
Abstract
Type I diabetes mellitus (T1D) is a condition typically diagnosed during adolescence. The diagnosis of T1D, combined with the typical changes that occur during this developmental period, can have an impact on the psychopathology of adolescents. The aim of this study is to evaluate the effectiveness of a psychological intervention incorporating new technologies in managing psychopathological aspects among adolescents with T1D. A systematic search was carried out using the PRISMA method in the ProQuest and Web of Science databases, resulting in the screening of 209 studies, of which nine were included. Two evaluators independently and blindly selected and assessed the studies, demonstrating an excellent level of agreement. The age range of participants in the included studies varied from 12 to 21, with the common factor being a T1D diagnosis. The studies examined various variables, such as adherence to treatment, quality of life, and symptoms of depression and anxiety. Many of the studies indicated improvements in these aspects. However, it is crucial to note that the overall quality of the studies was low. Consequently, there is a need for further research on psychological interventions incorporating new technologies, and there is room for improvement in the design quality of such studies. While acknowledging the current limitations, the future of interventions for T1D is intricately linked to advancements in the development and integration of new technologies.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Adolescence and T1D
Adolescence is the transitional phase that bridges childhood and adulthood. Allen and Waterman (2019) delineate three distinct stages: early adolescence spanning 10 to 13 years, middle adolescence covering 14 to 17 years, and late adolescence extending from 18 to 21 years. Preceding adolescence is preadolescence, which typically begins around age 9. Throughout both preadolescence and adolescence, continual physical and psychological changes occur, accompanied by pubertal development (Papalia & Martorell, 2017). Puberty represents a transformative stage marked by change and stress for adolescents. The hypothesis of stressful change posits an increased likelihood of psychopathology during this period (Allen & Waterman, 2019), with the risk escalating if the adolescent has a chronic condition such as diabetes.
Diabetes mellitus represents a significant noncommunicable ailment (Katz et al., 2015). The World Diabetes Report (OMS, 2016) classifies diabetes into two types: type 1 diabetes mellitus (T1D), resulting from insufficient insulin regulation of glucose concentration in the pancreas, and type 2 diabetes mellitus (T2DM), stemming from the body’s inability to effectively utilize produced insulin. While T2DM is more prevalent in the general population, T1D takes precedence among children and adolescents (Neves et al., 2017). Globally, diabetes has witnessed a dramatic surge, posing a substantial threat to mortality, with 1.5 million reported deaths in 2019 (OMS, 2021). Regarding T1D, studies in Spain estimate an incidence of 11–15 cases per 100,000 inhabitants under 15 years of age and a prevalence ranging between 0.08 and 0.2% (Gómez-Peralta et al., 2021). This presents a significant social challenge, requiring effective interventions, especially during the critical stages of preadolescence and adolescence (ages 10 to 15), when incidence rates are higher (Gómez-Rico et al., 2015; Pérez-Marín et al., 2015). This developmental period, marked by adolescents navigating stressful situations compounded by the adverse impacts of the disease, renders them more susceptible to psychological, physical, and social issues, as well as a diminished quality of life and treatment adherence (Dantzer et al., 2003; ; Pérez-Marín et al., 2015; Rechenberg et al., 2017). Addressing these challenges is imperative for enhancing the well-being of adolescents grappling with diabetes.
Psychopathology and type 1 diabetes in adolescents
A substantial number of adolescents grappling with type 1 diabetes mellitus (T1D) encounter an elevated risk of facing physical, psychological, and social challenges. This vulnerability is associated with the developmental stage in the life cycle and the complexities arising from the disease itself (Rechenberg et al., 2017). These complications demonstrate a bidirectional relationship, contributing to an increased prevalence of emotional issues (Pérez-Marín et al., 2015). Emotional problems in adolescents with T1D result from the cumulative impact of living with a chronic condition, encompassing factors such as pain, weakness, the necessity for care, and potential hospitalizations. Additionally, diabetes-specific stressors, including daily treatment routines, meticulous self-care practices, insulin injections, continuous blood glucose monitoring, dietary restrictions, limitations on physical activity, and ongoing apprehension about future physical and psychological consequences, contribute to these emotional challenges (Pérez-Marín et al., 2015; Souza et al., 2019).
Research by Rechenberg et al. (2017) highlighted that adolescents with T1D exhibit elevated stress levels, including disease-specific stress, negatively correlated with glycemic control, self-regulation behaviors, and overall quality of life compared to their non-diabetic peers (Bekele et al., 2022; Jensen et al., 2022). Furthermore, the constant oversight and control exerted by parents, caregivers, and relatives over the care of adolescents with T1D can serve as an additional stressor. This is particularly challenging during a crucial developmental stage when adolescents are striving for independence and autonomy (Gómez-Rico et al., 2015; Montali et al., 2022). The compounding effect of these stressors, combined with the typical challenges of adolescence, fosters the development of emotional problems and psychopathologies in adolescents with T1D (Gómez-Rico et al., 2015; Souza et al., 2019; Whittemore et al., 2010). Addressing these multifaceted stressors is crucial for promoting the well-being of adolescents navigating the complexities of diabetes.
Within the population of adolescents with T1D, depression or depressive symptoms are the most prevalent psychological issues and diagnoses, as noted by Hong et al. (2021). Approximately 20% of these adolescents have encountered or are currently dealing with conditions such as anxiety disorders, challenges related to self-image, self-esteem, or eating disorders. These issues, in turn, give rise to additional complications, including difficulties in social relationships (Lazo & Durán-Agüero, 2019; Whittemore et al., 2010). The emotional and affective ramifications of these challenges exert a detrimental impact on the physical well-being of adolescents with T1D. This, in turn, leads to suboptimal health behaviors, compromised self-care practices, and reduced adherence to treatment, thereby jeopardizing their physical integrity (Lacomba-Trejo et al., 2019). Consequently, the complexities stemming from a chronic condition such as T1D become apparent, particularly among the adolescent demographic, who are navigating a pivotal period in their lives. Considering these challenges, it becomes crucial to implement effective psychological tools and interventions. These should be designed to focus on protective and preventive measures, addressing the inherent risks associated with adolescence and with T1D. By identifying, modifying, and intervening in situations, thoughts, and behaviors that may impact adolescents both physically and psychologically, we can better equip them to navigate the intersection of adolescence and chronic disease (Gómez-Rico et al., 2015).
