
Abstract
The aim of this study was to explore the relationship between parents’ perceived social support and children’s mental health and the mediating role of parental marital quality and parent‒child relationships. The Multidimensional Scale of Perceived Social Support, the Parental Marital Quality Scale, the Child‒Parent Relationship Scale and the Strengths and Difficulties Questionnaire were used to survey 822 parents of young children (50% fathers) in Changchun, Jilin Province, China. The results indicated that (1) parents’ perceived social support was positively correlated with children’s mental health; (2) parental marital quality and parent‒child relationships play a simple mediating role between parents’ perceived social support and children’s mental health; and (3) parental marital quality and parent‒child relationships also play a chain mediating role between parents’ perceived social support and children’s mental health. This suggests that providing good social support for parents enhances the quality of marriages and parent‒child relationships and will also contribute to good mental health in children.
Highlights
Parents’ perceived social support is positively associated with children’s mental health.
Parental marital quality and parent‒child relationships play a simple mediating role and a chain mediating role between parents’ perceived social support and children’s mental health.
These findings have practical implications for parents, educators, and professionals in adopting appropriate methods to cultivate children’s mental health.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Mental health refers to a sustained mental state in which individuals have vitality, positive inner experiences, good social adjustment and positive social functioning and are able to effectively reach their physical and mental potential (Liu, 2001). Children’s mental health is divided into five main components: emotional symptoms, behavioral problems, attention-deficit/hyperactivity disorder, peer interaction and prosocial behavior (Goodman, 1994; Goodman & Goodman, 2009). In young children, good mental health promotes the development of peer relationships and prosocial behavior (Li, 2000), while poor mental health can lead to a range of problems, including aggressive behavior and anxiety (Wang et al., 2010). Ecosystem theory suggests that young children’s development is influenced by a range of environmental factors, such as factors in home, kindergarten and community environments, and that there are interactions between these environmental factors and the child’s internal factors that ultimately affect their development (Bronfenbrenner, 1979). In the available literature, there is a paucity of research on the impact of parents’ perceived social support on children’s mental health, and the ways in which external environmental factors, such as community and family factors, act on young children’s mental health are unclear. Therefore, based on ecosystem theory, this study aimed to examine the influence of parents’ perceived social support, parental marital quality and parent‒child relationships on children’s mental health; this will not only help clarify the research on the role of family and community factors in children’s mental health but also provide directions for subsequent interventions for children’s mental health and the development of mental health education in kindergartens.
Parents’ perceived social support and children’s mental health
Numerous studies have shown that young children’s mental health is influenced by many internal factors, including a child’s own temperament (Overton et al., 2015), parenting behavior (Rinaldi & Howe, 2012), and peer interaction (Holmes et al., 2016). External factors also influence the development of children’s mental health to varying degrees. Social support is one of the most important macrosocial factors influencing children’s mental health and refers to the subjective and objective support that individuals receive from their social networks, as well as their use of the support they receive (Xiao, 1994). Sources of social support generally include family support, friend support and other support (Zimet et al., 1990).
Social support can alleviate psychological stress through social bonding and maintain and improve an individual’s physical and mental health (Cohen & McKay, 2020; Yan et al., 2022.). Previous research has shown that social support may make parents more optimistic, which may improve their physical and mental health and increase the effectiveness of their parenting (Sehmi et al., 2020). When parents feel they have support and social networks at their disposal, their mental health improves (Taylor et al., 2015). Social support can help parents regulate their emotional responses to their children (Marroquín, 2011), and parents with high levels of social support have more consistent parenting behaviors (Byrnes & Miller, 2012). Social support can also provide parents with information about their child’s development and advice about appropriate parenting practices that can help them to adjust their expectations and improve their parenting skills (Cochran & Niegro, 2002). Conversely, a lack of or inadequate social support may be a risk factor for parental mental health, leading to inappropriate parenting practices (Belsky & Jafee, 2015). Mental health problems in parents can have adverse effects on parenting practices, causing parents to have fewer positive interactions with their infants and toddlers, to have higher rates of negative interactions and hostility, to communicate less effectively and to be less responsive to child behavior (Lovejoy et al., 2000; Gordon et al., 1989; Lovejoy et al., 1991; Goodman & Brumley, 1990). Therefore, parents’ perceived social support plays a crucial role in parenting beliefs and parents’ behavior, which may contribute to the development of children’s mental health. Thus, parents’ perceived social support may positively correlate with children’s mental health.
Mediating role of parental marital quality
Parental marital quality refers to a couple’s objective evaluation and subjective perception of marital harmony and is influenced by individual factors (i.e., values, expectations of marriage), intermarital factors (i.e., the distribution of power and roles between spouses) and external factors (i.e., economic status) (Fowers & Olson, 1986). Generally, parental marital quality can be categorized into three dimensions: marital satisfaction, partner communication and conflict resolution (Olson, 1986).
Good social support is conducive to marital quality. Several studies have shown that there is a significant positive relationship between the level of social support and marital quality (Xing et al., 2009; Xu & Hu, 2010; Noelle, 2015; Taylor et al., 2012). Social support plays an important role in determining the quality of marriage for Pakistani women (Qadir et al., 2013). Research from China has also shown that a couple’s perceived mutual family-of-origin emotional support contributes to marital quality for both partners (Yuan & Fang, 2016). This may be because social networks can provide various types of support that have reciprocal psychological and socioeconomic benefits (Brown et al., 2010). Positive social support can increase married individuals’ self-esteem and sense of self-worth and increase their marital satisfaction (Bryant & Conger, 1999). At the same time, when an individual feels emotionally supported, their perceived reality becomes a psychological reality; this psychological reality acts as a practical influence on behavior and development, which in turn influences the individual’s behavior and feelings in their marital relationship, leading to higher levels of satisfaction regarding the way their partner behaves in the relationship (Ma et al., 2015).
Parental marital quality has a significant impact on children’s mental health. The stability of the marital relationship contributes to the smooth functioning of other subsystems in the family, such as parent‒child relationships, and is closely related to the emotional and adaptive capacities of young children (Li et al., 2020). According to emotional security theory, the security and protection that young children receive in a positive family environment builds emotional security and has a profound impact on their subsequent physical and mental development, including their ability to manage and regulate their emotions, form close relationships with others and actively explore their surroundings (Davies & Cummings, 1998). Conversely, destructive interparental conflict increases children’s vulnerability to mental problems by undermining their ability to preserve emotional security within various family relationships (Davies et al., 2016). It has been shown that a good relationship between parents directly influences the physical and emotional development of young children (Fincham & Hall, 2005) and positively predicts the level of social-emotional development at approximately 3 years of age (Belsky et al., 1991). Children whose parents have a good relationship have a significantly reduced risk of internalizing behaviors (Leidy et al., 2009) and enhanced prosocial behavior (Wang et al., 2022), while children whose parents have a poor relationship are more likely to have internalizing problems, such as low self-esteem and depression (Gerard et al., 2006; Shek, 2000), as well as externalizing behavior problems (Gamliel et al., 2018). In addition, serious marital conflict is associated with belittling or punitive responses of fathers to their children’s negative emotions, which are likely to increase over time and will have a negative impact on children’s mental health (Davies et al., 2009). In other words, the better the parental marital quality, the better the mental health of the young child and the fewer internalizing behavioral problems he or she will experience. Thus, parental marital quality may mediate the relationship between parents’ perceived social support and young children’s psychological well-being.
