
Abstract
Purpose
This research was conducted to determine the impact of a planned training program and music on fear, anxiety, and depression among women undergoing cesarean section.
Methods
The sample of the randomized-controlled experimental study consisted of a total of 120 pregnant women (music 40, training 40, and the control 40) scheduled for cesarean section at the Obstetrics Service. Instrumental music from the Turkish music modes (the Hejaz, Neva, and Acemaşıran modes) was played for the music group, a planned training was given for the training group (what a cesarean section is, why a cesarean section should be performed, breastfeeding, mobilization, etc.) before the cesarean section, and no additional interventions were made for the control group. The data were collected using the Personal Information Form, Surgical Fear Questionnaire, and the Hospital Anxiety and Depression Scale.
Results
After the planned training and listening to music applications, statistically significant differences were found between the music, training, and the control groups in terms of the short-term, long-term sub-scale scores and the overall score of the Surgical Fear Questionnaire and the anxiety sub-scale scores of the Hospital Anxiety and Depression Scale (p < 0.05).
Conclusions
Listening to music before the cesarean section was effective in reducing women’s short-term and general surgical fears, and the training was also effective in reducing their short-term, long-term, and general surgical fears and anxiety levels. However, the applications did not change depression levels. According to these findings, listening to music and provision of training are recommended to reduce surgical fears and anxiety levels of women before a planned cesarean section.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although childbirth is a physiological event, it is also a process in which negative emotions such as pain, fear, stress, and anxiety are experienced by women (Sun et al., 2019). As a result of these physiological and psychological changes, women’s modes of delivery may sometimes change and women may have to undergo a cesarean section. Cesarean delivery is a mode of delivery that is increasingly and often preferred by women, although it is riskier for the health of mother and baby compared to normal delivery (Sun et al., 2019). Although the cesarean section rate recommended by the World Health Organization (WHO) is 15% the cesarean section rate in Turkey is 52.1%, according to the Turkey Demographic and Health Survey (2018) (TDHS, 2018; WHO, 2015).
For women, the pregnancy period can increase anxiety and the fear levels of individuals may increase in the pre-operative period (Sun et al., 2019). In one study, it was found that the overall anxiety rate was 58.9% before cesarean section, and in another study, moderate anxiety of 60.4% was found to be experienced (Field & Haloob, 2016; Sun et al., 2019). During this period, factors such as age, gender, educational status, social support, unknown, fear of death and body image, anesthesia, pain, risk of complications, and paralysis affect the surgical fear and anxiety (Field & Haloob, 2016; Sun et al., 2019). It is normal to experience fear and anxiety during the preoperative period. However, increasing the level of fear and anxiety can lead to many problems, such as delayed wound healing, prolonged hospital stays and treatment time, increased use of analgesics after surgery, lack of self-care after surgery, and increased physical and mental problems (Field & Haloob, 2016; Sun et al., 2019; WHO, 2015).
Depression is a mood disorder with a wide spectrum of fluctuating manifestations and is associated with increased risk of mortality and morbidity. The gestational period can increase women’s vulnerability to psychiatric diseases such as depression while prenatal depression affects 8-11% of women in developed countries, overall rates of depression during pregnancy reach 13% (Martínez-Paredes & Jácome-Pérez, 2019). Various environmental and genetic factors, such as hormonal changes, physical and emotional demands of pregnancy, as well as inadequate social support predispose pregnant women to perinatal depression. Furthermore, personal or family history of depression may increase the risk (Ghimire et al., 2021). Before surgery, patients experience high levels of fear, anxiety, and uncertainty about surgery, as well as general symptoms of anxiety and depression (Guy, 2015). In a study by Ryding et al. (2015), it was reported that fear of childbirth caused higher cesarean delivery rates in women with mental problems.
