
Abstract
The primary aim of this paper was to understand expressed emotion (EE) and its relationship to wellbeing in South Asians (SAs) living in the UK. A total of 529 participants of South Asian heritage were recruited from the UK and completed an online survey consisting of the family questionnaire, the level of expressed emotion scale (LEE), warmth measure, the hospital anxiety and depression scale. Components of EE and wellbeing were investigated using network analysis. Overall, the participants were classified as low EE for criticism, but high for emotional overinvolvement. They scored relatively high on the warmth scale. LEE scores were in the middle range. The network analysis revealed unique associations between EE subscales and symptoms of depression and anxiety, and highlighted positive aspects of EE. The network analysis also highlighted differences in EE between parents and partner. The findings provide an overview of the interactions and influence of EE variables within this population. Future research should focus on the differences between SA ethnicities and religions; differentiating between intrusive and non-intrusive involvement may help further explain part of the variance between variables; exploring first and second-generation immigrants would help discover the impact of acculturation and intergenerational trauma on EE.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Expressed emotion (EE) is defined as a measure of the family environment and emotional climate surrounding a caregiver’s attitude and behaviours, towards an individual. Traditionally, EE consists of five dimensions of interpersonal relationships: warmth, positive remarks, critical comments (CC), hostility and emotional over-involvement (EOI).
The construct of EE varies across cultures (Lopez et al., 2009). There is an inconsistent relationship between high emotional over-involvement and illness outcome, and emotional over-involvement may not be detrimental in all cultures (Singh et al., 2013). It has also been proposed that EOI is normative in some parts of India (Bhugra & McKenzie, 2003) where n individual who is not emotionally overinvolved would be considered as lacking in providing care. Additionally, in many cultures, speaking loudly is considered the norm but can be interpreted as an indicator of high EE. This could possibly be due to moderating effects of other EE constructs such as warmth and high mutual interdependence in kin relationships (Singh et al., 2013).
Collectivist and Eastern cultures have depicted lower levels of EE, such as rural India: 8%, Mexican Americans: 38% than Western and individualistic cultures such as UK: 45% and Anglo-Americans: 67% (Singh et al., 2013). Religion has been suggested as a contributing factor to these variations (Hashemi & Cochrane, 1999). Criticism has been shown to be higher in Pakistani than White families (Hashemi & Cochrane, 1999). Family criticism in Pakistan has been associated with: gender criticism, and religious and cultural aspect of criticism, while a cultural conceptualisation of EOI has been associated with self-sacrificing and overprotective behaviour (Akhtar et al., 2013). Critical comments are made more often when individuals deviate from the religious, social, and cultural traditions, such as not offering prayers, disobeying and disrespecting elders, and negligent attitudes towards health and personal hygiene. Women were also more likely to exhibit self-sacrificing behaviours such as selling valuable personal items and sacrificing their own pleasures. Large variation in EOI scores was accounted for by the sacrificing behaviours subscale. Whereas over-protection for girls was significantly higher than for males, by chaperoning them to public places and other cities.
Expressed emotion exists in both clinical and non-clinical populations (Hibbs et al., 1991). Studies of EE in families of healthy controls and in other populations are needed to further refine our understanding of the meaning and generalizability of the Expressed Emotion construct (Koenigsberg et al., 1995). Previous research has highlighted the need to establish a culturally normative understanding of EE (Bhugra & McKenzie, 2003; Hashemi & Cochrane, 1999) to accurately detect significantly high levels of EE requiring intervention. Researchers also call for examining positive EE (Singh et al., 2013). This study addresses a gap in literature, by exploring domains of EE and their relationship to depression and anxiety in South Asian populations living in the UK. To study this multifaceted concept of EE, a network analysis of the sub-constructs was conducted to estimate the interconnectedness of domains of EE and depression and anxiety. A network is any system that represents nodes (observed variables), that are connected by edges (associations) (Epskamp et al., 2018). Network analysis characterized the direct and indirect associations between variables and can inform hypotheses about potential causal pathways (Epskamp & Fried, 2018). Accommodating the unique role of each EE domain, can reveal the nuances through a cultural lens preventing pathologizing of emotions in these cultures (O'Driscoll et al., 2019).
