
Abstract
The current study examined multi-trajectories of aggression, hyperactivity/inattention and anxious/depressed problems, along with associated risk factors for trajectory group membership, using a person-centred approach. The sample included 2,857 children (50.1% males) enrolled in the Chilean Encuesta Longitudinal de la Primera Infancia cohort. Maternal reports using the Child Behaviour Checklist (CBCL) were completed when children were three, five and eleven years old. Information on risk/protective factors was collected using maternal reports and standardised assessments when children were aged three. Group-based multi-trajectory analysis was implemented. Results indicated that a five-group model best fit the data, with co-occurring symptoms across domains for all groups. Risk factors for membership of groups with the most elevated risk profiles included child sex, maternal age, single parent status, and maternal education, whilst children’s receptive language, maternal vocabulary skills, and not having early attendance in the educational system emerged as protective factors. These identified risk factors may be important targets for future intervention programmes in the Chilean context.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Accounting for individual variation in externalising and internalising problems across development, along with their multifactorial aetiology is essential for advancing understanding around the developmental heterogeneity in childhood psychopathology and developing early intervention strategies (Cicchetti, 2006). A growing body of research has examined longitudinal trajectories of externalising and internalising behaviours (Achenbach et al., 2016; Bevilacqua et al., 2021; Leban, 2021; Papachristou & Flouri, 2020). However, much of this work has modelled either externalising or internalising trajectories individually, often omitting outcomes for children displaying symptoms across both domains over time (Caspi & Moffit, 2018; Healy et al., 2022). The co-occurrence of externalising and internalising problems in childhood is frequent in both clinical and community samples (Achenbach et al., 2016; Healy et al., 2022; Isdahl-Troye et al., 2022; Willner et al., 2016). Compared to children exhibiting outcomes in a single domain, co-occurrence is also associated with greater risk of later maladaptive outcomes (e.g., mental illness, restriction in daily activities, social exclusion, delinquency, and suicidality (Dugre et al., 2019; Duprey et al., 2020; Murray et al., 2022; Winsper et al., 2020). Therefore, there is a growing need to model joint trajectories of externalising and internalising behaviours.
To date, nine studies have modelled joint trajectories of externalising and internalising problems (Dugre et al., 2019; Duprey et al., 2020; Fanti & Henrich, 2010; Girard, 2021; Murray, Eisner, et al., 2020; Nivard et al., 2017; Patalay et al., 2017; Shi et al., 2020; Winsper et al., 2020). Methodological differences notwithstanding, these findings provide robust evidence for the existence of co-occurring externalising and internalising problems across development. Most of these studies identified between four to six developmental trajectories, with all studies describing both a normative/low-risk and a high/chronic co-occurring group. Normative/low-risk trajectories were characterised by initially low stable or declining co-occurring externalising and internalising symptoms, typically comprising a large majority of the sampled population (i.e., 32.5-82.3%) (Duprey et al., 2020; Murray, Eisner, et al., 2020). In contrast, high/chronic co-occurring trajectories were characterised by moderate or high stability in both problem domains and denoted a much smaller percentage of the sampled populations (i.e., 3-7.7%) (Winsper et al., 2020; Girard, 2021). These two groups have been identified across studies investigating distinct developmental periods, ranging from early to late childhood (Fanti & Henrich, 2010; Girard, 2021; Patalay et al., 2017; Winsper et al., 2020), childhood to adolescence (Duprey et al., 2020; Murray, Eisner, et al., 2020; Nivard et al., 2017; Shi et al., 2020), and across adolescence only (Dugre et al., 2019).
Moreover, several additional trends have been identified in these studies. For example, externalising behaviours tend to decrease over time (Dugre et al., 2019; Fanti & Henrich, 2010; Girard, 2021; Murray, Eisner, et al., 2020; Nivard et al., 2017; Patalay et al., 2017; Shi et al., 2020; Winsper et al., 2020), particularly after the preschool period (Fanti & Henrich, 2010; Girard, 2021; Patalay et al., 2017). In contrast, internalising problems are likely to increase after the preschool stage (Dugre et al., 2019; Fanti & Henrich, 2010; Girard, 2021; Murray, Eisner, et al., 2020; Nivard et al., 2017; Patalay et al., 2017; Winsper et al., 2020), with a higher peak in adolescence (Dugre et al., 2019; Murray, Eisner, et al., 2020; Nivard et al., 2017). However, there is mixed evidence for ‘pure’ (i.e., problems that do not co-occur with others) and co-occurring trajectories of externalising and/or internalising behaviours. For example, only two studies reported a lack of support for ‘pure’ trajectories of either externalising or internalising behaviours from early to late childhood (Girard, 2021; Winsper et al., 2020). Conversely, two studies identified ‘pure’ externalising trajectories (Duprey et al., 2020; Shi et al., 2020), three described ‘pure’ internalising trajectories (Dugre et al., 2019; Murray, Eisner, et al., 2020; Nivard et al., 2017), and two reported both ‘pure’ externalising and internalising trajectories (Fanti & Henrich, 2010; Patalay et al., 2017).
Despite these advances in modelling co-occurring trajectories of externalising and internalising behaviours, all identified studies have been conducted with European or North American samples, with no studies examining potential co-occurring externalising and internalising trajectories within a South American context. Further, no studies to date have exclusively focused upon the co-occurrence of aggression, hyperactivity/inattention (externalising behaviours), and anxious depressed problems (internalising problems). These particular behaviours are amongst the most common childhood mental health difficulties (Egger & Angold, 2006), with population-based prevalence rates estimated at around 70% for aggression (when including both moderate desisting and high stable groups together) (Côté et al., 2006), around 21% and 20% for hyperactivity and inattention, respectively (when including elevated trajectories of hyperactivity or inattention and elevated trajectories of both) (Vergunst et al., 2019), and approximately 40% for anxious depressed symptoms (taking together moderate, high, increasing and decreasing groups) (Shore et al., 2018).
Antecedent factors
Externalising (e.g., aggression and hyperactivity/inattention) and internalising (e.g., anxious/depressed) behaviours have been associated with several risks and protective factors at the perinatal, child, and family levels. For perinatal factors, postnatal indicators such as low birth weight (Taylor et al., 2015), breastfeeding (Girard et al., 2018; Girard & Farkas, 2019), and maternal mental health (McAndrew, 2017; Morales et al., 2023) have been associated with offspring aggression, hyperactivity/inattention, and anxious depressed problems. Several potential mechanisms have been proposed for these associations, including neurodevelopmental immaturity and structural brain abnormalities at birth (Taylor et al., 2015), alongside psychological pathways such as maternal sensitivity and attunement to the infant’s needs (McAndrew, 2017).
With regard to child-level antecedents, sex has been extensively examined as a significant predictor. Boys are more likely to persistent higher levels of externalising behaviours over time (Sentse et al., 2017). Conversely, girls’ internalising symptoms tend to be more elevated initially and stable during adolescence (Jamnik & DiLalla, 2019; Morken et al., 2023). Sex differences can be explained via evolutionary (Archer, 2009) or social role (Chaplin et al., 2005) perspectives. Although both perspectives attribute social roles to males and females, such as boys being more active and girls being more prosocial, these theories differ regarding the causes of these role distinctions (Tremblay & Côté, 2019). Additionally, children’s language skills have been identified as a factor implicated in higher externalising and internalising problems across development. For example, studies using clinical samples reported that poorer language skills in childhood are associated with future increased anxiety, antisocial and aggressive behaviours (Beitchman et al., 2001; Conti-Ramsden et al., 2013), while population cohort samples suggest significant longitudinal associations between poor language and aggression, albeit with small effect sizes (Girard et al., 2014).
Concerning family antecedents, several maternal characteristics have been related to children’s externalising and internalising problems, such as adolescent pregnancy, single relationship status, and having low educational levels (Alavi et al., 2017; Farkas et al., 2023; Lee et al., 2020; Nagin & Tremblay, 2001). Maternal characteristics may cumulatively impact upon children’s outcomes given that combined multiple risk factors – rather than single features – are predictive of children’s behavioural outcomes (Atzaba-Poria et al., 2004). Furthermore, parental interaction styles have been associated with later problems in childhood (Gilliom & Shaw, 2004; Maciver & Girard, 2022), which may relate to the consecutive effects of attachment styles on development of self-regulatory skills, precipitating later mental health problems (Sroufe et al., 1999). Finally, from a demographic perspective socioeconomic status (SES) is of importance, whereby children from low-income homes are more likely to exhibit externalising outcomes (e.g., aggression, delinquency), and internalising problems (e.g., anxiety and depression) (Miller & Votruba-Drzal, 2017), although low SES has been described as more strongly associated with behavioural than emotional problems (Peverill et al., 2021). Three models have been described to explain these associations: family stress, resources and investment, and cultural pathways (Miller & Votruba-Drzal, 2017). The first model suggests that economic disadvantage affects children’s development through family economic stress, provoking parent psychological distress and impacting parent-child interactions (Elder, 1977). The second posits that less investment in materials and experiences that nurture children’s development, such as high-quality childcare, mental health services, and safe neighbourhoods, can be a risk factor for displaying later behavioural problems (Becker, 1991). Lastly, the cultural approach proposes that the lack of socioeconomic integration and the social isolation of more economically disadvantaged populations fails to ameliorate maladaptive behaviours that can precipitate suboptimal child behavioural outcomes (Lareau, 2011).