Some non-pharmacological practices can be performed to reduce the pain, anxiety, fear, and stress of a woman before delivery, and to help her have a positive childbirth experience (Sun et al., 2019). In the studies so far, it is reported that practices such as listening to music and providing information are effective in minimizing complications during and after surgery and reducing pain, anxiety, and fear (Field & Haloob, 2016; Hepp et al., 2018; Sun et al., 2019). It is noted that training patients cannot only increase their level of knowledge but also help them improve their coping skills (Saliminia et al., 2019). In another study, it was found that music listened to during labor and training given to primiparous pregnant women has positive effects on the labor process, reduces anxiety, labor pain, and sensitivity, while increasing control and cooperation in the mother (Sun et al., 2019). In another study, it was concluded that music listened to during cesarean section is an easily applicable and effective way to reduce the stress and anxiety of expectant mothers (Hepp et al., 2018). In addition, there are studies in the literature that report that listening to music is effective in lowering blood pressure and pulse in individuals (Handan et al., 2018; Ikonomidou et al., 2004; Labrague, et al., 2013; Liu et al., 2010; Ribeiro et al., 2018). However, practices such as training and listening to music can also increase women’s awareness of childbirth and enable them to prepare for childbirth more consciously (Hepp et al., 2018; Labrague, et al., 2013; Liu et al., 2010; Ribeiro et al., 2018).
By providing both physical and mental comfort to women through training and listening to music before a cesarean section, complications during and after cesarean section can be minimized, pain levels and fears of the unknown can be reduced, and the development of physical and mental problems that may occur during the postpartum period can be prevented. In this way, both the mother and the baby start a healthier postpartum process. Moreover, the findings obtained as a result of this study may guide midwives and nurses, who have important roles in the preoperative process, to plan and implement their provision of care. As a result, when the literature was examined, it was reported that the music played and the planned education given during the perioperative period increased patient satisfaction and reduced the patient’s fear, anxiety, and depression (Ersanlı Kaya & Kömürcü, 2016; Tan et al., 2020). In Turkey, the application of listening to music as a noninvasive intervention in the perioperative setting is limited in obstetrics and gynecology. Spontaneous training is provided instead of detailed planned training before cesarean section. In this context, this research was conducted to determine the impact of a planned training program and music on fear, anxiety, and depression among women undergoing cesarean section.
Music therapy positively affects women’s quality of life by reducing fear, anxiety, and depression. Especially before surgery, the uneasiness experienced by women in the face of the unknown affects mental health.
Hypotheses
-
H1: Music listened to by pregnant women before a cesarean section had an effect on fear of surgery.
-
H2: A planned training given to pregnant women before a cesarean section had an effect on fear of surgery.
-
H3: Music listened to by pregnant women before a cesarean section had an effect on anxiety and depression.
-
H4: A planned training given to pregnant women before a cesarean section had an effect on anxiety and depression.
Material and Methods
Study design
The randomized controlled experimental study was conducted based on the pre-test and post-test model. The study consisted of three groups as the experimental group (music and planned training) and the control group. Groups were randomly selected using https://randomizer.org/.
Setting and Sample
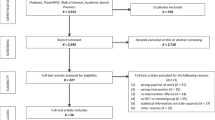
The study population consisted of pregnant women admitted to the Obstetrics and Gynecology Department of a hospital located in the Black Sea Region in Turkey for a planned cesarean section. This study was planned to compare the three groups (who listened to music, trained, and the control group) before cesarean section in terms of determining the effect of surgical fear, anxiety, and depression. The required minimum sample size was determined with the help of power analysis. Since the aim of the study was to determine the effect of surgery on fear, anxiety, and depression, one way ANOVA was chosen a priori to be used in power analysis. The reason for choosing this test is that three groups will be compared quantitatively in the study. In the study, with 5% type 1 error, 0.30 Cohen standardized effect size, three groups and 80% power, the minimum sample size was calculated as at least 111 in total (for three groups). The pregnant women in the study sample were divided into three groups by randomization: the music group (n = 40), the planned training group (n = 40), and the control group (n = 40) (Fig. 1). The data were collected between December 1, 2020, and March 30, 2021.
Inclusion criteria
-
Women who were hospitalized for planned cesarean section,
-
No previous history of surgery,
-
Having the first pregnancy,
-
Between the ages 19 and 35,
-
Who had no diagnosis of a physical or mental disease,
-
Who had no physical illness in her baby,
-
Women who agreed to participate in the research were included in the study.
Exclusion Criteria
-
Emergency caesarean section,
-
Multiparity,
-
Previous history of surgery,
-
Who had diagnosis of a physical or mental disease,
-
Incomplete completion of research questions.
Data collection tools
Personal Information Form: This form has 24 items, covering the socio-demographic characteristics, such as age, education, family type, smoking status, income level, place of residence, history of previous surgery (12 items), and pregnancy and childbirth-related items (12 items).
