
Abstract
Impairments in decision-making have been suggested as a predisposing factor to obesity development. Individuals with excess weight display riskier decisions than normal weight people. Furthermore, adolescence is a period of life in which risky behavior may increase. We aimed to investigate decision making applying the Outcome-Representation-Learning (ORL) model to the Iowa Gambling Task (IGT) in adolescents with excess weight. Twenty-nine excess weight and twenty-eight normal weight adolescents, classified according to their age-adjusted body mass index (BMI) percentile, participated in the study. Decision-making was measured using the IGT. A Bayesian computational ORL model was applied to assess reward learning, punishment learning, forgetfulness, win perseverance and deck perseverance. The IGT net score was lower in excess weight than normal weight adolescents (β = 2.85; p < .027). Reward learning (95% HDI [0.011, 0.232]) was higher, while forgetfulness (95% HDI [− 0.711, − 0.181]) and deck perseverance (95% HDI [− 3.349, − 0.203]) were lower, in excess weight than normal weight adolescents. Excess weight adolescents seemed better at learning the most rewarding choices and showed a random strategy based on reward and novelty seeking. Consequently, excess weight adolescents made more disadvantageous selections, and performed worse in the IGT.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nowadays, obesity is considered one of the most severe health problems worldwide. The World Health Organization (WHO) reported in 2016 that there were over 340 million children and adolescents with excess weight (World Health Organization, 2020). This growing prevalence is even more worrying if we take into account that overweight in childhood increases the probability of developing or maintaining obesity in adulthood (Suchindran et al., 2010). Furthermore, during childhood and adolescence, excess weight also causes several physical health problems (Sahoo et al., 2015) and has harmful psychosocial effects (Luppino et al., 2010; Moreno-Padilla et al., 2019; Sahoo et al., 2015).
Eating behavior as a decision-making proccess
Eating behavior is highly complex; beyond purely biological states (hunger and satiety), there is growing evidence that feeding behaviors are also modulated by decision-making processes (Ahima & Antwi, 2008; Chen et al., 2018) influenced by cravings or hedonic sensations, which may increase the incentive salience of food cues. Furthermore, the manner in which we perceive food and manage its intake has changed markedly in the last few decades due to the extreme psychosocial changes that have occurred in all western countries (Ludwig & Nestle, 2008). Specifically, unlimited access to foodstuffs and the readily availability of high-calorie foods in our “obesogenic” environments means that decision-making based on short-term rewards leads certain vulnerable individuals to overeat. People have to choose what, when and how much to eat, and this process is not always a healthy one; food intake may become a maladaptive and compulsive behavior.
Against this background, recent literature supports neurobiological and behavioral similarities between compulsive overeating and substances abuse, leading researchers to use the term ‘food addiction’ to describe this pattern of overeating (Blumenthal & Gold, 2010; Davis & Carter, 2009; Smith & Robbins, 2013; Volkow et al., 2013). These similarities are based on common brain mechanisms mediating the rewarding properties of natural rewards (like eating) and addictive drugs, leading to impaired decision-making (choice of short-term rewards) in both domains. In line with this, and in agreement with research on substance addictions, a recent review (Maxwell et al., 2020) reported that food addiction was also correlated with increased reward sensitivity and impulsivity.
Decision-making in adolescence
Adolescence is a critical period of life with respect to decision-making processes (Blakemore & Robbins, 2012), where teenagers are more likely to engage in risky behaviors such as dangerous driving, unprotected sex or substance abuse (Arnett, 1992; Greene et al., 2000). Structural magnetic resonance imaging (MRI) studies have explained this riskier decision-making in adolescence versus adulthood in terms of brain development, specifically citing the relative immaturity of prefrontal cortical control systems in adolescents, along with greater activation of the striatal areas in charge of reward processing and motivation (Ernst & Fudge, 2009; Galvan et al., 2006; Van Leijenhorst et al., 2010). The evidence points to a dissociation between the relatively slow, linear development of impulse control and response inhibition during this time versus the nonlinear development of the reward system, which is often hyper-responsive to rewards in adolescence (Giedd et al., 1999; Shaw et al., 2008). Furthermore, neuroimaging studies reported that decision-making abilities related to prefrontal cortex development continue to mature until 18–19 years of age (Konrad et al., 2013). This developmentally normative functional neurocircuitry could manifest behaviourally in robust incentive motivation (Luciana & Collins, 2012), reward reactivity (Galvan, 2010), and sensation seeking (Harden & Tucker-Drob, 2011), in association with the still-developing faculty of executive control.
