
Abstract
Self-compassion, a healthy way of relating to oneself, may promote psychological resilience during adolescence. How adolescents engage with self-compassion, and whether they have distinct self-compassionate or uncompassionate psychological profiles, is unclear. This study investigated potential self-compassion profiles based on responses to the Self-Compassion Scale–Short Form (SCS-SF) and examined their relationship with a range of mental health symptoms and cognitive and emotional tendencies. A large cross-sectional sample of high school students (N = 950; Mage = 13.70 years, SDage = 0.72, range = 12 to 16 years; 434 female and 495 male) completed several online self-report measures including the SCS-SF. Latent profile analysis identified parsimonious self-compassion profiles by gender using the six SCS-SF subscales. Five female profiles included ‘Low Self-Relating’, ‘Uncompassionate’, ‘High Self-Relating’, ‘Moderately Compassionate’ and ‘Highly Compassionate’. Comparatively, two male profiles included ‘Low Self-Relating’ and ‘Moderately Self-Relating’. Low Self-Relating involved low levels of both compassionate and uncompassionate responding, and Moderately Self-Relating involved higher levels of both. Low Self-Relating and Highly Compassionate profiles for females consistently reported lower levels of anxiety and depression symptoms, maladaptive perfectionism, intolerance of uncertainty, repetitive thinking and avoidance-fusion thinking patterns compared to the other female profiles. Low Self-Relating males reported more adaptive outcomes compared to Moderate Self-Relating males. These findings illustrate important adolescent gender differences in compassionate and uncompassionate self-response profiles. Results suggest self-compassion is an important psychological construct with diverse mental health benefits for females, whereas for males a lack of attachment to either response styles are linked with better psychological outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The global prevalence rate of adolescent mental disorders range from 13% (Griffin & McMahon, 2020; Polanczyk et al., 2015) to 20% (Kieling et al., 2011). Although this proportion is high, many adolescents do not develop a mental disorder despite experiencing multiple risk factors and adversity. Identification of protective psychological factors are crucial for the development of early psychological interventions, yet these remain poorly understood (Cabral & Patel, 2020; Haggerty & Mrazek, 1994). Self-compassion may be one such protective factor. Self-compassion refers to a healthy desire to help rather than hurt ourselves, particularly in times of distress or pain (Gilbert, 2009b; Gilbert & Procter, 2006; Neff, 2003b). The widely used self-report 26-item Self-Compassion Scale (SCS; Neff 2003a) measures six independent yet interacting sub-components. These include three beneficial compassionate self-responses (self-kindness, mindfulness and common humanity) and three detrimental uncompassionate self-responses (self-judgement, over-identification and isolation; Neff et al., 2018). Profile analyses of these six sub-components of self-compassion in adults (Phillips, 2019) and college students (Phillips, 2019; Wu et al., 2020) have identified distinct psychological profiles featuring differences in compassionate and uncompassionate self-responding. Such profiles, and whether they differ according to gender and their associations with mental health symptoms and emotion and cognitive tendencies, have not been examined in adolescence. Addressing this gap in knowledge is important given the high risk of mental illness at this vulnerable developmental life stage.
Self-Compassion and adolescence: theory and empirical findings
Gilbert (2009a) developed the three-circle affect regulation model of self-compassion. Specifically, Gilbert (2009a) proposes that self-compassion is a core feature of the self-soothing regulation system which serves a fundamental role in down-regulating emotion and encouraging recovery. This is in contrast to the drive (organisation of resources to motive toward a motivated goal) and threat (fight or flight response) regulation systems. Gilbert (2014) theorises that it is the inability to flexibly move between these affect regulation systems, often manifested as limited capacity to access the soothing system, that results in psychological distress and mental ill health. His theory is grounded in neuroscience, attachment theory and evolutionary psychology (Gilbert, 2014). According to Gilbert (2005, 2009a, 2014), self-compassion acts as a protective factor by increasing individuals’ capacity to access and activate the self-soothing system, resulting in balanced and adaptive responses to life’s adversities, rather than less-adaptive responses such as anger, shame, or intolerance of distress.
As mentioned earlier, self-compassion has been operationalised through the widely used self-report 26-item Self-Compassion Scale (SCS; Neff 2003a) and the shorter 12-item measure, which demonstrates near perfect correlation with the longer version (SCS-SF; Raes et al., 2011). Drawing on Buddhist philosophy, Neff, (2003b) defines self-compassion as a frame of mind comprised of six independent yet interacting sub-components. Self-kindness involves self-care and understanding as opposed to self-judgement, akin to harsh self-criticism. Mindfulness refers to a sense of equanimity and healthy acceptance and allowance of painful emotions, opposed to over-identifying and engaging in extreme reactions to such experiences. Finally, common humanity positions the individual to view their own experiences as part of a larger human experience and embrace the imperfection of life rather than feel isolated and alone in such experiences. These sub-components mutually interact as a dynamic system to create a self-response style (Neff, 2003a, 2019). Self-compassionate response styles appear to differ according to gender, with meta-analyses and large-sample studies finding that males report higher levels of self-compassion than females in adult (Yarnell et al., 2015, 2019) and adolescent samples (Bluth et al., 2017).
Emerging research suggests that self-compassion may serve as a protective buffer against mental illness in adolescent populations. This way of self-responding replaces harsh self-criticism, which is a key risk factor for many mental health diagnoses including depression (Gilbert et al., 2010) and problematic behaviours such as non-suicidal self-injury (Baetens et al., 2015). In adults, several meta-analyses have found self-compassion interventions result in significant reductions to a diverse range of mental health symptoms including anxiety, depression, disordered eating, and stress (Ferrari et al., 2019; Kirby et al., 2017). Specific to adolescents aged 10 to 19 years, a meta-analysis found a strong aggregate effect between lower self-compassion and higher psychological distress (comprised of a composite of anxiety, depression and stress outcomes; Marsh et al., 2018). Furthermore, self-compassion appears to serve as a protective buffer against mental health symptoms specifically during adolescence. Illustratively, self-compassion appears to weaken the links between perceived stress and internalising symptoms (Lathren et al., 2019), perfectionism and depression symptoms (Ferrari et al., 2018), and the link between academic difficulties and depressive symptoms (Lahtinen et al., 2020). Taken together, there is mounting evidence that self-compassion serves as a protective buffer against diverse symptoms of mental ill-health in adolescent populations and may be a suitable early intervention target.
In addition to immediate symptom alleviation (Ferrari et al., 2019; Kirby et al., 2017), self-compassion also appears to facilitate the cultivation of specific cognitive and emotional tendencies (Finlay-Jones, 2017; Inwood & Ferrari, 2018). A deficit in such skills are closely related to the presence of most psychological disorders, particularly mood disorders such as anxiety and depression (Campbell-Sills et al., 2006; Werner & Gross, 2010; Yap et al., 2018).Whereas responding to one’s self in a compassionate (rather than uncompassionate) approach appears to result in further development of such cognitive and emotional skills. For example, adolescents who tend to be self-compassionate are also more likely better able to recognise, label and manage their emotional state, all skills required when shifting from the threat or drive system to the self-soothing, self-compassion system (Gilbert, 2009b) An important cognitive and emotional skill relevant to adolescence is psychological flexibility. This refers to the ability the remain open and aware of the present moment and adapt to the demands of that moment whilst acting in accordance with one’s values and is an alternative to cognitive fusion and experiential avoidance (Greco et al., 2008; Hayes et al., 2009). It is likely that a greater tendency to be self-compassionate is related to greater psychological flexibility through encouraging a more balanced and realistic view of the world and oneself. Cognitive rumination, the tendency to fixate on negative or distressing thoughts, is closely related to self-criticism (McEvoy et al., 2010), and decreases in rumination are likely to be related to increased self-compassion. In addition, the ability to tolerate uncertainty is linked with greater psychological flexibility and resilience (Carleton et al., 2007). Distress disclosure is a further important skill during adolescence which refers to the likelihood of seeking help and confiding in others for support (Kahn & Hessling, 2001). These cognitive and emotional tendencies, including psychological flexibility, intolerance of uncertainty, rumination, and distress disclosure, are assessed in the current study.
