted. However, in line with the model proposed by Sümer (2003), the current results suggest an influence of variables of distal and, in turns, of the proximal context on the involvement in MVCs. Following this theoretical framework and considering results presented here, these findings are compatible with Sumer regarding the indirect influence of distal factor (i.e., psychological disconstraint) and, in turns, of the proximal ones (i.e., motor speed) on the likelihood of being involved in an MVC. It is likely that motor speed mediates the distal effects of disconstraint on MVC involvement. Consequently, results of the present study suggest that drivers with a high level of disconstraint and a quicker motor reaction may be most likely included in the driver group with MVC involvement. This assumption needs further investigation since the evidence that a quicker motor reaction may be a risk-factor for an MVC in those drivers with higher disconstraint may find important implications, especially in a preventative perspective. One might expect that quicker reaction times would be advantageous for drivers, helping them respond rapidly to potential hazards. However, this result takes on a different perspective by considering the role of self-control. In this context, impulsivity refers to a trait characterized by a lack of self-control and a tendency to act on immediate impulses without considering the consequences. A driver with a specific difficulty in impulse control, if also possessing high motor speed, may potentially be more prone to risky driving behaviors. In fact, an impulsive driver could trigger non-adaptive/aberrant and dangerous behaviors (i.e., abrupt lane changes, tailgating, or aggressive driving) more quickly than a person with the same impulsivity level but with slower reaction times. Moreover, while fast reaction times can be beneficial in some situations, they must be coupled with good judgment and the ability to consider the context. Impulsive individuals may react quickly but without considering the overall traffic situation, road conditions, or the potential risks associated with their actions. Impulsive individuals often have difficulty inhibiting their automatic responses, including their motor reactions. This lack of inhibitory control can lead to overly hasty decisions and actions on the road. Previous studies have shown the links between impulsivity, psychomotor speed, and injuries in clinical and non-clinical populations (i.e., ADHD; Chamberlain et al., 2017; Rommelse et al., 2007; Dinçer et al., 2022). Results of the present study seemed to suggest that a fast motor response in the absence of self-control can be dangerous for drivers and, more in general, for those using potentially hazardous tools requiring attention and control. This result aligns with dual-process theories of decision-making, which suggest that decisions often involve a balance between automatic, impulsive responses and more reflective, controlled processes (Kvaran et al., 2013). Understanding how these processes interact can provide valuable insights into various domains, including road safety.
Furthermore, a test of association between the grouping variable and the obtained classification model “t” was performed. Results showed that the model of classification was associated with driver group. While drivers caught for drunk driving showed mainly high disconstraint and low motor speed (below or above the cut-off score) those with a diagnosed systemic/multisystemic illness showed mostly low scores in both measures. As expected, participants belonging to both the systemic and the drunk driver groups showed motor speed under the 64th percentile. The results are in line with a high number of studies indicating changes in reaction speed in drunk drivers (i.e., effect of the long-term alcohol assumption) as well as in drivers with systemic illness (i.e., effect of the medications or the older age). We are aware that this result should be considered with caution. Further studies should replicate this model by testing for their efficiency in discriminating participants with an MVC on larger samples and with objective measures of crash involvement. Finally, results presented here suggest that a driver with a score higher than the cut-off on the disconstraint scale and the motor speed test is three times more likely to be part of the population of drivers involved in an MVC (Supplementary File 1). Considering the above, this evidence confirms those of previous studies suggesting a link between impulsivity (defined on a behavioral and dispositional level) and risky driving.
Overall, in line with theoretical frameworks proposed in early studies on human-related predictors of MVC involvement, the results presented here suggest that MVCs are associated with driver-related factors considered both extrinsic and intrinsic to the driving task (Evans, 1991; Elander et al., 1993; Sümer, 2003). In particular, the results suggest that variables related to the distal context (i.e., age and personality traits) play a crucial role for MVC involvement in drivers with clinical/forensic issues (i.e., medical condition and drunk driving). The results can have practical implications in both contexts, proving valuable for assessment and intervention practices. In terms of preventive measures, these findings can be useful to policymakers in planning the shift towards safer and more sustainable mobility, especially for elderly and vulnerable users (Lin & Cui, 2021). Similarly, disconstrant, as a variable related to the distal context, was found to be associated with MVCs in the community-dwelling group of drivers and, together with motor speed (proximal context), was found associated with MVCs in the global sample. These results suggest that the contextual-mediated model still represent a valid conceptual perspective for the classification of correlates of MVCs providing evidence on the efficiency of its applicability in samples of drivers with very different characteristics. It is likely that by integrating self-reported and objective variables included in both the proximal and distal context the fitness-to-drive assessment accuracy could be further strengthened.