Chilean context
All previous studies modelling externalising and internalising trajectories together (Dugre et al., 2019; Duprey et al., 2020; Fanti & Henrich, 2010; Girard, 2021; Murray, Eisner, et al., 2020; Nivard et al., 2017; Patalay et al., 2017; Shi et al., 2020; Winsper et al., 2020), have been conducted in high-income western countries (i.e., Europe and the USA). Consequently, these findings may not translate to countries with different social and economic structures. The impact of social determinants of mental health on children’s developmental trajectories may change in different countries as a function of broader social structural conditions (Farkas et al., 2023). For example, Chile is a country showing stable economic progress over the last three decades and is on track to become a developed economy. Nevertheless, it has one of the highest Gini scores among OECD countries, with pronounced inequality levels across the population, with 21% of children living in poverty (Olivier et al., 2018), and adverse effects on children apparent in several psychological and social domains (Garcia & De Oliveira, 2011).
Although current social policies in Chile promote children’s mental health and wellbeing (Torres et al., 2018), several challenges remain for children’s early socioemotional development. The national quality of life and health survey (ENCAVI, 2006) reported that 30% of Chilean children under five years old did not attain expected developmental milestones, with lower-income families reporting the highest risk for developmental delays. These conclusions are supported by national routine data, whereby problems in socioemotional development are more prominent for children in the lowest socioeconomic levels (i.e., 11.8% of socioemotional problems in the highest income quintile versus 33.7% in the lowest income; Centro Microdatos [Microdata Centre], 2012). International comparisons also showed that prevalence rates of externalising and internalising problems in Chile are notably higher than other countries with different socioeconomic conditions. In a comparative study of 24 countries (Rescorla et al., 2011), Chile had the poorest indicators for externalising problems and rates for internalising problems in preschool children were in the top six countries studied. These results were replicated in a 15-country comparison using caregiver and teacher reports of children’s behavioural and emotional problems (Rescorla et al., 2012). Here, the rates of externalising problems in Chilean resident children were particularly pronounced, which may be related to differences in social determinants of mental health specific to each county. For instance, even if population level social determinants appear to be similar across populations, individual and societal experiences and meaning may vary according to their sociocultural backgrounds, with potential variation in mental health problems expression (e.g., prevalence rates, severity of symptoms) (Bornstein, 2010). For example, South American countries are described as collectivist cultures (Triandis, 2001), which attribute importance to social hierarchy and embeddedness. This may consequently impact upon children’s behavioural and emotional socialisation experiences and expectations. Similarly, using a cross-cultural perspective, Farkas and colleagues (2023) compared the prevalence and aetiology of emotional problems in preschool children from Chile and Scotland, concluding that Chilean children displayed higher emotional problems (i.e., 10.4%) and identifying specific risk factors relevant for this region only, including low maternal education and area of the family dwelling. Both factors are related to lower SES and family adversity, concluding that broader social determinants of mental health play an important role in the development of children’s emotional problems. Therefore, this contextually informed direction offers an alternative approach to data-driven global mental health research, enabling investigation of potential divergence in (1) children’s developmental trajectories of co-occurring externalising and internalising difficulties and (2) contextual risk and protective factors which may distinguish between groups.
Aims & hypotheses
Research modelling longitudinal trajectories of co-occurring aggression, hyperactivity/inattention, and anxious depressed problems, which are among the most prevalent problems in childhood, is needed to further our understanding of how these problems may co-occur in presentation from early to late childhood. Moreover, there is a particularly large need to explore these developmental trajectories in cohorts from South American countries, given the current scarcity of studies from this region and higher observed prevalence rates. Therefore, the current study had two aims. First, to examine multi-trajectories of aggression, hyperactivity/inattention, and anxious depressed problems from three to eleven years old in a Chilean population to enhance knowledge around potential differing developmental presentations and prevalence rates in a South American country. Second, to identify common versus specific risk and protective factors for group membership at the perinatal, child, and family levels. This is the first study to simultaneously address these two aims. Supported by previous studies modelling joint externalising and internalising trajectories (Dugre et al., 2019; Duprey et al., 2020; Fanti & Henrich, 2010; Girard, 2021; Murray, Eisner, et al., 2020; Nivard et al., 2017; Patalay et al., 2017; Shi et al., 2020; Winsper et al., 2020), it was expected that between four and six trajectory groups would best fit the data, with a modal prediction of a five-group model. It was anticipated that within the 5 group model, the following groups would emerge: (i) a low-risk group (low to no-problems), (ii) a normative group (moderate decreasing aggressive and hyperactivity/inattention problems after five years old and low but slightly increasing anxious depressed symptoms), (iii) two ‘pure’ groups (an elevated decreasing aggressive and hyperactivity/inattention group with no anxious depressed problems, and an increasing anxious depressed group with no aggressive or hyperactivity/inattention symptoms), and finally (iv) a high/chronic group (aggressive and hyperactivity/inattention and increasing anxious depressed). For the second aim, following a cumulative model (Atzaba-Poria et al., 2004), it was expected that a greater amount of risk factors at the perinatal, child, and family levels would be identified in high/chronic co-occurring group as compared to the normative group. Moreover, due to the importance of socioeconomic factors in Chile, it was anticipated that related family variables (e.g., health provisional system, maternal education) would be significant risk factors for membership in the high/chronic co-occurring group.
Methods
Participants
The current study was a secondary analysis of longitudinal data using the Encuesta Longitudinal de la Primera Infancia (ELPI – Longitudinal Survey of Early Infancy) cohort, a representative cohort of Chilean families from all regions of the country, conducted between 2010 and 2017. Data from waves 1 to 3 were used, modelling outcomes for children aged three, five and 11 years old. Initial inclusion criteria for this sample were children between 24 and 47 months old, when first assessed in 2010 (n = 6,034). This age range was selected because developmental differences are expected by the second and third years of life (Côté et al., 2006; Egger & Angold, 2006). Exclusion criteria were: child not living with their biological mother at the first wave (due to the requirement of antenatal and postnatal antecedents; n = 89), incomplete child behavioural assessment data (since three complete time points were required to accurately apply a quadratic polynomial term in the group-based modelling strategy; n = 2,673). To account for data loss, sensitivity analyses were conducted using all cases that met age inclusion and the biological mother exclusion criteria to ensure robustness of findings and examine any possible differences (See Appendix I). Furthermore, as the selected age range included more than one year of difference between participants (24–47 months old), there was an age overlap between waves 1 and 2. This could theoretically bias the time variation component in trajectory analysis as the same developmental stage would be modelled twice, both in waves 1 and 2. Accordingly, a criterion for age difference between both waves was generated. Although, it would be advantageous to have at least a one-year difference between both waves to ensure differences between developmental stages are more apparent, this resulted in a considerably reduced sample size (i.e., n = 1,982). Therefore, a threshold of at least six-months difference between waves 1 and 2 was selected, including children aged between 29 and 47 months old in 2010 (i.e., n = 415 cases lost). Sensitivity analyses were also conducted using the sample with a one-year difference between waves 1 and 2 (Appendix II).
The final sample included 2,857 families who participated in all three waves. Demographic characteristics of the excluded and included cohorts are displayed in Table 1. These analyses revealed significant differences across several perinatal, child, and family antecedents, including for example an underrepresentation of children not attending the school system, children whose mothers had higher maternal depressive symptoms, and children with younger mothers. Therefore, sampling weights (which were estimated according to the probability of selecting the sample) were added to the trajectory analysis to return the sample distribution back to the population characteristics, to improve generalisability of results (For a comprehensive explanation of ELPI’s sampling weights, see Behrman et al. (2010)).
Procedure
Ethical approval
for the ELPI cohort was granted by the Microdata Centre of the University of Chile (Centro Microdatos, Universidad de Chile) with written consent collected from caregivers and children aged seven or above before all data collection. Additional ethical approval was granted from the University of Edinburgh School of Health and Social Science Research Ethics Committee to conduct this study in January 2021. Data collection was divided into two stages: the socio-demographic interview stage and the assessment stage. The first contact with the family was established by the interviewer who conducted the socio-demographic questionnaire face to face. After the questionnaire was completed, the interviewer arranged another visit to proceed with the second assessment stage. In this second visit, a psychologist attended the house of the selected child and conducted the assessment stage for the child and the main caregiver (For complete details of ELPI design and procedures, see Behrman (2010)).
