
Abstract
This study focuses on Intensive Care Units (ICU) and aims to test whether daily job demands are related to daily emotional exhaustion and secondary traumatic stress (STS) after work through the experience of passion at work and whether personal resources in ICU, such as empathy and self-compassion, moderate these relationships. A diary study was designed to assess day-level job demands, passion, empathy, self-compassion at work; and day-level emotional exhaustion and STS after work. The sample was 97 healthcare workers from ICU from different Spanish hospitals being selected by the snowball technique. This sample was assessed 5 days x two moments per day through a diary questionnaire. The multilevel analysis showed a negative mediational effect of harmonious passion between daily job demands and both emotional exhaustion and STS. Also, in predicting emotional exhaustion, a moderator effect of empathy on harmonious passion was found, as well as a moderator effect of self-compassion on obsessive passion. In predicting STS, a direct positive effect was found in empathy. Our findings highlight the vocational work of these healthcare workers, considering job demands as challenging and enhancing their harmonious passion to overcome the drawbacks. Moreover, empathy revealed to have a negative effect whereas self-compassion the contrary. Thus, increase the awareness on these personal resources and how to train them could be considered as valuable preventative measures.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Intensive Care Unit (ICU) healthcare workers are likely to suffer from burnout due to the high job demands they may face, considered as a syndrome of exhaustion, a cynical attitude toward work and a lack of sense of self-efficacy at work (Ballester-Arnal et al., 2016; Van Mol et al., 2015). Healthcare workers of ICU encounter job demands such as long shifts, life or death issues, crucial decision-making (van Mol et al., 2018), or are exposed to suffering and death cycle (Epp, 2012; Franklin, 2020). In this context, healthcare workers are exposed not only to feel burn-out but also to suffer job-related hazards that may generate a secondary exposure to stressful and traumatic events. This indirect exposure increases the likelihood of suffering secondary traumatic stress (STS) as well, considered as the physical and psychological distress in caregivers (Kelly, 2020; Wang et al., 2020). Literature of ICU has revealed that the risk of burnout could range from 6 to 47% (Chuang et al., 2016), whereas for STS ranges from 17% to 38.5%, (Van Mol et al., 2015).
Despite the undeniable importance of these negative outcomes, there are only a few empirical studies that focused comparatively on burnout and STS (Cieslak et al., 2014). Additionally, the vast majority of these studies use cross-sectional designs, so further research is needed that overcomes their drawbacks (Kelly, 2020; Shoji et al., 2015). Although authors suggest several emotional difficulties for healthcare workers on a daily basis (Blanco-Donoso et al., 2017), there is a lack of diary studies deepening into the effect of daily job demands, specifically in ICU context. In addition, findings revealed that especially pediatric ICU are more at risk of developing both burnout and STS (Austin et al., 2019), but only a few studies had provided empirical data and neither of them by a daily approach. According to that, we aim to contribute to improving models of both burnout and STS in ICU following a daily approach, attending specifically to daily job demands and personal experiences such as their passion at work and resources that healthcare workers may use in this health contexts such as empathy and self- compassion. In this sense, we aim to contribute to the existing literature studying passion at work from this daily approach attending to the distinction of the two types (i.e. harmonious and obsessive passion; Vallerand et al., 2003; Vallerand, 2008) and how the personal resources need for these professionals may interact with this passion. Finally, this study allows us to boost future preventative measures for the specific risky ICU context, which undoubtedly has a direct impact on the quality of caring for those healthcare workers (Gómez-Salgado et al., 2019). These preventative models stand out especially during this crisis time caused by COVID-19 that is directly impacting on healthcare professionals’ well- being (Giusti et al., 2020).
Burnout and secondary traumatic stress (STS)
Burnout has been deeply studied in many fields (Demerouti et al., 2003) and gain special importance when it comes to healthcare workers (Ortega-campos et al., 2019), concretely in this pandemic times (Luceño-Moreno et al., 2020). Among healthcare workers, the emotional exhaustion dimension stands to be the best indicator of burnout (Cieslak et al., 2014; Donahue et al., 2012), referring to the process of feeling drained out and extreme fatigued (Maslach, 2003). For this reason, we are focusing on emotional exhaustion to refer to burnout. Recent studies remark ICU context as a risky field for developing emotional exhaustion (van Mol et al., 2018), following the Job-Demands and Resource (JD-R) model.
The JD-R model has received enormous support to explain how job demands directly impact on job strain and, particularly, emotional exhaustion (Bakker & Demerouti, 2007, 2017; Bakker et al., 2004). Job demands are considered as those “physical, social, organizational aspects of the job that require sustained physical or mental effort and are therefore associated with certain physiological and psychological costs (e.g. exhaustion)” (Demerouti et al., 2001, p. 501). Due to the high job demands presented in ICU settings, such as high workloads, time and social pressure, urgent decision making and traumatic tasks (e.g. suffering cycle of children or youth people) (Colville et al., 2017; Embriaco et al., 2007), we hypothesized its relationship with emotional exhaustion.
In regard to STS, this outcome is considered as the stress response resulting from helping others who suffer from any traumatic event (Dominguez-Gomez & Rutledge, 2009; Figley, 1995). STS has been thoroughly studied in some nurse populations, e.g. psychiatric (Mangoulia et al., 2015), oncology (Ortega-campos et al., 2019) and emergency department (Morrison & Joy, 2016), but little is known specifically in ICU context (Cieslak et al., 2014; Van Mol et al., 2015). However, job-related demands specifically in ICU, involve traumatic content related to the patient’s critical care (Sacco et al., 2015). Consequently, dealing with these specific job demands may involve an exposure to traumatic events, linked with the task of “caring for individuals” (Kelly, 2020), which has been associated with an increase in STS (Shoji et al., 2015; Van Mol et al., 2015). Following the JD-R theory, these job demands may lead to experience stress but, in this case, as the course of caring for the trauma (Kelly, 2020). Additionally, when it comes to both emotional exhaustion and STS, experts highlight that both are highly related to the daily rigorous work (Wang et al., 2020), that could be the high workload, time and social pressure, and traumatic tasks in ICU settings (Chuang et al., 2016).
Moreover, authors suggest that even the more passionate workers, which become highly engaged in their job, may experience negative emotions of being emotionally drained out and fatigued (Donahue et al., 2012). This fact arises the attention paid to passion at work as personal experience, which may distinguish who are more likely to develop exhaustion (Donahue et al., 2012; Birkeland et al., 2018), and in turn, STS (Moreno-Jiménez et al., 2020). Vallerand’s et al. model (2003) and Vallerand (2008) allows us to better understand its influence on healthcare workers’ well-being.
The dualistic model of passion at work
Up to now, several studies have pointed out passion at work as a personal inclination which creates a sense of identity through work, and workers are fully engaged to invest time and effort on it (Trépanier et al., 2014). This passion gains importance especially in those jobs, which imply a great investment of time in emotionally-demanding tasks, such as healthcare professions (Tang et al., 2019). The majority of these professionals set work as a central feature which pushes them to continue investing resources at work (Ho & Astakhova, 2018). Surprisingly, this passion is normally linked to challenging work, which may activate this need to invest in it (Amarnani et al., 2019). Moreover, previous findings suggest that high job demands combined with high resources may lead to work engagement (Bakker & Albrecht, 2018) and this work engagement has been widely tested as a construct that is highly similar to passion at work, especially regarding their relationship with well-being and related outcomes (Birkeland & Buch, 2015). In this sense, current findings in ICU revealed that job demands posed in ICU settings (e.g. workload) are related to work engagement (van Mol et al., 2018), and findings in the general work context revealed that the more workers use their strength at work, the more they will like and love their work, thus experiencing more passion at work (Dubreuil et al., 2014). Furthermore, authors such as Amarnani et al. (2019) support the idea that those work contexts that involve challenge and vocational work, are those more likely to use this passion as an resource-intensive (Perrewé et al., 2014). In this sense, Perrewé et al. (2014) pointed out that passion is more than feeling affect towards work, as this passionate feeling is linked to specific work activities. In spite of the lack of scientific literature clearly establishing how job demands may predict passion, we hypothesized that specifically the job demands presented in the ICU could play a role concerning this passion towards healthcare professions. Thus, the job demands in ICU context, linked to the need of developing a high-quality job in the health context, might be the predictors to activate these resources investment to accomplish their caring duties and their passionate behaviours, according to Houlfort et al. (2014).