Conclusion
Globally, this study provides evidence on the applicability of the contextual-mediated model in the analysis of determinants of MVCs in different populations of drivers. The results showed here present some limitations, including the unbalanced gender groups sizes, the comparisons among groups of drivers who were unmatched for demographic characteristics and, more importantly, the self-reported nature of the MVCs measure. Further research is needed to overcome these limitations and to test the validity of the model in different geographical areas. Moreover, results presented here refer to observational data; more sophisticated methodology is needed to test their replicability in a causal model. The assessment of groups of drivers took place in different locations, potentially leading to a higher likelihood of response bias among drivers in the experimental groups compared to the community-dwelling group. This limitation characterizes self-reported measures of driving as suggested in previous study (Lajunen & Summala, 2003). Finally, the study does not overcome some of the methodological weaknesses highlighted by Af Wåhlberg (2003) concerning studies on MVCs and particularly that regarding the time period of the crash to be controlled in the analysis. However, the novelty of the present work consisted in implementing a rigorous and innovative techniques as the CART following a precise theoretical model of MVCs involvement. Moreover, another novelty was the interpretation through a Bayesian factor and the calculation of conditional probabilities of the frequencies emerged from the CART results. These results may represent a valuable source of knowledge for those researchers dealing with road safety promotion. Professionals of mobility centres and occupational therapists may find these results useful in order to develop and promote tailored road safety interventions as well as for licensing and fitness-to-drive assessment purposes. Considering these results, future studies may try to define driver-related risk of MVC involvement. Finally, these findings can be used by insurance companies to target resources and interventions towards those at high-risk drivers.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request. Data are located in controlled access data storage at University of Bari, Italy.
References
Abbasi, E., Li, Y., Wu, X., & Craig, B. (2021). Using classification and regression trees (CART) to identify factors contributing to vehicle crash severity in a Port City. International Journal of Transportation System, 29, 29–38.
Adrian, J., Postal, V., Moessinger, M., Rascle, N., & Charles, A. (2011). Personality traits and executive functions related to on-road driving performance among older drivers. Accident; Analysis and Prevention, 43(5), 1652–1659. https://doi.org/10.1016/j.aap.2011.03.023
af Wåhlberg, A. E. (2003). Some methodological deficiencies in studies on traffic accident predictors. Accident; Analysis and Prevention, 35(4), 473–486. https://doi.org/10.1016/s0001-4575(02)00025-8
Alavi, S. S., Mohammadi, M. R., Souri, H., Kalhori, M., Jannatifard, S., F., & Sepahbodi, G. (2017). Personality, driving behavior and mental disorders factors as predictors of road traffic accidents based on logistic regression. Iranian Journal of Medical Sciences, 42(1), 24–31.
Ang, B. H., Oxley, J. A., Chen, W. S., Yap, K. K., Song, K. P., & Lee, S. W. H. (2019). To reduce or to cease: A systematic review and meta-analysis of quantitative studies on self-regulation of driving. Journal of Safety Research, 70, 243–251. https://doi.org/10.1016/j.jsr.2019.07.004
Anstey, K. J., Wood, J., Lord, S., & Walker, J. G. (2005). Cognitive, sensory and physical factors enabling driving safety in older adults. Clinical Psychology Review, 25, 45–65. https://doi.org/10.1016/j.cpr.2004.07.008
Ball, K. K., Roenker, D. L., Wadley, V. G., Edwards, J. D., Roth, D. L., McGwin, G. Jr, Raleigh, R., Joyce, J. J., Cissell, G. M., & Dube, T. (2006). Can high-risk older drivers be identified through performance-based measures in a department of motor vehicles setting? Journal of the American Geriatrics Society, 54(1), 77–84. https://doi.org/10.1111/j.1532-5415.2005.00568.x
Ball, K., Edwards, J. D., Ross, L. A., & McGwin, G. Jr (2010). Cognitive training decreases motor vehicle collision involvement of older drivers. Journal of the American Geriatrics Society, 58(11), 2107–2113. https://doi.org/10.1111/j.1532-5415.2010.03138.x
Balog, P. (2018). A negatív érzelmek és a szív-és érrendszeri betegségek összefüggései = negative emotions associated with cardiovascular diseases. Orvosi Hetilap, 159(48), 2005–2010. https://doi.org/10.1556/650.2018.31221
Begg, D. J., & Langley, J. D. (2001). Changes in risky driving behavior from age 21 to 26 years. Journal of Safety Research, 32, 491–499. https://doi.org/10.1016/S0022-4375(01)00059-7
Bhagat, V., Haque, M., Simbak, N. B., & Jaalam, K. (2016). Study on personality dimension negative emotionality affecting academic achievement among Malaysian medical students studying in Malaysia and overseas. Advances in Medical Education and Practice, 7, 341–346. https://doi.org/10.2147/AMEP.S108477
Bosco, A., Spano, G., Caffò, A. O., Lopez, A., Grattagliano, I., Saracino, G., Pinto, K., Hoogeveen, F., & Lancioni, G. E. (2017). Italians do it worse. Montreal Cognitive Assessment (MoCA) optimal cut-off scores for people with probable Alzheimer’s disease and with probable cognitive impairment. Aging Clinical and Experimental Research, 29(6), 1113–1120. https://doi.org/10.1007/s40520-017-0727-6
Bosco, A., Ylenia, M., Lisi, A., Di Conza, A., Filippo, C., Caffò, A. O., & Grattagliano, I. (2020). Detecting faking good in military enlistment procedure according to a new index for the MMPI-2. Rassegna Italiana Di Criminologia, 14(2), 99–109.