Surgical Fear Questionnaire (SFQ): SFQ was developed by Theunissen et al. (2014), and its validity and reliability study was conducted by Bağdigen and Karaman Özlü (2018). The scale is an 11-point Likert type scale, consisting of eight items, scored between 0 and 10 points each. The scale consists of two sub-scales, consisting of four items each, measuring short-term fears and long-term fears related to the source of fear. The items in the scale are evaluated as “0:I am not afraid at all” to “10:I am very afraid”.
Hospital Anxiety and Depression Scale (HADS): HADS was developed by Zigmond and Snaith (1983), and its validity and reliability study was conducted by Aydemir et al. (1997). It is used for diagnosing anxiety and depression in a short time and determining the risk group. It is a 4-point Likert-type scale consisting of 14 items in total. There are seven items in the Anxiety and Depression sub-scale, and they are scored in the range of 0–3 points. The lowest and highest scores that can be taken in the sub-scales are 0 and 21, respectively.
Procedure
By visiting the women who met the research criteria, the purpose of the study was explained and their written informed consent was obtained. Women in all three groups were interviewed individually. This study was conducted in two sessions using pre- and post-tests. The Personal Information Form, the SFQ, and the HADS were filled out using the face-to-face interview method by the researcher for the women included in the music, training, and control groups on the day of their hospitalization (pre-test).
Support was received from experts working in the Faculty of Fine Arts of the university regarding the selection and application of music used in the research. In the study, the music played to women was composed of Turkish music modes, namely the Hejaz, Neva, and Acemaşıran modes. Turkish music is a genre of music with maqam unique to Turkish culture. It is among the most important elements of Turkish culture as it allows individuals to express their feelings easily. Our aim in including Turkish music makams in our study is to enable women to easily express their feelings in terms of spirituality in order to eliminate the fear, pain, and anxiety they experience before cesarean delivery. The Hejaz Mode is effective on the urogenital tract, raises the low pulse rate, and gives a sense of modesty. The Neva Mode in music relieves sadness and is useful in the treatment of mental illnesses. Acemaşıran Mode revives thoughts and emotions, facilitates childbirth, helps to relax, and relieves pain and spasm. Owing to these effects, instrumental music included in three music modes was used in the research based on export recommendation (Kılıç & Gurkan, 2021; TUMATA, 2020). Among the music we use in our study, ney and water sound are used in the Hijaz maqam, ney, kopuz, water sound, rebap, oud and ney are used in the Acemashiran maqam. The common feature of these instruments is that the emotions that people cannot express turn into sound and provide spiritual and physical integrity.
After the pre-test, the women in the music group listened to nonverbal, instrumental music in the Hejaz, Neva, and Acemaşıran Modes for 12 min with headphones, during the period when they felt well. Then, 1 h after the first music was played before the surgery, the music was listened to for 12 min again for the second time in the same way. SFQ and HADS were repeated 24 h after the surgery (post-test) (Fig. 2).
It is normal to experience fear and anxiety during the preoperative period so after the pre-test, the women in the training group received training on the psychological, physiological, legal preparation, pre- and post-surgery conditions, prepared in accordance with the literature, given by the researcher in a face-to-face setting, individually in accordance with the terms of adult training. The content of the training includes what a cesarean section is, why a cesarean section should be performed, before the surgery, clothes to wear, and the time to stop eating before the surgery and about post-operative baby care, breastfeeding, mobilization, etc., information is included. During the training, lecturing, discussion, question and answer methods, and a brochure developed by the researcher were used as course materials. Training given to each participant lasted approximately 30–45 min. SFQ and HADS were repeated 24 h after the surgery (post-test) (Fig. 2).
Standard care practices in the hospital were also performed for the women in the control groups (Fig. 2). The standard care includes admission of the patient to the clinic, obtaining her anamnesis, opening vascular access, performing a nonstress test, installing a urinary probe, receiving pre-operative instructions, and checking legal permits. The women included in the control group did not listened to music and planned training was not provided, only filling out the forms (pretest–posttest) was provided. Filling out the questionnaires took 10–15 min on average in all groups.
Statistical analysis
Research data were evaluated using the SPSS 23.0 program. The normal distribution of the data was tested by the Kolmogorov–Smirnov test and Shapiro–Wilk test. Number and percentile distribution were used to evaluate the socio-demographic characteristics of the women, the chi-square test was used to compare the characteristics between the groups, one-way analysis of variance (ANOVA) was used to compare the mean scores in the follow-up between the groups. In addition, the Bonferroni test was used to determine the group that differs, and the mean and standard deviation were used to evaluate the scale scores. The significance level was 0.05 for all tests, calculated with a 95% confidence interval.