Aims of the study
The primary aim was to describe the relationship between EE and depression and anxiety within SAs living in the UK. The nine subscales investigated were EOI, criticism, intrusiveness, emotional responsiveness, attitude towards illness, tolerance and expectations, warmth, anxiety, and depression.
Methods
Design
A cross-sectional, online survey was used. The study was approved by the Yorkshire and The Humber – South Yorkshire Research Ethics Committee (IRAS: 230,098).
Participants
A total of 529 responses were analysed. Participants were eligible for the study if they were: 1) living in the United Kingdom, 2) 18 years or older, 3) self-identifying as being of SA heritage i.e., from Afghanistan, Bangladesh, Bhutan, India, Nepal, Maldives, Pakistan, Sri Lanka, 4) had a significant person to answer the survey about, e.g., child, partner, sibling, friend. They were also required to have adequate English language skills to understand the information and questions in the survey.
Participants were recruited in 2022, via opportunity and snowball sampling. UK universities were contacted and asked to circulate the study’s email invitations to students and staff. The study was advertised on social media platforms such as Instagram. South Asian societies and religious societies were also contacted.
Materials and procedure
Sociodemographic questionnaire
Participants completed a sociodemographic measure capturing age, gender, ethnicity, religious orientation, country of birth and time spent in the UK. Then, they were asked to think of an individual they felt close to, e.g., a parent or their partner and answered 5 questions pertaining to the participant's chosen person. The questions included the participant’s relationship to the chosen person, if the person had any significant physical and MHIs, where significant referred to impacting one’s level of functioning and/or requiring additional care, treatment.
The family questionnaire
The Family questionnaire (FQ) is a 20-item scale (Wiedemann et al., 2002) that describes the relationship of the participant with the individual of close relationship, and the frequency of EE which aims to capture the way the participant acts toward the significant individual. This self-report scale consists of 2 subscales which assess the frequency of criticism (α = 0.99) and EOI (α = 0.99), with 10 items each. The cut-off values for high criticism and high EOI are 23 and 27 respectively. It has shown high levels of test–retest reliability, wherein correlation coefficients were r = 0.84 for the criticism subscale and r = 0.91 for the EOI subscale. It also correlated significantly with the Camberwell Family Interview ratings, which is considered the gold standard for measuring EE in research and has high sensitivity and moderate-to-high specificity (Wiedemann et al., 2002).
Level of expressed emotion
The Level of Expressed Emotion (LEE) provides an index of the perceived emotional environment in a person’s influential relationships (Cole & Kazarian, 1988). The 60 items assess four characteristic attitudes of significant others (Vaughn & Leff, 1981): 1) Intrusiveness; the recurrent efforts to either offer unwelcomed advice, which is usually critical in nature, or to establish contact, 2) Emotional response; the response to one’s illness, e.g., reacting angrily or feeling distressed about the one’s illness, which in turn feeds back into the poor health of the person 3) Attitude toward illness; the negative and detrimental attitudes towards the one’s illness e.g., blaming the individual for the illness, assuming the person has control over symptoms, and 4) Tolerance and expectations; whether the individual is intolerant of the levels of disturbing behaviour and impairments of the person (Cole & Kazarian, 1988). Each of these 4 subscales consists of 15 items. LEE scale has sound psychometric properties of internal consistency; reliability; independent from sex, age, and construct validity (test–retest reliability: 0.82, and criterion validity: 0.86) (Cole & Kazarian, 1988).