The mediating role of parent‒child relationships
Parent‒child relationships are interpersonal relationships established by the interaction between parents and children in a family based on blood and genetics. As the earliest social relationships to which people are exposed, parent‒child relationships affect many aspects of an individual’s personality development, social cognition and mental health (Wang & Feng, 2006). Currently, parent‒child relationships are mainly categorized into two dimensions: intimacy and conflict (Zhang et al., 2015). Increased levels of social support are effective in improving parent‒child relationships, increasing parent‒child warmth and decreasing parent‒child hostility (Lippold et al., 2018). This may be due to two reasons. On the one hand, social support can effectively contribute to the quality of children’s family life (Feng et al., 2022; Balcells-Balcells et al., 2019). Parents may have more time and energy to devote to parenting and can form better parent‒child relationships. On the other hand, social support can reduce parents’ stress, improve their mental health and positively influence their parenting behavior (Taylor et al., 2015; Ostberg & Hagekull, 2000). Parents can benefit from social support and obtain effective parenting advice and guidance (Dominguez & Watkins, 2003). Social support can also help parents regulate their emotional responses to their children and reduce the use of harsh parenting behaviors, resulting in more consistent parenting behaviors and more parental warmth (Marroquín, 2011; Byrnes & Miller, 2012; McConnell et al., 2011).
Parent‒child relationships and children’s mental health are closely related. Parent‒child relationships are important in children’s development. Compared to other interpersonal relationships in the family, parent‒child relationships have a more direct impact on children and are an important factor in the development of an individual’s personality, mental health and adjustment (Hu et al., 2009). Parent‒child attachment and parent‒child closeness are important expressions of parent‒child relationships. Parent‒child attachment is defined as the long-term, ongoing emotional bond that forms between a child and a caregiver. Secure attachment is an important foundation for good development and social adjustment in children, and parent‒child attachments have a certain stability as children grow older (Ainsworth, 1967). It has been shown that children with secure parent‒child attachments have better development of positive social skills, higher levels of cognitive functioning and better physical and mental health (Ranson & Urichuk, 2008). Parent‒child bonding refers to the close, warm emotional connection between parents and their children, which can be reflected in both positive interactive behaviors and intimate feelings toward each other (Zhao et al., 2013). Some researchers believe that parent‒child bonding is the basis for normal child development and is the most stable protective factor for healthy individual development (Barber et al., 2005). In conclusion, children who have close, warm parent‒child relationships have fewer externalizing and internalizing problems (Lamborn & Felbab, 2001), lower levels of suicidal ideation (Harris & Molock, 2000) and better mental health. Thus, parent‒child relationships may mediate the relationship between parents’ perceived social support and children’s mental health.
The chain mediating role of parental marital quality and parent‒child relationships
Family systems theory suggests that the family is composed of a marital subsystem, a maternal subsystem and a paternal subsystem, with the parental marital subsystem and the parent‒child system being closely related (Sang & Xi, 2005). There are currently two main theoretical assumptions in the study of marital relationships and parent‒child relationships: a spillover hypothesis and a compensatory hypothesis. The spillover hypothesis suggests that parents in higher quality marriages show more accepting attitudes, emotions and behaviors toward their children and are more sensitive to their children’s needs, resulting in a secure attachment between the parents and their children. Parents in stressful, conflictual marriages, however, focus more on their arguments and emotional behavior and less on the needs of their children, resulting in alienation and mistrust of the parents and tension in the parent‒child relationship (Easterbrooks & Emde, 1988; Erel & Burman, 1995). The compensatory hypothesis, on the other hand, assumes that there is a negative correlation between marital relationships and parent‒child relationships. In stressful and conflictual marriages, couples are unable to achieve emotional closeness and psychological satisfaction. As a result, parents turn to the parent‒child relationship for compensation, devoting more attention to their children and seeking to maintain close relationships with them (Engfer, 1988). For example, in a study of 203 families with adolescent children, poor marital relationship quality predicted improvements in mother-child relationship quality on the next day (Kouros et al., 2014). With regard to socialization processes, mothers are posited to be better able to compartmentalize family relationships, thereby keeping their feelings and perceptions of their marriage from adversely affecting their relationship with their child (Belsky et al., 1984). Both theoretical hypotheses explain the mechanisms at play in the relationship between marriage and parenthood. However, the spillover hypothesis is supported by more empirical studies, while there is little evidence to support the compensatory hypothesis (Zimet & Jacob, 2001). Parents who have experienced unhappy marriages are therefore more likely to behave indifferently and emotionally toward their children, resulting in deterioration of the parent‒child relationships rather than promoting closeness between them. At the same time, individuals who experience more social support are psychologically healthier and have higher quality marriages, and children who have close, warm parent‒child relationships have better mental health (Lamborn & Felbab, 2001; Harris & Molock, 2000). Thus, marital quality and parent‒child relationships may play a chain mediating role in the relationship between parents’ perceived social support and children’s mental health.
Current study
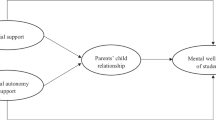
In summary, we proposed a chain mediation model to test the relationship between parents’ perceived social support and children’s mental health. We proposed the following hypotheses: (1) parents’ perceived social support is related to children’s mental health; (2) parental marital quality and parent‒child relationships play a simple mediating role between parents’ perceived social support and children’s mental health; and (3) parental marital quality and parent‒child relationships also play a chain mediating role between parents’ perceived social support and children’s mental health. A diagram of the research framework is shown in Fig. 1.

The proposed model
PSS = Perceived social support, PMQ = Parental marital quality, PCR = Parent‒child relationship, CPH = Children’s mental health
Methods
Participants
The study was approved by the ethics committee of the first author’s university, and an online questionnaire was distributed to parents of young children in Changchun in September 2022. All variables were reported by parents through the questionnaire. A total of 901 questionnaires were collected; 79 invalid questionnaires were excluded, and 822 valid questionnaires were collected, with a 91.2% return rate. All questions in the questionnaire were completed before submission, with no missing values.