Braitman, K. A., Kirley, B. B., McCartt, A. T., & Chaudhary, N. K. (2008). Crashes of novice teenage drivers: characteristics and contributing factors. Journal of Safety Research, 39(1), 47–54. https://doi.org/10.1016/j.jsr.2007.12.002
Breiman, L. (1984). Classification and Regression Trees (1st ed.). Routledge. https://doi.org/10.1201/9781315139470
Butcher, J. N., Dahlstrom, W. G., Graham, J. R., Tellegen, A., & Kaemmer, B. (1989). Minnesota Multiphasic personality inventory (MMPI-2). Manual for administration and scoring. University of Minnesota Press.
Castellucci, H. I., Bravo, G., Arezes, P. M., & Lavallière, M. (2020). Are interventions effective at improving driving in older drivers? A systematic review. BMC Geriatrics, 20(1), 125. https://doi.org/10.1186/s12877-020-01512-z
Chamberlain, S. R., Ioannidis, K., Leppink, E. W., Niaz, F., Redden, S. A., & Grant, J. E. (2017). ADHD symptoms in non-treatment seeking young adults: Relationship with other forms of impulsivity. CNS Spectrums, 22(1), 22–30. https://doi.org/10.1017/S1092852915000875
Chapman, W. W., & Haug, P. J. (1999). Comparing expert systems for identifying chest x-ray reports that support pneumonia. Proceedings. AMIA Symposium, 216–220.
Clarke, D. D., Ward, P., Bartle, C., & Truman, W. (2006). Young driver accidents in the UK: The influence of age, experience, and time of day. Accident Analysis and Prevention, 38(5), 871–878. https://doi.org/10.1016/j.aap.2006.02.013
Constantinou, E., Panayiotou, G., Konstantinou, N., Loutsiou-Ladd, A., & Kapardis, A. (2011). Risky and aggressive driving in young adults: Personality matters. Accident Analysis and Prevention, 43(4), 1323–1331. https://doi.org/10.1016/j.aap.2011.02.002
Curry, A. E., Mirman, J. H., Kallan, M. J., Winston, F. K., & Durbin, D. R. (2012). Peer passengers: How do they affect teen crashes? The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 50(6), 588–594. https://doi.org/10.1016/j.jadohealth.2011.10.016
Devins, G. M., & Seland, T. P. (1987). Emotional impact of multiple sclerosis: Recent findings and suggestions for future research. Psychological Bulletin, 101(3), 363–375.
Dinçer, M., Uğurtaş Gökçe, F. S., Gül, H., Taş Torun, Y., Bodur, Ş., & Cöngöloğlu, M. A. (2022). Is Processing Speed (Gs) related to hyperactivity (as a narrow cognitive area of gps): A Dimensional approach to heterogeneity of clinical and WISC-IV cognitive profiles in ADHD from RDoC/HiTOP perspective. Journal of Attention Disorders, 26(13), 1747–1761. https://doi.org/10.1177/10870547221099963
Doroudgar, S., Chuang, H. M., Perry, P. J., Thomas, K., Bohnert, K., & Canedo, J. (2017). Driving performance comparing older versus younger drivers. Traffic Injury Prevention, 18(1), 41–46. https://doi.org/10.1080/15389588.2016.1194980
Eboli, L., & Forciniti, C. (2020). The severity of traffic crashes in Italy: An explorative analysis among different driving circumstances. Sustainability, 12(3), 856. https://doi.org/10.3390/su12030856
Eduardo, M., & Ildefonso, M. M. (2020). On the long-run association between personality traits and road crashes: Findings from the British cohort study. Personality and Individual Differences, 155, 109677. https://doi.org/10.1016/j.paid.2019.109677
Elander, J., West, R., & French, D. (1993). Behavioral correlates of individual differences in road-traffic crash risk: An examination of methods and findings. Psychological Bulletin, 113(2), 279–294. https://doi.org/10.1037/0033-2909.113.2.279
Evans, L. (1991). Traffic safety and the driver. Van Nostrand Reinhold.