Profile analyses of self-compassion sub-components in older populations and different cultural contexts
Distinct self-compassion psychological profiles using the SCS have been identified in Australian adults (Phillips, 2019). Latent profile analysis of the six SCS subscales was conducted in a large adult community sample (N = 353, Mage= 41.54, SDage= 16.11), and further validated in a second university student sample (N = 312, Mage= 35.43, SDage= 13.18) (Phillips, 2019). Across the two samples, three self-compassionate mindsets were identified as distinct groups. The uncompassionate responding group were high on uncompassionate subscales (self-judgement, isolation, and over-identification) and low on compassionate subscales (self-kindness, common humanity, and mindfulness); in contrast the highly self-compassionate group were high on compassionate subscales and low on uncompassionate subscales. A third group emerged, moderately self-compassionate, who scored in a moderate range across all six subscales. Group membership explained 28.3% of variance in well-being outcomes (including life satisfaction, resilience, depression, anxiety and stress), and 31.6% of variance in cognitive and emotional tendencies (including cognitive reappraisal, positive refocusing, rumination, suppression, self-blame, and difficulties in emotion regulation; Phillips, 2019). These self-compassion profiles suggest adults recruited from the community and university students have a greater diversity in their experience of compassionate and uncompassionate self-relating than merely being low or high in self-compassion.
Wu et al. (2020) also conducted a latent profile analysis of the SCS in 358 Chinese college students (Mage = 19.18 years), and found different profile structures compared to the Australian sample analysed by Phillips (2019). Wu et al. (2020) identified four distinct groups including dialectical thinking combined with high or low self-compassion; and nondialectical thinking combined with high or low self-compassion. Dialectical thinking is more common in Eastern than Western cultures. The authors define dialectical thinking as an ability to hold multiple, contradictory viewpoints simultaneously without a need to seek a resolution or react in a polarising way. In other words, both positive and negative emotions about the same event are accepted and viewed as important and meaningful. Across dialectical and nondialectical thinking, those with high self-compassion reported higher levels of positive psychological wellbeing (self-esteem, life satisfaction and resilience) and lower levels of negative psychological wellbeing (trait anger and depression) compared to the two groups with low self-compassion. The difference in distinct SCS profiles which emerged for the Australian sample analysed by Phillips (2019)and the Chinese sample analysed by Wu et al.’s (2020) may partially be explained by the significant difference in the cultural and social context of these populations. Although the six subscales of the SCS have been analysed for adult populations, and relevant profiles identified (Phillips, 2019; Wu et al., 2020), this has not yet been examined in adolescent populations.
Current study
Profile analyses of Neff’s six sub-components of self-compassion in adults (Phillips, 2019) and college students (Phillips, 2019; Wu et al., 2020) have identified distinct psychological profiles. These profiles did not differ according to gender, but did have meaningful differences in mental health symptoms, psychological wellbeing, and cognitive and emotional tendencies. An analysis of such self-compassionate and uncompassionate self-responding profiles during adolescence has not been conducted, and differences according to gender and psychological outcomes are unknown. The present study is the first to analyse a detailed profile analysis of psychological profiles of self-compassionate and uncompassionate self-responding in adolescence. It was hypothesised that;
-
1.
Adolescents would not be a uniform group in their style of self-responding; instead, profile analyses would identify distinct subgroups of self-compassionate and uncompassionate self-responding.
-
2.
Distinct profiles of compassionate and uncompassionate self-responding would differ for adolescents according to gender.
-
3.
Distinct profiles of compassionate and uncompassionate self-responding would differ in their associations with mental health outcomes (Perfectionism, Anxiety and Low Mood symptoms) and cognitive and emotional tendencies (Distress Disclosure, Intolerance of Uncertainty, Repetitive Thinking and Avoidance and Fusion cognitive patterns).
Method
Sample
This study used a convenience sample. Adolescents completed online questionnaires as part of a baseline measure for a larger psychoeducational intervention study (Einstein, 2022) which is ongoing, and a smaller subset of this data has been analysed elsewhere (n = 541; Ferrari et al., 2018). As the baseline data were collected prior to the intervention, these data reflect general functioning in a community sample and are not affected by the intervention of the larger study. Nine hundred and twenty-nine adolescents participated in the study (Mage = 13.70 years, SDage = 0.72, range = 12 to 16 years). Adolescents in grades seven to 10 were recruited from six private schools located in New South Wales and Canberra in Australia. These included three female-only, two male-only and one co-educational school.
Of the 1,998 students invited to participate in the study, 1,060 students and their parents provided informed written consent (53%). One hundred and nine participants were excluded for not providing any responses beyond the initial page of the questionnaire, and a further 22 were excluded for missing data on one of the variables of interest in the current study. Of the final sample (N = 929), 434 reported they were female (46.7%), and 495 were male (53.3%). Most students were born in Australia (n = 829, 89.2%), the next most common country of origin was the UK (n = 18, 1.9%), Hong Kong (n = 11, 1.1%) and China (N = 10, 1.1%). Most participants predominantly spoke English in their family home (n = 898, 96.7%), followed by Cantonese (n = 11, 0.01%).
Measures
Basic demographic information was collected including grade and school attended, age, gender language spoken at home and country of birth. The following measures were utilised in the current study.
The Self-Compassion Scale- Short Form (SCS-SF) is a 12-item measure demonstrating near perfect correlation with the longer 26-item original scale (r = .97; Raes et al., 2011). The measure includes reverse coded items, for example “When times are really difficult, I tend to be tough on myself.” Responses to each item use a 5-point Likert scale ranging from Almost Never (1) to Almost Always (5). The current study used the scores from the 6 subscales comprised of the mean of relevant items, with higher scores on the compassionate subscales reflecting stronger tendencies toward Kindness, Common Humanity and Mindfulness. The uncompassionate self-response subscales were not reverse scored to enable greater clarity in interpreting graphs of the results in the present study, and therefore higher scores on the uncompassionate subscales reflected stronger tendencies toward Self-Judgement, Isolation and Over-Identification.
The SCS-SF has been used extensively in adolescent populations, including samples with a mean age 14.7 years (Marshall et al., 2015), 15.6 years (Bluth et al., 2018) and a range of 12 to 16 years (Muris, 2016). Spearman Brown reliability coefficients were examined in the current study to assess the internal consistency of the six subscales given they were each comprised of two items (Eisinga et al., 2013). According to thresholds proposed by Koo and Li (2016), subscales ranged from moderate to good reliability for males (Self-Kindness rSB = 0.544, Self-Judgement rSB = 0.815, Common Humanity rSB = 0.631, Isolation rSB = 0.697, Mindfulness rSB = 0.731 and Over-identification rSB = 0.754), and females (rSB = 0.355, Self-judgement rSB =0.825, Common humanity rSB = 0.0649, Isolation rSB = 0.672, Mindfulness rSB = 0.647 and Over-identification rSB = 0.765), with the exception of Self-Kindness for females (rSB = 0.355).
Mental health outcomes
The Spence Children’s Anxiety Scale (Spence, 1998) is a 44-item self-report measure of anxiety symptoms developed for use with children and adolescents aged 10–18 years. Six of the 44 items are positive filter items designed to reduce negative response bias. It includes a total overall score of anxiety symptoms (maximum score = 114) comprised of the summation of all subscales. The six subscales of specific domains include separation anxiety, social phobia, obsessive-compulsive disorder, panic-agoraphobia, generalised anxiety, and fear of physical injury. Responders are asked to rate the frequency of experiencing each symptom on a 4-point Likert scale from Never (0) to Always (3), for example “I worry about things”. In the current study the SCAS had very good internal consistency for the overall total score (Cronbach’s α = 0.905).
The Short Mood and Feelings Questionnaire (SMFQ; Sharp et al., 2006) is a 13-item measure of depressive symptoms including low mood and low self-worth. Adolescents report how reflective symptoms are of their own experiences over the past two weeks using a 3-point Likert scale ranging from Not True (0) to Very True (2). Higher scores on the SMFQ are indicative of more severe depression symptoms. “I felt so tired I just sat around and did nothing” is a sample item. The internal consistency of this scale was very good in the present study (Cronbach’s α = 0.915).