Psychological interventions in type 1 diabetes
Psychological interventions play a crucial role in addressing the complexity and emotional implications associated with type 1 diabetes (T1D) among adolescents, as discussed above. Previous literature on psychological interventions emphasizes several reasons why these interventions are vital at this stage (Winkley et al., 2020). In recent decades, the growing recognition of the need for effective psychological interventions for adolescents with T1D has spurred ongoing research efforts to enhance both physical and psychological health, treatment adherence, and overall quality of life in this population. First, effective management of T1D extends beyond the physical aspects of the disease alone, encompassing the emotional and psychological challenges that adolescents may encounter (Espinoza & Vega, 2023). These challenges include adapting to physical changes and the daily demands of treatment, such as insulin administration, constant glucose monitoring, and dietary and exercise restrictions (Kamody et al., 2018). Second, the literature highlights that adolescents with T1D often experience psychological problems such as depression, anxiety, and stress (Gómez-Rico et al., 2015; Souza et al., 2019; Whittemore et al., 2010). The pressures associated with the day-to-day management of the disease, combined with the typical demands of adolescence, can result in a significant emotional burden (Ouzouni et al., 2019). Psychological interventions are essential to address these issues and improve the mental well-being of adolescents with T1D. Additionally, psychological interventions also focus on improving adherence to treatment (Kamody et al., 2018). The literature has noted that adolescents often face challenges in maintaining consistent adherence to medical recommendations, and psychological interventions can play a crucial role in motivating and supporting adolescents to follow recommended care guidelines.
A 2023 study by Espinoza and Vega examined interventions for physiological and psychosocial aspects in children, adolescents, and young individuals with T1D. Adolescents constituted 35.6% of interventions, with 51.1% utilizing therapeutic education and 26.7% employing psychological methods such as cognitive-behavioral models. Quantitative designs were prevalent (73.3%), with a sizable portion being pilot studies, often involving in-person family participation, and only 2.2% reporting favorable outcomes. The study revealed a reliance on face-to-face modalities, prompting the need for more flexible, technology-mediated approaches to better engage and support adolescents in managing T1D (Espinoza & Vega, 2023).
Traditionally, diabetes interventions have been conducted in person, posing challenges for patients in adhering to self-care programs. These challenges arise from a lack of personalized care and suboptimal communication between patients and healthcare specialists (Kitsiou et al., 2017). In the current landscape, marked by technological advancements and the transformative effects of the COVID-19 pandemic since 2020 (Ramkissoon, 2021a, b, 2022), there has been a significant surge in the utilization of new technologies across various intervention domains (Espinoza & Vega, 2023). The integration of new technologies into medical and health practices is commonly known as m-Health. Notably, mobile phones now boast a global usage rate of approximately 100%, ensuring universal access to tools like apps. These apps facilitate the tracking of blood glucose levels, dietary habits, daily physical activity, and self-care while simultaneously enhancing communication between patients and healthcare professionals (Kitsiou et al., 2017). Existing literature underscores the efficacy of internet interventions in reaching adolescents (Grey et al., 2013; Valverde-Merino, 2018). Moreover, this type of intervention has shown promise in symptom improvement, optimization of self-management, and the promotion of self-efficacy (Newton & Ashley, 2013; Valverde-Merino, 2018). The widespread use of mobile phones and the potential of internet interventions offer valuable avenues to overcome barriers and provide more accessible and individualized care for individuals managing diabetes.
Objectives
Intervention programs customized for adolescents with T1D are crucial; however, until now, there has been limited understanding of the utilization of new technologies in designing interventions for this demographic and assessing their effectiveness. Notably, m-Health has shown promising outcomes in various healthcare settings (Newton & Ashley, 2013; Valverde-Merino, 2018). Hence, this study aims to assess the effectiveness of such interventions specifically within the adolescent population dealing with T1D.
Methods
Procedure
To achieve our objective, we conducted a comprehensive systematic review of interventions incorporating new technologies in the psychological treatment of adolescents with T1D. The goal was to identify the characteristics of treatment and other factors contributing to the success of these interventions, providing a reference for future research. The review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standard (Shamseer et al., 2015).
The methodology employed to fulfill the proposed objectives involved a thorough analysis of the scientific literature on new technologies in psychological interventions for adolescents with T1D to assess their effectiveness. The research question posed was: Do adolescents with type 1 diabetes (T1D) show greater improvement when new technologies are integrated into psychological interventions compared to interventions that do not incorporate them?
For the data search, the ProQuest and Web of Science (WOS) databases were used. A preliminary search of bibliographies was performed to identify optimal descriptors and refine the search parameters. Based on the volume of information available on the topic and aligned with previous research, we selected keywords in both English and Spanish to gather international information. The following Boolean expression was formulated (Mesh terms and keywords): summary (diabetes type I) AND summary (adolescents *) AND (psychology intervention) AND (new technologies) in WOS ProQuest and TS = (diabetes type 1) AND (adolescents *) AND (psychology intervention) AND (new technologies) in WOS.
For the term “adolescent,” only the root was selected to prevent information loss by excluding derivations of the word (e.g., adolescence, adolescents, etc.). The term “type I diabetes” was chosen to exclude studies not specifically addressing adolescents with this disease. The terms “psychology intervention” and “new technologies” were used to refine the search, selecting only studies that evaluated psychological interventions utilizing new technologies. Despite a well-defined search in ProQuest (N = 50,501), numerous studies were found, and many deviated significantly from the required topic. To narrow the results, it was mandated that the terms “type I diabetes” and “adolescents*” be present in the summary: ((summary (diabetes type 1) AND summary (adolescents*))), limiting the results to 199.
Initially, no temporal criterion was set, resulting in the identification of numerous studies (N = 210), many of which did not genuinely address new technologies. Consequently, a temporal criterion was imposed for the previous five years to focus on updated studies coinciding with advancements in new technologies within psychology. This timeframe also emphasized the five years when, due to the COVID-19 pandemic, remote communication surged exponentially, amplifying the use of new technologies across various domains, including psychological interventions. Other inclusion criteria stipulated that full texts were accessible, articles were scientific, and in either Spanish or English. A total of 39 articles were identified, with 36 from ProQuest and three from Web of Science (WOS).