Of the valid questionnaires, 50% were completed by fathers and 50% were completed by mothers; 17% of the parents were aged 30 years and under, 53.6% were aged 31–35 years, 20.2% were aged 36–40 years and 9.1% were aged 41 years and over. Among them, 12.4% had a monthly household income of less than RMB 3,000, 40.1% had an income of RMB 3,001–6,000, 25.2% had an income of RMB 6,001–9,000, 11.4% had an income of RMB 9,001–12,000 and 10.8% had an income over RMB 12,000. Among the child population, 26.6% were 3-year-olds, 21.2% were 4-year-olds, 33.1% were 5-year-olds and 19.1% were 6-year-olds; the mean age was 5.18, and the standard deviation was 1.34. A total of 54.31% of the children were boys. A total of 60.8% were only children.
Process
First, we developed a theoretical framework for this study and constructed a chain mediation model. Second, we invited parents of young children in Changchun, Jilin Province, China, to complete an online questionnaire. To ensure that the study met certain ethical norms, we obtained parental consent to conduct the survey, emphasized that the questionnaire was voluntary, and ensured the anonymity and confidentiality of the information collected. Again, we asked the parents to answer independently according to their own circumstances. It took approximately 10 min to complete the questionnaire. Finally, we collated and entered the collected data.
Measures
Parental marital quality scale
In this study, three dimensions from the Parental Marital Quality Scale (marital satisfaction, partner communication, and conflict resolution) were used to measure marital quality. One of the questions was “I am not satisfied with my partner’s personality traits and personal habits.“ This scale, which was developed by Fowers and Olson (Fowers & Olson, 1989) and translated by Ma (Ma et al., 1999), is scored using a 5-point scale ranging from “This is true” (1 point) to “Really not true” (5 points), with 30 questions and 3 subscales, each containing 10 questions. Higher scores indicate better marital quality. The Cronbach’s alpha coefficient for the scale was 0.877, and the CFA fit was good (χ2/df = 5.529, RMSEA = 0.074, CFI = 0.901, GFI = 0.951, TLI = 0.936, IFI = 0.952).
Perceived social support scale
The Perceived Social Support Scale (PSSS) was developed by Zimet et al. (Zimet et al., 1988) and translated into Chinese by Jiang and Huang (Huang, 1996). The scale is scored using a 7-point scale, ranging from “strongly disagree” (1) to “strongly agree” (7), with 12 questions divided into three dimensions: family support, friend support, and other support. One of the questions was “I can rely on my friends when things go wrong.“ Higher scores indicate more perceived social support. In this study, the Cronbach’s alpha coefficient for the scale was 0.939, and the CFA fit was good (χ2/df = 5.018, RMSEA = 0.078, CFI = 0.956, GFI = 0.949, TLI = 0.956, IFI = 0.940).
Child‒parent relationship scale
The Child‒Parent Relationship Scale (CPRS) was developed by Pianta (Pianta, 1992) and revised by Zhang et al. (Zhang et al., 2015) to assess parent‒child relationships. The scale is scored using a 5-point scale, ranging from “not at all” (1 point) to “fully” (5 points), with 22 questions in total. One of the questions was “I share an affectionate, warm relationship with my child”. The Cronbach’s alpha coefficient for this scale was 0.805, and the CFA fit was good (χ2/df = 4.379, RMSEA = 0.064, CFI = 0.994, GFI = 0.993, TLI = 0.982, IFI = 0.994).
Children’s mental health scale
The Strengths and Difficulties Questionnaire (SDQ) was modified by the British psychologist Goodman (Goodman, 1994; Goodman & Goodman, 2009) and revised by Kou et al. (Kou et al., 2015). This scale is scored using a 3-point scale, ranging from ‘does not meet’ (1 point) to ‘fully meets’ (3 points), with 25 questions divided into five dimensions: emotional symptoms, behavioral problems, attention-deficit/hyperactivity disorder, peer interaction and prosocial behavior. One of the questions was “Consideration of other people’s feelings”. The higher the score, the better the child’s mental health is. The questionnaire is available for parents, teachers and children and adolescents themselves (for those aged ≥ 11 years); the parent version was used in this study. The Cronbach’s alpha coefficient for the scale was 0.762, and the CFA fit was good (χ2/df = 5.891, RMSEA = 0.077, CFI = 0.905, GFI = 0.953, TLI = 0.906, IFI = 0.907).
Data analysis
In this study, the SPSS 23.0 software program was used for common method bias tests, descriptive statistical analysis of the variables, correlation analysis and regression analysis. Structural equation models were tested, and bootstrap analysis was performed using AMOS 24.0, where bootstrap methods were used to draw samples 5000 times and estimate 95% confidence intervals.
Results
Common method deviation test
Data for all variables in this study were reported by parents. An unrotated factor analysis was conducted for all questionnaire items using Harman’s one-way test (Zhou & Long, 2004). The results of the unrotated exploratory factor analysis extracted a total of 17 factors with a characteristic root greater than 1. The maximum factor variance explained was 19.116%, which was less than 40%, so there was no serious common method bias in this study.
Descriptive statistics and correlations
The descriptive statistics and correlations of all variables are presented in Table 1. The results indicate that parents’ perceived social support, parental marital quality, parent‒child relationships and children’s mental health were all significantly positively correlated with each other. Conflict in parent‒child relationships was significantly and negatively correlated with parents’ perceived social support, parental marital quality and children’s mental health and its dimensions; intimacy in parent‒child relationships was significantly and positively correlated with parental marital quality, parents’ perceived social support and children’s mental health and its dimensions.
Chain mediating role
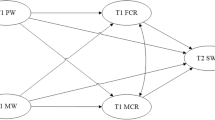
To further examine the relationships among parents’ perceived social support, parental marital quality, parent‒child relationships and children’s mental health and to test the mediating role of parental marital quality and parent‒child relationships, latent variable structural equation modeling was used to construct a model of the relationships among the four variables, as shown in Fig. 2. The results showed the following fit indicators of the model: χ2/df = 4.634, RMSEA = 0.067, NFI = 0.970, IFI = 0.975, TLI = 0.967 and CFI = 0.968. All indicators fit well, indicating that the data fit the constructed model well.

A model of the relationships among parents’ perceived social support, parental marital quality, parent‒child relationships and children’s mental health
Analysis of the pathways in this structural equation model showed the following: parents’ perceived social support was a significant positive predictor of children’s mental health (β = 0.14, p < .01), supporting Hypothesis 1. Parents’ perceived social support was a significant positive predictor of parental marital quality (β = 0.12, p < .01); parental marital quality was a significant positive predictor of parent‒child relationships (β = 0.59, p < .01); parent‒child relationships were a significant positive predictor of children’s mental health (β = 0.14, p < .01); parents’ perceived social support was a significant positive predictor of parent‒child relationships (β = 0.20, p < .01); and parental marital quality was a significant positive predictor of children’s mental health (β = 0.18, p < .01).