The Children’s Automatic Negative Thoughts scale (Schniering & Rapee, 2002) includes two subscales; Social Threat and Personal Failure, which measure self-report negative self-statements and automatic thoughts. Items include “I’m afraid I will make a fool of myself” and “I am worthless” on a 5-point Likert scale from Not at all (0) to All the time (4), and ten items in each subscale are summed to produce a total score. The CATS has been used to discriminate between clinical and non-clinical adolescent samples, with both subscales correlating with clinical symptoms of social anxiety and major depression (Micco & Ehrenreich, 2009). In the current study, both subscales showed very good internal consistency (Social Threat Cronbach’s α = 0.948; Personal Failure Cronbach’s α = 0.948).
Cognitive and emotional tendencies
The Distress Disclosure Index (DDI; Kahn & Hessling, 2001) was developed to measure the tendency to conceal psychological distress from others, as opposed to disclosure. This 12-item measure produces a total score with higher scores reflecting a stronger tendency to disclose experiences of distress to others. The scale uses a 5-point Likert scale ranging from Strongly disagree (1) to Strongly agree (5). The DDI includes items such as “When I feel upset, I usually confide in my friends”. The internal consistency for the measure in the current study was acceptable (Cronbach’s α = 0.568).
The Intolerance of Uncertainty Scale – Short form (IUS-short; Carleton et al., 2007) is a 12-item scale which measures the tendency to consider the possibility of a negative event as unacceptable, regardless of the probability it will occur. This is a core feature of anxiety pathologies such as worry. The scale produces two sub scores; first prospective anxiety involving fear and anxiety based on future events, for example “Unforeseen events upset me greatly”. Secondly, inhibitory anxiety which refers to the tendency to inhibit action or experience due to uncertainty, for example “When I am uncertain I can’t function very well”. Items are scored on a 5-point Likert scale ranging from Not at all characteristics of me (1) to Entirely characteristic of me (5), with higher scores on both subscales reflecting greater pathology. The internal consistency for the measure in the current study was very good (Cronbach’s α = 0.893).
The Avoidance and Fusion Questionnaire for Youth (AFQ-Y; Greco et al., 2008) measures psychological inflexibility in adolescence including cognitive fusion, experiential avoidance and ineffective action in the presence of unwanted internal experiences, for example “I can’t be a good friend when I feel upset”. This 17-item measure asks responders to indicate how true each statement is for them on a 5-point Likert scale ranging from Not at all true (0) to Very true (1). The measure produces a total score, with higher scores reflecting greater psychological inflexibility. The AFQ-Y is a reliable measure of psychological flexibility in adolescents aged 12–18 years (Muris et al., 2017). The AFQ-Y also has high construct validity and is negatively linked to self-related concepts such as self-compassion and self-worth, and positively linked to psychopathological internalising symptoms (Muris et al., 2017). The internal consistency for the measure in the current study was very good (Cronbach’s α = 0.922).
The Repetitive Thinking Questionnaire (RTQ-10; McEvoy et al., 2010) is a brief transdiagnostic measure of repetitive negative thinking. The 10 items measure the extent an individual engages in such thinking patterns, independent of a disorder-specific diagnostic features (e.g., “I know I shouldn’t think about the situation, but can’t help it”). Items are rated on a 5-point Likert scale, ranging from Not true at all (1) to Very true (5). The RTQ-10 has high internal consistency (α = 0.89; McEvoy et al., 2018). The internal consistency for the measure in the current study was very good (Cronbach’s α = 0.941).
Procedures
The Human Research Ethics Committees of Macquarie University (reference: 5201500115) and the Australian Catholic University (reference: 2016-197R) approved the study. All students enrolled in participating grades and schools were invited to join the study and took home hardcopy information and consent forms to their primary carer. Participants were only included in the current study if both the student and their primary caregiver had signed and returned a consent form. During class time and under teacher supervision, students within each cohort were asked to sit quietly and independently complete the questionnaires online, using electronic tablets or laptops. The questionnaire was administered via the Qualtrics platform (Qualtrics, Provo, UT), and the measures were randomly presented to avoid order-effects. The questionnaire took approximately 60 min to complete. The students received no form of reimbursement for their participation.
Statistical analysis
In order to determine whether different profiles of self-compassion scores existed across adolescents and address the study’s first aim, latent profile analysis using Maximum Likelihood Estimation was undertaken using Mplus v 7 (Muthén & Muthén, 1998) on the six self-compassion subscale scores. To determine how many profiles appropriately fit the data, we undertook an iterative approach, starting with a single profile model and subsequently fitting models with an increasing number of profiles and evaluating the results. The decision of the number of profiles was made using both theoretical consideration and statistical indices of model fit using a number of different metrics (Ferguson et al., 2020; Tekle et al., 2016). The bootstrapped likelihood ratio test, the Vuong-Lo-Mendell-Rubin likelihood ratio test, and the Lo-Mendell-Rubin adjusted likelihood ratio test both assess whether a given number of profiles is a significantly better fit than the previous number of profiles (a statistically significant result indicates the more complex model is an improvement on the previous model) and were used as the primary statistical indices when deciding how many profiles to retain. AIC and sample-size adjusted BIC values were also interpreted as indices of relative model fit, where smaller numbers are desirable. Higher entropy values, closer to 1, are desirable, and the number of participants in the smallest profile should ideally be no smaller than 5% of the sample. Finally, if there was ambiguity in the statistical results, the log likelihood values were also plotted to determine when the decreasing values plateaued.
In order to address the study’s first aim of determining whether self-compassion profiles differed by gender, analyses were initially conducted on the entire sample with both males and females together, and once an acceptable number of profiles was found for the single group, test of model invariance was run to determine if the model differed by gender using the Satorra-Bentler scaled chi-square difference test using the log likelihood values (Satorra & Bentler, 2010). The result showed significant differences in model parameters by gender, TRd(35) = 872.98, p < .001, which does not support a single model fitted to both males and females. Subsequently, the latent profile analyses were conducted separately for males and females, which resulted in different profiles across the genders; these are the models presented in the results. Once the number of profiles were settled upon, the posterior probabilities were used to determine profile membership of each adolescent, and associations with mental health outcomes and cognitive and emotional tendencies were determined using independent samples t-tests and one-way ANOVAs with pairwise comparisons using Tukey’s test. Eta squared effect sizes are reported for all tests to allow for comparability.
Results
Comparison of self-compassion subscales by gender
We compared the self-compassion subscale responses for male and female participants to determine whether the data should be analysed separately according to gender. Across all six subscales of the SCS-SF, males and females reported significantly different levels of self-compassion, thus providing a rationale for separating further analyses by gender. Females consistently reported significantly higher scores for both the compassionate and uncompassionate subscales of the SCS-SF compared to males. Specifically, there was a significant difference in the Self-Kindness sub scores for male (M = 2.69, SD = 0.94) and female (M = 3.03, SD = 0.83) groups; t(927) = -5.88, p < .001, and the Self-Judgement sub scores for male (M = 2.43, SD = 1.09) and female (M = 2.71, SD = 1.01) groups; t(927) = -3.88, p < .001. Similarly, there was a significant difference in the Common Humanity sub scores for male (M = 2.56, SD = 1.00) and female (M = 2.80, SD = 2.80) groups; t(927) = -3.84, p < .001; and also the Isolation sub scores for male (M = 2.61, SD = 1.12) and female (M = 2.85, SD = 1.07) groups; t(927) = -3.30, p < .001. And finally, there was a significant difference in Mindfulness sub scores for male (M = 2.95, SD = 1.06) and female (M = 3.17, SD = 0.88) groups; t(927) = -3.52, p < .001; and Over Identification sub scores for male (M = 2.52, SD = 1.09) and female (M = 2.76, SD = 1.10) groups; t(927) = -3.32, p < .001.