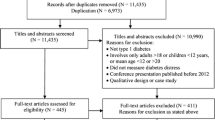
All articles were uploaded to Covidence, an online data extraction and screening tool (Covidence systematic review software, 2018). Duplicate articles (n = 1) were eliminated initially. Subsequently, two authors (PM and SV) independently reviewed all titles and abstracts, excluding studies not aligning with predetermined inclusion criteria. Titles excluded by either researcher or those with differing opinions (blinded) underwent a thorough examination and reevaluation based on inclusion and exclusion criteria. Disagreements between researchers were resolved through dialogue without the need for a third author to mediate. Following a final decision, all selected articles underwent a comprehensive full-text reevaluation by both authors. Each author independently determined whether to include the work in the review. Repeating the process, initially discarded articles or those with inclusion disagreements were thoroughly reviewed by each author. A final decision led to the inclusion of eight articles in the systematic review. Subsequently, a manual search was conducted through snowball sampling to identify relevant works within the references of the included articles. This search revealed one additional manuscript meeting the inclusion criteria. Figure 1 displays the flow diagram with the data and information used to answer the research question posed in this review.

Flow chart for study selection
Inclusion and exclusion criteria
The inclusion criteria were as follows: (a) the study assessed the efficacy of interventions that included new technologies; (b) the interventions targeted adolescents, (c) the disease type was T1D, (d) the study had to be a scientific article and be published in a scientific journal, (e) the publication had to be written in English or Spanish so that the authors could have a total understanding of the reading, (f) the article had to have been published in the past five years, in order to be up to date and refer to current technologies (2019 inclusive), and (g) the full text had to be complete and accessible via the University of Valencia databases.
Exclusion criteria were as follows: (a) nonadolescent population, (b) nonpsychological interventions, (c) interventions not directed at patients with T1D, (d) psychological interventions that did not use new technologies, (e) studies published in congresses, and (f) nonscientific articles. Once determined, all articles that met the inclusion criteria were included in the study. After the search of the bibliographies and with the relevant articles for our study selected, we proceeded to perform the analysis of the nine studies.
Quality assessment
To assess the quality of the studies, two authors (SV and PM) independently and blindly evaluated the included articles in this review using an adapted version of the “Study Quality Assessment Tool” developed by the “Effective Public Health Practice Project” (Thomas, 2003). The tool assessed seven criteria: (1) the study design (cross-sectional, descriptive, longitudinal studies, etc.), (2) representation and selection biases (randomization or lack thereof in the selection, generalizability of results to the rest of the population, sample size), (3) the number of dropouts and withdrawals (percentage of participants who dropped out in longitudinal studies, reasons for dropping out), (4) potential confounding factors (factors that may mask results), (5) data collection (how data are collected and whether the instruments are valid and reliable), (6) data analysis (quality of psychometric analyses and effect sizes), and (7) results (adequate information about objectives, hypotheses, and findings).
Scores for each criterion and study could be 1 (strong), 2 (moderate), or 3 (weak). The two evaluators (SV and PM) assigned scores for each criterion and study in a blinded manner. Subsequently, differences between the two were analyzed, and a joint agreement was reached, a process facilitated by minimal differences. For each study, there was an overall rating that could be strong, moderate, or weak based on the individual ratings for each criterion.
After resolving differences, each study received an overall quality score. A study was categorized as “strong” if there were no weak ratings and there were at least three strong ratings, “moderate” if there was a weak assessment or fewer than three strong ratings, or “weak” if there were two or more weak assessments. Therefore, a “strong” study indicated good quality, a “moderate” study indicated moderate quality, and a “weak” study indicated low quality (Glonti et al., 2015; Stroup et al., 2000).
Results
Study selection and screening
The study selection process for the included reviews is depicted in Fig. 1. After the bibliographic search in the databases was conducted, the temporal and inclusion and exclusion criteria were applied, and duplicate studies were eliminated, leaving a total of 38 articles. The researchers (SV and PM) read the titles and abstracts of the studies and jointly decided to exclude 22 that did not meet the inclusion criteria. In a second phase of the selection process, the researchers read the full text of the remaining 16 papers and excluded eight papers (five for not including a psychological intervention, two for not discussing new technologies, and one for not presenting a correct study design). This left eight for the review. A final study was included in the review by a method other than searching the databases. The article was found in the bibliography of a study included in the review and met all the criteria. Thus, the total number of studies selected for the review was nine.
Study characteristics
In this section, the participating results, the sample selection and research design, representativeness, variables, confounding factors, and inclusion and exclusion criteria of the different studies will be described (Table 1).
Participants
Table 1 summarizes the characteristics of the studies included in this review. The nine studies involved adolescent participants of both genders, totaling 628 participants with ages ranging from 13 to 22. The individual with the oldest reported age was considered a young adult. It is noteworthy that some studies incorporated adolescents’ relatives into the research (Holtz et al., 2021; Patton et al., 2022). As previously mentioned, the primary diagnosis for adolescents across the studies was T1D (Geirhos et al., 2022; Holtz et al., 2021; Malik et al., 2021; McAlpin et al., 2022; Paul and Moreno-Perez, 2019; Smith et al., 2021; Weissberg-Benchell et al., 2020). However, certain studies included samples with different diagnoses or comorbid problems. For instance, some focused on individuals facing challenges in adhering to the use of glucose monitors (Smith et al., 2021), while others examined adolescents with other chronic diseases and symptoms of anxiety and/or depression (Geirhos et al., 2022). One study partially selected adolescents without a T1D diagnosis but strongly associated with diagnosed individuals to report on a prevention program (Patton et al., 2022). Additionally, Larsen et al. (2022) exclusively chose Latina women from the United States as participants.
Sample selection and research design
In many of the studies, the prevalent design was a randomized controlled clinical trial (Geirhos et al., 2022; Larsen et al., 2022; Smith et al., 2021; Weissberg-Benchell et al., 2020). Single-focus group pilot studies were observed in some cases (Holtz et al., 2021; McAlpin et al., 2022), along with mixed-method feasibility designs incorporating both quantitative and qualitative data (Malik et al., 2021; Paul and Moreno-Perez, 2019), as well as qualitative designs (Patton et al., 2022).