Warmth
This scale was created by the researchers to specifically capture warmth. It consists of 5 items, influenced by The Family Attitudes Scale (Kavanagh et al., 1997), the Caregiving Relationship Questionnaire (Smith, 2013) and the Camberwell Family Interview (Vaughn & Leff, 1976). Each item is rated on a 4-point Likert scale (“Never/very rarely” = 1 to “Very often” = 4). Items include: “I am warm towards them”; “I appreciate what they do for me”; “I really value them”; “I want to understand how they see things”; “I feel very close to them”. Higher scores indicated higher levels of warmth in relationships. A pilot study to establish construct validity was run for this measure on a sample of participants who self-identify as SA and were asked for their opinions on what the scale was assessing. 40% answered “warmth” and other responses included “love”, “closeness” and “compassion”. Within this sample the confirmatory factor analysis of a single factor model showed good fit: loadings > 0.81, [RMSEA = 0.045 (90% CIs: 0 to 0.084); CFI = 1; TLI = 1], McDonald’s ω = 0.892.
Hospital anxiety and depression scale
The Hospital Anxiety and Depression scale (HADS) (Zigmond & Snaith, 1983) is a valid and reliable measure to screen for clinically significant levels of depression and anxiety. This 14-item self-assessment scale measures the severity of the disorders. Scores are calculated separately for depression and anxiety where 0–7 is normal, 8–10 is borderline abnormal/borderline case, 11–21 is abnormal.
Statistical analysis
All analysis was conducted using R (version 4.2.1) (Team, 2017).
A network of the nine subscales was estimated for the whole sample. Network differences between carers who were parents and partners were also estimated.
Within a network, nodes represent subscale scores. The weighted edges reveal the strength of the partial correlations between the nodes, these are visualised through the width and saturation of the edges in the network. Red lines denote negative associations, and blue lines positive associations. The edges in the network represent conditional independence relationships (the associations controlling for the effect of all other nodes). Edges are undirected, reflecting a bidirectional relationship.
Data was assessed to ensure it met assumptions for network analysis (Jones, 2022). Unequal variance was addressed through non-paranormal transformation. We assessed for collinearity and to remove redundant nodes; no reductions were suggested (goldbricker function).
The network modelling approach taken followed an Extended Bayesian Information Criterion (EBIC) least absolute shrinkage and selection operator (LASSO) procedure, implemented within a single Gaussian graphical model (Epskamp et al., 2017). The tuning parameter regularizes the estimated partial correlations network, minimizing model prediction error. The accuracy of edges and stability estimates for the network were calculated using a bootstrapping procedure (1000 iterations) (Epskamp & Fried, 2018).
Strength centrality (the sum of all the absolute edge weights connected to a node) was also estimated (Epskamp et al., 2018). The stability of the strength centrality metric was assessed using the correlation stability (CS) coefficient. This tests the highest number of cases that can be excluded to maintain a correlation of 0.7 between the original centrality indices and the centrality indices from a subset of the data. The CS-coefficient value should be great than 0.5 (Epskamp et al., 2018).
Results
Data, code, and supplementary figures are openly available in a repository: https://osf.io/c9va7/.
Sociodemographic and descriptive statistics
The sample consisted of 529 participants, with a mean age of 29.37 (6.93) years (See Table 1). The average number of years spent living in the UK was 9.63 (7.95). Slightly over half of the sample were females (53.1%), and almost a third of the participants were born in the UK. Majority of the participants belonged to an Afghani ethnic background (n = 137). 29% participants said they followed no religion, 27% described themselves as Christian and 25% as Muslim.
180 participants chose their partner as a person of close relationship. 66 of them had physical health issues such as diabetes and arthritis and 37 individuals had mental health difficulties, including depression, anxiety, and ADHD (Table 2). The mean scores and standard deviations for the subscales and total scores are reported in Table 3.
Network analysis
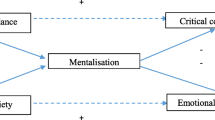
Th network is visualized in Fig. 1. Edge weight, centrality difference, and stability plots are included in the open access repository.