Clinical trial registration number
The study was registered at ClinicalTrials.gov (NCT05570201).
Results
The mean age of the women in the music group was 26.0 (SD 3.63) (min 19, max 35), the mean age of the women in the training group was 25.50 (SD 3.09) (min 18, max 31), and the mean age of the women in the control group was 26.4 (SD 3.42) (min 18, max 35). Some socio-demographic characteristics (age, education, family type, smoking status, income level, place of residence, history of previous surgery) of the women in the music, training, and control groups were similar, and there was no statistically significant difference between the groups (p > 0.05, Table 1).
The status of having received training on childbirth before the surgery was similar for the music, training, and the control groups, and there was no statistically significant difference between the groups (p > .05). Of the women, 90% in the music group, 87.5% in the training group, and 80% in the control group reported that they had not received training on childbirth, and 97.5% of the women in the music and training groups, and all of the women in the control group (100%) stated that they did not receive any training before surgery.
There was a statistically significant difference between the women in the music, training, and control groups prior to cesarean surgery in terms of pre-test SFQ sub-scale short-term scores, whereas there were statistically significant differences between the long-term and general SFQ scores (p > 0.05). According to the results of the advanced analysis, the short-term surgical fears of the training group were significantly higher in the pre-test compared to the music group.
In the post-test after the training and listening to music, statistically significant differences were found between the music, training, and the control groups in terms of the short-term, long-term sub-scale scores and the overall score of the SFQ (p < 0.05). According to the results of the advanced analysis, the short-term (p = 0.001) and general surgical fears (p = 0.001) of the music group and training group were significantly lower than those of the women in the control group. The long-term surgical fear scores (p = 0.001) of the training group were found to be significantly lower compared to the music and control groups (Table 2).
In the pre-test, a statistically significant difference was found between the music, training, and control groups’ anxiety scores of the HADS sub-scales (p < 0.05). According to the results of the advanced analysis of the group that has listened to music in the pre-test before the procedure were significantly higher than those of the training and control group (Table 3).
In the post-test, a statistically significant difference was found between the music, training, and control groups in terms of the anxiety scores, of the HADS sub-scales, after the training and listening to music applications (p < 0.05). According to the results of the advanced analysis, the anxiety scores (p = 0.042) of the training group were significantly lower than the music group (Table 3).
Discussion
This research was conducted to determine the impact of a planned training program and music on fear, anxiety, and depression among women undergoing cesarean section. The structure of the maqam, its melodic features, the method used, the variety of forms, lyrics, and instruments are full of the subtleties of a very wide geography and a cultural accumulation. Turkish music makams, which are shaped as a result of their cultural and social lives and human relations and reflect their cultural identity, reflect the characteristics of the historical past. Since the authorities are shaped by historical, sociological, cultural interactions, they are very important in expressing the feelings and thoughts of people. In our study, listening to music before cesarean section was chosen to reduce surgical fear and anxiety. The Hejaz Mode is effective on the urogenital tract, raises the low pulse rate, and gives a sense of modesty. The Neva Mode in music relieves sadness and is useful in the treatment of mental illnesses. Acemaşıran Mode revives thoughts and emotions, facilitates childbirth, helps to relax, and relieves pain and spasm. Owing to these effects, instrumental music included in three music modes was used in the research based on literature recommendation (Kılıç & Gurkan, 2021; TUMATA, 2020). Planned training is important in eliminating the uncertainty about the birth and postpartum period, including the woman in the process, and eliminating surgical fear and anxiety as a result of being informed about the procedures.
Since it is an important life experience for women, a pregnancy process that ends in the best way is extremely important from the point of view of the mother, the baby, and the family. In this context, the support of health care professionals using non-pharmacological methods such as playing music and providing information for pregnant women makes it even easier for a woman to adapt to the childbirth process (Karabulutlu, 2014).
A maximum of 40 points can be obtained from the short-term Surgical Fear Questionnaire. In this study, considering the short-term surgical fears of the music, training, and the control groups in the pre-test, it is seen that the scores of all three of them were above the average. Accordingly, undergoing a cesarean section, no previous history of surgery (83.3% for all the three groups), the experience of first pregnancy, and the fear that something will happen to them and their babies or they may die may explain the above-average levels of fear during this period. A study has shown that patients who have not previously undergone surgery and have not been hospitalized have high levels of fear (Kaya & Karaman Özlü, 2019). This result supports our study finding and draws attention to the issue of reducing women’s fears before surgery.