Notably, many studies did not specify the method of participant selection, while others intentionally chose their participants. For instance, Paul and Moreno-Perez (2019) recruited participants from a diabetes clinic and summer camp. Smith et al. (2021) randomly selected adolescents from a pediatric endocrinology clinic. Additionally, studies were identified that employed snowball sampling to select participants (Holtz et al., 2021). McAlpin et al. (2022) recruited participants based on a protocol involving informed consent from the relatives of adolescents, Geirhos et al. (2022) recruited participants through internet advertising, and Larsen et al. (2022) exclusively recruited adolescent Latinas who engaged in moderate to vigorous physical activity for at least 150 min per week.
Representativeness
Concerning the representativeness of the sample regarding dropouts in longitudinal studies, it was observed that in most of the studies, over 75% successfully completed the entire intervention (Holtz et al., 2021; Malik et al., 2021; Paul and Moreno-Perez, 2019; Smith et al., 2021; Weissberg-Benchell et al., 2020). Notably, in the study by Geirhos et al. (2022), only 60% completed the entire intervention. The challenges in completing interventions in most studies were often attributed to difficulties in accessing mobile phones, computers, and/or the internet, given that many interventions were online or involved new technologies. Additionally, there were instances of low engagement due to age-related factors or family circumstances of the adolescents (Holtz et al., 2021; Malik et al., 2021; McAlpin et al., 2022; Paul and Moreno-Perez, 2019; Smith et al., 2021; Weissberg-Benchell et al., 2020). It is noteworthy that financial compensation was offered in some studies to incentivize participants, leading to inconsistent performance with the interventions and some participants failing to complete them (Holtz et al., 2021; Malik et al., 2021).
Variables
Regarding the variables assessed in each of the studies, there was notable heterogeneity. Since all studies were related to T1D, hemoglobin emerged as a common medical variable measured across most studies (Holtz et al., 2021; Paul and Moreno-Perez, 2019; Smith et al., 2021; Weissberg-Benchell et al., 2020). Various other variables related to physical health were also examined, including glycemic control, quality of life associated with diabetes, and hemoglobin (Smith et al., 2021), competence in diabetes management skills (Holtz et al., 2021), ideas about diabetes prevention (McAlpin et al., 2022), and physical activity (Larsen et al., 2022). To measure these variables, different instruments were employed, such as internet-connected devices that measured blood glucose and insulin levels (Paul and Moreno-Perez, 2019), hemoglobin (HbA1c) (Holtz et al., 2021; Smith et al., 2021), the diabetes management skills questionnaire (Holtz et al., 2021), a physical activity questionnaire, and an accelerometer (Larsen et al., 2022).
Concerning the psychological variables and the central aspects of this study, factors such as motivation and self-efficacy in diabetes self-control were assessed using the Self-Efficacy for Diabetes Self-Management questionnaire (Paul and Moreno-Perez, 2019). The quality of life related to health was measured using both the generic PedsQL scale (Pediatric Quality of Life questionnaire) and informal interviews (Holtz et al., 2021; Larsen et al., 2022; Malik et al., 2021; Paul and Moreno-Perez, 2019; Smith et al., 2021). The presence of emotional disorders or depressive symptoms was also evaluated using instruments such as the depression questionnaire from the Center for Epidemiological Studies (CES-D) and the anxiety questionnaire of the Beck Anxiety Inventory (BAI), alongside self-report questionnaires and telephone interviews (Geirhos et al., 2022; Weissberg-Benchell et al., 2020).
Additional variables included problem-solving skills, gauged by the Adolescent Problem-Solving Skills Questionnaire (APSSQ) (Weissberg-Benchell, 2020); emotional and social needs, measured through semi-structured interviews and field notes (Patton et al., 2022); the effectiveness of interventions using internet-based cognitive behavioral therapy (CBT) (Geirhos et al., 2022); and social and environmental factors, knowledge, attitudes, beliefs, and behavioral influences impacting adolescent lifestyle behaviors associated with diabetes risk. Ideas regarding diabetes prevention and approaches to incorporating new mobile health technologies to enhance elements of goal setting, self-management, and peer support were explored through focus group discussions in the study by McAlpin et al. (2022). Additionally, the frequency and duration of participation and adherence to treatment were assessed through interviews, focus group discussions, and questionnaires such as the Diabetes Treatment Adherence Questionnaire (DTSQ) (Holtz et al., 2021; Smith et al., 2021).
Confounding factors
Considering potential confounding factors that may have influenced the results, it is worth noting that in certain studies, the actual impact of the intervention on the participants was not considered. Instead, the focus was solely on extracting information related to the targeted variables (e.g., the needs of adolescents with T1D and their parents or potential enhancements to intervention designs) (McAlpin et al., 2022; Patton et al., 2022). Other studies involved adolescents with both T1D and another chronic disease, alongside symptoms of anxiety and depression (Geirhos et al., 2022), introducing a potential factor that could alter or obscure the study results.
A cultural and social barrier was identified as a potential confounding factor in the study by Larsen et al. (2022), as the 200 participating adolescents were Latinas. In some studies, parents and/or relatives were also included, influencing the results of the study (Holtz et al., 2021; Patton et al., 2022). Lastly, it is essential to highlight that the focus of the present study is on interventions involving some form of new technology. Thus, a potential barrier or confounding factor in the studies could be adolescents who, for various reasons, lacked resources or easy access to using these new technologies, which could also impact the results.
Inclusion and exclusion criteria
Most of the studies specified their inclusion and exclusion criteria (Geirhos et al., 2022; Holtz et al., 2021; Larsen et al., 2022; Malik et al., 2021; Patton et al., 2022; Paul and Moreno-Perez, 2019; Smith et al., 2021; Weissberg-Benchell et al., 2020). A large part of the studies agreed on choosing the age of the participants as a criterion, which was approximately the age of adolescence and young adulthood, ranging from 12 to 21 years (Geirhos et al., 2022; Holtz et al., 2021; Larsen et al., 2022; Paul and Moreno-Perez, 2019; Smith et al., 2021; Weissberg-Benchell et al., 2020). Another central criterion was the diagnosis of T1D (Holtz et al., 2021; Malik et al., 2021; Paul and Moreno-Perez, 2019; Smith et al., 2021; Weissberg-Benchell et al., 2020). In addition, a significant criterion when including studies that deal with new technologies is that the participants had easy access to the internet (Paul and Moreno-Perez, 2019). Some studies added as a criterion the importance of the participants speaking English (Paul and Moreno-Perez, 2019). The article by McAlpin et al. (2022) included all adolescent patients if their relatives signed an informed consent. Finally, two studies included the presence of symptoms of anxiety or depression in the participants as a criterion (Geirhos et al., 2022).