Estimated network structure of the EE domains and anxiety and depression. The blue lines represent positive associations, and the red lines represent negative associations. The thickness denotes the strength of the edge. Thicker edges denote stronger associations. EOI—Emotional over-involvement. Nodes are coloured to reflect shared measures
Results show positive edges between EOI and FQ Criticism, significantly stronger than other edges in the network; followed by the association between Anxiety and Depression. Tolerance & expectations was strongly associated with Emotional responsiveness, Attitudes towards illness, and Intrusiveness. Warmth was strongly associated with Attitudes towards illness and Tolerance & expectations (significantly stronger than all but 5 other edges).
Depression was positively associated with Attitudes towards illness, and Emotional responsiveness and to a lesser degree EOI, and negatively associated with Warmth. While Anxiety was positively associated with EOI, Emotional responsiveness and Criticism, it was negatively associated with Attitude towards illness.
Strength centrality estimates were found to be stable (CS-coefficient = 0.75). There were no significant differences in centrality between most variables. Intrusiveness had lowest centrality and was significantly different to all variables apart from anxiety. The bootstrapped CIs were generally small and there was less overlap between the CI of the variables indicating stability of estimates.
Network comparison
The network for carers who were partners was compared to the network for parents. Comparison between the two groups were performed using the Network Comparison Test package (NCT; Van Borkulo et al., 2022). Based on 1000 permutations, we investigated network invariance (possible edge weight differences) and global strength invariance (possible difference on the absolute sum of network edge weights). From NCT analyses, we observed that networks were different in both strength (S = 0.763 with p = 0.0.027) and edges (M = 0.339, p = 0.003). Networks were estimated in subgroups and therefore edge weight estimates will be less reliable than in the overall network.
There were edge differences between the networks. Attitude towards illness and tolerance and expectations (absolute difference: 0.339, p < 0.001) where the edge was stronger in the parental network. A negative edge between EOI and tolerance and expectations (absolute difference: 0.154, p = 0.036) was only present in the parent network. Criticism and emotional responsiveness (absolute difference: 0.155644, p = 0.043) was only present in parental network. EOI and tolerance and expectations (absolute difference: 0.1240885, p = 0.018) where the edge was negative in the parental network and positive in the partner network and warmth and anxiety (absolute difference: 0.167, p = 0.036) where the edge was positive in the parental network and negative in the partner network.
There was also significant difference in strength centrality, with emotional responsiveness (p = 0.018) and anxiety (p = 0.023) less strongly connected in the partner network.
Discussion
The primary aim was to describe the relationship between EE and wellbeing indexed by depression and anxiety within SAs living in the UK. Overall, the participants were classified as low EE for FQ criticism, but high for EOI levels. They scored relatively high on the warmth scale. LEE scores were in the middle range. The network analysis revealed unique associations between EE and symptoms of depression and anxiety, and highlighted positive aspects of EE, which need to be interpreted within a cultural frame. The network analysis also highlighted differences in EE towards parents and partner.
Depression was positively associated with attitudes towards illness and emotional responsiveness and to a lesser degree EOI and was negatively associated with warmth. Items within the attitude towards illness and emotional responsiveness subscale represent a lack of emotional response including a lack of empathy and containment and criticism (Hale et al., 2007). For example, I calm him/her down when he/she is upset; I blame him/her for things not going well; I get angry with him/her for no reason; I make matters worse when things aren't going well; I get irritated when things don’t go right (emotional responsiveness); I say he/she just wants attention when he/she says he/she is not well; I don’t help him/her when he/she is upset or feeling unwell; I say he/she causes his/her troubles to occur in order to get back at me; I accuse him/her of exaggerating when he/she says he/she is unwell (attitude towards illness) (Cole & Kazarian, 1988). Unsurprisingly higher levels of depression result in a lack of emotional response and higher levels of criticism. Anxiety was positively associated with EOI, emotional responsiveness and criticism and negatively associated with attitude towards illness. This is consistent with studies showing higher levels of EOI particularly in a Pakistani sample suggesting that Pakistani families may generally have intense emotional interactions regardless of whether they are facing obvious stressors; aspects like higher EOI in these families may be indicative of cultural rather than pathological traits (Hashemi & Cochrane, 1999; Ikram et al., 2011).