Measures
Children’s aggression, hyperactivity/inattention, and anxious/depressed symptoms
Children’s aggression, hyperactivity/inattention and anxious/depressed symptoms at approximately three, five, and 11 years old were assessed using maternal reports from the Child Behaviour Checklist (Achenbach & Rescorla, 2001). The CBCL is a screening tool assessing multiple behavioural and emotional difficulties in children aged one-and-a-half to five years old in the preschool version, and children aged six to 18 years old in the school-age version. The preschool version comprises 99 items classified into seven behavioural subscales, and the school version includes 112 items organised into eight behavioural subscales. Both CBCL versions measure two higher-order factors: internalising (emotionally reactive, anxious/depressed, somatic complaints, and withdrawn subscales) and externalising (attention problems, rule-breaking, and aggressive behaviour subscales), although to account for developmental changes some items differ across subscale versions. Mothers rated each item on a three-point Likert scale ranging from 0 (not true) to 2 (very or often true), with higher scores indicating more problematic behaviours. The Spanish language CBCL has been previously validated with Chilean samples, reporting good psychometric properties with Cronbach’s alpha coefficients of 0.88 for the internalising and 0.90 for the externalising scales (Lecannelier et al., 2014). In the current study, the preschool and school versions of the CBCL were administered according to children’s developmental stage at each wave. Thus, only identical or virtually identical items across both versions were used in this study to maximise comparability over time. Eight items were included from the aggression subscale (‘destroys things belonging to his family or others’, ‘disobedient’, ‘gets in many fights’, ‘physically attacks people’, ‘your child is stubborn, moody, irritable’, ‘screams a lot’, ‘temper tantrums or hot-tempered’, ‘demands a lot of attention’). Means and standard deviations across waves were: Wave 1 M = 6.72, SD = 3.69; Wave 2 M = 4.88, SD = 3.62; Wave 3 M = 2.31, SD = 2.34. Three items were included from the attention problems subscale (‘cannot concentrate or pay attention for a long time’, ‘cannot sit still, restless, or hyperactive’, ‘your child moves quickly from one activity to another/leave unfinished what begins’) with the following means and standard deviations: Wave 1 M = 3.87, SD = 1.57; Wave 2 M = 3.26, SD = 1.85; Wave 3 M = 1.74, SD = 1.57. Four items were included from the anxious/depressed subscale (‘too fearful or anxious’, ‘self-conscious or easily embarrassed’, ‘your child is too fearful’, ‘unhappy, sad, or depressed’), with the following means and standard deviations: Wave 1 M = 1.94, SD = 1.65; Wave 2 M = 1.79, SD = 1.64; Wave 3 M = 1.57, SD = 1.55. Combined scores were created for each subscale by summing item scores (See Appendices III & IV for Inter-item and subscale correlations at ages three, five and 11).
Antecedent factors
When children were three years old, mothers gave retrospective reports on perinatal and birth outcomes, including: birth weight (kilos), breastfeeding length (months), antenatal depression (yes/no), postnatal depression (yes/no). Child characteristics included: sex (male/female) and attendance at any educational system level (yes/no). Family antecedents included: maternal age at the birth of the selected child (≤ 21 years; yes/no), marital status (single/not single), maximum educational level primary school or less (yes/no), region (central/not central), and provisional health system (public/private; acting as a proxy for economic status given that private health access in Chile is associated with higher economic status and the public system with a lower family income; Becerril-Montekio et al., 2011). Standardised measures were used to assess children’s receptive language with the Spanish version of the Peabody Picture Vocabulary Test (TVIP: Test de Vocabulario en Imágenes Peabody; Dunn & Dunn, 1986), which has been adapted with Chilean samples, demonstrating very high internal consistency (K-R = 0.98) (Strasser et al., 2010). Maternal IQ was assessed using the vocabulary subscale of the Wechsler Intelligence Adult Scale 3rd version (WAIS-III) (Wechsler, 1981); adapted for use with Chilean samples (Hermosilla, 1982). Finally, at assessment ELPI research assistants completed the infant version of the Home Observation for Measurement of the Environment (HOME) (Bradley & Caldwell, 1984) using the responsivity (i.e., quality of verbal and physical reactions towards the child during the interview) and acceptance (i.e., reactions towards child misbehaviour) subscales.
Statistical analysis
As only some items from the CBCL were used, a three-factor confirmatory factor analysis was conducted to assess model fit. The Chi-square test is commonly used to assess the global fit of the model, although this value is usually significant in large sample sizes. Therefore, alternative fit measures including the root mean square error of approximation (RMSEA), the root mean square residual (SRMR), and the comparative fit index (CFI) were also used to assess model fit. Model fit indices showed that the proposed three-factor model provided a good fit to the data across all ages, indicating discriminant validity. Model fit indices, model specification, identification, and estimation are reported in Appendix V.
A person-centred approach was used to examine multi-trajectories of aggression, hyperactivity/inattention, and anxious/depressed problems. Variable-centred approaches have commonly been used to understand normative developmental change (Laursen & Hoff, 2006) since they assume that the population has common patterns of change over time (e.g., vocabulary development). This approach aims to report the average trajectories of normative development, recognising factors that predict variation from that average trajectory (Laursen & Hoff, 2006). On the other hand, the person-centred approach aims to model trajectory clusters within the population and detect variables that discriminate between these groups. This model works on the assumption that the population can be approximated by different groups and patterns of change over time, identifying clusters of people who function similarly at some level and in a distinctive way as compared to other people at the same level (Magnusson, 2003; Nagin, 2005). Thus, the person-centred approach is suitable when individuals are expected to follow diverse patterns of behaviour over time (Laursen & Hoff, 2006). Consequently, based on the current research aims – hypothesising that aggression, hyperactivity/inattention, and anxious/depressed problems would show heterogeneity across identified trajectories – a person-centred strategy was selected.
Group-based trajectory modelling was conducted, which uses finite mixture modelling to account for the heterogeneity of developmental trajectories within the population (Nagin, 2005). More precisely, multi-trajectory modelling was performed to jointly examine children’s aggression, hyperactivity/inattention, and anxious/depressed problems. This model extension allows the modelling of various subtypes of behaviours together, specifying an overall development profile across multiple dimensions (Nagin et al., 2016). Model selection was conducted in two stages: (i) determining the number of groups that best fit the data and (ii) defining the polynomial (i.e., growth) terms of each group. For the first stage, two to eight group models were estimated to compare model fit according to each model’s Bayesian Information Criteria (BIC) and the Akaike Information Criterion (AIC). A larger BIC and AIC (i.e., more positive) is indicative of a better fitting model (Nagin, 2005). The five to seven group models provided the best fit using the BIC and AIC criteria. However, the largest BIC statistic change occurred between group 4 and group 5, whereas there were more minimal changes between groups 5 to 7. This suggests that the main fit improvement occurred with the five-group model (Table 2). Moreover, inspection of each model’s graphs indicated that the models with more groups (i.e., 6 to 8 groups) parsed identified groups into similar subgroups with lower percentages of participants and of less theoretical importance. Consequently, considering the best fit improvement of the BIC and AIC statistics, coupled with the principle of parsimony, a five-group multi-trajectory model was selected as best capturing the distinctive features of the data. An additional sensitivity analysis was conducted to test if results differed using linear growth trajectories only to determine the number of groups. These results further supported the five-group selection (Appendix VI). Next, polynomial terms were fitted in the five-group multi-trajectory model, starting with quadratic, linear, and constant terms until each parameter estimate was statistically significant. Once the multi-trajectory model was adjusted with polynomial terms, Nagin (2005) suggests additional criteria to assess the fit of the selected model. This includes the average posterior probabilities for group membership by assigned trajectory group (greater than 70) and odds of correct classification (greater than 5). Both indices provided additional support in favour of the five-group multi-trajectory model (See Table 3 for indices of model fit and Appendix VII for parameter estimates).
After model selection, risk/protective factors measured at the first time points were entered directly into the multi-trajectory model estimation to keep the inherent latent structure of the trajectory groups. Analyses were performed Stata v17.0, with a statistical threshold of p = 0.05. The term significance is used in place of statistical significance hereafter.