Main results
This section presents the primary findings of this research, focusing on the effects of interventions incorporating new technologies in adolescents diagnosed with T1D. To achieve this, various key variables related to mental health and quality of life were selected to gain clearer insights into their impacts. Additionally, assessing the acceptability of these interventions and the adherence to the treatment they facilitate was deemed crucial.
Health-related quality of life
Many studies obtained significant results in terms of health-related quality of life, where they saw that an intervention based on new technologies significantly improved the health-related quality of life of patients, achieving a better relationship with health, disease and, consequently, a better overall quality of life (improvements at the social, family, work level, etc.) (Holtz et al., 2021; Larsen et al., 2022; Smith et al., 2021).
Psychopathology
Interventions using new technologies obtained promising results in terms of the psychopathology of patients, achieving a significant reduction in the incidence of emotional disorders and anxiety and depressive symptoms (Geirhos et al., 2022; Weissberg-Benchell et al., 2020). The results of improving critical thinking skills and managing emotions were also significant compared to before starting the intervention (Weissberg-Benchell et al., 2020).
Motivation, self-esteem, and self-efficacy
Regarding motivation, the study by Paul and Moreno-Perez 2019, obtained greater motivation and confidence when dealing with the management of T1D thanks to the Can-Do-Tude online intervention. This intervention, based on the motivational interview, was related to a positive effect at the time of managing hemoglobin levels. It improved participants’ physical health and consequently increased their self-esteem, self-efficacy, and mental health.
Acceptance of the use of new technologies
It was observed in a generalized way that the acceptance of the interventions that used new technologies was extremely high, and patients were more receptive to them than normative treatments (Geirhos et al., 2022; Holtz et al., 2021; Malik et al., 2021). Patients reported greater accessibility to these interventions thanks to new technologies (Holtz et al., 2021; McAlpin et al., 2022; Patton et al., 2022).
Adherence to treatment
Related to the accessibility and acceptance mentioned above, the interventions that used new technologies obtained high adherence to treatment, a higher percentage of patients completed the interventions, and the dropout rates fell (Holtz et al., 2021; Smith et al., 2021). Further, there was a greater duration and frequency of participation (Malik et al., 2021).
Quality assessment
Table 1 displays the scores assigned to each study based on its quality. As mentioned earlier, scores for each criterion and study ranged from 1 (strong) to 3 (weak). Evaluators SV and PM independently and blindly assigned scores for each criterion and study. The table illustrates the overall scores for selection bias, study design, confounders, blinding, data collection methods, and withdrawals or dropouts, derived from the mean of scores for each criterion. Subsequently, the differences between the scores of both evaluators were analyzed, and an agreement was easily reached since the variations were minimal and did not impact the overall scores of each study. With the final scores for each criterion determined, we proceeded to calculate the overall quality score of the study, as shown in the “Global” column of Table 2. Many studies received a score of 3, indicating weak quality (55.5%) (Holtz et al., 2021; Larsen et al., 2022; Malik et al., 2021; McAlpin et al., 2022; Paul and Moreno-Perez, 2019). Among all the studies, 22.2% earned a score of 1, signifying strong quality. The study conducted by Smith et al. (2021) was the sole study designated as moderate quality.
Data extraction
A comprehensive table was created to succinctly summarize the relevant results from the studies included in this research. The table is systematically organized based on key characteristics of the studies. The selected information for the table includes identification details (first author and year of publication), title, country of origin, sample details (including sample size, the health condition or disease of the population, presence of caregivers or relatives, and the age of participants), variables and instruments used, study design, results, and primary conclusions. Furthermore, an additional table was formulated to outline the quality assessment ratings, utilizing the “Study Quality Assessment Tool” as a guiding instrument (Thomas, 2003) (Table 2).
Discussion
The primary aim of this study was to evaluate the effectiveness of interventions utilizing new technologies in adolescents diagnosed with type 1 diabetes mellitus (T1D), with a specific emphasis on their impact on psychological well-being. Given the widespread prevalence of T1D among adolescents globally, effective disease management requires addressing both the physical and psychological needs of this population. In recent years, there has been exploration into the potential of new technologies in the realm of psychological interventions for adolescents with T1D. These technologies offer unique opportunities to enhance psychological care and support, serving as powerful tools to reach a substantial portion of the population rapidly and effectively. However, it is essential to acknowledge that they also bring forth challenges and limitations.
In the context of psychological aspects, the studies under review assessed variables such as treatment adherence, the most extensively studied variable, along with self-concept, self-esteem, quality of life, anxiety, depression, and stress. Together, these variables provided a comprehensive perspective on the psychological factors influencing disease management and suggested that interventions employing new technologies can bring about positive modifications. Nevertheless, it is crucial to recognize that the psychological variables scrutinized in these studies are not exhaustive. There is a need for further research encompassing a broader array of psychological variables to gain a more comprehensive understanding of the genuine effectiveness of these interventions.
In general, it is important to note that promising results were obtained in relation to the psychological variables studied. Some examples of these results include a psychological intervention using new technologies significantly improving the self-control of diabetes in adolescents with T1D (Paul and Moreno-Perez, 2019). Web interventions promoting problem-solving training were shown to prevent symptoms of depression, anxiety, and emotional distress (Geirhos et al., 2022; Weissberg-Benchell et al., 2020). The most significant and consistent result across most studies was the improvement in adherence to treatment (Holtz et al., 2021; Malik et al., 2021; McAlpin et al., 2022; Smith et al., 2021). This last result is particularly relevant and promising, as many studies agree that the design of an intervention using new technologies is more attractive to adolescents, who are familiar and accepting of technologies. These technologies also offer them convenience, making it easier for them to follow the treatment.