In our study, the short-term and general surgical fear levels of the music group in the post-test were significantly lower than the women in the control group. Accordingly, listening to music was effective in reducing women’s short-term and general surgical fears, supporting our H1 hypothesis. Factors such as lack of hospital experience, the idea of surgery and pain, side effects of surgery, fear of injections and anesthesia can be considered as the causes of short-term fears of surgery (Bağdigen & Karaman, Özlü,2018). It has been reported that the music listened to before surgery also contributes to reducing fears since it distracts patients (Gonçalves et al., 2017). These results support our research findings.
In our study, short-term and general surgery fears of the women after training were found to be significantly lower than those in the control group, and long-term surgery fears were also found to be significantly lower than those in the music and the control groups. Accordingly, training given before the surgery was effective in reducing women’s short-term, long-term, and general surgical fears, supporting our H2 hypothesis. In the literature, it is stated that the level of fear of the unknown is high in individuals who have not previously undergone any surgical intervention (Gonçalves et al., 2017; Kiyohara et al., 2004). In this case, it is recommended to help patients who will undergo surgery to cope with their fears by allowing them to express their feelings and to provided information in accordance with their requirements (Akman Kılınç & Şenturan, 2020). A study has shown that the training given by health care professionals in the preoperative period reduces the levels of surgical fear (Ramesh et al., 2017). In another study, it was reported that providing information and providing support to reduce fear experienced before surgery also reduces individuals’ long-term fear levels (Çetinkaya & Karabulut, 2010). In addition, a study conducted by Doğu (2013) found that training given before surgery was effective in reducing surgical fears in 68.6% of individuals, which supports our study finding and draws attention to the importance of training (Doğu, 2013).
Anxiety scores of the women were found to be significantly lower after the training. Accordingly, the planned training given was effective in reducing women’s anxiety scores before the cesarean section, supporting our H4 hypothesis. An increase in anxiety in pregnant women can most often be caused by a sense of uncertainty related to childbirth (Ersanlı Kaya & Kömürcü, 2017; Fındık & Yıldızeli Topçu, 2012). Therefore, it is believed that with the planned training given to individuals, their fear of the unknown and anxiety levels decreases and they are relieved as a result. Similarly, in one study, it was concluded that planned preoperative training has a significant effect on reducing preoperative anxiety in pregnant women undergoing elective cesarean section under spinal anesthesia (Kalliyath et al., 2019). In another study, it was found that the training provided to the experimental group before a cesarean section decreases anxiety levels significantly compared to the control group (Ribeiro et al., 2018). Similar to our research, the importance of training is emphasized in the study by Saliminia et al. (2019), who found that levels of fear decrease in pregnant women after a face-to-face training and brochure given before the cesarean section (Saliminia et al., 2019). In addition, some study results in the literature show that anxiety levels decrease after providing training during labor (Bastani et al., 2006; Eslami et al., 2020; Guszkowska et al., 2013). It is seen that these results support our research findings.
Another non-pharmacological method used to reduce the anxiety levels of individuals before surgery is listening to music (Hepp et al., 2018; Handan et al., 2018). In our study, although it was concluded that training was significantly more effective in reducing anxiety than listening to music, the anxiety scores of the group that listened to music were found to decrease after listening to music. Similarly, in a study, the music chosen by the patient used as a perioperative intervention was found to cause a low level of change in anxiety scores and helped the mother’s mood level to remain stable (Denney et al., 2018). In another study, music was listened to by primipara pregnant women during labor, and it was found that music was effective in reducing anxiety levels (Ersanlı Kaya & Kömürcü, 2017). Hepp et al. (2018) concluded that music reduces anxiety levels after childbirth, and in a study by Handan et al. (2018), music therapy was found to reduce the physiological and cognitive responses of anxiety in women who have undergone multiple cesarean sections (Hepp et al., 2018; Handan et al., 2018). In addition, according to the results of a systematic review study, it was found that listening to music leads to relaxation in women, a decrease in anxiety levels, a decrease in psychosocial stress, and depression and other study findings are also in line with our finding (Shimada et al., 2021).
Study limitations
This study has some limitations. This study includes women admitted to the hospital for a planned cesarean section in Turkey, and the results obtained cannot be generalized to all women who underwent cesarean section. The study was conducted in a small province in the Black Sea region of Turkey, where the number of births is not very high. Therefore, the small sample size is another limitation. In addition, owing to the fact that the data was collected during the COVID-19 pandemic, longer follow-up and post-testing 24 h after the surgery was another limitation of the study.