Results
Group-based multi-trajectories
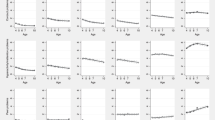
Five trajectory groups were identified, revealing different progressions of co-occurring aggression, hyperactivity/inattention and anxious/depressed problems. Group 1 (an estimated 30.3% of the cohort) was characterised by very low stable anxious/depressed problems and low decreasing aggression and hyperactivity/inattention problems from three to 11 years old. As preschool children are developmentally expected to display decreasing behavioural problems at this stage, this first group was labelled ‘normative’. Group 2 (an estimated 12.5% of the sampled population) labelled ‘low/moderate-high remitting’ was characterised by low levels of anxious/depressed problems at three years which decreased steadily until 11 years of age. Both aggression and hyperactivity/inattention problems started at moderate and high levels respectively and then decreased from three years onwards. By age 11, aggression, hyperactivity/inattention and anxious/depressed problems were virtually absent. Group 3 was the largest group (an estimated 38.9% of the cohort) and was labelled ‘low-stable/moderate-decreasing’. In this group, anxious/depressed problems were low and stable over time, while aggression and hyperactivity/inattention problems followed a linear declining trajectory from moderate levels at age three to low levels at age 11. In contrast to group 2, problems were initially lower and did not cease in late childhood. Moreover, anxious/depressed symptoms remained stable across time without a decreasing tendency. Group 4 (an estimated 15.9% of children) was characterised by initial moderate and slightly decreasing anxious/depressed symptoms and elevated levels of aggression and hyperactivity/inattention problems that declined towards late childhood. This group was, therefore, labelled ‘moderate/high decreasing’. Finally, Group 5 (an estimated 2.5% of the sampled population) was characterised by initial low anxious/depressed symptoms that increased linearly to moderate levels by age five and continued upwards until 11 years old, while aggression and hyperactivity/inattention problems were high and stable from early to late childhood. This group was, therefore, labelled ‘increasing/high-chronic’. Multi-trajectory groups are displayed in Fig. 1.

Multi-trajectories of aggression, hyperactivity/inattention and anxious/depressed problems from three to 11 years old
Antecedent factors for group membership
Risk and protective factors were modelled within the multi-trajectory estimation, using the normative trajectory group as the reference group. At the perinatal level, postnatal maternal depression decreased the likelihood of membership in group 2 relative to the normative reference group. No other perinatal antecedents were not significant for group membership. At the child level, male sex increased the likelihood of membership in all groups as compared to the reference group. Conversely, children with higher receptive language scores had a decreased likelihood of membership in all groups as compared to the normative group. Not attending formal education at age 3 resulted in a decreased likelihood of membership in the moderate/high decreasing (Group 4) and in the increasing/high chronic (Group 5) groups. At the family level, having a young mother (maternal age ≤ 21 years at childbirth) and single parent status increased the likelihood of membership in the low/moderate-high remitting (Group 2) and the moderate/high decreasing groups (Group 4). Low maternal educational level (primary school or less as the highest educational level) increased the likelihood of group membership in the moderate/high decreasing (Group 4) group only. Higher maternal vocabulary skills decreased children’s likelihood of membership in the low-stable/moderate-decreasing (Group 3), the moderate/high decreasing (Group 4), and the increasing/high chronic (Group 5) groups. Living in a non-central region increased the likelihood of membership in the low/moderate-high remitting (Group 2) group only. Finally, higher scores on the HOME responsivity subscale decreased the likelihood of membership in the low/moderate-high remitting (Group 2) group. See Table 4.
Discussion
The current study contributes to the emerging literature modelling developmental trajectories of co-occurring externalising (i.e., aggression and hyperactivity/inattention) and internalising (i.e., anxious/depressed) problems from early to late childhood using a group-based multi-trajectory modelling approach, whilst examining common versus specific risk/protective factors for group membership. Using the Chilean ELPI cohort, a nationally representative population-based cohort, findings indicated that a five-group model best captured the distinctive trajectory features of the data. Multi-trajectory analysis revealed developmental heterogeneity in the population, including one normative group and four groups with co-occurring externalising and internalising behavioural problems. All five groups showed differing levels of symptom severity and progressions of change over time, including decreasing, increasing, and stable problems. No evidence for ‘pure’ externalising or internalising trajectories were found. Moreover, whilst there were two common antecedents for membership in all groups relative to the normative group, most risk factors examined were specific to group membership.
Developmental heterogeneity in multi-trajectories
Findings partially supported the first hypothesis, identifying a five-group model. However, three of the five trajectory groups differed from our hypotheses. First, there was no support for a low-risk group, as all children displayed some level of problems in the externalising and internalising domains. This may have been attributable to the age range of children in the study. Developmental research suggests that behavioural problems are normative in preschool children given the developmental transformations occurring during this stage (e.g., mobility and autonomy) (Côté et al., 2006). Meanwhile, at this stage cognitive and emotional regulation skills are still developing, and this discrepancy may itself cause behavioural problems (Tremblay et al., 2004). This perspective is consistent with the normative group, with around 30% of the cohort exhibiting low stable internalising symptoms and low decreasing externalising problems between three and five years old. Notably, the normative group shows a stable trajectory of anxious/depressed symptoms, whereas other studies have reported that internalising problems tend to progressively increase from early childhood to the school period (Gilliom & Shaw, 2004). However, recent meta-analytic evidence suggests that > 50% of participants showed low or no depressive symptoms and that only a smaller proportion of participants in the adolescent period demonstrate increasing trajectories (Shore et al., 2018). This normative group has been identified in previous research jointly modelling externalising and internalising problems at similar age ranges (Fanti & Henrich, 2010; Girard, 2021; Patalay et al., 2017; Winsper et al., 2020).
Second, there was little evidence to support either a ‘pure’ externalising or internalising trajectory group as all five groups showed problems across aggressive, hyperactivity/inattention and anxious/depressed behaviours. In previous studies modelling co-occurring problems, only Girard (2021) and Winsper et al. (2020) also reported the absence of a ‘pure’ externalising or internalising trajectory group, whilst others reported only either ‘pure’ internalising (Dugre et al., 2019; Murray et al., 2020; Nivard et al., 2017) or ‘pure’ externalising (Duprey et al., 2020; Shi et al., 2020) trajectories. The absence of a ‘pure’ trajectory group challenges ‘classical’ models of psychopathology classification, which usually describe discrete and mutually exclusive categories of symptoms. There are several possible explanations for this variation. First, some models suggest that co-occurrence is a function of measurement overlap, resulting from the division of one underlying psychopathology construct (‘p-factor’) into separate domains (Caspi et al., 2014). Thus, ‘pure’ externalising or internalising symptoms are unlikely to appear when measuring different interrelated domains. However, the current study’s confirmatory factor analysis supported the proposed three-factor model (i.e., aggression, hyperactivity/inattention, anxious/depressed), indicating discriminant validity and suggesting co-occurrence here was not wholly attributable to measurement overlap. A second explanation is dependency across behaviours. Developmental cascade studies have shown that externalising problems can lead to internalising symptoms through psychosocial difficulties, such as peer rejection and academic failure (Flouri et al., 2019); and that internalising symptoms may affect attention, leading to externalising problems (Vaillancourt et al., 2013). The current study cannot infer directionality between behavioural problems, but considering the increasing/high chronic group, it could be that high and stable levels of aggression and hyperactivity/inattention lead to increasing anxious/depressed symptoms across childhood, supporting the assumption that dependency of behaviours contributes to co-occurrence. Future studies using developmental cascades within the ELPI cohort may help to explore this further. Lastly, the differentiation hypothesis, suggesting that development evolves from lack of- to increasing differentiation of behaviours, may inform the absence of ‘pure’ externalising and internalising trajectories in childhood (Nottelmann & Jensen, 1995). Here, co-occurrence could reflect a nonspecific expression of maladjustment; e.g. younger children may be displaying undifferentiated responses to environmental or internal stressors that will evolve into specific problems as they grow up (Nottelmann & Jensen, 1995 While this could explain why there were no ‘pure’ externalising or internalising trajectories from early childhood, it was not possible to directly test this in the current study, given that adolescent follow-up (when more differentiated behaviours would be expected) has not yet been collected in ELPI.
The presence of low/moderate-high remitting (Group 2), low-stable/moderate-decreasing (Group 3), and moderate/high decreasing (Group 4) groups was somewhat unexpected. The low/moderate-high remitting (Group 2) and low-stable/moderate-decreasing groups (Group 3) started with similar levels of problems in anxious/depressed and aggressive behaviours, at low and moderate levels respectively. The trajectory shape of the anxious/depressed symptoms was linear decreasing in the low/moderate-high remitting group (Group 2) and stable in the low-stable/moderate-decreasing group (Group 3). Hyperactivity/inattention problems started high in the low/moderate-high remitting group (Group 2) and moderate in the low-stable/moderate-decreasing group (Group 3), following a decreasing shape in both groups. The moderate/high decreasing group (Group 4) (15.9%) showed initial moderate and slightly decreasing anxious/depressed symptoms, with high decreasing symptoms in the aggression and hyperactivity/inattention problems that were at a moderate level when children were aged 11. In similar research, Murray et al. (2020) and Girard (2021) also used a group-based multi-trajectory approach to examine internalising and externalising problems, including ADHD and hyperactivity behaviours, respectively, in European-based cohorts. Both studies reported similar trajectories to the anxious/depressed and aggressive behaviours described in the current study; however, they identified an increasing ADHD and hyperactivity trajectory. In contrast, current results with the ELPI cohort revealed decreasing trajectories for the hyperactivity/inattention problems, with the exception of the increasing/high chronic group, which was high and stable. This difference between these cohorts and ELPI could be explained by the medicalisation of and intervention for hyperactivity/inattention problems in Chile. In 2009, a Chilean public policy aiming to expand access to regular education for students who required extraordinary resources incorporated attention and hyperactivity symptoms as part of an intervention program (MINEDUC, 2016). To be part of this intervention, children had to be diagnosed by a specialised doctor, which subsequently led increased ADHD diagnosis and use of psychopharmacology in primary schools. This integration policy and its associated intervention effect could help explain why hyperactivity/inattention problems were high at age three but decreased across the four identified trajectory groups within ELPI, given the high use of medication and additional supports offered to young children presenting with symptomology of ADHD. Future research focusing on timing, intervention exposure and prescribing could answer whether improvements are attributable to public health and educational policies in the Chilean context.