Correlations
Prior to the latent profile analysis, correlations between SCS-SF scores and other measures were conducted for descriptive purposes, split by gender (see Table 1). For females, correlation patterns on the SCS-SF were largely as expected; the compassionate subscales of the SCS-SF (Self-Kindness, Common Humanity and Mindfulness) were positively correlated with each other, and negatively correlated with the uncompassionate subscales (Self-Judgement, Isolation, Over-Identification; see Table 1). The reverse also tended to be true, with uncompassionate subscales positively correlating with each other. The strongest correlations for females were reported between the uncompassionate subscales of the SCS-SF; Over-Identification and Self-Judgement (r(432) = 0.71, p < .01), and Over-Identification and Isolation (r(432) = 0.72 p < .01). Unexpectedly for males, all subscales of the SCS-SF were positively correlated with each other, the strongest correlation between Isolation and Over-Identification (r(493) = 0.78 p < .01).
Overall, for females the uncompassionate subscales of the SCS-SF tended to most highly correlate with both poorer mental health outcomes and cognitive and emotional tendencies. In contrast, for males both compassionate and uncompassionate subscales tended to significantly correlate with both categories of outcomes. Age was not significantly correlated with any outcomes for males and showed a significant yet very weak positive correlation with some SCS-SF subscales and cognitive and emotional tendencies for males.
Latent profiles analysis by gender
A range of models were fit to determine profiles of compassionate and uncompassionate self-relating for males and females separately. Full results from all models are presented in Table 2. As demonstrated in the table, the bootstrapped likelihood ratio test remained significant across all model comparisons, which can often occur (Ferguson et al., 2020), and limited the usefulness of this statistic in model selection; the other likelihood ratio tests, as well as other statistical parameters, were used instead in model selection.
For males, models containing between 1 and 5 profiles were fit. The 5-profile solution was not an improvement on 4 profiles according to two of the three likelihood ratio tests, and so we did not fit models beyond 5 profiles. The 3-profile solution was not a significant improvement on the 2-profile solution according to two of the likelihood ratio tests (although p-values were only marginally non-significant). The statistical results showed that the best profile pattern was either 2 or 4 profiles, and the pattern of scores for both the 2 and 4 profile solutions were reviewed considering the conceptual model of the three compassionate and three uncompassionate subscales of the SCS-SF, in addition to considering the logical clarity of these profiles. Given the entropy value was also highest for the 2-profile solution, the decrease in log likelihood values flattened off after 2, and that parsimony is desirable, we chose the 2-profile solution for the male adolescents.
As can be seen in Fig. 1a, both male profiles were not particularly differentiated between compassion and uncompassionate scores. Profile M1, labelled “Low Self-Relating”, was characterised by low scores (means ranged between 1 and 2 out of 5) on all compassion and uncompassionate subscales. Of the male sample, 111 (14%) individuals were classified into this profile. Profile M2, labelled “Moderate Self-Relating”, was characterised by average scores (means ranged from 2.5 to 3.5 out of 5) on all compassion and uncompassionate subscales. Most of the male sample (384 boys, 76%) were classified into this profile.
In contrast to the relative simplicity of the 2-profile male results, the female results showed a more complex pattern of compassionate and uncompassionate self-responding profiles; models containing between 1 and 6 profiles were fit to the female sample. Each model was a statistically significant improvement from 2 to 5 profiles. However, two of the three likelihood ratio tests indices showed no statistically significant improvement from 5 to 6 profiles. Therefore, a 5-profile result was deemed best fit on balance of the statistical indices. Two of the three likelihood ratio tests showed no significant improvement from the 5 to the 6-profile model, whereas each model was a significant improvement from 2 to 5 profiles. Scores from the 5-profile model were then interpreted.
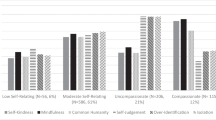
As can be seen in Fig. 1b, profile F1, labelled “Low Self-Relating”, was characterised by relatively low scores across all six subscales. Fifty females (12%) were classified into this profile. Profile F2, “Uncompassionate”, demonstrated high uncompassionate and low compassionate scores, indicating a tendency to be uncompassionate toward one’s self; 83 females (19%) were classified into this profile. Profile F3, “High Self-Relating”, included high scores across all six subscales of the SCS-SF, with no clear differentiation between compassion and uncompassionate self-relating; 69 females (16%) were classified into this profile. Profile F4, “Moderately Compassionate”, presented with slightly higher scores on compassionate subscales compared to uncompassionate subscales, indicating a tendency to relate to oneself compassionately, whilst also engaging in uncompassionate response styles. This was the largest profile with 174 (40%) of the sample. Finally, profile F5 “Highly Compassionate” is characterised by very low uncompassionate and high compassion self-relating scores and was comprised of 58 (13%) of the female sample.

Self-Compassion Profiles for Male (a) and Female (b) Adolescents
Note: SK = Self-Kindness, SJ = Self-Judgement, CH = Common Humanity, IS = Isolation, MI = Mindfulness, OI = Over Identification. Higher mean scores on all subscales reflect greater endorsement of that subscale
Using self-compassion profiles to predict mental health outcomes and cognitive and emotional tendencies
For females, the results of the ANOVAs were used to determine whether there were mental health and cognitive and emotional skill differences between the self-compassion profiles. These analyses showed distinct patterns, consistent across all outcomes (see Table 3 for full results, and Supplementary Information for figures). The Uncompassionate (F2) and High Self-Relating (F3) profiles consistently presented with the worst psychological outcomes. In contrast, the Low Self-Relating (F1) and Highly Compassionate (F5) profiles were consistently related to better psychological outcomes. The Moderately Compassionate (F4) profile were consistently related to moderate psychological outcomes. All effect sizes were large, demonstrating that self-compassion profiles were strongly associated with mental health outcomes and cognitive and emotional tendencies.
For males, there was a consistent difference in scores between the two profiles for all outcomes except distress disclosure as illustrated by independent samples t-tests (see Table 4, and Supplementary Information for figures). For all other mental health and cognitive and emotional skill measures, the Low Self-Relating profile (M1) showed better outcomes than the Moderate Self-Relating (M2). Effect sizes were mostly moderate to large, with the biggest difference seen in repetitive thinking, followed by avoidance and fusion, and low mood.
Discussion and conclusion
The central finding of this study was that the compassionate and uncompassionate elements of self-responding, as measured by the six subscales of the SCS-SF, interacted to create distinct self-compassion profiles across a large adolescent sample. This supported the first hypothesis as adolescents were not a uniform group in their style of self-responding. The second hypothesis was also supported. These profiles differed significantly between genders, with five profiles emerging for females and two for males. In females, the Highly Compassionate (F5) profile comprised of high endorsement of compassionate subscales and low endorsement of uncompassionate; the Moderately Compassionate (F4) profile included adolescents who were high in compassionate responding, but who also tended to engage in uncompassionate self-responding, and the Uncompassionate (F2) profile was characterised by high endorsement of the three uncompassionate subscales and low endorsement of the compassionate subscales. A Low Self-Relating (F1) profile featuring low endorsement of all six subscales and a High Self-Relating (F3) profile including high endorsement of all six subscales also emerged for females in the sample. In contrast, male adolescent response patterns on the SCS-SF yielded only two profiles. These male profiles shared some characteristics with the female profiles Low Self-Relating (F1) and High Self-Relating (F3). The Low Self-Relating (M1) profile reflected low endorsement of all six subscales, and the Moderate Self-Relating (M2) profile reflected moderately high endorsement of all six subscales. For both male profiles, responses across the six subscales of the SCS-SF did not tend to differ and were either consistently low or consistently moderate.