The total indirect effect of parental marital quality and parent‒child relationships on children’s mental health was 0.265. Specifically, the mediating effect of parental marital quality and parent‒child relationships consisted of indirect effects generated by three pathways: (1) the indirect effect through the pathway of parents’ perceived social support → parental marital quality → children’s mental health was 0.220; (2) the indirect effect through the pathway of parents’ perceived social support → parent‒child relationships → children’s mental health was 0.034; and (3) the indirect effect through the pathway of parents’ perceived social support → parental marital quality → parent‒child relationships → children’s mental health was 0.011. The ratio of the intermediary effect to the total effect was 65%.
The test was conducted using bootstrap analysis, with confidence intervals set at 95%, and a significant mediating effect was indicated if the 95% confidence interval for the mediating effect value did not include 0. The 95% confidence intervals for each pathway of action from parents’ perceived social support to children’s mental health are shown in Table 2. As seen from the results in Table 2, the bootstrapped 95% confidence intervals for the mediating effects of parents’ perceived social support → parental marital quality → children’s mental health and parents’ perceived social support → parent‒child relationship → children’s mental health pathways and the chain mediating effect of parents’ perceived social support → parental marital quality → parent‒child relationships → children’s mental health pathway did not include 0, indicating that all three indirect effects were significant. These results supported Hypothesis 2 and Hypothesis 3.
Discussion
Based on ecosystem theory, in this study, we explored the influence of social factors (parents’ perceived social support) on children’s mental health through family factors (parental marital quality and parent‒child relationships). The results showed that parents’ perceived social support positively correlated with children’s mental health and that parental marital quality and parent‒child relationships played a simple mediating role and a chain mediating role between parents’ perceived social support and children’s mental health.
Parents’ perceived social support is positively related to children’s mental health
Our results indicated that parents’ perceived social support positively correlated with children’s mental health. In other words, the higher the parents’ perceived social support, the less likely young children are to experience mental health disorders and the better their mental health is likely to be. Hypothesis 1 was supported by these results. Moreover, this finding is consistent with previous results: better family functioning, more social support, and more resilience skills were related to better child well-being (Gaspar et al., 2022). In addition, the findings of this study confirm that the result of a positive relationship between parental perceived social support and children’s mental health can also be applied to children aged 3–6 years in China. Previous studies have noted that social support can alleviate psychological stress through social bonding and maintain and improve an individual’s mental and physical health (Cohen & McKay, 2020). Social support may make parents more optimistic, thus improving their physical and mental health and increasing the effectiveness of their parenting (Sehmi et al., 2020). Social support may also help parents regulate their emotional responses to their children, and parents with high levels of social support have more consistent parenting behaviors (Byrnes & Miller, 2012). Conversely, a lack of or inadequate social support may be a risk factor for parents’ mental health, leading to inappropriate parenting practices (Belsky & Jafee, 2015). Social support can also provide parents with information about their children’s development and appropriate parenting practices, and this information and advice can help them to adjust their expectations and improve their parenting skills (Cochran & Niegro, 2002). Therefore, it can be said that the higher the level of perceived social support of parents, the higher their level of effective parenting is likely to be, which may contribute positively to children’s mental health.
The mediating role of parental marital quality and parent‒child Relationships
Our study shows that parental marital quality and parent‒child relationships play a simple mediating role between perceived parental social support and children’s mental health, which supports Hypothesis 2. First, our study revealed that parental marital quality mediated the relationship between parents’ perceived social support and children’s mental health. Social networks can provide various types of support that have reciprocal psychological and socioeconomic benefits (Brown et al., 2010). Positive social support can increase a married person’s self-esteem, sense of self-worth and marital satisfaction (Bryant & Conger, 1999). When individuals feel emotionally supported in a marriage, the reality they perceive becomes a psychological reality; this psychological reality acts as a practical influence on behavior and development, which in turn influences how the individual behaves and feels in their marital relationship, leading to a higher level of satisfaction regarding the way their partner behaves in the relationship. A good relationship between parents has a direct impact on the physical and emotional development of young children (Fincham & Hall, 2005) and can also positively predict the level of social-emotional development around the age of three (Belsky et al., 1991). Children whose parents have good relationships have a significantly reduced risk of internalizing behaviors (Leidy et al., 2009) and enhanced prosocial behaviors, while children with poor parental relationships are more likely to have internalizing problems, such as low self-esteem and depression (Gerard et al., 2006; Shek, 2000), as well as externalizing behavior problems (Gamliel et al., 2018).
Second, our study found that parent‒child relationships mediated the relationship between parents’ perceived social support and young children’s mental health. Social support may help parents regulate their emotional response to their children (Marroquín, 2011), resulting in more consistent parenting behaviors and more parental warmth and less likelihood of using harsh parenting behaviors across a range of child ages (Byrnes & Miller, 2012; Ceballo & McLoyd, 2002; Marroquín, 2011; McConnell et al., 2011). Researchers believe that social support helps parents cope with adversity and improve their enthusiasm while raising children (Milgrom et al., 2019). Specifically, researchers surveyed Mexican mothers and found that mothers who received more social support had higher parenting efficacy and a healthier mental status (Izzo, 2000). Recently, many studies have confirmed that providing adequate and necessary social support for mothers can significantly enhance their parenting confidence, relieve their parenting pressure, and improve their parenting competence, thereby enhancing their parental warmth (Coert et al., 2021; Douglas, 2018; Mathew et al., 2017; Mason et al., 1994). A more detailed longitudinal study of rural parents in two-parent families was also conducted that investigated whether perceived control and social support in adolescents in sixth grade were independently or interactively associated with changes in parenting behaviors (discipline, standard-setting) and parent‒child warmth and hostility over 6 months and whether these associations differed by parental gender. The results showed that greater perceived control predicted more increases in consistent parental discipline and standard setting, while greater social support predicted increases in parent‒child warmth and decreases in parent‒child hostility. Parental perceived control moderated the effect of social support on parental warmth: for mothers only, social support was significantly associated with parental warmth only when mothers’ perceived self-control was low (but not high) (Lippold et al., 2018). Most studies agree that social support facilitates parents’ own healthy physical and mental development and positive parenting behaviors, which in turn lead to a good parent‒child relationship. Furthermore, parent‒child relationships have an impact on the mental health of young children. Children who have close, warm parent‒child relationships have fewer externalizing and internalizing problems (Lamborn & Felbab, 2001), lower levels of suicidal ideation (Harris & Molock, 2000) and better mental health. Parent‒child attachment is an important indicator of a good parent‒child relationship. Children with secure parent‒child attachments have better development of positive social skills, higher levels of cognitive functioning and better physical and mental health (Ranson & Urichuk, 2008).