Interestingly warmth was positively correlated with EOI and intrusiveness. Unsurprisingly warmth was negatively correlated with depression emotional responsiveness, tolerance and expectations, attitude towards illness, and criticism. Within the EOI and intrusiveness subscales there is overlap between warmth and expression of concern and love that might be consistent with cultural norms. Items from EOI such as “I tend to neglect myself because of him/her”; “I regard my own needs as less important”; “he/she is an important part of my life”; “I have given up important things in order to be able to help him/her” (Wiedemann et al., 2002), are indicative of self-sacrificing behaviours often observed in SA cultures (Browning, 2017; Ramanathan et al., 2023; Sharif et al., 2022; Shariff, 2009). Similarly, items from the intrusiveness subscale such as “insists on knowing where I’m going”; “often checks up on me to see what I am doing”, might be indicative of culturally appropriate behaviours in particular within parent child relationships and indicate an acceptable level of care and therefore may not be perceived as intrusive (Sharif et al., 2022). Findings indicated a direct association between EOI and intrusiveness although surprisingly this did not appear to be very strong. However, the differentiation between intrusive involvement and non-intrusive involvement has not been researched in detail (O'Driscoll et al., 2019). Intrusive involvement is defined as manipulative ways to exert your influence over another person (McCarty et al., 2004). EOI is about violating interpersonal boundaries and maintaining a balance between being close to the person and allowing them to be independent, even in collectivistic cultures (Singh et al., 2013). It could be that the violation of these boundaries is the norm in some of the SA ethnicities. For example Indian and Pakistani mothers in London have been found to show higher levels of protectiveness and supervision compared to Indians (Iqbal & Golombok, 2018). The absence of warmth may be more harmful than the presence of criticism in collectivistic cultures, and EOI and warmth are hard to tease apart (Singh et al., 2013). Furthermore, the negative association between warmth and attitude towards illness and tolerance and expectations shows that the expression of irritability and criticism is more concerning than the presence of EOI in this sample.
Attitude toward illness (criticism) and tolerance and expectations (irritability) (Hale et al., 2007) were stronger in the parental network in comparison to the partner network. The parent network also showed a negative association between EOI and tolerance and expectations, whereas this was positive within the partner network. Emotional responsiveness and anxiety were much less strongly connected in the partner network. These findings might be explained by intergenerational trauma which is higher in migrant groups and is often transmitted by diminished parental emotional availability, dysfunctional communication styles and overinvolvement (Flanagan et al., 2020) resulting in lower levels of empathy, criticism and irritability. Furthermore the emphasis on collectivist values within SAs can create a burden of high expectations and family pressure and the community will try to hide problems from friends and family in order to avoid cultural shame and stigma (Ramanathan et al., 2023; Sharif et al., 2022). Given that a high proportion of the sample were from Afghanistan and Pakistan, these are regions that value high level of resilience at the cost of displaying empathy (Niazi, 2019; Rogers, 2021).
Differences within the parent and partner network may also be explained by processes such as acculturation and intergenerational differences. Navigating bicultural identities in particular within second-generation migrant groups leads to compromise and negotiating and accepting differences that have an impact on expression of emotion within the South Asian diaspora in the UK (Sharif et al., 2022). Thus, the positive association between EOI and tolerance and expectations within the partner network might be due to a more Westernized conceptualization of EOI as intrusive and interfering so unsurprisingly this is likely to be related to criticism.
Strengths and limitations
This study addresses a gap in the literature by investigating domains of EE with anxiety and depression in a diverse sample of SA participants living in the UK. The network analysis revealed important partial correlations between the nodes. While hypotheses can be drawn from the study around mediation pathways and causal pathways, these would need to be tested within a longitudinal study. It also puts into perspective how processes such as migration, parenting styles, acculturation play a large role in EE and how cultural, religious, and societal values and expectations also contribute significantly.