On the contrary, passion at work can turn out to be a personal demand, following JD-R model, with specific daily behaviors toward one’s work (e.g. spend more time working, rumination thoughts, increase your effort in a work-related task, flow experiences). Specifically, personal demands are defined as “the requirement the individuals set for their own performance and behaviour that force them to invest effort in their work” (Barbier et al., 2013, p.751). According to Vallerand et al. (2003) and Vallerand (2008), those passionate workers would set work as a core component in their lives, and they would freely invest more time, effort, and resources at work (Birkeland & Buch, 2015). To understand how job demands may trigger this passion for work and this may predict exhaustion and STS, we used the Conservation of Resources (COR) theory (Hobfoll, 2001).
The COR theory suggests that exposure to job-related demands may involve a loss of resources, which, in turn, may boost the development of specific negative outcomes. Recent findings on this theory support that in work settings in which the investments, or indeed, demands, are prolonged, passion at work play a role giving valued resources and, in some way, preventing from this loss of resources due to the need of maintaining them along time (Amarnani et al., 2019). However, despite this statement, these studies have not deepened into this process whether job demands predict passion for work as a loss of resources and whether this may lead to negative outcomes, such as exhaustion and STS, although it has been suggested. In this sense, high job demands presented in ICU (e.g. need of attending to patients without time of recovery, time pressure with urgent decision making throughout the shift and social pressure related to keep a high-quality job, among others) may activate their passion at work, as challenging tasks, and consequently, differentiated profiles which may lead to different outcomes. Thus, it seems relevant to distinguish between the two types of passionate workers (Vallerand et al., 2003; Vallerand, 2008).
On the one hand, harmonious passion means that one loves his/her job, the job occupies a significant space, but can keep the control over the work (Mageau & Vallerand, 2007). These harmoniously passionate workers feel the pleasure that derives from the work-related tasks, but they will be able to continue with their personal life without suffering (Donahue et al., 2012). Passionate employees may experience high ICU-related demands as challenging and gratifying and make heavy investments in work because they love what they do (Houlfort et al., 2018). For this reason, this passion has been associated with positive outcomes, such as recovery and job satisfaction (Jowett et al., 2013), which, in turn, involve less emotional exhaustion (Donahue et al., 2012) and could be a protecting factor for STS (Moreno-Jiménez et al., 2020). According to the COR theory, this passion may allow healthcare workers to keep their resources in order to properly deal with high job-related demands (Amarnani et al., 2019). Current studies supported that harmonious passion could mediate between the job demands (i.e. strength use at work) and positive outcomes (i.e. subjective vitality) (Dubreuil et al., 2014), considering this subjective vitality as the feeling of being energetic and alive, contrary to emotional exhaustion (Kilroy et al., 2020). So that, we hypothesized that:
-
Hypothesis 1: Daily harmonious passion at work is expected to mediate the relationship between daily job demands and daily emotional exhaustion as well as secondary traumatic stress after work.
On the other hand, obsessive passion has been positively associated with outcomes such as workaholic behaviors, work/life conflict, less recovery and problems with disengaging from work (Lavigne et al., 2014). The obsessively passionate worker may feel an urge to continue working despite the negative consequences they may experience (Amarnani et al., 2019). Previous studies tested the mediating role of this obsessive passion in predicting symptomatology related to exercise dependence, in which the self-regulation acting through the obsessive passion makes more likely to continue practicing exercise and generate an unbalanced lifestyle (Parastatidou et al., 2014). In the highly demanding ICU context, the inner pressure to get a high-quality job and get external rewards could be even stronger, making the obsessively passionate worker to do heavier investments on work (Houlfort et al., 2014), what involves a greater loss of specific resources to deal with job-related demands, according to COR theory (Amarnani et al., 2019). Thus, this may be associated with more exhaustion (Vallerand et al., 2010). To the best of our knowledge, there are few studies focused on that passion and STS, and they pointed out to be a risk factor as well (Moreno-Jiménez et al., 2020). Thus, we hypothesize as follows:
-
H.2 Daily obsessive passion at work is expected to mediate the relationship between daily job demands and daily emotional exhaustion as well as secondary traumatic stress after work.
The role of personal resources
Although we discussed that the high daily job demands within the ICU context make healthcare workers more passionate in their work which consequently consumes their daily energy (daily exhaustion) and increases the risk to experience STS, we still need to consider crucial personal resources which play a key role in the healthcare context. More specifically, Amarnani et al. (2019) establish career adaptability as the variable related to the adaptation to complex and demanding occupational challenges, but being mainly focused on employees of high demanding private organizations. In contrast, healthcare professionals’ motives could be outstandingly different from those workers of private institutions, as their vocation is more related to passion for caring (Gómez-Salgado et al., 2019). In this sense, the emotional demanding occupational context of ICU may activate these passionate behaviors that could interact with other resources more related to caring, i.e. empathy and self-compassion (Raab, 2014). Current findings place emphasis on these personal resources in ICU (i.e. empathic abilities) to deepen into the differences in responding to job-related demands (van Mol et al., 2018). Van Mol et al. (2018) supported that the healthcare workers in ICU are seemingly exposed to the job-demands, so that to study the personal resources displayed seems relevant to test the outcomes associated, specifically when these healthcare workers may show different levels of work engagement. Besides, Bakker and Sanz-Vergel (2013) stated that challenging demands in nursing work are related to higher personal resources displayed in order to accomplish their duties. Hence, according to the JD-R theory (Bakker & Demerouti, 2017), it seems important to study the effect of empathy and self-compassion in the relationship between their passion at work and emotional exhaustion and STS.
Firstly, empathy understood as “the capacity to fully understand other’s feelings and be able to put in the other’s place” was formulated as a main risk factor for developing STS, especially in caring professions (Figley, 1995; Moreno-Jiménez et al., 2008). These authors support that empathic abilities may in turn make healthcare workers feel the patients’ pain as their own pain, increasing the risk of feeling overwhelmed and be highly affected by traumatic events. So that:
-
Hypothesis 3: Daily empathy at work is positively related to daily (a) emotional exhaustion and (b) secondary traumatic stress after work.
Moreover, previous studies in emergency workers reveled that those workers with high empathy are more at risk of developing STS, especially in situations with high workload and time pressure, which is high job demands (Moreno-Jiménez et al., 2008). It seems that the presence of high empathy skills makes more likely an emotional contagion as studies support (Moreno-Jiménez et al., 2020; van Mol et al., 2018). This emotional contagion through empathy may impact on the relationship between passionate workers, activated by the job demands (i.e. high workload and time pressure), and the consumed energy (daily exhaustion) or STS experience, as authors suggest. Specifically, obsessive workers feel an inner pressured to develop their work, and the need to be empathic may enhance its negative effect on exhaustion and STS. In contrast, harmonious passionate workers feel free to develop their work but its natural disposition to engage working may be affected by these empathic skills, diminishing the positive effect of harmonious passion on exhaustion and STS. We hypothesized as follows:
-
Hypothesis 4: Daily empathy at work moderates the relationship between daily harmonious passion at work and (a) emotional exhaustion and (b) secondary traumatic stress after work, such that there is a less strong/negative relationship when empathy is high than when it is low.
-
Hypothesis 5: Daily empathy at work moderates the relationship between daily obsessive passion at work and (a) emotional exhaustion and (b) secondary traumatic stress after work, such that there is a stronger positive relationship when empathy is high than when it is low.