The studies mentioned earlier highlight that interventions of this nature often do not necessitate physical presence but can be conducted entirely online or in a blended format. This flexibility proves highly beneficial for individuals facing challenges in traveling for treatment or lacking motivation to do so, thereby enhancing participation. The widespread availability of new technologies and their accessibility (given that much of the global population possesses devices enabling internet connectivity) implies that such interventions will become increasingly prevalent in our lives. It is noteworthy to mention that since 2019, coinciding with the onset of the COVID-19 pandemic (Ramkissoon, 2021a, b, 2022), there has been a surge in the use of new technologies across various aspects of life, including work, education, and medical services. This trend extends to psychological interventions, as demonstrated in the systematic review, which incorporates updated studies originating during the pandemic.
Limitations
However, despite the promising possibilities offered by new technologies, it is essential to note that research on psychological interventions based on new technologies for adolescents with T1D is still very limited. A large majority of the studies obtained in the initial database search were excluded because, despite being psychological interventions for adolescents with T1D, they did not utilize new technologies, reflecting the novelty of this field. The studies meeting the criteria were scarce, and the majority exhibited a distinct lack of rigor, often featuring pilot or feasibility designs, highlighting the pressing need for more rigorous and large-scale investigations. This limitation was also evident when assessing the quality of the studies, with the majority being of weak quality (Holtz et al., 2021; Larsen et al., 2022; Malik et al., 2021; McAlpin et al., 2022; Paul and Moreno-Perez, 2019). Consequently, the absence of randomized controlled studies with control groups hampers our comprehensive understanding of the effectiveness of this type of intervention.
While new technologies offer accessibility and acceptance, they also pose challenges. One such challenge is the digital divide, which may exclude individuals lacking access to technologies or lacking the skills to benefit from these interventions. Additionally, interventions conducted on mobile applications or online platforms might be inadequate or fail to specifically address the unique problems faced by adolescents. Hence, it is crucial to consider cultural and socioeconomic diversity when developing new interventions to prevent exclusion and ensure that these tools are culturally sensitive.
Despite the mentioned limitations and lack of rigor, the reviewed studies present effective and promising results that underscore the importance of incorporating psychological interventions involving new technologies in the comprehensive management of T1D. This is why new technologies can become a key tool for monitoring treatment, providing emotional support, offering psychoeducation to adolescents and their families, managing T1D, and improving both physical and psychological symptoms.
Conclusions
In addressing future research, it is crucial to confront the limitations, and several key considerations can be outlined for the advancement and enhancement of these interventions. These include (1) Conducting Rigorous Research: Strive for more rigorous and high-quality research, emphasizing an increased number of randomized controlled studies and longitudinal follow-ups. (2) Personalizing Interventions: Adapt interventions with new technologies to the individual needs of adolescents. Personalize interventions based on factors such as autonomy level, age, gender, and individual needs, leveraging the capabilities of new technologies. (3) Integrating Platforms: Integrate different technologies and approaches across various platforms, including mobile devices, online platforms, monitors, etc. (4) Multidisciplinary Collaboration: Foster multidisciplinary collaboration among diverse professionals, involving both health professionals and technology experts, to support and optimize interventions based on new technologies. (5) User-Centered Approach: Strive for a user-centered approach that encompasses different systems (family, friends, school). Ensure the confidentiality and privacy of each user’s data. Considering these proposed enhancements and given the promising results thus far, it appears that new technologies are poised to play a pivotal role in the future of psychological interventions targeting adolescents with T1D.
Data availability
This study has not generated a dataset of data generated and/or analyzed, but for any request please contact the corresponding author.
References
Allen, B. & Waterman, H. (2019). Stages of adolescence. Healthy Children Pediatricians. Retrieved from https://www.healthychildren.org/English/ages-stages/teen/Pages/Stagesof-Adolescence.aspx. Accessed 7 Feb 2024
Bekele, B. T., Demie, T. G., & Worku, F. (2022). Health-related quality-of-Life and associated factors among children and adolescents with type 1 diabetes mellitus: A cross-sectional study. Pediatric Health, Medicine and Therapeutics, 13, 243–256. https://doi.org/10.2147/PHMT.S364454
Covidence systematic review software. (2018). Available Accesible from: http://www.covidence.org. Accessed 7 Feb 2024
Dantzer, C., Swendsen, J., Maurice-Tison, S., & Salamon, R. (2003). Anxiety and depression in juvenile diabetes: A critical review. Clinical Psychology Review, 23(6), 787–800. https://doi.org/10.1016/S0272-7358(03)00069-2
Espinoza, M. P. M., & Vega, M. G. (2023). Características de las intervenciones en diabetes tipo 1 de 2003 a 2021: Una revisión bibliográfica. Psicología y Salud, 33(1), 19–30. https://doi.org/10.25009/pys.v33i1.2769