It is not clear why a different number of profiles emerged for female compared to male adolescents. Neither Phillips (2019) nor Wu et al. (2020) ran separate self-compassion profile analyses according to gender, however we examined gender separately in the current study due to significant differences in self-compassion responses for males and females identified in our preliminary analyses .A potential reason for the difference between males and females in the current study may include differences in cultural norms and expectations about self-response patterns and self-concept according to gender (Rankin et al., 2004). These gender norms and expectations may reflect those of broader Australian society. Societal perceptions of femininity tend to encourage the expression of greater nuance in recognising and labelling emotional states. In contrast, societal expectations of masculinity promote stoicism and suppression. These societal norms common to Western countries may partially explain the two male profiles which emerged; those who endorse emotional states and those who do not, compared to greater nuance in the five profiles of self-relating for females. The differences in gender profiles may also be a result of pubertal or hormonal differences (Pfeifer & Allen, 2020) or differences in emotion regulation ability (Broderick, 1998; De Boo & Spiering, 2010), with some research suggesting females mature and develop greater self-awareness earlier than males (Rankin et al., 2004; Zimmermann & Iwanski, 2014). This greater self-awareness in females may explain the greater diversity of self-reported self-compassion profiles for female adolescents compared to male in the current study.
The number of self-compassion profiles identified in adolescent males and females in the current study were notably different to those found in previous research (Phillips, 2019; Wu et al., 2020), and may reflect cultural and age differences in the samples analysed. The current study was based on a sample recruited from Australian high schools, the majority who were born in Australia (the next most common country of birth was the UK; 1.9%) and spoke English as a first language (next most common language was Cantonese, spoken by 0.01%), thus the self-compassion profiles which emerged may only apply to Caucasian Australian adolescents. In contrast, Phillips (2019) found a three profile solution in Australian university students and community adults; uncompassionate, moderately compassionate and highly compassionate. Thus, within the Australian context, different self-compassion profiles emerged for community adults (Phillips, 2019) and high school students (current study). Specific to the current study, adolescence is a developmental time of intense self-evaluation, and individuals are likely to experience fluctuations in their sense of self markedly different to adult populations. It may be the case that adults have developed a more consistent sense of self which translates into clearer self-compassion profiles of self-relating. This trend supports a developmental perspective of self-compassion differing across time and life stage.
In contrast to the three male and five female profiles which emerged in the current study, Wu et al. (2020) found four profiles in Chinese college students; dialectical thinking combined with high or low self-compassion; and nondialectical thinking combined with high or low self-compassion. It is interesting that across western (current study), and Eastern (Wu et al., 2020) samples, a similar self-compassion profile emerged; Low Self-Relating (current study) and dialectical thinking and low self-compassion (Wu et al., 2020). Dialectical thinking is an ability more commonly recognised in Eastern cultures compared to Western. As previously mentioned, it refers to an ability to accept contradictory viewpoints simultaneously with equanimity. The Low Self-Relating profile for males and females in the current study involved low endorsement of both self-compassionate and uncompassionate survey items and may reflect a form of dialectical thinking. It is unclear why this pattern of self-relating emerged in both a Chinese university sample and an Australian high school student sample, and may speak to identification of a common human experience. Nonetheless, the overall number of self-compassion profiles notably differed across these studies. Taken together, this body of research potentially indicates that compassionate and uncompassionate self-response patterns differ across the lifespan and by gender and by culture.
With respect to the third hypothesis, the results found that these profiles meaningfully predicted mental health outcomes including social and personal perfectionism, anxiety symptoms and depression symptoms. For females, the Uncompassionate (F2) and High Self-Relating (F3) profiles were consistently related to the poorer psychological outcomes including greater personal and social perfectionism, and greater anxiety and depression symptoms. This finding suggests that being high in self-compassion does not lead to further mental health benefits if the individual is also high in uncompassionate self-responses, as seen in the High Self-Relating (F3) profile. In contrast, the Compassionate (F5) as well as the Low Self-Relating (F1) profiles consistently reported the healthiest outcomes, including less social and personal perfectionism and fewer anxiety and depression symptoms. The Moderately Compassionate (F4) profile presented with moderate symptoms of mental ill-health compared to the other profiles. For males, the Low Self-Relating (M1) profile consistently reported better mental health outcomes compared to the Moderate Self-Relating (M2) profile. Effect sizes across these mental health outcomes tended to be large for females and moderate for males, indicating that both male and female profiles were robust in predicting such outcomes. The strength of the female profiles as predictor variables for mental health outcomes may be partially explained by the higher number of profiles increasing the ability of these profiles to explain more variance in outcomes.
An examination of differences in cognitive and emotional tendencies across the profiles also addressed the third hypothesis of this study. For female adolescents, the profiles predicted similar patterns in cognitive and emotional skill to the mental health outcome analyses. Uncompassionate (F2) and High Self-Relating (F3) profiles consistently reported a stronger tendency to engage in repetitive thinking, a poorer ability to tolerate uncertainty, lower likelihood to disclose distress to others and avoidant and fused cognitive thinking styles which consistently have been found to underpin a range of mental illnesses (Greco et al., 2008; Muris et al., 2017). In contrast, the Low Self-Relating (F1) as well as the Compassionate (F5) profiles consistently reported greater engagement in healthy cognitive and emotional tendencies including less repetitive, avoidant, and fused thinking styles, and greater ability to tolerate uncertainty and disclose distress to others. Like mental health outcomes, the Moderately Compassionate (F4) profile was associated with cognitive and emotional skill scores that fell between the four other profiles. Repetitive thinking was the most strongly associated with membership of the five different female profiles. Overall, this consistent pattern in females supports greater self-compassion and weaker uncompassionate self-response styles as resulting in greater engagement in healthier cognitive and emotional tendencies. Across both male profiles, healthier cognitive and emotional skill engagement mirrored the patterns evident in the mental health outcomes. Low Self-Relating (M1) profiles predicted less repetitive, avoidant, and fused thinking styles and greater tolerance of uncertainty compared to Moderate Self-Relating (M2). For males, distress disclosure, a potential indicator of adaptive help-seeking behaviour, did not significantly differ between the two profiles, indicating that both profiles are equally likely to disclose to others when feeling distressed.
Drawing these findings together, the female compassion and uncompassionate profiles identified in the current study were as expected given the theoretical structure of the SCS-SF (Raes et al., 2011). Across the five profiles, the three self-compassionate subscales garnered similar response patterns, and these tended to be independent of the three self-critical subscales, as seen in the Uncompassionate (F2), Moderately Compassionate (F4) and Compassionate (F5) profiles. However, two profiles which emerged in both males and females which require further consideration and interpretation. These were the Low Self-Relating (F1 and M1) profiles with low levels of endorsement across all six subscales of the SCS-SF, and High Self-Relating (F3) and Moderate Self-Relating (M2) profiles with high levels of endorsement across all six subscales. Neff (2019) clarifies that the six subscales are intended to interact to form a ‘systems level balance’ between compassionate and uncompassionate responses styles, and whilst it is a trend for increases in compassion subscales to coincide with decreases in uncompassionate self-responding (and vice versa), theoretically it is not improbable for response patterns to all six subscales to be similar, as is the case in the current findings. Taken together, these findings suggest all six subscales of the SCS-SF offer useful insight to the psychological functioning of adolescents. Importantly, the current study suggests the SCS-SF subscales act independently and use of a total score of the SCS-SF in future adolescent samples may not be meaningful, as argued by others (Brenner et al., 2017; López et al., 2015; Muris, 2016; Muris et al., 2016).
A potential interpretation of the Low Self-Relating (F1 and M1) and the High Self-Relating (F3 and M2) profiles for both genders is offered by Wu et al. (2020). The authors interpret a similar response pattern in Chinese college students to reflect a difference between dialectical thinking, an ability to hold multiple, contradictory viewpoints simultaneously, and nondialectical thinking which view contradictions as uncomfortable problems requiring resolution. Nondialectical thinking may be similar to self-ambivalence involving strong contradictory self-evaluations simultaneously (Riketta & Ziegler, 2006). Self-ambivalence refers to the co-presence of positive and negative self-evaluations, and is closely related to low self-esteem and a poor self-concept (Riketta & Ziegler, 2006). It may be the case that the High Self-Relating (F3) and Moderate Self-Relating (M2) profiles reflect nondialectical and self-ambivalent thinking, which involves greater polarisation of reactions to uncomfortable, contradictory cognitions, emotions, or experiences. In contrast, the Low Self-Relating (F1 and M1) profiles may reflect dialectical thinking styles, where the individual does not overidentify with either self-compassionate or self-critical thinking.