Most importantly, the chain role of parental marital quality and parent‒child relationships in mediating the relationship between parents’ perceived social support and children’s mental health was also confirmed in this study. This result supports Hypothesis 3. The spillover hypothesis suggests that parents in higher quality marriages show more accepting attitudes, emotions and behaviors toward their children and are more sensitive to their children’s needs, resulting in secure attachments between parents and children. Parents in stressful, conflictual marriages, however, focus more on their arguments and emotional behavior and pay less attention to the needs of their children, resulting in alienation and mistrust of the parents and tension in the parent‒child relationships (Easterbrooks & Emde, 1988). As a result, parents who have experienced unhappy marriages are more likely to display indifferent and emotional behavior toward their children, resulting in a deterioration of the parent‒child relationship rather than promoting closeness between them. At the same time, individuals who experience more social support are more psychologically healthy and have higher quality marriages, and children who have close, warm parent‒child relationships have better mental health (Lamborn & Felbab, 2001). Therefore, parents who experience more social support are more optimistic about their present and future lives and have higher quality marriages, which subsequently contribute to good parent‒child relationships and thus have a positive impact on children’s mental health. Additionally, the mediating effect through parents’ perceived social support → parental marital quality → children’s psychological health is much larger than the other two mediating pathways, which may be because a family system begins with the establishment of a marriage, and the marital relationship is the basic subsystem in a family and has a strong influence on the function of the whole family (Erel & Burman, 1995). The quality of marital relationships is an important factor affecting other family relationships (Yu & Gamble, 2008). If parents are experiencing marriage conflicts, they are less sensitive to their children’s needs, showing more negative reactions to parent–child communication, which further increases the likelihood of children’s mental health problems (Kong et al., 2011). Moreover, children take parental behavior as an example according to social learning theory (Rosenstock et al., 1988). If children are constantly exposed to marital conflicts, they take the negative acquired behavior into the parent–child interaction, thus triggering parent–child conflicts (Easterbrooks & Emde, 1988). It can be argued that parental marital quality is the foundation of a family relationship, and other relationships revolve around parental marital quality, which therefore has a much greater mediating role than the other two pathways.
The findings of the current study have various theoretical and practical implications. Theoretically, this study confirms Bronfenbrenner’s ecosystem theory, as the findings confirm that social factors (perceived social support) can influence an individual’s mental health through family factors (parental marital quality and parent‒child relationships) and that improvements in parents’ perceived social support, parental marital quality and parent‒child relationships are more conducive to the development of good mental health in young children. In addition, this study validates emotional security theory, which states that a good marital relationship is more conducive to children’s mental health development. In terms of practice, this study offers new intervention or support pathways for the development of children’s mental health. First, we encourage the provision of necessary social support for parents, as previous research has shown that there are many benefits of parents’ perceived social support, which helps parents develop good mental and physical states and good parenting behaviors (Sehmi et al., 2020). Thus, young children will also benefit from good care from their parents, which will contribute to the development of their mental health, as shown in this study. Second, we encourage parents to build good marital relationships, as the family begins with the establishment of the marital relationship and the marital system nurtures the parent‒child system. The quality of the marital relationship is a central element in family unity and harmony and plays a pivotal role in family life (Cox & Paley, 1997). Tension in parental marital relationships can cause hostility between parents and their children, which in turn can lead to problems for children (Low & Stocker, 2005; Gerard et al., 2006). Finally, we equally encourage parents and young children to maintain good parent‒child relationships. The establishment of positive parent‒child relationships is an important condition for the psychological well-being of children. Compared to other interpersonal relationships in the family, parent‒child relationships have a more direct impact on children and are an important factor in the development of an individual’s personality, psychological well-being and adjustment. All of the above educational suggestions have the potential to help reduce parenting difficulties, improve positive parenting skills, build good parent‒child relationships and ultimately promote the development of children’s mental health.
Limitations and conclusion
We acknowledge a number of limitations of the present study. First, all data were collected by means of parental reports, and although we used the Harman one-way test and confirmed that there was no significant common method bias in the current study, the associations between variables may have been overstated. Therefore, multiple methods (e.g., behavioral observation or peer reporting) need to be used to measure these variables in future studies. Second, a cross-sectional research method was used in this study, which made it difficult to measure the causal relationships between variables. Future research should use longitudinal research methods to test the variable relationships observed in this study. Third, there may be other mediating variables in the relationship between parents’ perceived social support and children’s mental health, and future research should consider the role of other mediating variables to further enrich and improve the mechanisms by which parents’ perceived social support influences children’s mental health.
In summary, there are simple and chain mediating effects of parental marital quality and parent‒child relationships on the relationship between parents’ perceived social support and children’s mental health. These results suggest that parental marital quality and parent‒child relationships play an important role in the relationship between parents’ perceived social support and children’s mental health. The findings of this study further support ecosystem theory and provide new interventions or support pathways for the development of children’s mental health.
Data Availability
As this study is a topic being led by the first author, the datasets generated and/or analyzed in the study are currently not publicly available, and this study is part of the topic but is available from the corresponding author upon reasonable request.
References
Ainsworth, M. D. S. (1967). Infancy in Uganda: Infant care and the growth of love. Johns Hopkins Press.
Balcells-Balcells, A., Giné, C., Guàrdia-Olmos, J., Summers, J. A., & Mas, J. M. (2019). Impact of supports and partnership on family quality of life. Research in Developmental Disabilities, 85, 50–60. https://doi.org/10.1016/j.ridd.2018.10.006
Barber, B. K., Stolz, H. E., & Olsen, J. A. (2005). Parental support, psychological control, and behavioral control: Assessing relevance across time, culture, and method. Monographs of the Society for Research in Child Development, 70(4), 1–137. http://www.jstor.org/stable/3701442
Belsky, J., & Jafee, S. R. (2015). The multiple determinants of parenting. In D. Cicchetti, & D. J. Cohen (Eds.), Developmental psychopathology: Risk, disorder, and adaptation (pp. 38–85). Wiley Online Library.
Belsky, J., Youngblade, L., Rovine, M., & Volling, B. (1991). Patterns of marital change and parent–child interaction. Journal of Marriage and the Family, 53(2), 487–498. https://doi.org/10.2307/352914
Belsky, J., Gilstrap, B., & Rovine, M. (1984). The Pennsylvania infant and Family Development Project, I: Stability and Change in Mother-Infant and Father-Infant Interaction in a family setting at one, three, and nine months. Child Development, 55(3), 692–705. https://doi.org/10.2307/1130122
Bronfenbrenner, U. (1979). The Ecology of Human Development: Experiments by Nature and Design (pp. 56–82). Harvard University Press.
Brown, E., Orbuch, T. L., & maharaj, A. (2010). Social networks and marital stability among black american and white american couples. In K. T. Sullivan, & J. Davila (Eds.), Support processes in intimate relationships (pp. 319–334). Oxford University Press.