Conclusion
While the provision of training and listening to music before the cesarean section was effective in reducing women’s short-term and general surgical fears, the planned training was effective in reducing their short-term, long-term, and general surgical fears and anxiety levels. In line with these results, it is recommended to play music for pregnant women to reduce their fear and anxiety levels before cesarean section, to provide planned training for cesarean section surgery and the postpartum period, to create an appropriate physical environment for listening to music and training in operating rooms. In addition, it is recommended to provide necessary tools for listening to music (headphones, CD player, MP3 player, etc.), inform health care professionals, and conduct studies with large sample groups that also use different modes in Turkish music.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Akman Kılınç, E., & Şenturan L. (2020). Effect of face-to-face education on patient’s anxiety in perioperative period: A randomized controlled trial. Journal of Izmir Katip Celebi University Faculty of Health Sciences, 5, 291-297. Retrieved from https://dergipark.org.tr/en/pub/ikcusbfd/issue/57021/690065
Aydemir, Ö., Güvenir, T., Küey, L., & Kültür, S. (1997). Reliability and Validity of the Turkish version of Hospital Anxiety and Depression Scale. Turkish Journal of Psychiatry, 8, 280–287. Retrieved from https://www.researchgate.net/publication/284678404_Validity_and_Reliability_of_Turkish_Version_of_Hospital_Anxiety_and_Depression_Scale
Bağdigen, M., & Karaman Özlü, Z. (2018). Validation of the Turkish Version of the Surgical Fear Questionnaire. Journal of PeriAnesthesia Nursing, 33, 708–714. https://doi.org/10.1016/j.jopan.2017.05.007
Bastani, F., Hidarnia, A., Montgomery, K. S., Aguilar-Vafaeii, M. E., & Kazemnejad, A. (2006). Does relaxation education in anxious primigravid Iranian women influence adverse pregnancy outcomes? a randomized controlled trial. J Perinat Neonatal Nursing, 20, 138–146. https://doi.org/10.1097/00005237-200604000-00007
Çetinkaya, F., & Karabulut, N. (2010). The impact on the level of anxiety and pain of the training before operation given to adult patients who will have abdominal operation. Journal of Anatolia Nursing and Health Sciences,13, 20–26. https://doi.org/10.4236/ss.2011.26065. Retrieved from https://www.scirp.org/journal/paperinformation.aspx?paperid=6880
Denney, J. M., Blackburn, K. L., Bleach, C. C., Martinez, A. R., Philips, J. B., Lanier, K., Dean, L., & Mertz, H. (2018). The effects of music intervention on women’s anxiety before and after cesarean delivery: A randomized controlled trial. Music and Medicine, 10, 225–232. https://doi.org/10.47513/mmd.v10i4.622.
Doğu, Ö. (2013). Meeting the needs of education and training in patients with planned surgery preparation psychological effects of individual patient-Sakarya sample. Duzce University Journal of Health Sciences Institute, 3, 10–13.
Ersanlı Kaya, C., & Kömürcü, N. (2017). Effect of education and musical therapy given during labor on the process of birth in ınduced primipara pregnant women. International Journal of Medical Science and Clinical Inventions, 4, 2797–2807. https://doi.org/10.18535/ijmsci/v4i3.14. Retrieved from https://valleyinternational.net/index.php/ijmsci/article/view/731
Eslami, J., Hatami, N., Amiri, A., & Akbarzadeh, M. (2020). The potential beneficial effects of education and familiarity with cesarean section procedure and the operating room environment on promotion of anxiety and pain intensity: A randomized controlled clinical trial. J Educ Health Promot, 9, 240. https://doi.org/10.4103/jehp.jehp_31_20
Fındık, Ü. Y., & Yıldızeli Topçu, S. (2012). Effect of the way of surgery on preoperative anxiety. Faculty of Health Sciences Nursing Journal, 19, 22–33. Retrieved from https://dergipark.org.tr/tr/download/article-file/88619
Gonçalves, M., Cerejo, M. N. R., & Martins, J. C. (2017). The influence of the information provided by nurses on preoperative anxiety. Revista de Enfermagem Referência, 14, 17–26. https://doi.org/10.12707/RIV17023
Ghimire, U., Papabathini, S. S., Kawuki, J., Obore, N., & Musa, T. H. (2021). Depression during pregnancy and the risk of low birth weight, preterm birth and intrauterine growth restriction-an updated meta-analysis. Early Human Development, 152, 105243. https://doi.org/10.1016/j.earlhumdev.2020.105243
Group for the Research and Promotion of Turkish Music (TUMATA), http://www.tumata.com, 2020 (accessed 3 October 2022).