Faílde-Garrido, J. M., Martínez Torres, J., Rodríguez-Castro, Y., & García-Rodríguez, M. A. (2022). Do road offenders constitute a unique clinical and sociodemographic profile? The relationship between crime and road safety. Psychology Crime & Law, 1–21. https://doi.org/10.1080/1068316X.2022.2126841
Fawcett, T. (2006). An introduction to ROC analysis. Pattern Recognition Letters, 27(8), 861–874. https://doi.org/10.1016/j.patrec.2005.10.010
Fraade-Blanar, L. A., Ebel, B. E., Larson, E. B., Sears, J. M., Thompson, H. J., Chan, K. C. G., & Crane, P. K. (2018). Cognitive decline and older driver crash risk. Journal of the American Geriatrics Society, 66(6), 1075–1081. https://doi.org/10.1111/jgs.15378
Gicquel, L., Ordonneau, P., Blot, E., Toillon, C., Ingrand, P., & Romo, L. (2017). Description of various factors contributing to traffic accidents in youth and measures proposed to alleviate recurrence. Frontiers in Psychiatry, 8, 94. https://doi.org/10.3389/fpsyt.2017.00094
Graveling, A. J., & Frier, B. M. (2015). Driving and diabetes: Problems, licensing restrictions and recommendations for safe driving. Clinical Diabetes and Endocrinology, 1, 8. https://doi.org/10.1186/s40842-015-0007-3
Hakamies-Blomqvist, L. E. (1993). Fatal accidents of older drivers. Accident; Analysis and Prevention, 25(1), 19–27. https://doi.org/10.1016/0001-4575(93)90093-c
Harkness, A. R., McNulty, J. L., Finn, J. A., Reynolds, S. M., Shields, S. M., & Arbisi, P. (2014). The MMPI–2–RF personality psychopathology five (PSY–5–RF) scales: Development and validity research. Journal of Personality Assessment, 96(2), 140–150.
Hassan, H. M., & Abdel-Aty, M. A. (2013). Exploring the safety implications of young drivers’ behavior, attitudes and perceptions. Accident; Analysis and Prevention, 50, 361–370. https://doi.org/10.1016/j.aap.2012.05.003
Hastie, T., Tibshirani, R., Friedman, J. H., & Friedman, J. H. (2009). The elements of statistical learning: Data mining, inference, and prediction (Vol. 2, pp. 1–758). springer.
Hegarty, M., & Waller, D. (2004). A dissociation between mental rotation and perspective-taking spatial abilities. Intelligence, 32(2), 175–191. https://doi.org/10.1016/j.intell.2003.12.001
Hu, T. Y., Xie, X., & Li, J. (2013). Negative or positive? The effect of emotion and mood on risky driving. Transportation Research part F: Traffic Psychology and Behaviour, 16, 29–40. https://doi.org/10.1016/j.trf.2012.08.009
IBM Corp Released 2012. IBM SPSS statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.
Iversen, H., & Rundmo, T. (2004). Attitudes towards traffic safety, driving behaviour and accident involvement among the Norwegian public. Ergonomics, 47(5), 555–572. https://doi.org/10.1080/00140130410001658709
Janke, M. K. (1991). Accidents, mileage, and the exaggeration of risk. Accident; Analysis and Prevention, 23(2–3), 183–188. https://doi.org/10.1016/0001-4575(91)90048-a
Javadi, S. M., Azad, F., Tahmasebi, H., Rafiei, S., Rahgozar, H., M., & Tajlili, A. (2015). Study of psycho-social factors affecting traffic accidents among young boys in Tehran. Iranian Red Crescent Medical Journal, 17(7), e22080. https://doi.org/10.5812/ircmj.22080v2
Jenkins, D. G., & Quintana-Ascencio, P. F. (2020). A solution to minimum sample size for regressions. PLoS ONE, 15(2), e0229345. https://doi.org/10.1371/journal.pone.0229345
Jongen, S., Vuurman, E. F., Ramaekers, J. G., & Vermeeren, A. (2016). The sensitivity of laboratory tests assessing driving related skills to dose-related impairment of alcohol: A literature review. Accident; Analysis and Prevention, 89, 31–48. https://doi.org/10.1016/j.aap.2016.01.001
Kalra, S., Jena, B. N., & Yeravdekar, R. (2018). Emotional and psychological needs of people with diabetes. Indian Journal of Endocrinology and Metabolism, 22(5), 696–704. https://doi.org/10.4103/ijem.IJEM_579_17
Kunishige, M., Fukuda, H., Iida, T., Kawabata, N., Ishizuki, C., & MIyaguchi, H. (2019). Spatial navigation ability and gaze switching in older drivers: A driving simulator study. Hong Kong Journal of Occupational Therapy: HKJOT, 32(1), 22–31. https://doi.org/10.1177/1569186118823872
Kvaran, T., Nichols, S., & Sanfey, A. (2013). The effect of analytic and experiential modes of thought on moral judgment. Progress in Brain Research, 202, 187–196. https://doi.org/10.1016/B978-0-444-62604-2.00011-3
Kweon, Y. J., & Kockelman, K. M. (2003). Overall injury risk to different drivers: Combining exposure, frequency, and severity models. Accident; Analysis and Prevention, 35(4), 441–450. https://doi.org/10.1016/s0001-4575(02)00021-0
Kwok, J. C. W., Gélinas, I., Benoit, D., & Chilingaryan, G. (2015). Predictive validity of the Montreal Cognitive Assessment (MoCA) as a screening tool for on-road driving performance. British Journal of Occupational Therapy, 78(2), 100–108.