Bryant, C. M., & Conger, R. D. (1999). Marital success and domains of social support in long-term relationships: Does the influence of network members ever end? Journal of Marriage and Family, 61(2), 437–450. https://doi.org/10.2307/353760
Byrnes, H. F., & Miller, B. A. (2012). The relationship between neighborhood characteristics and effective parenting behaviors: The role of social support. Journal of Family Issues, 33(12), 1658–1687. https://doi.org/10.1177/0192513X12437693
Ceballo, R., & McLoyd, V. C. (2002). Social support and parenting in poor, dangerous neighborhoods. Child Development, 73(4), 1310–1321. https://doi.org/10.1111/1467-8624.00473
Cochran, M., & Niegro, S. (2002). Parenting and social networks. In M. H. Bornstein (Ed.), Handbook of parenting: Social conditions and applied parenting (pp. 123–148). Lawrence Erlbaum Associates Publishers.
Coert, S. L., Adebiyi, B. O., Rich, E., & Roman, N. V. (2021). A comparison of the relationship between parental efficacy and social support systems of single teen mothers across different family forms in south african low socioeconomic communities. BMC Women’s Health, 21(1), 1–11. https://doi.org/10.1186/s12905-021-01300-w
Cohen, S., & McKay, G. (2020). Social support, stress and the buffering hypothesis: A theoretical analysis. Handbook of psychology and health (pp. 253–267). Routledge.
Cox, M. J., & Paley, B. (1997). Families as systems. Annual Review of Psychology, 48, 243–267. https://doi.org/10.1146/annurev.psych.48.1.243
Davies, P. T., & Cummings, E. M. (1998). Exploring children’s emotional security as a mediator of the link between marital relations and child adjustment. Child Development, 69(1), 124–139. https://doi.org/10.1111/j.1467-8624.1998.tb06138.x
Davies, P. T., Sturge-Apple, M. L., Woitach, M. J., & Cummings, E. M. (2009). A process analysis of the transmission of distress from interparental conflict to parenting: Adult relationship security as an explanatory mechanism. Developmental Psychology, 45(6), 1761–1773. https://doi.org/10.1037/a0016426
Davies, P. T., Martin, M. J., & Sturge-Apple, M. L. (2016). Emotional security theory and developmental psychopathology. In D. Cicchetti (Ed.), Developmental psychopathology: Theory and method (pp. 199–264). John Wiley & Sons, Inc.
Dominguez, S., & Watkins, C. (2003). Creating networks for survival and mobility: Social capital among african-american and latin-american low-income mothers. Social Problems, 50(1), 111–135. https://doi.org/10.1525/sp.2003.50.1.111
Douglas, A. M. (2018). It takes a village to raise a child: Perceived community support and parenting satisfaction and efficacy among American Indian young mothers (Order No. 10935650). Available from Publicly Available Content Database. (2114973695). https://www.proquest.com/dissertations-theses/takes-village-raise-child-perceived-community/docview/2114973695/se-2
Easterbrooks, M. A., & Emde, R. N. (1988). Marital and parent-child relationship: Role of affect in the family system. In A. H. Robert, & S. H. Joan (Eds.), Relationships within families: Mutual influences (pp. 83–103). Oxford University Press.
Engfer, A. (1988). The interrelatedness of marriage and the mother-child relationship. In R. A. Hinde, & J. S. Hinde (Eds.), Relationships within families: Mutual influences (pp. 104–118). Oxford, England, New York: Oxford University Press.
Erel, O., & Burman, B. (1995). Interrelatedness of marital relations and parent-child relations: A meta-analytic review. Psychological Bulletin, 118(1), 108–132. https://doi.org/10.1037/0033-2909.118.1.108
Feng, Y., Zhou, X., Qin, X., Cai, G., Lin, Y., Pang, Y., & Zhang, L. (2022). Parental self-efficacy and family quality of life in parents of children with autism spectrum disorder in China: The possible mediating role of social support. Journal of Pediatric Nursing, 63, 159–167. https://doi.org/10.1016/j.pedn.2021.10.014
Fincham, F. D., & Hall, J. H. (2005). Parenting and the marital relationship. In L. Tom, & O. Lynn (Eds.), Parenting: An ecological perspective (pp. 205–233). Lawrence Erlbaum Associates Publishers.
Fowers, B. J., & Olson, D. H. (1986). Predicting marital success with prepare: A predictive validity study. Journal of Marital and Family Therapy, 12(4), 403–413. https://doi.org/10.1111/j.1752-0606.1986.tb00673.x
Fowers, B. J., & Olson, D. H. (1989). Enrich marital inventory-a discriminant validity and cross-validation assessment. Journal of Marital and Family Therapy, 15(1), 65–79. https://doi.org/10.1111/j.1752-0606.1989.tb00777.x
Gamliel, K. H., Dollberg, D. G., & Levy, S. (2018). Relations between parents’ anxiety symptoms, marital quality, and preschoolers’ externalizing and internalizing behaviors. Journal of Child and Family Studies, 27(12), 3952–3963. https://doi.org/10.1007/s10826-018-1212-3
Gaspar, T., Gomez-Baya, D., Trindade, J. S., Guedes, B., Cerqueira, F., A., & de Matos, M. G. (2022). Relationship between family functioning, parents’ psychosocial factors, and children’s well-being. Journal of Family Issues, 43(9), 2380–2397. https://doi.org/10.1177/0192513X211030722
Gerard, J. M., Krishnakumar, A., & Buehler, C. (2006). Marital conflict, parent-child relations, and youth maladjustment: A longitudinal investigation of spillover effects. Journal of Family Issues, 27(7), 951–975. https://doi.org/10.1177/0192513X05286020
Goodman, R. (1994). A modified version of the rutter parent questionnaire including extra items on children’s strengths: A research note. Journal of Child Psychology and Psychiatry and Allied Disciplines, 35(8), 1483–1494. https://doi.org/10.1111/j.1469-7610.1994.tb01289.x
Goodman, S. H., & Brumley, H. E. (1990). Schizophrenic and depressed mothers: Relational deficits in parenting. Developmental Psychology, 26(1), 31–39. https://doi.org/10.1037/0012-1649.26.1.31
Goodman, A., & Goodman, R. (2009). Strengths and difficulties questionnaire as a dimensional measure of child mental health. Journal of the American Academy of Child and Adolescent Psychiatry, 48, 400–403. https://doi.org/10.1097/CHI.0b013e318198
Gordon, D., Burge, D., Hammen, C., Adrian, C., Jaenicke, C., & Hiroto, D. (1989). Observations of interactions of depressed women with their children. The American Journal of Psychiatry, 146(1), 50–55. https://doi.org/10.1176/ajp.146.1.50
Harris, T. L., & Molock, S. D. (2000). Cultural orientation, family cohesion, and family support in suicide ideation and depression among african american college students. Suicide and Life-threatening Behavior, 30(4), 341–353. https://doi.org/10.1111/j.1943-278X.2000.tb01100.x
Holmes, C. J., Kim-Spoon, J., & Deater-Deckard, K. (2016). Linking executive function and peer problems from early childhood through middle adolescence. Journal of Abnormal Child Psychology, 44(1), 31–42. https://doi.org/10.1007/s10802-015-0044-5
Hu, N., Deng, L., Zhang, J., Fang, X., Chen, L., & Mei, H. (2009). A longitudinal study of the relationship between Family Functioning and adolescent problematic behaviors. Psychological Development and Education, 25(4), 93–100. https://doi.org/10.16187/j.cnki.issn1001-4918.2009.04.014. (In Chinese).