Finally, findings regarding ICU healthcare workers remark that care involves compassion as a way to alleviate individuals’ pain, being as much important as this compassion attitude toward oneself to alleviate the own pain (Raab, 2014). In this regard, self-compassion is defined as an attitude of self-kindness, acting with no self-judging, and considering one’s mistake as a normal part of human beings (Neff, 2003). Little is known empirically about self-compassion attitude in healthcare workers, but seems to strongly protect against STS (Moreno-Jiménez et al., 2020) and is suggested to reduce emotional exhaustion as well (Saadat & Kain, 2018). Self-compassion seems to potentially alleviate the stress response provoked by high workload and prolonged job-related demands in emotionally-demanding tasks through this self-care attitude, as is stated by Beaumont et al. (2016) using midwives students. In this sample, self-compassion is negatively related to burnout and STS, and positively related to well-being. For this reason, self-compassion may prevent the feeling of being overwhelmed and loss of energy in ICU as similar to occur in this sample. Thus:
Hypothesis 6: Daily self-compassion at work is negatively related to daily (a) emotional exhaustion and (b) secondary traumatic stress after work.
Also, van Mol et al. (2018) remark that those healthcare workers in ICU that may feel more engaged and part of the organization, they will display more attitudes related to compassion. This compassion attitudes may affect the relationship between passion at work, which makes workers more engaged in their work and create a sense of identity towards work (Donahue et al., 2012), and the associated consequences (Raab, 2014). In that regard, none study has proven the relationship between self-compassion and passion, but it could be a personal resource which potentially boosts the harmonious passion behaviors by enhancing self-care attitudes (Saadat & Kain, 2018), and struggle with the obsessive passion by diminishing the inner pressure to continue working. Hence, the positive outcomes associated with harmonious passion (e.g. more recovery after work, Donahue et al, 2012), could be enhanced due to self-compassion skills, highly related to well-being, and less burnout (e.g. by this recovering time; Beaumont et al., 2016). Moreover, a self-kindness attitude as it is self-compassion, could promote a non-self-judging behavior, which in turn may decrease the rumination process more related to the obsessively passionate profile (Donahue et al., 2012). This fact could open a space between work and worker, enabling more self-care attitudes. So that:
-
Hypothesis 7: Daily self-compassion at work is expected to have a boosting effect between daily harmonious passion at work and (a) emotional exhaustion and (b) secondary traumatic stress after work, such that there is a stronger negative relationship when self-compassion is high than when it is low.
-
Hypothesis 8: Daily self-compassion at work is expected to have a buffering effect between daily obsessive passion at work and (a) emotional and (b) secondary traumatic stress after work, such that there is a less strong/positive relationship when self-compassion is high than when it is low.
Figure 1 represents the proposed research model.

Proposed research model. Note: All measures are day-level; 1 at work 2 after work
Methods
Participants
The sample was composed of 97 health professionals of ICU from four hospitals in Spain, being 32% male and 68% female. The average age was 39.48 years (SD 10.05) and years of tenure were 11.03 (SD 9.04). In addition to this, 74.2% refers to be in a partnership, whereas 25.8% refers to not have a partner. In our sample, there were included physicians (33%), nurses (54.6%), and nursing assistants (12.4%), being 64.9% of the morning shifts, 21.6% of the afternoon shift, and 13.4% referring to both shifts. Our sample was divided into two types of ICU: workers from pediatrics ICU were 34%, whereas 66% came from general ICU. Regarding previous traumatic experience, 40.3% of the sample refer to not have experienced any traumatic experience previously.
Measures
All measures were obtained from the original item reworded as “today at work” to collect daily measures at work, and “today” to collect daily measures after work for five days (Nezlek, 2007). All questionnaires presented below were previously validated for Spanish sample.
Daily job demands
This measure was obtained through the Secondary Traumatic Stress Scale (STS, Meda et al., 2012) which include the assessment of specific job demands related to trauma in emergency fields and was adapted to intensive care settings. Within this measure, we assessed social pressure (e.g. “when the relative or the patient is a health professional, I feel uncomfortable developing my work”); time pressure (e.g. “in our service, the pressure for initially attending to a patient is very high”); and traumatic task (e.g. “I feel that cases that are similar to me in some way, affect to me a lot”). The total scale consisted of 5 items with a Likert-scale response ranging from 1 (totally disagree) to 4 (totally agree). The Cronbach alpha was 0.70, ranging from 0.61 to 0.73 among days, calculating this from day 1 to 5.
Daily passion at work
This variable was measured through Passion Towards Work scale (Serrano Fernández, et al., 2017). It consists of 9-item scale in which are assessed: harmonious passion, with a 4-item scale which evaluates the balance that a worker keeps in his/her life and work (e.g. “my work is in harmony with other activities of my life”) and obsessive passion, with a 5-item scale, which reflects the difficulties to disengage from work (e.g. “I emotionally depend on my work”). Responses were ranging from 1 (“totally disagree”) to 7 (“totally agree”). The Cronbach alpha of the general passion was 0.85. Concerning both types of passion, harmonious passion obtained a Cronbach alpha of 0.85, having a variability between 0.82 and 0.86 among days, whereas the alpha of obsessive passion was 0.83, having a variability between.82 and 0.86 among days, calculating this from day 1 to 5.
Daily empathy at work
For this measure, the empathy scale included in STS scale was used (Meda et al., 2012). This scale consisted of 4 items (e.g. “I emotionally involve too much with certain patients”). The response format was a Likert scale ranging from 1 (“totally disagree”) to 4 (“totally agree”). The Cronbach obtained was 0.81, ranging from 0.75 to 0.83 among days, calculating this reliability from day 1 to 5.
Daily self-compassion at work
The brief version of the 4-item scale of Self-Compassion was used (SCS, Garcia-Campayo et al., 2014), in which is assessed the attitude of kindness and not judging toward oneself (e.g. “I try to see my mistakes as a normal part of human being condition”). The response format is a Likert scale ranging from 1 (“rarely”) to 5 (“almost always”). The alpha was 0.59, ranging from.52 to 0.63 among days, calculating this from day 1 to 5.
Daily emotional exhaustion after work
This variable was assessed through a 4-item scale (e.g. “I feel physically and mentally exhausted”) from a Nursing Burnout Scale (Garrosa et al., 2008; Moreno-Jiménez et al., 2000). The scale response format was ranging from 1 (“totally agree”) to 4 (“totally disagree”). The Cronbach alpha was 0.90, ranging from 0.90 to 0.92 between day 1 and 5.
Daily secondary traumatic stress after work
This scale (STS; Meda et al., 2012) allow us to assess the three dimensions as follows: a) compassion fatigue, as the process of being emotionally tired due to the empathic skills displayed as a helping worker (e.g. “I feel emotionally without strength”); b) shattered assumptions, as the changes in values, beliefs and thoughts about oneself, the world and the others due to the continued exposure to traumatic events (e.g. My work makes me see the world as unfair”); and c) symptomatology, referring to the symptomatology involved in post-traumatic stress disorder, including intrusion, avoidance and arousal symptoms (e.g. “I remember even the name of some patients”). The response format was ranging from 1 (“completely disagree”) to 4 (“completely agree”). The Cronbach alpha was 0.67, ranging from 0.60 to 0.84 among days, calculating this from day 1 to 5.
Procedure
The project was first announced through different meetings with the supervisors in different ICUs in tertiary hospitals, offering a clinical session to all interested health workers of ICU who were invited and asked to freely participate. After these clinical sessions, those interested in participating were given a package of questionnaires in a closed and franked envelope to protect their data. Moreover, in each package they may generate a code to be identified, protecting by this way their personal information, and were personally collected from each participant in order to guarantee confidentiality. This package contained a general questionnaire with the sociodemographic variables and diary protocol which were created with the above-mentioned instruments, and depending on their shifts. Considering the worker shift allowed us to equalize the data collection: a) for the morning shift, they were compelled to fill the diary immediately after work before lunch, and at home before going to sleep; and b) for the afternoon shift, they were compelled to fill it immediately after work at night before going to sleep, and the next morning. By this way, we aimed to collect data regarding the work shift to assess every aspect related to work (predictors in our model), and after work, assessed after a brief period of recovery from work (outcomes). This procedure allowed us to separate the assessment moments, which reduces the common-method variance (Podsakoff et al., 2003). The general procedure was to fill the diaries in two moments per day for five working days. In total, 120 packages of questionnaires were spread in the four hospitals, so we could account for a response rate of 80.83%.