La Torre, G., Van Beeck, E., Quaranta, G., Mannocci, A., & Ricciardi, W. (2007). Determinants of within-country variation in traffic accident mortality in Italy: a geographical analysis. International Journal of Health Geographics, 6, 49. https://doi.org/10.1186/1476-072X-6-49
Lajunen, T., & Summala, H. (2003). Can we trust self-reports of driving? Effects of impression management on driver behaviour questionnaire responses. Transportation Research Part F: Traffic Psychology and Behaviour, 6(2), 97–107. https://doi.org/10.1016/S1369-8478(03)00008-1
Langford, J., & Koppel, S. (2006). Epidemiology of older driver crashes–identifying older driver risk factors and exposure patterns. Transportation Research Part F: Traffic Psychology and Behaviour, 9(5), 309–321. https://doi.org/10.1016/j.trf.2006.03.005
Ledger, S., Bennett, J. M., Chekaluk, E., & Batchelor, J. (2019a). Cognitive function and driving: Important for young and old alike. Transportation Research Part F: Traffic Psychology and Behaviour, 60, 262–273. https://doi.org/10.1016/j.trf.2018.10.024
Ledger, S., Bennett, J. M., Chekaluk, E., Batchelor, J., & Meco, A. D. (2019b). Cognitive function and driving in middle adulthood: Does age matter? Transportation Research Part F: Traffic Psychology and Behaviour, 66, 471–484. https://doi.org/10.1016/j.trf.2019.10.002
Lin, D., & Cui, J. (2021). Transport and mobility needs for an ageing society from a policy perspective: Review and implications. International Journal of Environmental Research and Public Health, 18(22), 11802. https://doi.org/10.3390/ijerph182211802
Liu, P., Jiang, Z., Li, T., Wang, G., Wang, R., & Xu, Z. (2021). User experience and usability when the automated driving system fails: Findings from a field experiment. Accident Analysis & Prevention, 161, 106383. https://doi.org/10.1016/j.aap.2021.106383
Lu, Y., Jin, X., Feng, L. W., Tang, C., Neo, M., & Ho, R. C. (2022). Effects of illness perception on negative emotions and fatigue in chronic rheumatic diseases: Rumination as a possible mediator. World Journal of Clinical Cases, 10(34), 12515–12531. https://doi.org/10.12998/wjcc.v10.i34.12515
Lucidi, F., Giannini, A. M., Sgalla, R., Mallia, L., Devoto, A., & Reichmann, S. (2010). Young novice driver subtypes: Relationship to driving violations, errors and lapses. Accident; Analysis and Prevention, 42(6), 1689–1696. https://doi.org/10.1016/j.aap.2010.04.008
Lucidi, F., Mallia, L., Lazuras, L., & Violani, C. (2014). Personality and attitudes as predictors of risky driving among older drivers. Accident; Analysis and Prevention, 72, 318–324. https://doi.org/10.1016/j.aap.2014.07.022
Lucidi, F., Mallia, L., Giannini, A. M., Sgalla, R., Lazuras, L., Chirico, A., Alivernini, F., Girelli, L., & Violani, C. (2019). Riding the adolescence: Personality subtypes in young moped riders and their association with risky driving attitudes and behaviors. Frontiers in Psychology, 10, 300. https://doi.org/10.3389/fpsyg.2019.00300
Ma, Z., Mei, G., & Cuomo, S. (2021). An analytic framework using deep learning for prediction of traffic accident injury severity based on contributing factors. Accident; Analysis and Prevention, 160, 106322. https://doi.org/10.1016/j.aap.2021.106322
Magallón-Neri, E., Díaz, R., Forns, M., Goti, J., & Castro-Fornieles, J. (2015). Personality psychopathology, drug use and psychological symptoms in adolescents with substance use disorders and community controls. PeerJ, 3, e992. https://doi.org/10.7717/peerj.992
Martino, V., Grattagliano, I., Bosco, A., Massaro, Y., Lisi, A., Campobasso, F., Marchitelli, M. A., & Catanesi, R. (2016). A New Index for the MMPI-2 test for detecting dissimulation in forensic evaluations: A pilot study. Journal of Forensic Sciences, 61(1), 249–253. https://doi.org/10.1111/1556-4029.12889
Mathias, J. L., & Lucas, L. K. (2009). Cognitive predictors of unsafe driving in older drivers: A meta-analysis. International Psychogeriatrics, 21(4), 637–653. https://doi.org/10.1017/S1041610209009119
McGwin, G. Jr, & Brown, D. B. (1999). Characteristics of traffic crashes among young, middle-aged, and older drivers. Accident; Analysis and Prevention, 31(3), 181–198. https://doi.org/10.1016/s0001-4575(98)00061-x
McKnight, A. J., Langston, E. A., McKnight, A. S., JA, R., & Lange, J. E. (1995). Why people drink and drive: The bases of drinking-and-driving decisions (No. DOT HS 808 251). United States. National Highway Traffic Safety Administration.