Guszkowska, M., Langwald, M., & Sempolska, K. (2013). Influence of a relaxation session and an exercise class on emotional states in pregnant women. Journal of Reproductive and Infant Psychology, 31, 121–133. https://doi.org/10.1080/02646838.2013.784897
Guo, P. (2015). Preoperative education interventions to reduce anxiety and improve recovery among cardiac surgery patients: A review of randomised controlled trials. Journal of clinical nursing, 24(1–2), 34–46. https://doi.org/10.1111/jocn.12618
Field, A., & Haloob, R. (2016). Complications of caesarean section. The Obstetrician and Gynaecologist, 18, 265–272. https://doi.org/10.1111/tog.12280
Handan, E., Canbulat Sahiner, N., Demirgöz Bal, M., & Dissiz, M. (2018). Effects of music during multiple ceseraen section delivery. Journal of the College of Physicians and Surgeons Pakistan, 28, 247–249. https://doi.org/10.29271/jcpsp.2018.03.247
Hepp, P., Hagenbeck, C., Gilles, J., Wolf, O. T., Goertz, W., Janni, W., Balan, P., Fleisch, M., Fehm, T., & Schaal, N. K. (2018). Effect of music intervention during caesarean delivery on anxiety and stress of the mother a controlled, randomised study. BMC Pregnancy and Childbirth, 18, 435. https://doi.org/10.1186/s12884-018-2069-6
Ikonomidou, E., Rehnström, A., & Naesh, O. (2004). Effect of music on vital signs and postoperative pain. AORN Journal, 80, 269–278. https://doi.org/10.1016/s0001-2092(06)60564-4
Karabulutlu, O. (2014). Non-pharmacological methods used in labor pain control. Caucasian Journal of Science, 1, 43–50. Retrieved from https://dergipark.org.tr/tr/pub/cjo/issue/33897/384968
Kaya, M., & Karaman Özlü, Z. (2019). The determination of the relationship between the perception of surgical fear and social support in patients who undergoing elective surgery. Journal of Anatolia Nursing and Health Sciences, 22, 281–290, https://doi.org/10.17049/ataunihem.550029. Retrieved from https://nursing-ataunipress.org/en/the-determination-of-the-relationship-between-the-perception-of-surgical-fear-and-social-support-in-patients-who-undergoing-elective-surgery-16157
Kalliyath, A. K., Korula, S. V., Mathew, A., Abraham, S. P., & Isac, M. (2019). Effect of preoperative education about spinal anesthesia on anxiety and postoperative pain in parturients undergoing elective cesarean section: A randomized controlled trial. J Obstet Anaesth Crit Care, 9, 14–17. https://doi.org/10.4103/joacc.JOACC_35_18
Kılıç, A., & Gurkan, O. C. (2021). Evidence-based use of music therapy during pregnancy, birth and postpartum. KTO Karatay University Journal of Health Sciences, 2(1), 47–60.