Data analysis
A hierarchical modeling approach (HLM) was used due to our data structure of 2 levels (Nezlek, 2007): level 1 was day-level (N = 485 occasions) and level 2 was person-level measure (N = 97 participants). According to Ohly et al. (2010), we centered variables distinctively depending on their level, centering the person-level variable (i.e. ICU) around the grand mean (level 2 of person-level), and the day-level variables (i.e. job demands, harmonious and obsessive passion, empathy, self-compassion, emotional exhaustion, and STS) around the person-level, in order to allow comparison between-person and within-person. Data analysis was conducted using MLwiN 2.28 software (Leckie & Charlton, 2013). Due to the limited space in tables, the null model of each HLM per variable is shown within the note section. Moreover, multilevel mediation analysis was conducted in order to get the indirect effect using Preacher’s online tool (Selig & Preacher, 2009) and R program. After testing the significance of the interaction effect of the day-level moderators (empathy and self-compassion at work) and the predictor variable (passion at work) on the outcomes (emotional exhaustion and secondary traumatic stress), we conducted the simple slope test (Preacher et al., 2006).
Results
Preliminary analysis
Means, standard deviations, Cronbach’s alpha, the intraclass correlation (ICC) and all correlations between interesting variables are shown in Table 1. The ICC depicts the variance at the day-level that is explained by the person-level. Moreover, we conducted t-test to compare whether there are differences between our interested variables in two types of ICU. We found significant differences in these variables: a) daily job demands, being higher in pediatric ICU (F = 4.48; t = -0.96; p < 0.05; M = 2.85); b) daily harmonious passion, being higher in pediatric ICU (F = 4.21; t = -3.11; p < 0.05; M = 4.83); and c) daily emotional exhaustion, being higher in adult ICU (F = 6.75; t = 0.662; p < 0.05; M = 2.58).
Hypothesis testing
The results of our hierarchical linear modelling are shown in Table 2 for emotional exhaustion and in Table 3 for secondary traumatic stress. As observed, the null model of each variable (i.e. emotional exhaustion in Table 2 and secondary traumatic stress in Table 3) is shown in the note section. Firstly, regarding the main effects of job demands on the mediators (passion at work), we found a non-significant relationship between daily job demands and daily obsessive passion at work (B = 0.109; SE = 0.108; t = 1.009, p > 0.05) but a significant and positive relationship between daily job demands and daily harmonious passion at work (B = 0.395; SE = 0.104; t = 3.798; p < 0.001). Moreover, only daily harmonious passion at work was significant and negatively related to both daily emotional exhaustion (B = -0.094; SE = 0.045; t = -2.089; p < 0.05) and STS (B = -0.113; SE = 0.053; t = -2.132; t < 0.05), as we observe in Tables 2 and 3.
Secondly, regarding the main effect of daily job demands and the outcomes, we found a significant and positive relationship between daily job demands and daily emotional exhaustion after work (B = 0.200; SE = 0.095; t = 2.105; p < 0.05), which is maintained over the models in spite of the inclusion of moderator variables, as we can see in models 4 and 5 in Table 2. As is visible in Table 3, we found a significant and positive relationship between daily job demands and daily STS after work before the inclusion of moderator variables (model 2, B = 0.300; SE = 0.110; t = 2.727; p < 0.01). Table 3 shows a significant effect of daily job demands on secondary traumatic stress with the inclusion of the mediator, but loses its significance later with interaction models (models 4 and 5 in Table 3). Following Mathieu & Taylor (2007) suggestions, we could test the indirect effects of harmonious passion at work to contrast its mediational effect (hypothesis 1), but no support was found for the mediational effect of obsessive passion (hypothesis 2) due to the nonsignificant relationship between the predictor (daily job demands) and the mediator (daily obsessive passion at work) and the mediator with neither outcome (emotional exhaustion nor STS).
The mediating effect of daily harmonious passion at work
Starting with the mediation of daily harmonious passion on daily job demands and exhaustion, we found a significant and negative indirect effect (95% CI [-0.085, -0.004]). Due to the significant direct effect of daily job demands on daily exhaustion above-mentioned, we pointed out a partial mediation effect.
Continuing with the mediation effect of daily harmonious passion on daily job demands and secondary traumatic stress, we found a significant indirect effect as well (95% CI [-0.098, -0.011]). Due to the significant direct effect of daily job demands on daily STS presented above, we pointed out a partial mediation effect. Thus, statistical findings support hypothesis 1 for both emotional exhaustion and secondary traumatic stress.
Interaction effects
Daily emotional exhaustion after work
As we can see in Table 2, the inclusion of moderators (model 4) showed a nonsignificant improvement (difference of -2 × log = 2.053, df = 2; p > 0.05), so we did not find statistical support for neither hypothesis 3 (a) nor for hypothesis 6 (a). In contrast, we found a significant fit improvement with the inclusion of interaction effects (model 5; difference of -2 × log = 9.88, df = 4; p < 0.001). Regarding daily harmonious passion, the interaction between daily harmonious passion and daily empathy at work significantly predicted emotional exhaustion after work (B = 0.188; SE = 0.080; p < 0.05) (see Table 2). Furthermore, simple slope test revealed that the relation between daily harmonious passion and exhaustion was significant for those with low empathy at work (γ = -0.282, SE = 0.01, z = -2.82, p < 0.01; see Fig. 2), whereas for those with higher empathy profile the relation was nonsignificant (γ = 0.094, SE = 0.077, z = 1.213, p > 0.05; see Fig. 2). These findings supported hypothesis 4 (a). Moreover, statistical findings provide no support for hypothesis 7 (a) as we found that the interaction between daily harmonious passion and daily self-compassion at work was not significantly related to emotional exhaustion.

Day-level interaction between harmonious passion at work and empathy at work in predicting daily emotional exhaustion after work
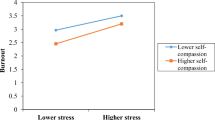
Moreover, despite the non-significant effect of daily obsessive passion at work on daily exhaustion after work (Table 2; B = -0.067; SE = 0.043; p > 0.05), the interaction effect between daily obsessive passion and self-compassion at work was significantly related to emotional exhaustion (B = -0.153; SE = 0.072; p < 0.05). Simple slope test revealed this significant effect for those workers with high self-compassion (γ = -0.22, SE = 0.070, z = -3.111, p > 0.01), but not among those with low self-compassion (γ = 0.086, SE = 0.094, z = 0.906, p > 0.05) (Fig. 3). These findings provide support for hypothesis 8 (a). Our findings did not support hypothesis 5 (a) as we found that the interaction between daily obsessive passion and daily empathy at work was not significantly related to emotional exhaustion.

Day-level interaction between obsessive passion and self-compassion at work in predicting daily emotional exhaustion after work
Daily secondary traumatic stress after work
As shown in Table 3, the inclusion of moderators (model 4) showed a fit improvement in comparison with model 3 (difference of -2 × log = 10.263, df = 2; p < 0.001), providing a significant and positive effect of daily empathy at work on STS (B = 0.253; SE = 0.092; p < 0.01), but nonsignificant effect of daily self-compassion. Furthermore, the inclusion of interaction terms resulted in a nonsignificant improvement in the model fit (Table 3, model 5). Moreover, none of the interactions were significantly related to STS. Only daily empathy was positively and significantly related to daily STS in model 4. These findings only supported hypothesis 3 (b), and hypothesis 4 (b), 5 (b), 7 (b) and 8 (b) of the interaction effects had to be rejected.