As anticipated, the analysis revealed a high chronic aggressive and hyperactivity/inattention and increasing anxious depressed trajectory group, which had the lowest prevalence rate of all groups (Group 5 = 2.5%). Levels of aggression and hyperactivity/inattention started high and remained stable through the school period. Conversely, anxious/depressed symptoms increased from moderate to high levels. This result is consistent with previous research with a similar developmental range, which has also reported a small group with high stable externalising and increasing internalising problems across childhood, although these studies found slightly higher prevalence rates of 3 − 7.7% (Fanti & Henrich, 2010; Girard, 2021; Patalay et al., 2017; Winsper et al., 2020). The presence of this increasing/high chronic group supports the position that a small percentage of children do not show a normative decline in aggression or hyperactivity/attention problems, following a pathway of persistent externalising problems through childhood (Côté et al., 2006; Tremblay et al., 2004).
Antecedent factors for group membership
The study’s second aim was to identify common versus specific risk/protective factors for group membership at the perinatal, child, and family levels. Two common factors predicted membership in all groups relative to the normative reference group. These antecedents were at the child level and included children’s sex and receptive language. Relative to females, boys had 1.81, 1.66, and 1.42 higher odds of belonging to the low/moderate-high remitting (Group 2), low-stable/moderate-decreasing (Group 3), and moderate/high decreasing (Group 4) groups, respectively. While the odds ratio was close to four-fold for membership in the increasing/high-chronic group (Group 5). These findings are in line with previous joint trajectories research, indicating that co-occurrence is more frequent amongst boys (Fanti & Henrich, 2010; Girard, 2021; Murray et al., 2020; Patalay et al., 2017; Shi et al., 2020). However, in the current study male sex was a common risk factor for all elevated groups, whereas in other studies it was found to be a specific risk factor for elevated groups only (Girard, 2021; Patalay et al., 2017). Furthermore, results indicate that receptive language skills were a protective factor for not belonging to groups with co-occurring symptoms. Specifically, for each point increase, the odds ratio of group membership decreased by 2%, 3%, 3%, and 4% for the low/moderate-high remitting (Group 2), low-stable/moderate-decreasing (Group 3), moderate/high decreasing (Group 4), and increasing/high-chronic (Group 5) groups, respectively. This finding extends previous research examining language skills as a significant factor for externalising problems (Conti-Ramsden et al., 2013; Girard et al., 2014) by adding its significant effect in co-occurring symptoms using a population cohort sample. If children can better express themselves and better understand verbal interactions with others, the likelihood of using substitute forms of communication (e.g., aggressive behaviours) should decline. Additionally, better language skills can help facilitate emotional identification and regulation, helping children to modulate and better understand their emotions, thereby decreasing potential internalising problems (Hentges et al., 2021).
Four factors were common for some groups only. At the child level, lack of early attendance in the school system was protective for belonging to the moderate/high decreasing (Group 4) and increasing/high-chronic (Group 5) groups. This was an unexpected finding since early attendance in educational centres has been described as a protective factor for both behavioural and emotional problems, with a gradient effect for low SES (Larose et al., 2021). On the other hand, the results align with other Chilean studies (Narea et al., 2022), suggesting that early school attendance is a risk factor for developing externalising problems. A potential explanation could be that in the Chilean preschool system, the teacher-child ratio is more than 20 children per teacher, resulting in classrooms with large groups of children and few adults. This could potentially reduce children’s individual attention, negatively impacting on children’s school adjustment and peer interactions, consequently increasing the risk for behavioural and emotional problems (Narea et al., 2022). Moreover, at the family level, several maternal characteristics were significant for group membership. Young maternal age and single parent status were risk factors for membership in the low/moderate-high remitting (Group 2) and moderate/high decreasing (Group 4) groups. These antecedents have been previously reported as significant factors for co-occurring externalising and internalising problems (Girard, 2021). Notably, Groups 2 and 4 exhibited similar trajectories across the three areas of difficulty (albeit with higher symptoms in Group 4), while the low-stable/moderate-decreasing (Group 3) and the increasing/high-chronic (Group 5) groups presented different longitudinal presentations with stable or increasing problems instead of decreasing. Thus, findings suggest that co-occurring decreasing externalising and internalising trajectories are more common amongst families with younger mothers and single parents. Lastly, maternal vocabulary skills were a protective factor for the low-stable/moderate-decreasing (Group 3), moderate/high decreasing (Group 4), and increasing/high-chronic (Group 5) groups. For each point increase in the vocabulary subscale, the odds for membership were reduced by 5%, 8%, and 12% for groups 3, 4, and 5, respectively.
Four factors were specific to group membership, including postnatal maternal depression, the HOME responsivity subscale, and region for the low/moderate-high remitting group (Group 2), and maternal education for the moderate/high decreasing group (Group 4). For the low/moderate-high remitting group (Group 2), postnatal maternal depression decreased the likelihood of membership. Depressed mothers may be exhibiting low sensitivity and attunement to the baby’s need in the postpartum period (McAndrew, 2017), which could be related to increased co-occurring externalising and internalising problems but time limited to the preschool stage only. Moreover, the odds of membership in the low/moderate-high remitting group (Group 2) decreased by 11% for each point increase in the HOME responsivity subscale, suggesting that the quality of verbal and physical reactions towards the child played a protective role against decreasing co-occurring externalising and internalising problems in prescool children. This is consistent with previous studies indicating that the home environment is associated with less risk for externalising and internalising problems (Fanti & Henrich, 2010; Gilliom & Shaw, 2004). Additionally, living in non-central areas of the country (i.e., south or north regions), increased the likelihood of membership in the low/moderate-high remitting group (Group 2), suggesting that more remote locations with poorer social connectedness or less resource access may increase the risk for children’s problems, albeit in the preschool period only. Lastly, maternal education had a larger effect for the moderate/high decreasing (Group 4) group, suggesting that lower maternal educational levels are a greater risk for higher-decreasing anxious/depressed, aggressive, and hyperactivity/inattentive problems. This association may be explained via lower maternal cognitive and language skills, which is consistent with results showing a higher risk for co-occurring problems when mothers have worse vocabulary abilities (Groups 3, 4 and 5). Other potential mechanisms for this association can be found in the lower income associated with lower educational levels, which may result in elevated maternal stress that can impact children’s development. For instance, a recent Chilean study tested associations between maternal education and children’s language and cognitive development, reporting that maternal stress, depression, and the quality of the home environment mediated this positive association (Telias et al., 2022). However, future studies should elucidate the specific pathways between maternal education and childhood behavioural and emotional problems.
According to the cumulative model, whereby the more risk children are exposed to, the more problem behaviours they will develop (Atzaba-Poria et al., 2004), it was expected that the high/chronic co-occurring group (Group 5) would show more risk factors in comparison to other groups. Surprisingly, the low/moderate-high remitting (Group 2) and moderate/high decreasing (Group 4) groups exhibited more associated risk factors than the high/chronic co-occurring group (Group 5). This result may reflect unobserved risk or protective factors specific to the increasing/high-chronic group (Group 5), that we were unable to capture. Notably, results showed overlap of antecedents common to groups 4 and 5, suggesting that elevated symptoms groups share similar features at the child and family levels. Additionally, variables associated with socioeconomic conditions (i.e., provisional health system, maternal education) were not associated with membership likelihood in the increasing/high-chronic group (Group 5) as was expected. However, considering the large national evidence emphasising the importance of broader socioeconomic determinants of mental health in childhood (Centro Microdatos, 2012; ENCAVI, 2006; Farkas et al., 2023 this result may reflect that the selected study variables were not fully able to capture the effect of socioeconomic inequalities. Therefore, studies should further explore differences between SES levels, social inequalities, resource access and their associations with co-occurring externalising and internalising problems. Finally, with the exception of postnatal depression for the low/moderate-high remitting (Group 2), no perinatal antecedents significantly predicted group membership. This is surprising, given previous research on co-occurring problems have reported significant associations with prenatal exposure to smoking, and low birth weight (Girard, 2021; Murray, Eisner, et al., 2020; Patalay et al., 2017). This discrepancy may relate to the measurement of these variables in ELPI, which were based on maternal retrospective report three years after the perinatal period, introducing a high risk of recall bias (Keenan et al., 2017).