One of the main limitations of the study is the heterogeneity of the sample and influencing factors. Participants reported coming from several different SA ethnicities, religions, born in different countries, and most likely of different generations. There are significant differences between people of different SA ethnicities, religions and immigrant generations, and the influence of all these factors needs consideration (Akhtar et al., 2013; Hashemi & Cochrane, 1999). This highlights the importance of looking separately at SA cultures where some of them may be more heavily influenced by religious values. Future studies should employ study designs and methods of recruitment to ensure the high representativeness of the sample collected. The small number of participants in each ethnic group did not allow us to carry out a sub-group analysis, which would have provided a baseline measure for each ethnicity to better understand culturally appropriate EE in SAs.
This study considered an oft-neglected domain of EE, warmth, by developing and including a measure of the construct. It could be argued that the small number of items may contribute to the lack of variance in responses. However, in a construct that is unambiguous or narrow in scope, single or low-item measures should not be considered invalid and there has been a recent push for low-item measures in psychological science (Allen et al., 2022). Within this sample the confirmatory factor analysis of a single factor model showed good fit and the association between warmth and other subscales indicate construct validity. Nonetheless, the measure needs to be validated in a larger sample.
Directions for future research
Differentiating between intrusive and non-intrusive involvement may help further explain part of the variance between variables. Additionally, investigating the differences in EE between religions and constituents of SA ethnicities, e.g., Pakistan and India, and focus on the under-research SA countries such as Sri Lanka. Exploring first and second-generation immigrants would help discover the impact of acculturation and intergenerational trauma on EE.
Implications and conclusion
This study provides insight into a vastly complex structure of EE and its relationship to wellbeing in the South Asian population living in the UK. In particular, the need to differentiate between intrusive and non-intrusive emotional overinvolvement is crucial and understanding cultural influences and the presence and influence of warmth on other EE dimensions. The findings support the notion that the absence of warmth might be more problematic than the presence of criticism and intrusive involvement in South Asian cohorts. Also, recognising that intense emotional interactions consistent with EOI, might be cultural rather than pathogenic traits and perceived EE is therefore a better measure of distress. Whilst the cross-cultural inconsistency of EE is well documented, the underlying mechanisms, cultural influences and other processes such as acculturation, resulting in differences between Western and South Asian populations remain to be better understood.
Data availability
Study materials and data are also available upon request.
References
Akhtar, N., Suhail, K., Rana, S. A., & Singh, S. P. (2013). Development of culturally-specific family criticism scale and emotional over-involvement scale. Pakistan Journal of Psychological Research, 199–126. Retrieved from https://www.proquest.com/scholarly-journals/development-culturally-specific-family-criticism/docview/1524245031/se-2
Allen, M. S., Iliescu, D., & Greiff, S. (2022). Single item measures in psychological science: A call to action. European Journal of Psychological Assessment, 38(1), 1–5. https://doi.org/10.1027/1015-5759/a000699
Bhugra, D., & McKenzie, K. (2003). Expressed emotion across cultures. Advances in Psychiatric Treatment, 9(5), 342–348. https://doi.org/10.1192/apt.9.5.342
Browning, M. A. (2017). Self-sacrifice vs. collectivism: Examining construct overlap with Asian-Americans. Alliant International University.