Discussion
This study aimed to test the mediational effect of passion at work in the relationship between job demands and negative outcomes in ICU on a day-level basis, and uncover the role of personal resources especially relevant among healthcare workers, namely empathy and self-compassion skills. Testing these goals, we thoroughly contribute to the literature in several ways. Firstly, we surpass cross-sectional designs widely implemented in this field (Kelly, 2020). Secondly, our findings pointed out the relevance of daily harmonious passion experiences at work in negatively predict negative outcomes particularly prevalent in the ICU settings, despite the lack of papers in this vein (Cieslak et al., 2014). Finally, we provide empirical results to contrast the JD-R model specifically in ICU, placing an emphasis on passionate health workers working in a demanding context. Thus, this study strongly contributes to future intervention research aimed at enhancing healthcare workers’ well-being, which seems linked to the quality of both care and life (Gómez-Salgado et al., 2019).
As a starting point, the consideration of both emotional exhaustion and STS allows us to better understand these negative outcomes. In this regard, our findings are in line with Bakker and Demerouti (2007, 2017) who concluded that job demands are directly related to job strain. In our study, job demands were related to emotional exhaustion and STS. Both outcomes are directly affected by daily rigorous work (time and social pressure, work overload, traumatic task) (Wang et al., 2020). Both outcomes were measured after work, which highlights that job demands create such load effects that expand themselves also outside working time. These findings outline the consequences that working in a demanding context such as ICU may have for healthcare workers.
Passion for work plays a key role in these healthcare workers when it comes to explaining the intermediate process between the job demands and the outcomes. According to Houlfort et al. (2014), challenging work indeed activates their passionate attitude to invest resources at work, considering challenging work as high demanding job contexts. In our study, high daily job demands predict those harmonious passionate profiles, and consequently, this daily harmonious passion is negatively related to both exhaustion and STS, as literature support (Moreno-Jiménez et al., 2020; Vallerand et al., 2010). This result allows us to determine two steps: a) ICU-related demands activate their personal experience to love their job and identify themselves with these ICU-related tasks, pushing them to do heavier invest of time and resources on it (Amarnani et al., 2019) considering them as gratifying and challenging; and b) afterward, this perception of the high job demands as challenging, makes those workers to display behaviors associated with harmonious passion (e.g. recovery activities, less rumination) making them less prone to feel exhausted or stressed by traumatic tasks (Donahue et al., 2012). According to Hobfoll (2001) and Amarnani et al. (2019), the conservation of resources through this harmonious passion plays a key protective role against developing emotional exhaustion and STS, having indistinctively similar effects on both. Thus, with regard to daily rigorous work and their natural passion for this, they displayed their harmonious passion in order to maintain a good level of resources during the investment at work. At the same time, this passion allows them to keep the high-quality job required in the health context. These findings on harmonious passion are similar to the previous studies in which the job demands are related to work engagement (van Mol et al., 2018), and also to research suggesting that harmonious passion mediates between the job demands and well-being outcomes (Dubreuil et al., 2014). In our study, harmonious passion had a negative relationship with emotional exhaustion and STS.
Furthermore, the preliminary comparative results of the two types of ICU may reflect the afore-mentioned process. For instance, pediatric ICU seems to have higher job demands, and indeed, higher harmonious passion profiles. Moreover, emotional exhaustion is found to be lower in pediatric ICU in comparison with adult ICU, which underlines the idea that those with higher harmonious passion are less likely to feel exhausted (Donahue et al., 2012). These findings seem to be in line with Meadors et al. (2010), in which the levels of burnout are lower in pediatric healthcare professionals and we provide a possible explanation of this fact through the role of harmonious passion.
In regard to daily obsessive passion at work, we showed that neither daily job demands nor negative outcomes are related to this kind of profile. In this sense, daily obsessive passion seems not to play a key role in this model, considering it as a proper personal demand and more related to those jobs in which spending more hours at work involves a greater amount of money, networking, or external rewards. In the ICU context, where the external rewards are controlled and not increased depending on work hours, the specific job demands are associated with the harmonious side which brings them to more adaptive behaviors against negative outcomes. Moreover, it seems that the job demands presented in ICU are acknowledged as part of ICU work and they are related to work engagement in these specific workers, as van Mol et al. (2018) suggest. This fact points out the vocational work that healthcare workers in ICU are developing. This work engagement is associated with the harmonious passion rather than the obsessive one (Vallerand et al., 2003). Besides, another explanation is possible whether we consider the moment of assessment. In our study, both types of passion were assessed at work shifts, in which they could experience their harmonious passion due to their vocational work (van Mol et al., 2018). In contrast, the obsessively passionate experiences could enhance once they stayed at home. This argument seems to be plausible according to Donahue et al.’s findings (2012), in which obsessive passionate workers manifest their obsession through cognitive processes such as rumination, and this may be displayed after work (e.g. being at home). Further research focusing on how passion fluctuates along the day is needed to better understand the mechanism of both types of passion.
Finally, this study allows us to speculate about the different nature of both outcomes, emphasizing the personal resources naturally develop in healthcare professionals. On the one hand, emotional exhaustion seems an outcome more related to the loss of energy and resources invested at work (Bakker & Demerouti, 2017), rather than empathic skill related to caring tasks (Kelly, 2020). The lack of a direct effect of empathy on this outcome and the significant interaction effects of empathy and self-compassion depending on their passion at work allow us to explain this. Specifically, we found an interaction between this empathic skills and harmonious passion, suggesting that the healthcare workers are more able to display their harmoniously passionate profile, loving his/her job and keeping a balanced work/life, especially when empathy is low than when it is high, linked to lower levels of emotional exhaustion. This relates to the general assumption proposed by Vallerand et al. (2003) and Vallerand (2008) who defined harmonious passion as a balance between work and other worker’s life activities, in which work occupies a significant space in their lives, but not unbalanced. When high empathy plays a role increasing the risk of emotional contagion (Figley, 1999; Moreno-Jiménez et al., 2008, 2020), this balance could be broken, increasing the likelihood of feeling exhausted. Thus, empathy plays a role by diminishing the positive effect of harmonious passion profiles in regards to exhaustion.
Concerning self-compassion, this personal resource may destroy the unbalance followed by obsessive passion (Parastatidou et al., 2014), showing a buffering effect between this passion and exhaustion, as it is supported by literature (Saadat & Kain, 2018). Furthermore, the lack of interaction with harmonious passion may be due to the similarity of both concepts. In this regard, those harmoniously passionate workers may display self-compassion attitude which boost recovery activities and keep a balance in their life, as part of their current harmonious passion.
On the other hand, whereas the afore-mentioned model of emotional exhaustion could be widely applied to several fields in which empathy and self-compassion play roles in work-related tasks (e.g., social workers, psychologist, and emergency services), STS seems an outcome specifically for this helping career, where the empathy plays a role in its development (Figley, 1999; Moreno-Jiménez et al., 2008), regardless of their passionate attitude. This lack of any interaction effect and the outstanding role of empathy as a direct predictor, allow us to suggest that STS is a negative outcome derived from helping others and experiencing as own their pain/suffering (Figley, 1999). Thus, harmonious passion plays a role between the daily ICU demands related to helping tasks, and their levels of STS, diminishing this relationship. In addition, empathy seems to positively predict this STS, being a risk factor regardless of the type of passion. In this regard, our preliminary comparative findings about pediatric ICU showed nonsignificant differences regarding empathy and STS among the two types of ICU. These findings highlight that healthcare workers displayed similar empathy resources regardless of the type of ICU, and in turn, this predicts similar levels of STS on both.