Huang, L., Jiang, Q., & Ren, W. (1996). Research on the correlation between coping style, social support, and psychosomatic symptoms of cancer patients. Chinese Mental Health Journal, 4, 160–161. (In Chinese).
Izzo, C., Weiss, L., Shanahan, T., & Rodriguez-Brown, F. (2000). Parental self-efficacy and social support as predictors of parenting practices and children’s socioemotional adjustment in mexican immigrant families. Journal of Prevention & Intervention in the Community, 20(1–2), 197–213. https://doi.org/10.1300/J005v20n01_13
Kong, J. W., Liang, X. Y., & Meng, X. (2011). Survey on the impact of parents’ relationship and parent-child communication on mental health status of junior middle school students. Chinese Journal of School Health, 32(1), 53–54. Available at: http://en.cnki.com.cn/Article_en/CJFDTotal-XIWS201101025.htm
Kou, J., Du, Y., & Xia, L. (2015). Reliability and validity of “children strengths and difficulties questionnaire” in Shanghai norm. Shanghai Archives of Psychiatry, 17(1), 25–28. (In Chinese).
Kouros, C. D., Papp, L. M., Goeke-Morey, M. C., & Cummings, E. M. (2014). Spillover between marital quality and parent–child relationship quality: Parental depressive symptoms as moderators. Journal of Family Psychology, 28(3), 315–325. https://doi.org/10.1037/a0036804
Lamborn, S. D., & Felbab, A. J. (2001). Applying ethnic equivalence and cultural values models to african-american teens’ perceptions of parents. Journal of Adolescence, 26(5), 605–622. https://doi.org/10.1016/S0140-1971(03)00059-9
Leidy, M. S., Parke, R. D., Cladis, M., Coltrane, S., & Duffy, S. (2009). Positive marital quality, acculturative stress, and child outcomes among mexican Americans. Journal of Marriage and Family, 71(4), 833–847. https://doi.org/10.1111/j.1741-3737.2009.00638.x
Li, C., Jiang, S., Fan, X., & Zhang, Q. (2020). Exploring the impact of marital relationship on the mental health of children: Does parent-child relationship matter? Journal of Health Psychology, 25(10–11), 1669–1680. https://doi.org/10.1177/1359105318769348
Li, D. (2000). A study of factors influencing children’s pro-social behavior. Psychological Science, 23(03), 285–288. https://doi.org/10.16719/j.cnki.1671-6981.2000.03.007(Chinese Journal).
Lippold, M. A., Glatz, T., Fosco, G. M., & Feinberg, M. E. (2018). Parental perceived control and social support: Linkages to change in parenting behaviors during early adolescence. Family Process, 57(2), 432–447. https://doi.org/10.1111/famp.12283
Liu, H. (2001). Reconceptualization of the concept and criteria of mental health. Psychological Science, 24(04), 480–481. https://doi.org/10.16719/j.cnki.1671-6981.2001.04.031(In Chinese).
Lovejoy, M. C. (1991). Maternal depression: Effects on social cognition and behavior in parent-child interactions. Journal of Abnormal Child Psychology, 19, 693–706. https://doi.org/10.1007/BF00918907
Lovejoy, M. C., Graczyk, P. A., O’Hare, E., & Neuman, G. (2000). Maternal depression and parenting behavior: A meta-analytic review. Clinical Psychology Review, 20(5), 561–592. https://doi.org/10.1016/S0272-7358(98)00100-7
Low, S. M., & Stocker, C. (2005). Family functioning and children’s adjustment: Associations among parents’ depressed mood, marital hostility, parent-child hostility, and children’s adjustment. Journal of Family Psychology, 19(3), 394–403. https://doi.org/10.1037/0893-3200.19.3.394
Ma, H., Wang, X., Liu, Y., Luo, H., & Zhang, C. (2015). Structural equation model of marital quality factors of urban and rural residents. Chinese Journal of Behavioral Medical Science, 24(11), 1029–1032. https://doi.org/10.16128/j.cnki.1005-3611.2016.03.025(In Chinese).
Ma, H., Wang, X., & Wang, X. (1999). Mental health rating manual: The OSLON Marital Quality Questionnaire (pp. 153–156). Chinese Journal of Mental Health.
Marroquín, B. (2011). Interpersonal emotion regulation as a mechanism of social support in depression. Clinical Psychology Review, 31(8), 1276–1290. https://doi.org/10.1016/j.cpr.2011.09.005
Mason, C. A., Cauce, A. M., Gonzales, N., Hiraga, Y., & Grove, K. (1994). An ecological model of externalizing behaviors in african american adolescents: No family is an island. Journal of Research on Adolescence, 4, 639–655. https://doi.org/10.1207/s15327795jra0404_12
Mathew, S., Zhai, F., & Gao, Q. (2017). Social support and parental nurturance among asian indian families in the US: Mediating role of parenting self-efficacy. Journal of Family and Economic Issues, 38(3), 354–369. https://doi.org/10.1007/s10834-017-9530-y
McConnell, D., Breitkreuz, R., & Savage, A. (2011). From financial hardship to child difficultness: Main and moderating effects of perceived social support. Child Care Health and Development, 37(5), 679–691. https://doi.org/10.1111/j.1365-2214.2010.01185.x
Milgrom, J., Hirshler, Y., Reece, J., Holt, C., & Gemmill, A. W. (2019). Social support—a protective factor for depressed perinatal women? International Journal of Environmental Research and Public Health, 16(8), 1426. https://doi.org/10.3390/ijerph16081426
Noelle, M. St. Vil. (2015). A culture of mutual support: The impact of giving and receiving of practical and emotional support on African American marital satisfaction. Journal of Family Social Work, 18(2),78–89. https://doi.org/10.1080/10522158.2014.981909
Ostberg, M., & Hagekull, B. (2000). A structural modeling approach to the understanding of parenting stress. Journal of Clinical Child Psychology, 29(4), 615–625. https://doi.org/10.1207/S15374424JCCP2904_13
Overton, W. F., Molenaar, P. C. M., & Lerner, R. M. (2015). Handbook of child psychology and developmental science: Theory and method. John Wiley & Sons, Inc.
Pianta, R. C. (1992). Child-parent relationship scale (CPRS). University of Virginia Press.