Geirhos, A., Domhardt, M., Lunkenheimer, F., Temming, S., Holl, R. W., Minden, K., Warschburger, P., Meissner, T., Mueller-Stierlin, A. S., & Baumeister, H. (2022). Feasibility and potential efficacy of a guided internet- and mobile-based CBT for adolescents and young adults with chronic medical conditions and comorbid depression or anxiety symptoms (youthCOACHCD): A randomized controlled pilot trial. BMC Pediatrics, 22(1). https://doi.org/10.1186/s12887-022-03134-3
Glonti, K., Gordeev, V. S., Goryakin, Y., Reeves, A., Stuckler, D., Mckee, M., & Roberts, B. (2015). A systematic review on health resilience to economic crises. PLoS ONE, 10(4), e0123117. https://doi.org/10.1371/journal.pone.0123117
Gómez-Peralta, F., Menéndez, E., Conde, S., Conget, I., & Novials, A. (2021). Características clínicas y manejo de la diabetes tipo 1 en España. Estudio SED1. Endocrinología, Diabetes y Nutrición, 68(9), 642–653
Gómez Rico, I., Pérez Marín, M., & y Montoya Castilla, I. (2015). Diabetes mellitus tipo 1: Breve revisión de los principales factores psicológicos asociados. Anales De Pediatría, 82(1), e143–e146. https://doi.org/10.1016/j.anpedi.2014.04.003
Grey, M., Whittemore, R., Jeon, S., Murphy, K., Faulkner, M. S., & y Delamater, A. (2013). Internet psycho-education programs improve outcomes in youth with type 1 diabetes. Diabetes Care, 36(9), 2475–2482. https://doi.org/10.2337/dc12-2199
Holtz, B., Mitchell, K. M., Holmstrom, A. J., Cotten, S. R., Dunneback, J. K., Jimenez-Vega, J., Ellis, D. A., & Wood, M. A. (2021). An mhealth-based intervention for adolescents with type 1 diabetes and their parents: Pilot feasibility and efficacy single-arm study. JMIR MHealth and UHealth, 9(9). https://doi.org/10.2196/23916
Hong, K. M. C., Glick, B. A., Kamboj, M. K., & Hoffman, R. P. (2021). Glycemic control, depression, diabetes distress among adolescents with type 1 diabetes: Effects of sex, race, insurance, and obesity. Acta Diabetologica, 58(12), 1627–1635. https://doi.org/10.1007/s00592-021-01768-w
Jensen, M. V., Broadley, M., Speight, J., Chatwin, H., Scope, A., Cantrell, A., ... & Hypo‐RESOLVE consortium. (2022). The impact of hypoglycaemia in children and adolescents with type 1 diabetes on parental quality of life and related outcomes: A systematic review. Pediatric Diabetes, 23(3), 390–405. https://doi.org/10.1111/pedi.13308
Kamody, R. C., Berlin, K. S., Rybak, T. M., Klages, K. L., Banks, G. G., Ali, J. S., Alemzadeh, R., Ferry, R. J., Jr., & Diaz Thomas, A. M. (2018). Psychological Flexibility Among Youth with Type 1 Diabetes: Relating Patterns of Acceptance, Adherence, and Stress to Adaptation. Behavioral Medicine, 44(4), 271–279. https://doi.org/10.1080/08964289.2017.1297290
Katz, J., Rosenbloom, B. N., y Fashler, S. (2015). Chronic Pain, Psychopathology, and DSM 5 Somatic Symptom Disorder. The Canadian Journal of Psychiatry, 60(4), 160–167.https://doi.org/10.1177/070674371506000402
Kitsiou, S., Paré, G., Jaana, M., & Gerber, B. (2017). Effectiveness of mHealth interventions for patients with diabetes: An overview of systematic reviews. PLoS ONE, 12(3), e0173160. https://doi.org/10.1371/journal.pone.0173160
Korey K. Hood, Samantha Huestis, Allison Maher, Debbie Butler, Lisa Volkening, Lori MB Laffel; Síntomas depresivos en niños y adolescentes con diabetes tipo 1: Asociación con características específicas de la diabetes. Diabetes Care 1 de junio de 2006; 29(6), 1389. https://doi.org/10.2337/dc06-0087
Lacomba-Trejo, L., Valero-Moreno, S., & Montoya-Castilla, I. (2019). Adolescente con Diabetes Mellitus Tipo 1: problemas emocionales, conductuales y de autoestima. Revista de Psicología de la Salud, 7(1), 22–44. https://doi.org/10.21134/pssa.v7i1.876
Larsen, B., Greenstadt, E., Olesen, B., Osuna, L., Godino, J., Marcus, B., Dunsiger, S., Meyer, D., & Zive, M. (2022). A multiple technology-based physical activity intervention for Latina adolescents in the USA: Randomized controlled trial study protocol for Chicas Fuertes. Trials, 23(1). https://doi.org/10.1186/s13063-022-06105-2
Lazo, C., & Durán-Agüero, S. (2019). Efecto del diagnóstico de la diabetes mellitus y su complicación con los trastornos de la conducta alimentaria. Revista Chilena De Nutrición, 46(3), 352–360. https://doi.org/10.4067/S0717-75182019000300352
Malik, F. S., Lind, C., Duncan, S., Mitrovich, C., Pascual, M., & Yi-Frazier, J. P. (2021). Augmenting Traditional Support Groups for Adolescents with Type 1 Diabetes Using Instagram: Mixed Methods Feasibility Study. JMIR Diabetes, 6(4). https://doi.org/10.2196/21405.
McAlpin, N., Elaiho, C. R., Khan, F., Cruceta, C., Goytia, C., & Vangeepuram, N. (2022). Use of Focus Groups to Inform a New Community-Based Youth Diabetes Prevention Program. International Journal of Environmental Research and Public Health, 19(15). https://doi.org/10.3390/ijerph19159655
Montali, L., Zulato, E., Cornara, M., Ausili, D., & Luciani, M. (2022). Barriers and facilitators of type 1 diabetes self-care in adolescents and young adults. Journal of Pediatric Nursing, 62, 136–143. https://doi.org/10.1016/j.pedn.2021.09.014
Neves, C., Neves, J. S., Oliveira, S. C., Oliveira, A., & Carvalho, D. (2017). Diabetes Mellitus Tipo 1. Revista Portuguesa De Diabetes, 12(4), 159–167.
Newton, K. T., & Ashley, A. (2013). Pilot study of a web-based intervention for adolescents with type 1 diabetes. Journal of Telemedicine and Telecare, 19(8), 443–449. https://doi.org/10.1177/1357633X13512069
Organización Mundial de la Salud. (2016). Informe mundial sobre la diabetes: resumen de orientación. Organización Mundial de la Salud. Recuperado de: https://apps.who.int/iris/handle/10665/204877. Accessed 7 Feb 2024
Organización Mundial de la Salud. (2021). Diabetes. Recuperado de: https://www.who.int/es/news-room/fact-sheets/detail/diabetes. Accessed 7 Feb 2024
Ouzouni, A., Galli-Tsinopoulou, A., Kyriakos kazakos, M. D., & Maria Lavdaniti, R. N. (2019). Adolescents with diabetes type 1: Psychological and behavioral problems and compliance with treatment. International Journal of Caring Sciences, 12(2), 1-7.