To conclude, whereas both outcomes could be likely in these ICU settings, as many authors suggest (Cieslak et al., 2014), we may distinguish between an energy depletion of exhaustion more directly related to job demands in demanding work settings (Bakker & Demerouti, 2017), and STS, more related to the content of the task and the help provided specifically during traumatic events (Cieslak et al., 2014). According to this, the latest studies in the field have proposed to study both outcomes to describe in-depth the consequences of caregiving (Kelly, 2020). Our study provides empirical results of this new phenomenon specifically in ICU.
Limitations and future research
There are some limitations that should be considered. Firstly, we use self-report measures for building the diary package, so that, there is a lack of objective measures regarding the job demands and outcomes, specifically their levels of exhaustion. This fact may boost future researches aim to develop objective measures in such ICU context which allow us to better understand the predictors and outcomes. In spite of this, the daily approach taking repeated measures along five days in two moments per day (485 assessments occasions) allows us to deepen into the interesting variables and their variability over time, obtaining a better measure in comparison with a cross-sectional design. Moreover, this specific design allows us to not commit errors due to the response tendencies by centering the variables in a person-level as is recommend (Ohly, et al., 2010).
Secondly, linked to this self-report, we found some acceptable reliability indexes, such as self-compassion, in which the inclusion of only four items to avoid the large extension and fatigue of healthcare workers may involve the loss of reliability. Future research should emphasize the assessments in this specific context with validated brief versions of scales to avoid the overload of these healthcare workers. Moreover, a longitudinal approach from this diary study by repeating it after 6 months, should strengthen these findings building a more robust theoretical model that can guide intervention research.
Finally, the variety of professionals (physicians, nurses, nurse assistants) and the different shifts made us to thoroughly study how to overcome all possible biases. In this regard, a previous focused group with the person in charge of each unit was executed to establish the best way to assess, including the majority of professionals and shifts as part of the whole unit of interest. Thus, we tried to control the shift by designing a different package for morning, afternoon, or night shifts to control this potential threat and assess the same state at work or after work.
Conclusions
Our findings are relevant for further preventative measures. Firstly, according to several studies (van Mol et al., 2015), the job demands in ICU revealed to have a negative impact on healthcare workers’ well-being, which should be diminished to prevent the long-term consequences of developing negative outcomes. Moreover, Shoji et al. (2015) revealed that only exhaustion is able to predict STS in a longitudinal study, after a 6-month follow-up. According to that, we should pay special attention to the symptoms related to emotional exhaustion, such as their feeling of drained out, in order to prevent the second step, STS. In that regard, it is undeniably important to develop specific assessments in ICU healthcare workers for early detection of these possible outcomes.
Moreover, the present research addresses several findings to propose intervention measures in healthcare contexts. For applied psychology, job crafting techniques as are supported by Gordon et al. (2018) could be considered as valuable techniques to redesign job context from a bottom-up approach and enhance their harmonious passion at work which seems relevant. Moreover, enhancing their awareness of personal resources, such as empathy and self-compassion, may allow them to properly use them to boost the effect of harmonious passion in terms of preventing the loss of resources, accordingly with their need to keep a high-quality job.
Finally, in terms of research, this work also points out the differential mechanism that passion at work may have and new explicative variables that could be taken into consideration. Self-compassion could be one ability considered in those harmonious passionate workers which may enhance the positive outcomes associated.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Amarnani, R. K., Lajom, J. A. L., Restubog, S. L. D., & Capezio, A. (2019). Consumed by obsession: Career adaptability resources and the performance consequences of obsessive passion and harmonious passion for work. Human Relations. https://doi.org/10.1177/0018726719844812
Austin, B., Downing, C., & Hastings-Tolsma, M. (2019). Experience of neonatal intensive care unit nurses in providing developmentally-supportive care: A qualitative study. Nursing and Health Sciences, 21(3), 336–344. https://doi.org/10.1111/nhs.12603
Bakker, A. B., & Albrecht, S. (2018). Work engagement: Current trends. Career Development International, 23(1), 4–11.
Bakker, A. B., & Demerouti, E. (2007). The Job Demands-Resources model: State of the art. Journal of Managerial Psychology, 22(3), 309–328. https://doi.org/10.1108/02683940710733115
Bakker, A. B., & Demerouti, E. (2017). Job demands-resources theory: Taking stock and looking forward. Journal of Occupational Health Psychology, 22(3), 273–285. https://doi.org/10.1037/ocp0000056
Bakker, A. B., & Sanz-Vergel, A. I. (2013). Weekly work engagement and flourishing: The role of hindrance and challenge job demands. Journal of Vocational Behavior, 83(3), 397–409. https://doi.org/10.1016/j.jvb.2013.06.008
Bakker, A. B., Demerouti, E., & Verbeke, W. (2004). Using the job demands-resources model to predict burnout and performance. Human Resource Management, 43(1), 83–104. https://doi.org/10.1002/hrm.20004
Ballester-Arnal, R., Gómez-Martínez, S., Gil-Juliá, B., Ferrándiz-Sellés, M. D., & Collado-Boira, E. J. (2016). Burnout y factores estresantes en profesionales sanitarios de las unidades de cuidados intensivos. Revista de Psicopatologia y Psicologia Clinica, 21(2), 129–136. https://doi.org/10.5944/rppc.vol.21.num.2.2016.16146
Barbier, M., Hansez, I., Chmiel, N., & Demerouti, E. (2013). Performance expectations, personal resources, and job resources: How do they predict work engagement? European Journal of Work and Organizational Psychology, 22(6), 750–762. https://doi.org/10.1080/1359432X.2012.704675
Beaumont, E., Durkin, M., Hollins Martin, C. J., & Carson, J. (2016). Compassion for others, self-compassion, quality of life and mental well-being measures and their association with compassion fatigue and burnout in student midwives: A quantitative survey. Midwifery, 34, 239–244. https://doi.org/10.1016/j.midw.2015.11.002
Birkeland, I. K., & Buch, R. (2015). The dualistic model of passion for work: Discriminate and predictive validity with work engagement and workaholism. Motivation and Emotion, 39(3), 392–408. https://doi.org/10.1007/s11031-014-9462-x
Birkeland, I. K., Richardsen, A. M., & Dysvik, A. (2018). The role of passion and support perceptions in changing burnout: A Johnson-Neyman approach. International Journal of Stress Management, 25(2), 163. https://doi.org/10.1037/str0000057
Blanco-Donoso, L. M., Garrosa, E., Demerouti, E., & Moreno-Jiménez, B. (2017). Job resources and recovery experiences to face difficulties in emotion regulation at work: A diary study among nurses. International Journal of Stress Management, 24(2), 107–134. https://doi.org/10.1037/str0000023
Chuang, C. H., Tseng, P. C., Lin, C. Y., Lin, K. H., & Chen, Y. Y. (2016). Burnout in the intensive care unit professionals: a systematic review. Medicine, 95(50). https://doi.org/10.1097/MD.0000000000005629
Cieslak, R., Shoji, K., Douglas, A., Melville, E., Luszczynska, A., & Benight, C. C. (2014). A meta-analysis of the relationship between job burnout and secondary traumatic stress among workers with indirect exposure to trauma. Psychological Services, 11(1), 75–86. https://doi.org/10.1037/a0033798
Colville, G. A., Smith, J. G., Brierley, J., Citron, K., Nguru, N. M., Shaunak, P. D., Tam, O., & Perkins-Porras, L. (2017). Coping with staff burnout and work-related posttraumatic stress in intensive care. Pediatric Critical Care Medicine, 18(7), e267–e273. https://doi.org/10.1097/PCC.0000000000001179
Demerouti, E., Nachreiner, F., Bakker, A. B., & Schaufeli, W. B. (2001). The job demands-resources model of burnout. Journal of Applied Psychology, 86(3), 499–512.