Meles, H. G., Gebrehiwot, D. B., Gebrearegay, F., Wubet, G. G., & Gebregergis, T. (2021). Identification of determinant factors for car accident levels occurred in Mekelle City, Tigray, Ethiopia: Ordered logistic regression model approach. Momona Ethiopian Journal of Science, 13(2), 225–239. https://doi.org/10.4314/mejs.v13i2.3
Mikuls, T. R., Merickel, J., Gwon, Y., Sayles, H., Petro, A., Cannella, A., Snow, M. H., Feely, M., England, B. R., Michaud, K., & Rizzo, M. (2023). Vehicle control as a measure of real-world driving performance in patients with rheumatoid arthritis. Arthritis care & Research, 75(2), 252–259. https://doi.org/10.1002/acr.24769
Mohamed, J., Mohamed, A. I., Ali, D. A., & Gebremariam, T. T. (2023). Prevalence and factors associated with ever had road traffic accidents among drivers in Hargeisa city. Somaliland 2022 Heliyon, 9(8), e18631. https://doi.org/10.1016/j.heliyon.2023.e18631
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., Cummings, J. L., & Chertkow, H. (2005). The montreal cognitive assessment, MoCA: A brief screening tool for mild cognitive impairment. Journal of the American Geriatrics Society, 53(4), 695–699. https://doi.org/10.1111/j.1532-5415.2005.53221.x
Noland, R. B., & Quddus, M. A. (2004). A spatially disaggregate analysis of road casualties in England. Accident; Analysis and Prevention, 36(6), 973–984. https://doi.org/10.1016/j.aap.2003.11.001
Nori, R., Palmiero, M., Bocchi, A., Giannini, A. M., & Piccardi, L. (2020). The specific role of spatial orientation skills in predicting driving behaviour. Transportation Research part F: Traffic Psychology and Behaviour, 71, 259–271. https://doi.org/10.1016/j.trf.2020.04.009
Oster Jr, C. V., & Strong, J. S. (2013). Analyzing road safety in the United States. Research in Transportation Economics, 43(1), 98–111. https://doi.org/10.1016/j.retrec.2012.12.005
Owsley, C., Ball, K., Sloane, M., Roenker, D., & Bruni, J. (1991). Visual perceptual/cognitive correlates of vehicle crashes in older drivers. Psychology and Aging, 6, 403415.
Owsley, C., McGwin, G. Jr, & Ball, K. (1998). Vision impairment, eye disease, and injurious motor vehicle crashes in the elderly. Ophthalmic Epidemiology, 5(2), 101–113. https://doi.org/10.1076/opep.5.2.101.1574
Portela-Pino, I., Alvariñas-Villaverde, M., Martínez-Torres, J., & Pino-Juste, M. (2021). Influence of the perception of barriers in practice of PA in adolescents: Explanatory model. Healthcare, 9(4), 380. https://doi.org/10.3390/healthcare9040380
Reason, J., Manstead, A., Stradling, S., Baxter, J., & Campbell, K. (1990). Errors and violations on the roads: A real distinction? Ergonomics, 33(10–11), 1315–1332. https://doi.org/10.1080/00140139008925335
Rolison, J. J., Regev, S., Moutari, S., & Feeney, A. (2018). What are the factors that contribute to road accidents? An assessment of law enforcement views, ordinary drivers’ opinions, and road accident records. Accident; Analysis and Prevention, 115, 11–24. https://doi.org/10.1016/j.aap.2018.02.025
Rommelse, N. N., Altink, M. E., Oosterlaan, J., Buschgens, C. J., Buitelaar, J., De Sonneville, L. M., & Sergeant, J. A. (2007). Motor control in children with ADHD and non-affected siblings: Deficits most pronounced using the left hand. Journal of Child Psychology and Psychiatry and Allied Disciplines, 48(11), 1071–1079. https://doi.org/10.1111/j.1469-7610.2007.01781.x
Saeed, S., Wahbi, A., Abdulazeez, N. M., Nada, S., & Abuzeid, D. (2023). Motor-vehicle accidents victims in Khartoum-Sudan; Identification and analysis of related risk factors, safety measures, and injury severity. Acta Scientific Orthopaedics, 6(6), 78–94. https://doi.org/10.31080/ASOR.2023.06.0760
Saeednejad, M., Sadeghian, F., Fayaz, M., Rafael, D., Atlasi, R., Kazemzadeh Houjaghan, A., Abedi Kichi, R., Asgardoon, M. H., Mahmoudabadi, Z., Salamati, H., Naji, Z., Rahimi-Movaghar, Z., V., & Salamati, P. (2020). Association of social determinants of health and road traffic deaths: A systematic review. Bulletin of Emergency and Trauma, 8(4), 211–217. https://doi.org/10.30476/beat.2020.86574
Salthouse, T. A. (2000). Aging and measures of processing speed. Biological Psychology, 54(1–3), 35–54. https://doi.org/10.1016/s0301-0511(00)00052-1
Salthouse, T. A. (2009). When does age-related cognitive decline begin? Neurobiology of Aging, 30(4), 507–514. https://doi.org/10.1016/j.neurobiolaging.2008.09.023
Schuhfried GmbH (2016). Manual: Fitness to Drive Screening. Test Label DRIVESC. Version 03-Revision 1.