Strengths and limitations
The current study has several strengths, including the use of the group-based multi-trajectory approach to jointly model aggression, hyperactivity/inattention and anxious/depressed problems from early to late childhood, using a large and representative birth cohort from Chile, and incorporating multilevel variables as predictors for group membership. Nevertheless, some limitations need consideration. First, combining the preschool and school versions of the CBCL resulted in item reduction due to non-identical items across waves. However, reduction was necessary to maximise comparability over time, ensuring observed changes were attributable to developmental change. Moreover, results of the confirmatory factor analysis showed that the three-factor model was a good fit for this data, indicating discriminant validity between subscales. Second, assessment of aggression, hyperactivity/inattention and anxious/depressed behaviours relied on maternal report, whereas reports from multiple informants with the combination of behavioural observations would have been optimal. That said, maternal reports are a commonly used and reliable method of assessing children’s behaviours (Shaw et al., 2003). Moreover, maternal reports were used to collect information on perinatal and demographic data. Future research should include links to administrative data or health service records to confirm information regarding these variables. Third, attrition between the entire ELPI cohort and the selected sample revealed several demographic differences that might affect population representativity. However, to overcome these disparities, sampling weights were used to bring the distribution back to the population characteristics, ensuring greater generalizability of findings. Fourth, there was a large developmental gap between five and 11 years old, limiting our understanding of any developmental changes during the primary school period. Finally, ELPI data were only available until children were 11 years old, thus critical developmental changes that may occur after that age, such as potential adolescent-onset groups were not modelled. Once new waves of ELPI are available, findings should be replicated to extend trajectories from early childhood to the adolescent period.
Study implications
Notwithstanding the mentioned limitations, our results could help guide improvements in early childhood public policies in Chile and other South American settings with similar social backgrounds. Specifically, longitudinal identification of groups showing high co-occurring problems and associated risk and protective factors is important for targeting children and families that may need greater support starting in early stages of development. All risks and protective factors found in this study are manifest in infancy or toddlerhood, suggesting clear implications for prevention targeted at early developmental periods. Importantly, prevention and intervention policies within mental health support programs should consider the co-occurrence of externalising and internalising problems as a rule and not an exception. This requires assessment of both externalising and internalising problem domains once one domain has been flagged. Further, current early childhood Chilean policies, such as Chile Crece Contigo (ChCC; Chile grows with you), could target early intervention programs based on risk signals such as boys with early attendance in the school system, who display low receptive language skills and were born to young single mothers with lower educational levels and vocabulary skills. The early identification of high-risk groups of children could facilitate timely support, reducing the potential for more severe co-occurring externalising and internalising symptoms across childhood. For instance, early educational interventions encouraging language development in early childhood – particularly for children with earlier school attendance – could be an effective strategy for preventing children from following elevated co-occurring externalising and internalising problem trajectories. Additionally, extra support (e.g., parenting workshops, educational support) can be offered to young single mothers who have lower educational achievements and vocabulary skills. Moreover, considering that the study provided evidence for the presence of externalising and internalising problems from the early years, which persisted across childhood, it is important to extend current national policies towards targeting childhood problems at earlier stages of development. For instance, the mental health support program from ChCC, which aims to identify and support socioemotional problems of children between five and nine years old, could target earlier developmental periods to prevent sustained presentation across childhood.
Data Availability
The data that support the findings of this study are available from the Ministerio de Desarrollo Social y Familia http://observatorio.ministeriodesarrollosocial.gob.cl/elpi-tercera-ronda.
References
Achenbach, T. M., Ivanova, M. Y., Rescorla, L. A., Turner, L. V., & Althoff, R. R. (2016). Internalising/externalising problems: Review and recommendations for clinical and research applications. Journal of the American Academy of Child and Adolescent Psychiatry, 55(8), 647–656. https://doi.org/10.1016/j.jaac.2016.05.012
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA Preschool-Age Forms & Profiles. University of Vermont, Research Center for Children, Youth, and Families
Alavi, N., Roberts, N., & DeGrace, E. (2017). Comparison of parental socio-demographic factors in children and adolescents presenting with internalising and externalising disorders. International Journal of Adolescent Medicine and Health, 29(2), https://doi.org/10.1515/ijamh-2015-0049
Archer, J. (2009). Does sexual selection explain human sex differences in aggression? The Behavioural and Brain Sciences, 32(3–4), 249–266. https://doi.org/10.1017/S0140525X09990951
Atzaba-Poria, N., Pike, A., & Deater-Deckard, K. (2004). Do risk factors for problem behaviour act in a cumulative manner? An examination of ethnic minority and majority children through an ecological perspective. Journal of Child Psychology and Psychiatry, 45(4), 707–718. https://doi.org/10.1111/j.1469-7610.2004.00265.x
Becerril-Montekio, V., Reyes, J. D., & Manuel, A. (2011). Sistema de salud de Chile. Salud Pública de México, 53, s132–s142
Becker, G. S. (1991). A treatise on the family. In Enl (Ed.), Gary S. Becker. Harvard University Press
Behrman, J., Bravo, D., & Urzúa, S. (2010). Encuesta Longitudinal de la Primera Infancia: Aspectos metodológicos y primeros resultados. Retrieved from http://observatorio.ministeriodesarrollosocial.gob.cl/elpi-primera-ronda
Beitchman, J. H., Wilson, B., Johnson, C. J., Atkinson, L., Young, A., Adlaf, E., Escobar, M., & Douglas, L. (2001). Fourteen-year follow-up of speech/language-impaired and control children: Psychiatric outcome. Journal of the American Academy of Child & Adolescent Psychiatry, 40(1), 75–82. https://doi.org/10.1097/00004583-200101000-00019
Bevilacqua, L., Kelly, Y., Heilmann, A., Priest, N., & Lacey, R. E. (2021). Adverse childhood experiences and trajectories of internalizing, externalizing, and prosocial behaviors from childhood to adolescence. Child Abuse & Neglect, 112, 104890–104890. https://doi.org/10.1016/j.chiabu.2020.104890
Bornstein, M. H. (2010). Handbook of cultural developmental science. Psychology Press
Bradley, R. H., & Caldwell, B. M. (1984). The HOME Inventory and family demographics. Developmental Psychology, 20(2), 315–320. https://doi.org/10.1037/0012-1649.20.2.315
Caspi, A., Houts, R. M., Belsky, D. W., Goldman-Mellor, S. J., Harrington, H., Israel, S., Meier, M. H., Ramrakha, S., Shalev, I., Poulton, R., & Moffitt, T. E. (2014). The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clinical Psychological Science, 2(2), 119–137. https://doi.org/10.1177/2167702613497473
Caspi, A., & Moffitt, T. E. (2018). All for one and one for all: Mental disorders in one dimension. The American Journal of Psychiatry, 175, 831–844. https://doi.org/10.1176/appi.ajp.2018.17121383
Centro Microdatos [Microdata Centre] (2012). Informe resultados evaluaciones. Segunda ronda. Encuesta Longitudinal de la Primera Infancia Retrieved from http://observatorio.ministeriodesarrollosocial.gob.cl/storage/docs/elpi/2012/Informe_Resultados_Evaluaciones_Test_2012.pdf
Chaplin, T. M., Cole, P. M., & Zahn-Waxler, C. (2005). Parental socialization of emotion expression: Gender differences and relations to child adjustment. Emotion Journal, 5(1), 80–88. https://doi.org/10.1037/1528-3542.5.1.80
Cicchetti, D. (2006). Development and psychopathology. Developmental psychopathology: Theory and method (2nd ed., 1 vol., pp. 1–23). John Wiley & Sons, Inc