Demerouti, E., Bakker, A. B., Vardakou, I., & Kantas, A. (2003). The convergent validity of two burnout instruments: A multitrait-multimethod analysis. European Journal of Psychological Assessment, 19(1), 12–23. https://doi.org/10.1027//1015-5759.19.1.12
Dominguez-Gomez, E., & Rutledge, D. N. (2009). Prevalence of secondary traumatic stress among emergency nurses. Journal of Emergency Nursing, 35(3), 199–204. https://doi.org/10.1016/j.jen.2008.05.003
Donahue, E. G., Forest, J., Vallerand, R. J., Lemyre, P. N., Crevier-Braud, L., & Bergeron, É. (2012). Passion for work and emotional exhaustion: The mediating role of rumination and recovery. Applied Psychology: Health and Well-Being, 4(3), 341–368. https://doi.org/10.1111/j.1758-0854.2012.01078.x
Dubreuil, P., Forest, J., & Courcy, F. (2014). From strengths use to work performance: The role of harmonious passion, subjective vitality, and concentration. Journal of Positive Psychology, 9(4), 335–349. https://doi.org/10.1080/17439760.2014.898318
Embriaco, N., Papazian, L., Kentish-Barnes, N., Pochard, F., & Azoulay, E. (2007). Burnout syndrome among critical care healthcare workers. Current Opinion in Critical Care, 13(5), 482–488. https://doi.org/10.1097/MCC.0b013e3282efd28a
Epp, K. (2012). Burnout in critical care nurses: a literature review. Dynamics (Pembroke, Ont.), 23(4), 25–31.
Figley, C. R. (1995). Compassion fatigue as secondary traumatic stress disorder: an overview. In C. R. Figley (Ed.), Compassion fatigue. Coping with secondary traumatic stress disorder in thos who treat the traumatized (pp. 1–21). Brunner-Routledge.
Figley, C. R. (1999). Compassion fatigue as secondary traumatic stress disorder: An overview. In Figley (Ed.), Compassion fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatized (pp. 1–20). Brunner-Routledge.
Franklin, C. (2020). Intensive care burnout. In J. Hidalgo et al. (Eds.), Critical care administration (pp. 207–214). Springer.
Garcia-Campayo, J., Navarro-Gil, M., Andrés, E., Montero-Marin, J., López-Artal, L., & Demarzo, M. M. P. (2014). Validation of the Spanish versions of the long (26 items) and short (12 items) forms of the Self-Compassion Scale (SCS). Health and Quality of Life Outcomes, 12(1), 1–9.
Garrosa, E., Moreno-Jiménez, B., Liang, Y., & González, J. L. (2008). The relationship between socio-demographic variables, job stressors, burnout, and hardy personality in nurses: an exploratory study. International Journal of Nursing Studies, 45(3), 418–427. https://doi.org/10.1016/j.ijnurstu.2006.09.003
Giusti, E. M., Pedroli, E., D’Aniello, G. E., StrambaBadiale, C., Pietrabissa, G., Manna, C., StrambaBadiale, M., Riva, G., Castelnuovo, G., & Molinari, E. (2020). The psychological impact of the COVID-19 outbreak on health professionals: A cross-sectional study. Frontiers in Psychology, 11(July), 1–9. https://doi.org/10.3389/fpsyg.2020.01684
Gómez-Salgado, J., Navarro-Abal, Y., López-López, M. J., Romero-Martín, M., & Climent-Rodríguez, J. A. (2019). Engagement, passion and meaning of work as modulating variables in nursing: A theoretical analysis. International Journal of Environmental Research and Public Health, 16(1). https://doi.org/10.3390/ijerph16010108
Gordon, H. J., Demerouti, E., Le Blanc, P. M., Bakker, A. B., Bipp, T., & Verhagen, M. A. M. T. (2018). Individual job redesign: Job crafting interventions in healthcare. Journal of Vocational Behavior, 104(April 2016), 98–114. https://doi.org/10.1016/j.jvb.2017.07.002
Ho, V. T., & Astakhova, M. N. (2018). Disentangling passion and engagement: An examination of how and when passionate employees become engaged ones. Human Relations, 71(7), 973–1000. https://doi.org/10.1177/0018726717731505
Hobfoll, S. E. (2001). The influence of culture, community, and the nested-self in the stress process: Advancing conservation of resources theory. Applied Psychology, 50(3), 337–421. https://doi.org/10.1111/1464-0597.00062
Houlfort, N., Philippe, F. L., Vallerand, R. J., & Ménard, J. (2014). On passion and heavy work investment: Personal and organizational outcomes. Journal of Managerial Psychology, 29(1), 25–45. https://doi.org/10.1108/JMP-06-2013-0155
Houlfort, N., Philippe, F. L., Bourdeau, S., & Leduc, C. (2018). A comprehensive understanding of the relationships between passion for work and work-family conflict and the consequences for psychological distress. International Journal of Stress Management, 25(4), 313–329. https://doi.org/10.1037/str0000068
Jowett, S., Lafrenière, M. A. K., & Vallerand, R. J. (2013). Passion for activities and relationship quality: A dyadic approach. Journal of Social and Personal Relationships, 30(6), 734–749. https://doi.org/10.1177/0265407512467748
Kelly, L. (2020). Burnout, compassion fatigue, and secondary trauma in nurses: Recognizing the occupational phenomenon and personal consequences of caregiving. Critical Care Nursing Quarterly, 43(1), 73–80. https://doi.org/10.1097/CNQ.0000000000000293
Kilroy, S., Bosak, J., Flood, P. C., & Peccei, R. (2020). Time to recover: The moderating role of psychological detachment in the link between perceptions of high-involvement work practices and burnout. Journal of Business Research, 108, 52–61. https://doi.org/10.1016/j.jbusres.2019.10.012
Lavigne, G. L., Forest, J., Fernet, C., & Crevier-Braud, L. (2014). Passion at work and workers’ evaluations of job demands and resources: A longitudinal study. Journal of Applied Social Psychology, 44(4), 255–265. https://doi.org/10.1111/jasp.12209
Leckie, G. B., & Charlton, C. M. J. (2013). runmlwin: A program to run the MLwiN multilevel modeling software from within Stata. Journal of Statistical Software, 52(11). https://doi.org/10.18637/jss.v052.i11
Luceño-Moreno, L., Talavera-Velasco, B., García-Albuerne, Y., & Martín-García, J. (2020). International Journal of Environmental Research and Public Health, 17(15), 1–19.
Mageau, G. A., & Vallerand, R. J. (2007). The moderating effect of passion on the relation between activity engagement and positive affect. Motivation and Emotion, 31(4), 312–321. https://doi.org/10.1007/s11031-007-9071-z
Mangoulia, P., Koukia, E., Alevizopoulos, G., Fildissis, G., & Katostaras, T. (2015). Prevalence of secondary traumatic stress among psychiatric nurses in Greece. Archives of Psychiatric Nursing, 29(5), 333–338. https://doi.org/10.1016/j.apnu.2015.06.001
Maslach, C. (2003). Job burnout: New directions in research and intervention. Current Directions in Psychological Science, 12, 189–192. https://doi.org/10.1111/1467-8721.01258
Mathieu, J. E., & Taylor, S. R. (2007). A framework for testing meso-mediational relationships in Organizational Behavior. Journal of Organizational Behavior: The International Journal of Industrial, Occupational and Organizational Psychology and Behavior, 28(2), 141–172. https://doi.org/10.1002/job.436
Meadors, P., Lamson, A., Swanson, M., White, M., & Sira, N. (2010). Secondary traumatization in pediatric healthcare providers: Compassion fatigue, burnout, and secondary traumatic stress. Omega: Journal of Death and Dying, 60(2), 103–128. https://doi.org/10.2190/OM.60.2.a
Meda, R., Moreno-Jiménez, B., Palomera, A., Arias, E., & Vargas, R. (2012). La Evaluación del Estrés Traumático Secundario. Estudio Comparado en Bomberos y Paramédicos de los Servicios de Emergencia de Guadalajara, México. Terapia Psicologica, 30(2), 31–41. https://doi.org/10.4067/S0718-48082012000200003
Moreno-Jiménez, B., Garrosa, E., & González-Gutiérrez, J. L. (2000). El desgaste profesional de enfermería. Desarrollo y validación factorial del CDPE. Archivos de Prevención de Riesgos Laborales, 3(1), 18–28.