Indeed, many third-wave, evidence-based therapeutic interventions seek to cultivate a healthy non-attachment to internal experiences (cognitions, emotions, physiological reactions, etc.) which may be akin to a dialectical response style (Ciarrochi et al., 2020; Sahdra et al., 2017). An Acceptance and Commitment Therapy (ACT) approach seeks to cultivate psychological flexibility through mechanisms such as mindfulness and defusion, referring to the process of observing rather than getting caught up and ‘fused’ with our internal experience (Hayes et al., 2009). Similarly, Dialectical Behavioural Therapy (DBT) seeks to cultivate emotion regulation tendencies through targeting distress tolerance, acceptance and mindful awareness, all processes which arguably overlap with a dialectical response style (Linehan, 1991). The approach of these interventions appears to be supported by the results of the current study. A consistent pattern emerged for Low Self-Relating (F1 and M1) profiles in both genders to predict better mental health outcomes and healthier engagement in cognitive and emotional tendencies; and High Self-Relating (F3) and Moderate Self-Relating (M2) profiles related to poorer outcomes and strategies.
Implications and directions for future research and clinical practice
The findings of the current study have important theoretical and clinical implications, which also provide direction for future research. A key theoretical implication is the measurement of self-compassion in adolescent samples. Adolescents in the current study appear to systemically respond to the six facets of s the SCS-SF differently according to gender. The self-compassionate profiles identified in the female adolescent group reflect greater nuance and complexity than males. These differences based on gender align with a larger body of research calling for acknowledgement of gender when measuring self-compassion during both adulthood (Yarnell et al., 2015, 2019) and adolescence (Bluth et al., 2017). Taken together, this research suggests that failing to account for gender when measuring self-compassion may produce results which lack nuance and lose important variation in self-response styles between different genders. Across different profiles for females, those with higher self-compassion and lower uncompassionate self-responding tend to have better mental health outcomes and use more adaptive cognitive and emotional tendencies. In addition, males do not tend to differ in whether they are self-compassionate or self-critical, but rather differ in their level of attachment to both self-compassionate and self-critical response styles. In other words, a dialectical versus nondialectical approach to interacting with one’s internal experience better identifies meaningful profiles in males than levels of self-compassion, with better mental health and cognitive and emotional tendencies corresponding to a dialectical, or non-attached, way of relating oneself.
These gender differences may have important implications for self-compassion based interventions which target adolescent populations. The current findings suggest females who tend to have a more self-compassionate and weaker self-critical response style are more likely to experience positive mental health. These benefits include fewer anxiety and depression symptoms, lower levels of perfectionism, and healthier cognitive and emotional tendencies such as disclosing distress to others, tolerating uncertainty, avoiding repetitive thinking, and approaching distress (rather than avoiding), as well as defusing from unhelpful internal experiences. Importantly, high levels of self-compassion in females are not enough to result in these psychological benefits, high self-compassion must also be accompanied with low uncompassionate responding. The findings of the current study may be interpreted as support for the self-compassion construct to be an ideal target for psychological intervention for female adolescents in the general community. Psychological interventions which cultivate self-compassionate and reduce self-critical response styles may result in improvements in mental health and cognitive and emotional tendencies for female adolescents, as suggested by the profiles in the current study. Furthermore, the diversity of mental health outcomes and cognitive and emotional tendencies that were meaningfully predicted by self-compassion profiles also supports the view of self-compassion as an ideal intervention target when seeking to cultivate generalised psychological resilience. In other words, self-compassion appears to have a beneficial influence on a wide range of emotional and cognitive internal experiences.
In comparison, the clinical implications of the current study for male adolescents are less straightforward. The optimal mental health outcomes and cognitive and emotional tendencies for males were associated with the Low Self-Relating (M1) profile, which was low on both compassionate and uncompassionate response styles. This may suggest that for males it is more effective to target non-attachment to one’s inner experience rather than prioritising one style of self-responding over another. In addition, given that profiles for both genders meaningfully predicted both mental health outcomes and cognitive and emotional tendencies, the present study may indicate that identifying an adolescent’s self-relating style prior to intervention may help guide targeted treatment. These results question the benefits of current wellbeing initiatives that encourage deep reflection into psychological thinking for 12 to 14% of the teenagers in the classroom. Both Low Self-Relating profiles (F1 and M1; comprised of 12 and 14% of our sample respectively) showed that low self-relating was associated cross sectionally with less psychological dysfunction. Future research could further validate the use of the SCS-SF to identify self-compassion profiles in adolescents, and empirically assess whether certain profiles engage and benefit from psychological intervention differently.
Potential study limitations and conclusion
This study also involved several limitations which require acknowledgement. The self-compassion measure used was the SCS-SF, a 12-item short version of the original SCS (Raes et al., 2011). Although this version has been extensively used in adolescent samples (Bluth et al., 2018; Marshall et al., 2015; Muris, 2016), and demonstrates a near-perfect correlation with the longer 24-itemed scale (Raes et al., 2011), each subscale is comprised of only two items, and thus may be less sensitive to subtle differences in compassionate and uncompassionate response styles. Furthermore, self-report measures were used in the current study. Providing responses to multiple constructs in the same survey may lead to spurious correlations between items that are independent from ‘true’ effects due to similarity in response style, social desirability, or priming effects. In addition, this sample was homogenous; a community sample of Western adolescents aged between 12 and 16 years, the majority of whom were born in Australia (89.2%) and predominantly spoke English in their family home (96.7%). The limited cultural diversity in this sample indicates results may not readily generalise to those from different cultures, or populations experiencing clinical mental health symptoms. Furthermore, this study was based on a large cross-sectional data set. Whilst such data is useful for identifying relevant self-compassion profiles according to gender and mapping those profiles onto mental health outcomes and cognitive and emotional tendencies, future longitudinal research could assess the predictive strength of such profiles across time.
In conclusion, this study identified self-compassionate and unself-compassionate response profiles using the SCS-SF in a large adolescent cross-sectional sample. Two distinct profiles emerged for males which were characterised by low and moderate levels of compassionate and uncompassionate self-responding. The profile with lower levels of both consistently predicted better mental health outcomes and cognitive and emotional tendencies. In contrast, five more nuanced profiles emerged for females, and the profiles higher in self-compassionate responding consistently predicted better mental health outcomes and cognitive and emotional tendencies. These results confirm that for adolescent females, self-compassion is an important psychological construct with diverse mental health benefits, whereas for males, a lack of attachment to self-compassionate and self-critical response styles is linked with healthier psychological outcomes.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Baetens, I., Claes, L., Hasking, P., Smits, D., Grietens, H., Onghena, P., & Martin, G. (2015). The Relationship Between Parental Expressed Emotions and Non-suicidal Self-injury: The Mediating Roles of Self-criticism and Depression. Journal of Child and Family Studies, 24(2), 491–498. https://doi.org/10.1007/s10826-013-9861-8
Bluth, K., Campo, R. A., Futch, W. S., & Gaylord, S. A. (2017). Age and gender differences in the associations of self-compassion and emotional well-being in a large adolescent sample. Journal of Youth and Adolescence, 46(4), 840–853. https://doi.org/10.1007/s10964-016-0567-2
Bluth, K., Mullarkey, M., & Lathren, C. (2018). Self-compassion: A potential path to adolescent resilience and positive exploration. Journal of Child and Family Studies, 27(9), 3037–3047. https://doi.org/10.1007/s10826-018-1125-1
Brenner, R. E., Heath, P. J., Vogel, D. L., & Credé, M. (2017). Two is more valid than one: Examining the factor structure of the Self-Compassion Scale (SCS). Journal of Counseling Psychology, 64(6), 696. https://doi.org/10.1037/cou0000211
Broderick, P. C. (1998). Early adolescent gender differences in the use of ruminative and distracting coping strategies. The Journal of Early Adolescence, 18(2), 173–191. https://doi.org/10.1177/0272431698018002003
Cabral, M. D., & Patel, D. R. (2020). Risk Factors and Prevention Strategies for Anxiety Disorders in Childhood and Adolescence. In Y. K. Kim (Ed.), Anxiety Disorders. Advances in Experimental Medicine and Biology (Vol. 1191, pp. 543–559). Springer. https://doi.org/10.1007/978-981-32-9705-0_27
Campbell-Sills, L., Barlow, D. H., Brown, T. A., & Hofmann, S. G. (2006). Effects of suppression and acceptance on emotional responses of individuals with anxiety and mood disorders. Behaviour Research and Therapy, 44(9), 1251–1263. https://doi.org/10.1016/j.brat.2005.10.001
Carleton, R. N., Norton, M. A. P. J., & Asmundson, G. J. G. (2007). Fearing the unknown: A short version of the Intolerance of Uncertainty Scale. Journal of Anxiety Disorders, 21(1), 105–117. https://doi.org/10.1016/j.janxdis.2006.03.014
Ciarrochi, J., Sahdra, B. K., Yap, K., & Dicke, T. (2020). The Role of Nonattachment in the Development of Adolescent Mental Health: a Three-Year Longitudinal Study. Mindfulness, 11(9), 2131–2139. https://doi.org/10.1186/s40359-019-0342-8
De Boo, G. M., & Spiering, M. (2010). Pre-adolescent gender differences in associations between temperament, coping, and mood. Clinical Psychology & Psychotherapy, 17(4), 313–320. https://doi.org/10.1002/cpp.664
Einstein, D.A., McEvoy, P., McMaugh, A., Rapee, R.M., Abbott, M., Ferrari., M., & Karin, E. (2022). Insight study: Targeting Intolerance of Uncertainty in youth [Unpublished raw data.]