Sommer, M., Heidinger, C., Arendasy, M., Schauer, S., Schmitz-Gielsdorf, J., & Häusler, J. (2010). Cognitive and personality determinants of post-injury driving fitness. Archives of Clinical Neuropsychology: The Official Journal of the National Academy of Neuropsychologists, 25(2), 99–117. https://doi.org/10.1093/arclin/acp109
Spoerri, A., Egger, M., von Elm, E., & Swiss National Cohort Study. (2011). Mortality from road traffic accidents in Switzerland: Longitudinal and spatial analyses. Accident; Analysis and Prevention, 43(1), 40–48. https://doi.org/10.1016/j.aap.2010.06.009
Sümer, N. (2003). Personality and behavioral predictors of traffic accidents: Testing a contextual mediated model. Accident; Analysis and Prevention, 35(6), 949–964. https://doi.org/10.1016/s0001-4575(02)00103-3
Svetina, M. (2016). The reaction times of drivers aged 20 to 80 during a divided attention driving. Traffic Injury Prevention, 17(8), 810–814. https://doi.org/10.1080/15389588.2016.1157590
Taubman-Ben-Ari, O., Mikulincer, M., & Gillath, O. (2004). The multidimensional driving style inventory–scale construct and validation. Accident; Analysis and Prevention, 36(3), 323–332. https://doi.org/10.1016/S0001-4575(03)00010-1
Teranishi, K., Ohtsubo, T., Nakamura, S., Matsuba, Y., & Nakanishi, M. (2019). Effects of different visual-support viewpoints upon behavior and cognition in spatial mobility. Transactions of Society of Automotive Engineers of Japan, 50, 883–890. https://doi.org/10.11351/jsaeronbun.50.883
The Jamovi Project (2022). Jamovi (Version 2.3) [Computer Software]. Retrieved from https://www.jamovi.org. Accessed 12 May 2023.
Theofilatos, A., Yannis, G., Kopelias, P., & Papadimitriou, F. (2016). Predicting road accidents: A rare-events modeling approach. Transportation Research Procedia, 14, 3399–3405. https://doi.org/10.1016/j.trpro.2016.05.293
Thomas, P., Morris, A., Talbot, R., & Fagerlind, H. (2013). Identifying the causes of road crashes in Europe. Annals of advances in automotive medicine. Association for the Advancement of Automotive Medicine. Annual Scientific Conference, 57, 13–22.
Tinella, L., Lopez, A., Caffò, A. O., Grattagliano, I., & Bosco, A. (2020). Spatial mental transformation skills discriminate fitness to drive in young and old adults. Frontiers in Psychology, 11, 604762. https://doi.org/10.3389/fpsyg.2020.604762
Tinella, L., Lopez, A., Caffò, A. O., Nardulli, F., Grattagliano, I., & Bosco, A. (2021a). Cognitive efficiency and fitness-to-drive along the lifespan: The mediation effect of visuospatial transformations. Brain Sciences, 11(8), 1028. https://doi.org/10.3390/brainsci11081028
Tinella, L., Caffò, A. O., Lopez, A., Nardulli, F., Grattagliano, I., & Bosco, A. (2021b). Reassessing fitness-to-drive in drinker drivers: The role of cognition and personality. International Journal of Environmental Research and Public Health, 18(23), 12828. https://doi.org/10.3390/ijerph182312828
Tinella, L., Caffò, A. O., Lopez, A., Grattagliano, I., & Bosco, A. (2021c). The impact of two MMPI-2-Based models of personality in predicting driving behavior. Can demographic variables be disregarded? Brain Sciences, 11(3), 313. https://doi.org/10.3390/brainsci11030313
Tinella, L., Koppel, S., Lopez, A., Caffò, A. O., & Bosco, A. (2022). Associations between personality and driving behavior are mediated by mind-wandering tendency: A cross-national comparison of Australian and Italian drivers. Transportation Research part F: Traffic Psychology and Behaviour, 89, 265–275. https://doi.org/10.1016/j.trf.2022.06.019
Tinella, L., Bosco, A., Traficante, S., Napoletano, R., Ricciardi, E., Spano, G., & Caffò, A. O. (2023). Fostering an age-friendly sustainable transport system: A psychological perspective. Sustainability, 15(18), 13972. https://doi.org/10.3390/su151813972
Ucińska, M., Odachowska, E., Gąsiorek, K., & Kruszewski, M. (2021). Age and experience in driving a vehicle and psychomotor skills in the context of automation. Open Engineering, 11(1), 453–462. https://doi.org/10.1515/eng-2021-0045
Ünal, A. B. (2006). Assessment of computer-based and self-reported hazard perception skills among drivers: The role of personality and driving skills (Master’s thesis, Middle East Technical University).