Moreno-Jiménez, B., MoranteBenadero, M. E., Rodríguez-Carvajal, R., & Rodríguez-Muñoz, R. (2008). Resistencia y vulnerabilidad ante el trauma: El efecto moderador de las variables de personalidad. Psicothema, 20(1), 124–130.
Moreno-Jiménez, J. E., Rodríguez-Carvajal, R., Chico-Fernández, M., Lecuona, Ó., Martínez, M., Moreno-Jiménez, B., Montejo, J. C., & Garrosa, E. (2020). Risk and protective factors of secondary traumatic stress in Intensive Care Units: An exploratory study in a hospital in Madrid (Spain). Medicina Intensiva (English Edition), 44(7), 420–428. https://doi.org/10.1016/j.medine.2019.06.013
Morrison, L. E., & Joy, J. P. (2016). Secondary traumatic stress in the emergency department. Journal of Advanced Nursing, 72(11), 2894–2906. https://doi.org/10.1111/jan.13030
Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self and Identity, 2, 223–250. https://doi.org/10.1080/15298860390209035
Nezlek, J. B. (2007). A multilevel framwork for understanding relationships among traits, states, situations and behaviours. European Journal of Personality, 21, 789–810. https://doi.org/10.1002/per
Ohly, S., Sonnentag, S., Niessen, C., & Zapf, D. (2010). Diary studies in organizational research. An introduction and some practical recommendations. Journal of Personnel Psychology, 9(2), 79–93. https://doi.org/10.1027/1866-5888/a000009
Ortega-Campos, E., Vargas-Román, K., Velando-Soriano, A., Suleiman-Martos, N., Cañadas-de la Fuente, G. A., Albendín-García, L., & Gómez-Urquiza, J. L. (2019). Compassion fatigue, compassion satisfaction, and burnout in oncology nurses: A systematic review and meta-analysis. Sustainability, 12(1), 72. https://doi.org/10.3390/su12010072
Parastatidou, I. S., Doganis, G., Theodorakis, Y., & Vlachopoulos, S. P. (2014). The mediating role of passion in the relationship of exercise motivational regulations with exercise dependence symptoms. International Journal of Mental Health and Addiction, 12(4), 406–419. https://doi.org/10.1007/s11469-013-9466-x
Perrewé, P. L., Hochwarter, W. A., Ferris, G. R., Mcallister, C. P., & Harris, J. N. (2014). Developing a passion for work passion: Future directions on an emerging construct. Journal of Organizational Behavior, 35(1), 145–150. https://doi.org/10.1002/job
Podsakoff, P. M., MacKenzie, S. B., Lee, J. Y., & Podsakoff, N. P. (2003). Common method biases in behavioral research: a critical review of the literature and recommended remedies. Journal of Applied Psychology, 88(5), 879. https://doi.org/10.1037/0021-9010.88.5.879
Preacher, K., Curran, P., & Bauer, D. (2006). Computational tools for probing interactions in multiple linear regression, multilevel modeling and latent curve analysis. Journal of Educational and Behavioral Statistics, 31(3), 437–448. https://doi.org/10.3102/10769986031004437
Raab, K. (2014). Mindfulness, self-compassion, and empathy among health care professionals: A review of the literature. Journal of Health Care Chaplaincy, 20(3), 95–108. https://doi.org/10.1080/08854726.2014.913876
Saadat, H., & Kain, Z. N. (2018). Wellness interventions for anesthesiologists. Current Opinion in Anaesthesiology, 31(3), 375–381. https://doi.org/10.1097/ACO.0000000000000598
Sacco, T. L., Ciurzynski, S. M., Harvey, M. E., & Ingersoll, G. L. (2015). Compassion satisfaction and compassion fatigue among critical care nurses. Crit Care Nurse, 35(4), 32–42. https://doi.org/10.4037/ccn2015392
Selig, J. P., & Preacher, K. J. (2009). Mediation models for longitudinal data in developmental research. Research in Human Development, 6(2–3), 144–164. https://doi.org/10.1080/15427600902911247
Shoji, K., Lesnierowska, M., Smoktunowicz, E., Bock, J., Luszczynska, A., Benight, C. C., & Cieslak, R. (2015). What comes first, job burnout or secondary traumatic stress? Findings from two longitudinal studies from the U.S. and Poland. PLoS ONE, 10(8), 1–15. https://doi.org/10.1371/journal.pone.0136730
Tang, F. W. K., Ling, G. C. C., Lai, A. S. F., Chair, S. Y., & So, W. K. W. (2019). Four Es of caring in contemporary nursing: Exploring novice to experienced nurses. Nursing and Health Sciences, 21(1), 85–92. https://doi.org/10.1111/nhs.12561
Trépanier, S. G., Fernet, C., Austin, S., Forest, J., & Vallerand, R. J. (2014). Linking job demands and resources to burnout and work engagement: Does passion underlie these differential relationships? Motivation and Emotion, 38(3), 353–366. https://doi.org/10.1007/s11031-013-9384-z
Vallerand, R. J. (2008). On the psychology of passion: In search of what makes people’s lives most worth living. Canadian Psychology/psychologie Canadienne, 49(1), 1–13. https://doi.org/10.1037/0708-5591.49.1.1
Vallerand, R. J., Blanchard, C., Mageau, G. A., Koestner, R., Ratelle, C., Léonard, M., Gagné, M., & Marsolais, J. (2003). Les passions de l’âme: On obsessive and harmonious passion. Journal of Personality and Social Psychology, 85(4), 756–767. https://doi.org/10.1037/0022-3514.85.4.756
Vallerand, R. J., Paquet, Y., Philippe, F. L., & Charest, J. (2010). On the role of passion for work in burnout: A process model. Journal of Personality, 78(1), 289–312. https://doi.org/10.1111/j.1467-6494.2009.00616.x
Van Mol, M. M. C., Kompanje, E. J. O., Benoit, D. D., Bakker, J., Nijkamp, M. D., & Seedat, S. (2015). The prevalence of compassion fatigue and burnout among healthcare professionals in intensive care units: A systematic review. PLoS ONE, 10(8), 1–23. https://doi.org/10.1371/journal.pone.0136955
van Mol, M. M. C., Nijkamp, M. D., Bakker, J., Schaufeli, W. B., & Kompanje, E. J. O. (2018). Counterbalancing work-related stress? Work engagement among intensive care professionals. Australian Critical Care, 31(4), 234–241. https://doi.org/10.1016/j.aucc.2017.05.001
Wang, J., Okoli, C. T. C., He, H., Feng, F., Li, J., Zhuang, L., & Lin, M. (2020). Factors associated with compassion satisfaction, burnout, and secondary traumatic stress among Chinese nurses in tertiary hospitals : A cross-sectional study. International Journal of Nursing Studies, 102, 1–8. https://doi.org/10.1016/j.ijnurstu.2019.103472
Funding
This work was supported by the predoctoral fellowship FPI-UAM 2017 linked to the mobility fellowship FPI-UAM 2019 of Autonomous University of Madrid; and the I + D + I National Project of Ministerio de Ciencia e Innovación (PID2019-106368 GB-I00) / AEI/10.13039/501100011033.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical statement
Informed consent was given to all participants in this study. The whole study followed the ethical standards established by a research ethics committee (reference number CEI 71- 1276).
Conflict of interest
The authors declare to not have any conflict of interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Moreno-Jiménez, J.E., Demerouti, E., Blanco-Donoso, L.M. et al. Passionate healthcare workers in demanding intensive care units: its relationship with daily exhaustion, secondary traumatic stress, empathy, and self-compassion. Curr Psychol 42, 29387–29402 (2023). https://doi.org/10.1007/s12144-022-03986-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-03986-z