Eisinga, R., Te Grotenhuis, M., & Pelzer, B. (2013). The reliability of a two-item scale: Pearson, Cronbach, or Spearman-Brown? International journal of public health, 58(4), 637–642.
Ferguson, S. L., Moore, G., E. W., & Hull, D. M. (2020). Finding latent groups in observed data: A primer on latent profile analysis in Mplus for applied researchers. International Journal of Behavioral Development, 44(5), 458–468. https://doi.org/10.1177/0165025419881721
Ferrari, M., Hunt, C., Harrysunker, A., Abbott, M. J., Beath, A. P., & Einstein, D. A. (2019). Self-compassion interventions and psychosocial outcomes: A meta-analysis of RCTs. Mindfulness, 10, 1455–1473. https://doi.org/10.1007/s12671-019-01134-6
Ferrari, M., Yap, K., Scott, N., Einstein, D. A., & Ciarrochi, J. (2018). Self-compassion moderates the perfectionism and depression link in both adolescence and adulthood. PLOS ONE, 13(2), e0192022. https://doi.org/10.1371/journal.pone.0192022
Finlay-Jones, A. L. (2017). The relevance of self‐compassion as an intervention target in mood and anxiety disorders: A narrative review based on an emotion regulation framework. Clinical Psychologist, 21(2), 90–103. https://doi.org/10.1111/cp.12131
Gilbert, P. (2005). Compassion: Conceptualisations, research and use in psychotherapy. Routledge.
Gilbert, P. (2009a). Introducing compassion-focused therapy. Advances in Psychiatric Treatment, 15(3), 199–208. https://doi.org/10.1192/apt.bp.107.005264
Gilbert, P. (2009b). The nature and basis for compassion focused therapy. Hellenic Journal of Psychology, 6(3), 273–291.
Gilbert, P. (2014). The origins and nature of compassion focused therapy. British Journal of Clinical Psychology, 53(1), 6–41. https://doi.org/10.1111/bjc.12043
Gilbert, P., McEwan, K., Irons, C., Bhundia, R., Christie, R., Broomhead, C., & Rockliff, H. (2010). Self-harm in a mixed clinical population: The roles of self‐criticism, shame, and social rank. British Journal of Clinical Psychology, 49(4), 563–576. https://doi.org/10.1348/014466509X479771
Gilbert, P., & Procter, S. (2006). Compassionate mind training for people with high shame and self-criticism: Overview and pilot study of a group therapy approach. Clinical Psychology & Psychotherapy: An International Journal of Theory & Practice, 13(6), 353–379. https://doi.org/10.1002/cpp.507
Greco, L. A., Lambert, W., & Baer, R. A. (2008). Psychological Inflexibility in Childhood and Adolescence: Development and Evaluation of the Avoidance and Fusion Questionnaire for Youth. Psychological Assessment, 20(2), 93–102. https://doi.org/10.1037/1040-3590.20.2.93
Griffin, E., & McMahon, E. (2020). Adolescent mental health: Global data informing opportunities for prevention. EClinicalMedicine, 24, 100413. https://doi.org/10.1016/j.eclinm.2020.100413
Haggerty, R. J., & Mrazek, P. J. (1994). Reducing risks for mental disorders: Frontiers for preventive intervention research. National Academies Press.
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2009). Acceptance and commitment therapy. American Psychological Association Washington, DC.
Inwood, E., & Ferrari, M. (2018). Mechanisms of Change in the Relationship between Self-Compassion, Emotion Regulation, and Mental Health: A Systematic Review. Applied Psychology: Health and Well‐Being, 10(2), 215–235. https://doi.org/10.1111/aphw.12127
Kahn, J. H., & Hessling, R. M. (2001). Measuring the tendency to conceal versus disclose psychological distress. Journal of Social and Clinical Psychology, 20(1), 41–65. https://doi.org/10.1521/jscp.20.1.41.22254
Kieling, C., Baker-Henningham, H., Belfer, M., Conti, G., Ertem, I., Omigbodun, O., Rohde, L. A., Srinath, S., Ulkuer, N., & Rahman, A. (2011). Child and adolescent mental health worldwide: evidence for action. The Lancet, 378(9801), 1515–1525. https://doi.org/10.1016/S0140-6736(11)60827-1
Kirby, J. N., Tellegen, C. L., & Steindl, S. R. (2017). A meta-analysis of compassion-based interventions: Current state of knowledge and future directions. Behavior Therapy, 48(6), 778–792. https://doi.org/10.1016/j.beth.2017.06.003
Koo, T., & Li, M. (2016). Cracking the code: providing insight into the fundamentals of research and evidence-based practice a guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine, 15(2), 155–163.