United States - National Highway Traffic Safety Administration– NHTSA (2019). Traffic Safety Facts 2017. A Compilation of Motor Vehicle Crash Data. U.S. Department of Transportation Washington, DC 20590.
Vandenberg, S. G., & Kuse, A. R. (1978). Mental rotations, a group test of three-dimensional spatial visualization. Perceptual and Motor Skills, 47(2), 599–604. https://doi.org/10.2466/pms.1978.47.2.599
Veltri, C. O., Sellbom, M., Graham, J. R., Ben-Porath, Y. S., Forbey, J. D., & White, R. S. (2014). Distinguishing personality psychopathology five (PSY-5) characteristics associated with violent and nonviolent juvenile delinquency. Journal of Personality Assessment, 96(2), 158–165. https://doi.org/10.1080/00223891.2013.843539
Venkatasubramaniam, A., Wolfson, J., Mitchell, N., Barnes, T., JaKa, M., & French, S. (2017). Decision trees in epidemiological research. Emerging Themes in Epidemiology, 14, 11. https://doi.org/10.1186/s12982-017-0064-4
Wang, C. H., Tsay, S. L., & Bond, A. E. (2005). Post-traumatic stress disorder, depression, anxiety and quality of life in patients with traffic-related injuries. Journal of Advanced Nursing, 52(1), 22–30. https://doi.org/10.1111/j.1365-2648.2005.03560.x
Wang, W., Qie, T., Yang, C., Liu, W., Xiang, C., & Huang, K. (2021). An intelligent lane-changing behavior prediction and decision-making strategy for an autonomous vehicle. IEEE Transactions on Industrial Electronics, 69(3), 2927–2937.
West, S. G., Finch, J. F., & Curran, P. J. (1995). Structural equation models with nonnormal variables: Problems and remedies. In R. H. Hoyle (Ed.), Structural equation modeling: Concepts, issues, and applications (pp. 56–75). Sage Publications, Inc.
Wilcox, A., & Hripcsak, G. (1999). Classification algorithms applied to narrative reports. Proceedings. AMIA Symposium, 455–459.
Williams, A. F., & Shabanova, V. I. (2003). Responsibility of drivers, by age and gender, for motor-vehicle crash deaths. Journal of Safety Research, 34(5), 527–531. https://doi.org/10.1016/j.jsr.2003.03.001
World Health Organization (2018). Global Status Report on Road Safety 2018; WHO: Geneva, Switzerland.
Yang, J., Du, F., Qu, W., Gong, Z., & Sun, X. (2013). Effects of personality on risky driving behavior and accident involvement for Chinese drivers. Traffic Injury Prevention, 14(6), 565–571. https://doi.org/10.1080/15389588.2012.748903
Yasmeen, S. (2019). Road Traffic crashes (RTCs) and its determinants: Public Health Issue. International Journal of Collaborative Research on Internal Medicine & Public Health, 11(3), 911–916.
Youssef, D., Salameh, P., Abou-Abbas, L., & Salmi, L. R. (2023). Driving anger dimensions and their relationship with aberrant driver behavior in Lebanon: Results from a national self-reported survey. PLoS ONE, 18(3), e0283293. https://doi.org/10.1371/journal.pone.0283293
Zamzuri, Z. H., & Qi, K. Z. (2022). Classifying the severity levels of traffic accidents using decision trees. In International Conference on Mathematical Sciences and Statistics 2022 (ICMSS 2022) (pp. 173–181). Atlantis Press.
Zhang, X., Qu, X., Tao, D., & Xue, H. (2019). The association between sensation seeking and driving outcomes: A systematic review and meta-analysis. Accident Analysis and Prevention, 123, 222–234. https://doi.org/10.1016/j.aap.2018.11.023
Zicat, E., Bennett, J. M., Chekaluk, E., & Batchelor, J. (2018). Cognitive function and young drivers: The relationship between driving, attitudes, personality and cognition. Transportation Research Part F: Traffic Psychology and Behaviour, 55, 341–352. https://doi.org/10.1016/j.trf.2018.03.013
Funding
Open access funding provided by Università degli Studi di Salerno within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tinella, L., Bosco, A., Koppel, S. et al. Sociodemographic and psychological factors affecting motor vehicle crashes (MVCs): a classification analysis based on the contextual-mediated model of traffic-accident involvement. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-06186-z
Accepted:
Published:
DOI: https://doi.org/10.1007/s12144-024-06186-z