Conti-Ramsden, G., Mok, P. L. H., Pickles, A., & Durkin, K. (2013). Adolescents with a history of specific language impairment (SLI): Strengths and difficulties in social, emotional and behavioural functioning. Research in Developmental Disabilities, 34(11), 4161–4169. https://doi.org/10.1016/j.ridd.2013.08.043
Côté, S., Vaillancourt, T., LeBlanc, J., Nagin, D., & Tremblay, R. (2006). The development of physical aggression from toddlerhood to pre-adolescence: A nation wide longitudinal study of canadian children. Journal of Abnormal Child Psychology, 34(1), 71–85. https://doi.org/10.1007/s10802-005-9001-z
Dugre, J. R., Dumais, A., Dellazizzo, L., & Potvin, S. (2019). Developmental joint trajectories of anxiety-depressive trait and trait-aggression: Implications for co-occurrence of internalising and externalising problems. Psychological Medicine, 50(8), 1338–1347. https://doi.org/10.1017/S0033291719001272
Dunn, L. M., & Dunn, L. (1986). Test de vocabulario imágenes Peabody: adaptación española. Mepsa Madrid
Duprey, E. B., Oshri, A., & Liu, S. (2020). Developmental pathways from child maltreatment to adolescent suicide-related behaviours: The internalising and externalising comorbidity hypothesis. Development and Psychopathology, 32(3), 945–959. https://doi.org/10.1017/S0954579419000919
Egger, H. L., & Angold, A. (2006). Common emotional and behavioural disorders in preschool children: Presentation, nosology, and epidemiology. Journal of Child Psychology and Psychiatry, 47(3–4), 313–337. https://doi.org/10.1111/j.1469-7610.2006.01618.x
Elder, G. H. (1977). Children of the Great Depression: Social change in life experience. Jr. University of Chicago Press. Glen H. Elder
ENCAVI (2006). Encuesta Nacional de Calidad de Vida y Salud. Retrieved from http://epi.minsal.cl/encuesta-encavi/
Fanti, K., & Henrich, C. (2010). Trajectories of pure and co-occurring internalising and externalising problems from age 2 to age 12: Findings from the National Institute of Child Health and Human Development Study of Early Child Care. Developmental Psychology, 46(5), 1159–1175. https://doi.org/10.1037/a0020659
Farkas, C., Girard, L. C., & MacBeth, A. (2023). Predictors of emotional problems in 5-year-old children: An international comparison between two cohorts in Chile and Scotland. Current Psychology, 42, 390–405. https://doi.org/10.1007/s12144-020-01336-5
Flouri, E., Papachristou, E., Midouhas, E., Ploubidis, G. B., Lewis, G., & Joshi, H. (2019). Developmental cascades of internalising symptoms, externalising problems and cognitive ability from early childhood to middle adolescence. European Psychiatry, 57, 61–69. https://doi.org/10.1016/j.eurpsy.2018.12.005
Garcia, B., & De Oliveira, O. (2011). Family changes and public policies in Latin America. Annual Review of Sociology, 37(1), 593–613. https://doi.org/10.1146/annurev-soc-081309-150205
Gilliom, M., & Shaw, D. S. (2004). Codevelopment of externalising and internalising problems in early childhood. Development and Psychopathology, 16(2), 313–333. https://doi.org/10.1017/s0954579404044530
Girard, L. C., Doyle, O., & Tremblay, R. E. (2018). Breastfeeding and externalising problems: A quasi-experimental design with a national cohort. European Child & Adolescent Psychiatry, 27(7), 877–884. https://doi.org/10.1007/s00787-017-1085-9
Girard, L. C., & Farkas, C. (2019). Breastfeeding and behavioural problems: Propensity score matching with a national cohort of infants in Chile. British Medical Journal Open, 9(2), e025058. https://doi.org/10.1136/bmjopen-2018-025058
Girard, L. C., Pingault, J. B., Falissard, B., Boivin, M., Dionne, G., & Tremblay, R. E. (2014). Physical aggression and language ability from 17 to 72 Months: Cross-lagged effects in a population sample. PLoS One, 9(11), e112185. https://doi.org/10.1371/journal.pone.0112185
Girard, L. C. (2021). Concomitant trajectories of internalising, externalising, and peer problems across childhood: A person-centred approach. Research on Child and Adolescent Psychopathology, 49(12), 1551–1565. https://doi.org/10.1007/s10802-021-00851-8
Healy, C., Brannigan, R., Dooley, N., Staines, L., Keeley, H., Whelan, R., Clarke, M., Zammit, S., Kelleher, I., & Cannon, M. (2022). Person-centered trajectories of psychopathology from early childhood to late adolescence. JAMA network open, 5(5), e229601. https://doi.org/10.1001/jamanetworkopen.2022.9601
Hentges, R. F., Devereux, C., Graham, S. A., & Madigan, S. (2021). Child language difficulties and internalizing and externalizing symptoms: A meta-analysis. Child Development, 92(4), e691–e715.
Hermosilla, M. (1982). La escala de inteligencia de wechsler para adultos (WAIS): Manual. Pontificia Universidad Católica de Chile. Facultad de Psicología
Isdahl-Troye, A., Villar, P., Domínguez-Álvarez, B., Romero, E., & Deater-Deckard, K. (2022). The development of co-occurrent anxiety and externalizing problems from early childhood: A latent transition analysis Approach. Research on Child and Adolescent Psychopathology, 50(4), 505–519. https://doi.org/10.1007/s10802-021-00865-2
Jamnik, M. R., & DiLalla, L. F. (2019). Health outcomes associated with internalising problems in early childhood and adolescence. Frontiers in Psychology, 10, 60–60. https://doi.org/10.3389/fpsyg.2019.00060
Keenan, K., Hipwell, A., McAloon, R., Hoffmann, A., Mohanty, A., & Magee, K. (2017). Concordance between maternal recall of birth complications and data from obstetrical records. Early Human Development, 105, 11–15. https://doi.org/10.1016/j.earlhumdev.2017.01.003
Lareau, A. (2011). Unequal childhoods: class, race, and family life / Annette Lareau (2nd edition, with an update a decade later. ed.). University of California Press
Larose, M. P., Côté, S. M., Ouellet-Morin, I., Maughan, B., & Barker, E. D. (2021). Promoting better functioning among children exposed to high levels of family adversity: The protective role of childcare attendance. Journal of Child Psychology and Psychiatry and Allied Disciplines, 62(6), 762–770. https://doi.org/10.1111/jcpp.13313
Laursen, B., & Hoff, E. (2006). Person-centred and variable-centred approaches to longitudinal data. Merrill-Palmer Quarterly, 52(3), 377–389. https://doi.org/10.1353/mpq.2006.0029
Leban, L. (2021). The effects of adverse childhood experiences and gender on developmental trajectories of internalizing and externalizing outcomes. Crime & Delinquency, 67(5), 631–661. https://doi.org/10.1177/0011128721989059
Lecannelier, F., Pérez Ewert, J. C., Groissman, S., Gallardo, D., Bardet, A. M., Bascuñan, A., & Rodríguez, J. (2014). Validación del inventario de conductas infantiles para niños de entre 1½-5 años (CBCL 1½-5) en la ciudad de Santiago de Chile. Universitas Psychologica, 13, 491–500. https://doi.org/10.11144/Javeriana.UPSY13-2.vici
Lee, J. O., Jeong, C. H., Yuan, C., Boden, J. M., Umaña-Taylor, A. J., Noris, M., & Cederbaum, J. A. (2020). Externalizing behavior problems in offspring of teen mothers: A meta-analysis. Journal of Youth and Adolescence, 49, 1146–1161
Maciver, L., & Girard, L. C. (2022). The association between paternal depression and adolescent internalising problems: A test of parenting style as a mediating pathway. Current Psychology (2022). https://doi.org/10.1007/s12144-022-03110-1
Magnusson, D. (2003). The person approach: Concepts, measurement models, and research strategy. New Directions for Child and Adolescent Development, 101, 3–23. https://doi.org/10.1002/cd.79
McAndrew, A. J. (2017). Maternal perinatal depression: Emotional development in offspring from infancy to adolescence. Early Child Development and Care, 189(1), 168–177. https://doi.org/10.1080/03004430.2017.1292398
Miller, P., & Votruba-Drzal, E. (2017). The role of family income dynamics in predicting trajectories of internalising and externalising problems. Journal of Abnormal Child Psychology, 45(3), 543–556. https://doi.org/10.1007/s10802-016-0181-5
MINEDUC (2016). Programa de integración escolar PIE. Retrieved from https://especial.mineduc.cl/wp-content/uploads/sites/31/2016/09/Manual-PIE.leyOK_.web_-1.pdf
Morales, M. F., Girard, L. C., Raouna, A., & MacBeth, A. (2023). The association of different presentations of maternal depression with children’s socio-emotional development: A systematic review. PLOS Global Public Health, 3(2), e0001649. https://doi.org/10.1371/journal.pgph.0001649
Morken, I. S., Viddal, K. R., von Soest, T., & Wichstrøm, L. (2023). Explaining the Female Preponderance in Adolescent Depression-A Four-Wave Cohort Study. Research on Child and Adolescent Psychopathology. https://doi.org/10.1007/s10802-023-01031-6
Murray, A. L., Booth, T., Auyeung, B., Eisner, M., & Ribeaud, D. O., I (2020). Outcomes of ADHD symptoms in late adolescence: Are developmental subtypes important? Journal of Attention Disorders, 24(1), 113–125. https://doi.org/10.1177/1087054718790588