Páez, J. A., Triana, J. D., Ruiz, M. A., Masmela, K. M., Parada, Y. A., Peña, C. A., Perdomo, C. M., Quintanilla, R. A., Ramírez, A. F., y Villamil, E. S. (2016). Complicaciones crónicas de la diabetes mellitus: visión práctica para el médico de atención primaria. Revista Cuarzo, 22(1), 13–38. https://doi.org/10.26752/cuarzo.v22.n1.144
Papalia, D. E., & Martorell, G. (2017). Desarrollo humano (13.ª ed.). McGraw Hill.
Patton, S. R., Maahs, D., Prahalad, P., & Clements, M. A. (2022). Psychosocial Needs for Newly Diagnosed Youth with Type 1 Diabetes and Their Families. Current Diabetes Reports, 22, 385–392. https://doi.org/10.1007/s11892-022-01479-8
Paul, L. & Moreno-Perez, A. (2019). Beta Testing Can-Do-Tude: An Online Intervention Using the Principles of Motivational Interviewing for Adolescents with Type 1 Diabetes. Online Journal of Nursing Informatics (OJNI), 23(1). Available at http://www.himss.org/ojni. Accessed 7 Feb 2024
Pérez-Marín, M., Gómez-Rico, I., & Montoya-Castilla, I. (2015). Type 1 Diabetes Mellitus: Psychosocial factors and adjustment of pediatric patient and his/her family. Review. Archivos Argentinos De Pediatría, 113(2), 158–162. https://doi.org/10.5546/aap.2015.158
Ramkissoon, H. (2021a). Place affect interventions during and after the COVID-19 pandemic. Frontiers in Psychology, 12, 726685. https://doi.org/10.3389/fpsyg.2021.726685
Ramkissoon, H. (2021b). Body-mind medicine interventions in COVID-19 place confinement for mental, physical, and spiritual wellbeing. OBM Integrative and Complementary Medicine, 6(2), 1–17.
Ramkissoon, H. (2022). COVID-19 adaptive interventions: Implications for wellbeing and quality-of-life. Frontiers in Psychology, 13, 810951. https://doi.org/10.3389/fpsyg.2022.810951
Rechenberg, K., Whittemore, R., Holland, M., & Grey, M. (2017). General and diabetes specific stress in adolescents with type 1 diabetes. Diabetes Research and Clinical Practice, 130, 1–8. https://doi.org/10.1016/j.diabres.2017.05.003
Shamseer, L., Moher, D., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., & Stewart, L. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P): Elaboration and explanation. BMJ, 349(7647), 1–25. https://doi.org/10.1136/bmj.g7647
Smith, M. B., Albanese-O’Neill, A., Yao, Y., Wilkie, D. J., Haller, M. J., & Keenan, G. M. (2021). Feasibility of the web-based intervention designed to educate and improve adherence through learning to use continuous glucose monitor (IDEAL CGM) training and follow-up support intervention: Randomized controlled pilot study. JMIR Diabetes, 6(1). https://doi.org/10.2196/15410
Souza, M. A. D., Freitas, R. W. J. F. D., Lima, L. S. D., Santos, M. A. D., Zanetti, M. L., & Damasceno, M. M. C. (2019). Calidad de vida relacionada con la salud de los adolescentes con diabetes mellitus tipo 1. Revista Latinoamericana de Enfermagem, 27. 441–458. https://doi.org/10.22289/2446-922X.V8N1A26
Stroup, D. F., Berlin, J. A., Morton, S. C, Olkin, I., Williamson, G. D., Rennie, D.,... Thacker, S. B. (2000). Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA, 283(15), 2008–2012.https://doi.org/10.1001/jama.283.15.2008
Thomas, H. (2003). Quality assessment tool for quantitative studies. Effective Public Health Practice Project. BMJ Publishing Group.
Valverde-Merino, M. I. (2018). Adherencia terapéutica: factores modificadores y estrategias de mejora. Ars Pharmaceutica (Internet), 59(4), 251–258. https://doi.org/10.30827/ars.v59i4.7357
Weissberg-Benchell, J., Shapiro, J. B., Bryant, F. B., & Hood, K. K. (2020). Supporting Teen Problem-Solving (STEPS) 3-year outcomes: Previniendo la angustiaemocional específica de la diabetes y los síntomas depresivos en adolescentes con diabetes tipo 1. Journal of Consulting and Clinical Psychology, 88(11), 1019–1031. https://doi.org/10.1037/ccp0000608
Whittemore, R., Jaser, S., Guo, J., & Grey, M. (2010). A conceptual model of childhood adaptation to type 1 diabetes. Nursing Outlook, 58(5), 242–251. https://doi.org/10.1016/j.outlook.2010.05.001
Whittemore, R., Jaser, S.S., Jeon, S., Liberti, L., Delamater, A., Murphy, K. y Grey, M. (2012). An internet coping skills training program for youth with type I diabetes. Six-month outcomes. Nursing Research, 61(6), 395-404.https://doi.org/10.1097/NNR.0b013e3182690a29
Winkley, K., Upsher, R., Stahl, D., Pollard, D., Brennan, A., Heller, S., & Ismail, K. (2020). Systematic review and meta-analysis of randomized controlled trials of psychological interventions to improve glycaemic control in children and adults with type 1 diabetes. Diabetic Medicine, 37(5), 735–746. https://doi.org/10.1111/dme.14264
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval (include appropriate approvals or waivers)
Because this is a systematic review, we relied on those who conducted the studies reviewed here to follow the 1964 Declaration of Helsinki and its later addenda.
Consent to participate
Because this is a systematic review, we relied on those who conducted the studies we reviewed to obtain informed consent.
Consent for publication
Not applicable.
Conflict of interest
The authors have no conflict of interest. Funding: Funded by the European Union - NextGenerationEU. Public aid for strategic projects aimed at the ecological transition and the digital transition, from the State Plan for Scientific, Technical and Innovation Research for the period 2021-2023, within the framework of the Recovery, Transformation and Resilience Plan. Aid granted by the Government of Spain, Ministry of Science, Innovation and Universities, State Research Agency (TED2021-131070B-C21).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Morales, P., Valero-Moreno, S. & Pérez-Marín, M. New technologies in psychological intervention for adolescents with type I diabetes: a systematic review. Curr Psychol 43, 17577–17592 (2024). https://doi.org/10.1007/s12144-024-05694-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-024-05694-2