Cole, J. D., & Kazarian, S. S. (1988). The level of expressed emotion scale: A new measure of expressed emotion. Journal of Clinical Psychology, 44(3), 392–397. https://doi.org/10.1002/1097-4679(198805)44:3%3c392::aid-jclp2270440313%3e3.0.co;2-3
Epskamp, S., & Fried, E. I. (2018). A tutorial on regularized partial correlation networks. Psychological Methods, 23(4), 617–634. https://doi.org/10.1037/met0000167
Epskamp, S., Borsboom, D., & Fried, E. I. (2017). Estimating psychological networks and their accuracy: a tutorial paper. Behavior Research Methods. https://doi.org/10.3758/s13428-017-0862-1
Epskamp, S., Borsboom, D., & Fried, E. I. (2018). Estimating psychological networks and their accuracy: A tutorial paper. Behavior Research Methods, 50(1), 195–212. https://doi.org/10.3758/s13428-017-0862-1
Flanagan, N., Travers, A., Vallieres, F., Hansen, M., Halpin, R., Sheaf, G., Rottmann, N., & Johnsen, A. T. (2020). Crossing borders: A systematic review identifying potential mechanisms of intergenerational trauma transmission in asylum-seeking and refugee families. European Journal of Psychotraumatology, 11(1), 1790283. https://doi.org/10.1080/20008198.2020.1790283
Hale, W. W., 3rd., Raaijmakers, Q. A., Gerlsma, C., & Meeus, W. (2007). Does the level of expressed emotion (LEE) questionnaire have the same factor structure for adolescents as it has for adults? Social Psychiatry and Psychiatric Epidemiology, 42(3), 215–220. https://doi.org/10.1007/s00127-006-0145-0
Hashemi, A. H., & Cochrane, R. (1999). Expressed emotion and schizophrenia: A review of studies across cultures. International Review of Psychiatry, 11(2–3), 219–224. https://doi.org/10.1080/09540269974401
Hibbs, E. D., Hamburger, S. D., Lenane, M., Rapoport, J. L., Kruesi, M. J., Keysor, C. S., & Goldstein, M. J. (1991). Determinants of expressed emotion in families of disturbed and normal children. Journal of Child Psychology and Psychiatry, 32(5), 757–770. https://doi.org/10.1111/j.1469-7610.1991.tb01900.x
Ikram, A., Suhail, K., Jafery, S. Z., & Singh, S. (2011). Rates of expressed emotions in Pakistani relatives of patients with schizophrenia. The Israel Journal of Psychiatry and Related Sciences, 48(2), 74–81.
Iqbal, H., & Golombok, S. (2018). The generation game: Parenting and child outcomes in second-generation South Asian immigrant families in Britain. Journal of Cross-Cultural Psychology, 49, 25–43. https://doi.org/10.1177/0022022117736039
Jones, P. (2022). networktools: Tools for identifying important nodes in networks. R package version 1.5.0. https://CRAN.R-project.org/package=networktools
Kavanagh, D. J., O’Halloran, P., Manicavasagar, V., Clark, D., Piatkowska, O., Tennant, C., & Rosen, A. (1997). The Family Attitude Scale: Reliability and validity of a new scale for measuring the emotional climate of families. Psychiatry Research, 70(3), 185–195. https://doi.org/10.1016/s0165-1781(97)00033-4
Koenigsberg, H. W., Klausner, E., Chung, H., Pelino, D., & Campbell, R. (1995). Expressed Emotion and Warmth: Extending the EE Construct to Insulin-dependent Diabetes Mellitus. International Journal of Mental Health, 24(2), 50–63. http://www.jstor.org/stable/41344723
Lopez, S. R., Ramirez Garcia, J. I., Ullman, J. B., Kopelowicz, A., Jenkins, J., Breitborde, N. J., & Placencia, P. (2009). Cultural variability in the manifestation of expressed emotion. Family Process, 48(2), 179–194. https://doi.org/10.1111/j.1545-5300.2009.01276.x
McCarty, C. A., Lau, A. S., Valeri, S. M., & Weisz, J. R. (2004). Parent-child interactions in relation to critical and emotionally overinvolved expressed emotion (EE): Is EE a proxy for behavior? Journal of Abnormal Child Psychology, 32(1), 83–93. https://doi.org/10.1023/b:jacp.0000007582.61879.6f
Niazi, A. W. M. (2019). Intergenerational trauma in second generation afghan american males (Order No. 13897012). Available from ProQuest Central; ProQuest Dissertations & Theses Global. (2239958537). Retrieved from https://www.proquest.com/dissertations-theses/intergenerational-trauma-second-generation-afghan/docview/2239958537/se-2