Murray, A. L., Eisner, M., Nagin, D., & Ribeaud, D. (2020). A multi-trajectory analysis of commonly co-occurring mental health issues across childhood and adolescence. European Child & Adolescent Psychiatry. https://doi.org/10.1007/s00787-020-01679-1
Murray, A. L., Nagin, D., Obsuth, I., Ribeaud, D., & Eisner, M. (2022). Young adulthood outcomes of joint mental health trajectories: A group-based trajectory model analysis of a 13-year longitudinal cohort study. Child Psychiatry & Human Development, 53(5), 1083–1096. https://doi.org/10.1007/s10578-021-01193-8
Nagin, D. (2005). Group-based modeling of development. Cambridge, Mass: Harvard University Press
Nagin, D., Jones, B., Passos, V. L., & Tremblay, R. E. (2016). Group-based multi-trajectory modeling. Statistical Methods in Medical Research, 27(7), 2015–2023. https://doi.org/10.1177/0962280216673085
Nagin, D., & Tremblay, R. E. (2001). Parental and early childhood predictors of persistent physical aggression in boys from kindergarten to high school. Archives of General Psychiatry, 58(4), 389–394. https://doi.org/10.1001/archpsyc.58.4.389
Narea, M., Cumsille, P., & Allel, K. (2022). The impact of time of entrance to center-based care on children’s general, language, and behavioral development. International Journal of Behavioral Development, 46(4), 278–285. https://doi.org/10.1177/0165025422108961
Nivard, M. G., Lubke, G. H., Dolan, C. V., Evans, D. M., Pourcain, S., Munafo, B., M. R., & Middeldorp, C. M. (2017). Joint developmental trajectories of internalising and externalising disorders between childhood and adolescence. Development and Psychopathology, 29(3), 919–928. https://doi.org/10.1017/S0954579416000572
Nottelmann, E. D., & Jensen, P. S. (1995). Comorbidity of Disorders in children and adolescents. In T. H. Ollendick, & R. J. Prinz (Eds.), Advances in clinical child psychology (pp. 109–155). Springer US
Olivier, T., Thomas, M., Yajna, G., & Ilya, K. (2018). Child poverty in the OECD: Trends, determinants and policies to tackle it. In: OECD Publishing
Papachristou, E., & Flouri, E. (2020). Distinct developmental trajectories of internalising and externalising symptoms in childhood: Links with mental health and risky behaviours in early adolescence. Journal of Affective Disorders, 276, 1052–1060. https://doi.org/10.1016/j.jad.2020.07.130
Patalay, P., Moulton, V., Goodman, A., & Ploubidis, G. B. (2017). Cross-domain symptom development typologies and their antecedents: Results from the UK millennium cohort study. Journal of the American Academy of Child and Adolescent Psychiatry, 56(9), 765–776e762. https://doi.org/10.1016/j.jaac.2017.06.009
Peverill, M., Dirks, M. A., Narvaja, T., Herts, K. L., Comer, J. S., & McLaughlin, K. A. (2021). Socioeconomic status and child psychopathology in the United States: A meta-analysis of population-based studies. Clinical Psychology Review, 83, 101933. https://doi.org/10.1016/j.cpr.2020.101933
Rescorla, L., Achenbach, T., Ivanova, M., Bilenberg, N., Bjarnadottir, G., Denner, S., et al. (2012). Behavioural/emotional problems of preschoolers: Caregiver/teacher reports from 15 societies. Journal of Emotional and Behavioural Disorders, 20(2), 68–81. https://doi.org/10.1177/1063426611434158
Rescorla, L., Achenbach, T., Ivanova, M., Harder, V., Otten, L., Bilenberg, N., et al. (2011). International comparisons of behavioural and emotional problems in preschool children: Parents’ reports from 24 societies. Journal of Clinical Child & Adolescent Psychology, 40(3), 456–467. https://doi.org/10.1080/15374416.2011.563472
Sentse, M., Prinzie, P., & Salmivalli, C. (2017). Testing the direction of longitudinal paths between victimization, peer rejection, and different types of internalising problems in adolescence. Journal of Abnormal Child Psychology, 45(5), 1013–1023. https://doi.org/10.1007/s10802-016-0216-y
Shaw, D. S., Gilliom, M., Ingoldsby, E. M., & Nagin, D. S. (2003). Trajectories leading to school-age conduct problems. Developmental Psychology, 39(2), 189–200. https://doi.org/10.1037//0012-1649.39.2.189
Shi, Q., Ettekal, I., Deutz, M. H. F., & Woltering, S. (2020). Trajectories of pure and co-occurring internalising and externalising problems from early childhood to adolescence: Associations with early childhood individual and contextual antecedents. Developmental Psychology, 56(10), 1906–1918. https://doi.org/10.1037/dev0001095
Shore, L., Toumbourou, J. W., Lewis, A. J., & Kremer, P. (2018). Review: Longitudinal trajectories of child and adolescent depressive symptoms and their predictors - a systematic review and meta-analysis. Child and Adolescent Mental Health, 23(2), 107–120. https://doi.org/10.1111/camh.12220
Sroufe, L. A., Carlson, E. A., Levy, A. K., & Egeland, B. (1999). Implications of attachment theory for developmental psychopathology. Development and Psychopathology, 11(1), 1–13. https://doi.org/10.1017/s0954579499001923
Strasser, K., Larraín, A., López de Lérida, S., & Lissi, M. R. (2010). La comprensión narrativa en edad preescolar: Un instrumento para su medición. Psykhe, 19(1), 75–87. https://doi.org/10.4067/S0718-22282010000100006
Taylor, H. G., Margevicius, S., Schluchter, M., Andreias, L., & Hack, M. (2015). Persisting behavior problems in extremely low birth weight adolescents. Journal of Developmental and Behavioural Pediatrics, 36(3), 178–187. https://doi.org/10.1097/DBP.0000000000000139
Telias, A., Narea, M., & Abufhele, A. (2022). A mediation analysis to disentangle relations between maternal education and early child development. International Journal of Behavioral Development, 46(6), 568–575. https://doi.org/10.1177/01650254221108143
Torres, A., Lopez Boo, F., Parra, V., Vazquez, C., Segura-Pérez, S., Cetin, Z., & Pérez-Escamilla, R. (2018). Chile Crece Contigo: Implementation, results, and scaling-up lessons. Child: care health and development, 44(1), 4–11. https://doi.org/10.1111/cch.12519
Tremblay, R. E., & Côté, S. M. (2019). Sex differences in the development of physical aggression: An intergenerational perspective and implications for preventive interventions. Infant Mental Health Journal, 40(1), 129–140. https://doi.org/10.1002/imhj.21760
Tremblay, R. E., Nagin, D. S., Seguin, J. R., Zoccolillo, M., Zelazo, P. D., Boivin, M., & Japel, C. (2004). Physical aggression during early childhood: Trajectories and predictors. Pediatrics, 114(1), e43–e50. https://doi.org/10.1542/peds.114.1.e43
Triandis, H. C. (2001). Individualism-collectivism and personality. Journal of Personality, 69(6), 907–924. https://doi.org/10.1111/1467-6494.696169
Vaillancourt, T., Brittain, H. L., McDougall, P., & Duku, E. (2013). Longitudinal links between childhood peer victimization, internalising and externalising problems, and academic functioning: Developmental cascades. Journal of Abnormal Child Psychology, 41(8), 1203–1215. https://doi.org/10.1007/s10802-013-9781-5
Vergunst, F., Tremblay, R. E., Galera, C., Nagin, D., Vitaro, F., Boivin, M., & Cote, S. M. (2019). Multi-rater developmental trajectories of hyperactivity-impulsivity and inattention symptoms from 1.5 to 17 years: A population-based birth cohort study. European Child & Adolescent Psychiatry, 28(7), 973–983. https://doi.org/10.1007/s00787-018-1258-1
Wechsler, D. (1981). The psychometric tradition: Developing the Wechsler adult intelligence scale. Contemporary Educational Psychology
Willner, C. J., Gatzke-Kopp, L. M., & Bray, B. C. (2016). The dynamics of internalising and externalising comorbidity across the early school years. Development and Psychopathology, 28(4pt1), 1033–1052. https://doi.org/10.1017/S0954579416000687
Winsper, C., Bilgin, A., & Wolke, D. (2020). Associations between infant and toddler regulatory problems, childhood co-developing internalising and externalising trajectories, and adolescent depression, psychotic and borderline personality disorder symptoms. Journal of Child Psychology and Psychiatry and Allied Disciplines, 61(2), 182–194. https://doi.org/10.1111/jcpp.13125
Funding
This work was supported by the National Agency for Research and Development (ANID)/ Scholarship Program / DOCTORADO BECAS CHILE/2019–72200120.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors have no competing interests to declare that are relevant to the content of this article.
Informed Consent Statement
Informed consent was obtained from the children?s parents included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Morales, M.F., MacBeth, A., Nagin, D. et al. Developmental trajectories of aggression, hyperactivity/inattention, and anxious depressed mood: co-occurring problems within a chilean context. Curr Psychol 43, 3928–3943 (2024). https://doi.org/10.1007/s12144-023-04530-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-04530-3