Qadir, F., Khalid, A., Haqqani, S., & Medhin, G. (2013). The association of marital relationship and perceived social support with mental health of women in Pakistan. Bmc Public Health, 13(1), 1–13. https://doi.org/10.1186/1471-2458-13-1150
Ranson, K. E., & Urichuk, L. J. (2008). The effect of parent–child attachment relationships on child biopsychosocial outcomes: A review. Early Child Development and Care, 178(2), 129–152. https://doi.org/10.1080/03004430600685282
Rinaldi, C. M., & Howe, N. (2012). Mothers’ and fathers’ parenting styles and associations with toddlers’ externalizing, internalizing, and adaptive behaviors. Early Childhood Research Quarterly, 27(2), 266–273. https://doi.org/10.1016/j.ecresq.2011.08.001
Rosenstock, I. M., Strecher, V. J., & Becker, M. H. (1988). Social learning theory and the health belief model. Health Education Quarterly, 15(2), 175–183. https://doi.org/10.1177/109019818801500203
Sang, B., & Xi, J. (2005). A study on the effect mechanism of family ecosystems on development of children’s mental health. Psychological Development and Education, (1), 80–86. (In Chinese)
Sehmi, R., Maughan, B., Matthews, T., & Arseneault, L. (2020). No man is an island: Social resources, stress and mental health at mid-life. The British Journal of Psychiatry, 217(5), 638–644. https://doi.org/10.1192/bjp.2019.25
Shek, D. (2000). Parental marital quality and well-Being, parent-child relational quality, and chinese adolescent adjustment. The American Journal of Family Therapy, 28(2), 147–162. https://doi.org/10.1080/019261800261725
Taylor, R. J., Brown, E., Chatters, L. M., & Lincoln, K. D. (2012). Extended family support and relationship satisfaction among married, cohabitating, and romantically involved African Americans and Black Caribbeans. Journal of African American Studies, 16(3), 373–389. https://doi.org/10.1007/s12111-011-9205-y
Taylor, Z. E., Conger, R. D., Robins, R. W., & Widaman, K. F. (2015). Parenting practices and perceived social support: Longitudinal relations with the social competence of mexican-origin children. Journal of Latina-o psychology, 3(4), 193–208. https://doi.org/10.1037/lat0000038
Wang, M., Liu, L., & Wang, Y. (2010). The relationship between parental marital quality, parent-child attachment and young children’s anxiety. Chinese Journal of Clinical Psychology, 18(6), 802–805. https://doi.org/10.16128/j.cnki.1005-3611.2010.06.002(Chinese Journal).
Wang, S., Zhao, B., Wu, H., & Liu, W. (2022). The effects of marital quality on children’s pro-social behavior: The chain mediating model of parental positive emotion expression, parenting behavior and the gender difference. Psychological Development and Education, 38(3), 323–330. https://doi.org/10.16187/j.cnki.issn1001-4918.2022.03.03(In Chinese).
Wang, Y., & Feng, W. (2006). Main progress of research on parent-child relation. Chinese Journal of Special Education, (7),77–83. (In Chinese)
Xiao, S. (1994). Theoretical foundations and research applications of the Social Support Scale. Journal of Clinical Psychological Medicine, 4(2), 98–100. (In Chinese).
Xing, Y., Li, N., Tang, Y., & Liang, B. (2009). The relationships among married adult’s social support, coping styles and marital satisfaction. China Journal of Health Psychology, 17(5), 565–567. https://doi.org/10.13342/j.cnki.cjhp.2009.05.024(In Chinese).
Xu, H., & Hu, P. (2010). Correlation study on personality, social support and marital quality of young married women. China Journal of Health Psychology, 18(6), 680–682. https://doi.org/10.13342/j.cnki.cjhp.2010.06.032(In Chinese).
Yan, Z., Ren, J., Lin, W., & Wu, J. (2022). Parents’ perceived social support and children’s approaches to learning in rural China: A moderated mediation model. International Journal of Environmental Research and Public Health, 19(21), 14533. https://doi.org/10.3390/ijerph192114533
Yuan, X., & Fang, X. (2016). Origin family support and its relation to marital quality in chinese couples. Chinese Journal of Clinical Psychology, 24(3), 495–498. https://doi.org/10.16128/j.cnki.1005-3611.2016.03.025(In Chinese).
Yu, J. J., & Gamble, W. C. (2008). Pathways of influence: Marital relationships and their association with parenting styles and sibling relationship quality. Journal of Child and Family Studies, 17, 757–778. https://doi.org/10.1007/s10826-008-9188-z
Zhao, J., Liu, X., & Zhang, W. (2013). Peer rejection, peer acceptance and psychological adjustment of left-behind children: The roles of parental cohesion and children’s cultural beliefs about adversity. Acta Psychologica Sinica, 45(7), 797–810. (In Chinese).
Zhou, H., & Long, L. (2004). Statistical remedies for common method biases. Advances in Psychological Science, 12(6), 942–950. (In Chinese).
Zimet, G. D., Powell, S. S., Farley, G. K., Werkman, S., & Berkoff, K. A. (1990). Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. Journal of Personality Assessment, 55(3), 610–617. https://doi.org/10.1080/00223891.1990.9674095
Zimet, D. M., & Jacob, T. (2001). Influences of marital conflict on child adjustment: Review of theory and research. Clinical Child and Family Psychology Review, 4(4), 319–335. https://doi.org/10.1023/A:1013595304718
Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. https://doi.org/10.1207/s15327752jpa5201_2
Acknowledgements
We are grateful to all the children and parents who participated in this study. We have no conflicts of interest to disclose. We confirm that appropriate consideration has been made to protect intellectual property rights related to this work. There are no known obstacles to this publication in terms of intellectual property rights and publication time. Nevertheless, we confirm that any experimental work involving animals or human patients in this manuscript is conducted under ethical approval from all relevant institutions.
Funding
This research was funded by the National Social Science Foundation of China, grant number 19BSH049.
Author information
Authors and Affiliations
Contributions
Conceptualization, Z.Y. and Y.S.; methodology, Z.Y. and Y.S.; software, Y.S.; validation, Z.Y., Y.S. and W.L.; formal analysis, Z.Y. and Y.S.; investigation, Z.Y.; data curation, Z.Y. and Y.S.; writing—original draft preparation, Z.Y., Y.S. and W.L.; writing—review and editing, Z.Y. and W.L.; visualization, Y.S. and W.L.; supervision, Z.Y. and W.L.; project administration, Z.Y.; funding acquisition, Z.Y. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
No potential conflict of interest was reported by the authors.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (20220916. 06) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yan, Z., Yu, S. & Lin, W. Parents’ perceived social support and children’s mental health: the chain mediating role of parental marital quality and parent‒child relationships. Curr Psychol 43, 4198–4210 (2024). https://doi.org/10.1007/s12144-023-04625-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-04625-x