Lahtinen, O., Järvinen, E., Kumlander, S., & Salmivalli, C. (2020). Does self-compassion protect adolescents who are victimized or suffer from academic difficulties from depression? European Journal of Developmental Psychology, 17(3), 432–446. https://doi.org/10.1080/17405629.2019.1662290
Lathren, C., Bluth, K., & Park, J. (2019). Adolescent self-compassion moderates the relationship between perceived stress and internalizing symptoms. Personality and Individual Differences, 143, 36–41. https://doi.org/10.1016/j.paid.2019.02.008
Linehan, M. M., Armstrong, H. E., Suarez, A., Allmon, D., & Heard, H. L. (1991). Cognitive behavioral treatment of chronically parasuicidal borderline patients. Archives of General Psychiatry, 48(12), 1060–1064. https://doi.org/10.1001/archpsyc.1991.01810360024003
López, A., Sanderman, R., Smink, A., Zhang, Y., van Sonderen, E., Ranchor, A., & Schroevers, M. J. (2015). A reconsideration of the Self-Compassion Scale’s total score: self-compassion versus self-criticism. PLOS ONE, 10(7), e0132940. https://doi.org/10.1371/journal.pone.0132940
Marsh, I. C., Chan, S. W., & MacBeth, A. (2018). Self-compassion and psychological distress in adolescents—a meta-analysis. Mindfulness, 9(4), 1011–1027. https://doi.org/10.1007/s12671-017-0850-7
Marshall, S. L., Parker, P. D., Ciarrochi, J., Sahdra, B., Jackson, C. J., & Heaven, P. C. (2015). Self-compassion protects against the negative effects of low self-esteem: A longitudinal study in a large adolescent sample. Personality and Individual Differences, 74, 116–121. https://doi.org/10.1016/j.paid.2014.09.013
McEvoy, P. M., Hyett, M. P., Ehring, T., Johnson, S. L., Samtani, S., Anderson, R., & Moulds, M. L. (2018). Transdiagnostic assessment of repetitive negative thinking and responses to positive affect: Structure and predictive utility for depression, anxiety, and mania symptoms. Journal of Affective Disorders, 232, 375–384. https://doi.org/10.1016/j.jad.2018.02.072
McEvoy, P. M., Mahoney, A. E. J., & Moulds, M. L. (2010). Are worry, rumination, and post-event processing one and the same?: Development of the repetitive thinking questionnaire. Journal of Anxiety Disorders, 24(5), 509–519. https://doi.org/10.1016/j.janxdis.2010.03.008
Micco, J. A., & Ehrenreich, J. T. (2009). Validity and specificity of the children’s automatic thoughts scale in clinically anxious and non-clinical children. Cognitive Therapy and Research, 33(5), 532–536. https://doi.org/10.1007/s10608-009-9230-5
Muris, P. (2016). A protective factor against mental health problems in youths? A critical note on the assessment of self-compassion. Journal of Child and Family Studies, 25(5), 1461–1465. https://doi.org/10.1007/s10826-015-0315-3
Muris, P., Meesters, C., Herings, A., Jansen, M., Vossen, C., & Kersten, P. (2017). Inflexible youngsters: Psychological and psychopathological correlates of the Avoidance and Fusion Questionnaire for Youths in nonclinical Dutch adolescents. Mindfulness, 8(5), 1381–1392. https://doi.org/10.1007/s12671-017-0714-1
Muris, P., Otgaar, H., & Petrocchi, N. (2016). Protection as the mirror image of psychopathology: further critical notes on the self-compassion scale. Mindfulness, 7(3), 787–790. https://doi.org/10.1007/s12671-016-0509-9
Muthén, L. K., & Muthén, B. O. (1998). Mplus userVs guide. In: Los Angeles, CA: Muthén & Muthén
Neff, K. D. (2003a). The development and validation of a scale to measure self-compassion. Self and Identity, 2(3), 223–250. https://doi.org/10.1080/15298860309027
Neff, K. D. (2003b). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85–101. https://doi.org/10.1080/15298860390129863
Neff, K. D. (2019). Setting the record straight about the Self-Compassion Scale. Mindfulness, 10(1), 200–202. https://doi.org/10.1007/s12671-018-1061-6
Neff, K. D., Tóth-Király, I., & Colisomo, K. (2018). Self-compassion is best measured as a global construct and is overlapping with but distinct from neuroticism: A response to Pfattheicher, Geiger, Hartung, Weiss, and Schindler (2017). European Journal of Personality, 32(4), 371–392. https://doi.org/10.1002/per.2148
Pfeifer, J. H., & Allen, N. B. (2020). Puberty initiates cascading relationships between neurodevelopmental, social, and internalizing processes across adolescence. Biological Psychiatry. https://doi.org/10.1016/j.biopsych.2020.09.002
Phillips, W. J. (2019). Self-compassion mindsets: The components of the self-compassion scale operate as a balanced system within individuals. Current Psychology. https://doi.org/10.1007/s12144-019-00452-1
Polanczyk, G. V., Salum, G. A., Sugaya, L. S., Caye, A., & Rohde, L. A. (2015). Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry, 56(3), 345–365. https://doi.org/10.1111/jcpp.12381
Raes, F., Pommier, E., Neff, K. D., & Van Gucht, D. (2011). Construction and factorial validation of a short form of the self-compassion scale. Clinical Psychology & Psychotherapy, 18(3), 250–255. https://doi.org/10.1002/cpp.702
Rankin, J. L., Lane, D. J., Gibbons, F. X., & Gerrard, M. (2004). Adolescent self-consciousness: Longitudinal age changes and gender differences in two cohorts. Journal of Research on Adolescence, 14(1), 1–21. https://doi.org/10.1111/j.1532-7795.2004.01401001.x
Riketta, M., & Ziegler, R. (2006). Self-ambivalence and self-esteem. Current Psychology, 25(3), 192–211. https://doi.org/10.1007/s12144-006-1003-7
Sahdra, B. K., Ciarrochi, J., Parker, P. D., Basarkod, G., Bradshaw, E. L., & Baer, R. (2017). Are people mindful in different ways? Disentangling the quantity and quality of mindfulness in latent profiles and exploring their links to mental health and life effectiveness. European Journal of Personality, 31(4), 347–365. https://doi.org/10.1002/per.2108
Satorra, A., & Bentler, P. M. (2010). Ensuring positiveness of the scaled difference chi-square test statistic. Psychometrika, 75(2), 243–248. https://doi.org/10.1007/s11336-009-9135-y
Schniering, C. A., & Rapee, R. M. (2002). Development and validation of a measure of children’s automatic thoughts: the children’s automatic thoughts scale. Behaviour Research and Therapy, 40(9), 1091–1109. https://doi.org/10.1016/S0005-7967(02)00022-0
Sharp, C., Goodyer, I. M., & Croudace, T. J. (2006). The Short Mood and Feelings Questionnaire (SMFQ): A Unidimensional Item Response Theory and Categorical Data Factor Analysis of Self-Report Ratings from a Community Sample of 7-through 11-Year-Old Children. Journal of Abnormal Child Psychology, 34(3), 365–377. https://doi.org/10.1007/s10802-006-9027-x
Spence, S. H. (1998). A measure of anxiety symptoms among children. Behaviour Research and Therapy, 36(5), 545–566. https://doi.org/10.1016/S0005-7967(98)00034-5
Tekle, F. B., Gudicha, D. W., & Vermunt, J. K. (2016). Power analysis for the bootstrap likelihood ratio test for the number of classes in latent class models. Advances in Data Analysis and Classification, 10(2), 209–224. https://doi.org/10.1007/s11634-016-0251-0
Werner, K., & Gross, J. J. (2010). Emotion regulation and psychopathology: A conceptual framework. In A. M. Kring, & D. M. Sloan (Eds.), Emotion regulation and psychopathology: A transdiagnostic approach to etiology and treatment. The Guilford Press.
Wu, Q., Chen, C., Liang, Y., Zhou, N., Cao, H., Du, H., Lin, X., & Chi, P. (2020). Not Only the Forest and Trees but Also the Ground They Are Rooted in: Identifying Profiles of Self-Compassion from the Perspective of Dialecticism. Mindfulness, 11(8), 1967–1977. https://doi.org/10.1007/s12671-020-01406-6
Yap, K., Mogan, C., Moriarty, A., Dowling, N., Blair-West, S., Gelgec, C., & Moulding, R. (2018). Emotion regulation difficulties in obsessive‐compulsive disorder. Journal of Clinical Psychology, 74(4), 695–709. https://doi.org/10.1002/jclp.22553
Yarnell, L. M., Neff, K. D., Davidson, O. A., & Mullarkey, M. (2019). Gender differences in self-compassion: Examining the role of gender role orientation. Mindfulness, 10(6), 1136–1152. https://doi.org/10.1007/s12671-018-1066-1
Yarnell, L. M., Stafford, R. E., Neff, K. D., Reilly, E. D., Knox, M. C., & Mullarkey, M. (2015). Meta-analysis of gender differences in self-compassion. Self and Identity, 14(5), 499–520. https://doi.org/10.1080/15298868.2015.1029966
Zimmermann, P., & Iwanski, A. (2014). Emotion regulation from early adolescence to emerging adulthood and middle adulthood: Age differences, gender differences, and emotion-specific developmental variations. International Journal of Behavioral Development, 38(2), 182–194.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ferrari, M., Beath, A., Einstein, D.A. et al. Gender differences in self-compassion: a latent profile analysis of compassionate and uncompassionate self-relating in a large adolescent sample. Curr Psychol 42, 24132–24147 (2023). https://doi.org/10.1007/s12144-022-03408-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-03408-0