O’Driscoll, C., Sener, S. B., Angmark, A., & Shaikh, M. (2019). Caregiving processes and expressed emotion in psychosis, a cross-cultural, meta-analytic review. Schizophrenia Research, 208, 8–15. https://doi.org/10.1016/j.schres.2019.03.020
R Core Team. (2022). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing. URL https://www.R-project.org/
Ramanathan, A., Miah, S., Nagularaj, L., Sharif, H. S., & Shaikh, M. (2023, January 26). Perceived expression of emotion in individuals with a first episode of psychosis from a South Asian background. https://doi.org/10.31219/osf.io/6cmfd
Rogers, R. G. (2021). Intergenerational transmission of war trauma among afghan refugees in canada (Order No. 28770792). Available from ProQuest Central; ProQuest Dissertations & Theses Global. (2619233441). Retrieved from https://www.proquest.com/dissertations-theses/intergenerational-transmission-war-trauma-among/docview/2619233441/se-2
Sharif, H. S., Miah, S. K., Ramanathan, A., Glover, N., & Shaikh, M. (2022). Expression of emotion in the British South Asian Diaspora: A Qualitative Study. medRxiv, 2022.2012.2021.22283824. https://doi.org/10.1101/2022.12.21.22283824
Shariff, A. (2009). Ethnic identity and parenting stress in South Asian families: Implications for culturally sensitive counselling. Canadian Journal of Counselling, 43(1), 35–46. Retrieved from https://cjc-rcc.ucalgary.ca/article/view/ 58908
Singh, S. P., Harley, K., & Suhail, K. (2013). Cultural specificity of emotional overinvolvement: A systematic review. Schizophrenia Bulletin, 39, 449–463. https://doi.org/10.1093/schbul/sbr170
Smith, L. M. (2013). Ethnic differences in caregiving processes in first-episode psychosis. King’s College London. https://ethos.bl.uk/OrderDetails.do?uin=uk.bl.ethos.650759
Van Borkulo, C. D., van Bork, R., Boschloo, L., Kossakowski, J. J., Tio, P., Schoevers, R. A., ... & Waldorp, L. J. (2022). Comparing network structures on three aspects: A permutation test. Psychological Methods. https://doi.org/10.1037/met0000476
Vaughn, C., & Leff, J. (1976). The measurement of expressed emotion in the families of psychiatric patients. The British Journal of Social and Clinical Psychology, 15(2), 157–165. https://doi.org/10.1111/j.2044-8260.1976.tb00021.x
Vaughn, C. E., & Leff, J. P. (1981). Patterns of emotional response in relatives of schizophrenic patients. Schizophrenia Bulletin, 7(1), 43–44. https://doi.org/10.1093/schbul/7.1.43
Wiedemann, G., Rayki, O., Feinstein, E., & Hahlweg, K. (2002). The Family Questionnaire: Development and validation of a new self-report scale for assessing expressed emotion. Psychiatry Research, 109(3), 265–279. https://doi.org/10.1016/s0165-1781(02)00023-9
Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scand., 67(6), 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
Author information
Authors and Affiliations
Contributions
ZF: collection, analysis or interpretation of data.
HSS: collection of data.
CO: analysis or interpretation of data, drafting the article or revising it critically for important intellectual content.
MS: conception or design; interpretation of data; drafting the article or revising it critically for important intellectual content.
Corresponding author
Ethics declarations
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Yorkshire and The Humber – South Yorkshire Research Ethics Committee (IRAS: 230098) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual adult participants included in the study.
Conflicts of interest
The authors declare they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
All authors have given final approval of the version to be published.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shaikh, M., Fatima, Z., Sharif, H.S. et al. Expressed emotion and wellbeing in South Asian heritage families living in the UK. Curr Psychol 43, 8852–8860 (2024). https://doi.org/10.1007/s12144-023-04937-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-04937-y