Kiyohara, L. Y., Kayano, L. K., Oliveira, L. M., Yamamoto, M. U., Inagaki, M. M., Ogawa, N. Y., Gonzales, San Martin, & P.E., Mandelbaum, R., Okubo, S.T., Watanuki T., & Vieira, J. E. (2004). Surgery information reduces anxiety in the pre-operative period. Rev Hosp Clín Fac Med Sao Paulo, 59, 51–56. https://doi.org/10.1590/s0041-87812004000200001
Labrague, L. J., Rosales, R. A., Rosales, G. L., & Fiel, G. B. (2013). Effects of soothing music on labor pain among Filipino mothers. Clinical Nursing Studies, 1, 35–42. https://doi.org/10.5430/cns.v1n1p35
Liu, Y. H., Chang, M. Y., & Chen, C. H. (2010). Effects of music therapy on labour pain and anxiety in Taiwanese first-time mothers. J Clin Nurs, 19, 1065–1072. https://doi.org/10.1111/j.1365-2702.2009.03028.x
Martínez-Paredes, J. F., & Jácome-Pérez, N. (2019). Depression in pregnancy. Revista Colombiana de Psiquiatría (English ed.), 48(1), 58–65. https://doi.org/10.1016/j.rcpeng.2017.07.002
Ramesh, C., Nayak, B. S., Pai, V. B., Patil, N. T., George, A., George, L. S., George, L. S., & Sanatombi Devi, E. (2017). Effect of preoperative education on postoperative outcomes among patients undergoing cardiac surgery: A systematic review and meta-analysis. J Perianesth Nurs, 32, 518–529. https://doi.org/10.1016/j.jopan.2016.11.011
Ribeiro, M. K. A., Alcântara-Silva, T. R. M., Oliveira, J. C. M., Paula, T. C., Dutra, J. B. R., Pedrino, G. R., Simoes, K., Sousa, R. B., & Rebelo, A. C. S. (2018). Music therapy intervention in cardiac autonomic modulation, anxiety, and depression in mother of preterms: randomized controlled trial. BMC Psychol, 6, 57. https://doi.org/10.1186/s40359-018-0271-y
Ryding, E. L., Lukasse, M., Parys, A. S. V., Wangel, A. M., Karro, H., Kristjansdottir, H., Schroll, A.M., Schei, B., & Bidens Group. (2015). Fear of childbirth and risk of cesarean delivery: A cohort study in six European countries. Birth, 42(1), 48–55. https://doi.org/10.1111/birt.12147
Saliminia, A., Azimaraghi, O., Ebadi, Z., Azizinik, F., & Movafegh, A. (2019). Impact of face-to-face educational outreach plus printed materials on preoperative anxiety level in Iranian parturient undergoing elective cesarean section delivery. Archives of Anesthesiology and Critical Care, 5, 41–44. https://doi.org/10.18502/aacc.v5i2.749.
Shimada, B. M. O., dos Santos, M. S. O. M., Cabral, M. A., Silva, V. O., & Vagetti, G. C. (2021). Interventions among pregnant women in the field of music therapy: A systematic review. Rev Bras Ginecol Obstet, 43, 403–413. https://doi.org/10.1055/s-0041-1731924
Sun, Y., Huang, K., Hu, Y., Yan, S., Xu, Y., Zhu, P., & Tao, F. (2019). Pregnancy-specific anxiety and elective cesarean section in primiparas: A cohort study in China. PLoS One, 14, e0216870. https://doi.org/10.1371/journal.pone.0216870
Tan, D. J. A., Polascik, B. A., Kee, H. M., Hui Lee, A. C., Sultana, R., Kwan, M., Raghunathan, K., Belden, C. M., & Sng, B. L. (2020). The effect of perioperative music listening on patient satisfaction, anxiety, and depression: A quasiexperimental study. Anesthesiology research and practice, 2020, 1–6. https://doi.org/10.1155/2020/3761398
Theunissen, M., Peters, M. L., Schouten, E. G. W., Fiddelers, A. A. A., Willemsen, M. G. A., Pinto, P. R., Gramke, H. F., & Marcus, M. A. E. (2014). Validation of the surgial fear question naire in adult patients waiting for elective surgery. PLoS One, 9, e100225. https://doi.org/10.1371/journal.pone.0100225
Turkey Demographic and Health Survey (TDHS), Hacettepe University Institute of Population Studies, Retrieved on October 3, 2022 .https://hips.hacettepe.edu.tr/en/2018_turkey_demographic_and_health_survey-198,
World Health Organization. Department of Reproductive Health and Research. World Health Organization, Retrieved on October 3, 2015 from https://www.who.int/reproductivehealth/publications/maternal_perinatal_health/cs-statement/en/
Zigmond, S., & Snaith, P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand, 67, 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
Acknowledgements
The authors are grateful to the Editor of Journal of Current Psychology and the reviewers for providing us with insightful suggestions to make this work more valuable.
Funding
Open access funding provided by the Scientific and Technological Research Council of Türkiye (TÜBİTAK). No funding was received for conducting this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest regarding the publication of this paper.
Ethical Considerations
After obtaining the ethics committee approval from the Non-Interventional Clinical Research Ethics Committee of the University (decision no: 2019-10/21), written permission was also obtained from the studied institution. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Guney, D., Pinar, S.E. Effects of planned training and music listened to before a cesarean section on surgical fear, anxiety and depression: A randomized controlled trial. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-06095-1
Accepted:
Published:
DOI: https://doi.org/10.1007/s12144-024-06095-1