According to the above, the available evidence points to a significant positive association between high sensitivity to rewards, as measured by self-report scales, and overeating, with a preference for high-fat and sweet food seen in adolescents in particular (De Cock et al., 2016; Loxton & Dawe, 2001). In line with this, Delgado-Rico et al (2012) also reported that reward sensitivity was the main predictor of elevated sensation seeking – an impulsivity measure – in adolescents with excess weight. A recent systematic review (Mamrot & Hanć, 2019) also supported the relationship between executive dysfunction and excessive body mass in children and adolescents. Therefore, as stated above, adolescents with excess weight could be more vulnerable to reward signals due to striatal predominance over the executive control system, leading to decision-making that is biased towards short-term rewards in adolescents with excess weight; consequently, it may be harder for them to resist highly rewarding palatable food.
Decision-making in people with overweight and obesity
One of the most widely used tasks to evaluate decision-making is the Iowa Gambling Task (IGT) (Bechara et al., 1994). This task has frequently been used to assess decision-making strategies in people with obesity (Brogan et al., 2010, 2011; Davis et al., 2010; Koritzky et al., 2012; Mallorquí-Bagué et al., 2016), and two recent meta-analyses (Rotge et al., 2017; Yang et al., 2018) concluded that adults with obesity performed worse on the IGT than healthy weight participants, especially in decisions under risk. These results suggest that excessive intake of highly palatable foods might be underpinned by an inability to successfully weigh the risks of reward and punishment (Fagundo et al., 2012). However, studies assessing decision making in adolescents with overweight and obesity are scarcer and show contradictory results. Concretely, two studies in adolescents reported that those with excess weight performed significantly worse in the IGT than normal weight adolescents, and showed a clear preference for disadvantageous risky decks (Verbeken et al., 2014; Verdejo-García et al., 2010). However, another study of overweight and normal weight adolescents showed no group differences in decision-making after a social stressor (Verdejo-Garcia et al., 2015). More studies are needed in this field to improve understanding and differentiation of the possible cognitive processes underlying performance on the IGT in this population.
Computational models to evaluate cognitive processes during decision-making
In this line, the classical method to analyze the IGT provides a score that represents a unidimensional construct of decision-making. This unidimensional construct shows whether a participant is able to understand the contingencies of the task and make choices with consideration of the consequences, and whether the participant’s decisions are risky or not. However, decision-making is not a single entity; rather, it involves several neurocognitive processes. For a better understanding of the decision-making process, a popular framework developed for the fields of economics, psychology and machine-learning, called value-based decision-making (Rangel et al., 2008), posits that (i) our brain assigns a subjective value to each available choice, then (ii) selects the option with the highest value (i.e., the most rewarding one), and finally (iii) updates the values of the options based on actually experienced outcomes (i.e., learning).
These cognitive processes can be extracted from the IGT using computational models (Ahn et al., 2008; Busemeyer & Stout, 2002; d’Acremont et al., 2009; Worthy et al., 2013). Haines et al. (2018) recently proposed the Outcome-Representation Learning (ORL) model, a novel reinforcement learning model that explicitly accounts for the effects of expected value, gain–loss frequency, choice perseveration, and reversal learning processes. The five processes/parameters in the ORL model can be summarized as follows: reward learning (Arew), or the propensity to learn faster regarding the rewards of each deck, where higher values imply faster learning of the reward contingencies; punishment learning (Apun), or the propensity to learn faster regarding the punishments of each deck, where higher values imply faster learning of punishment contingencies; forgetfulness (K), or the speed at which people forget their previous choices of decks and the associated outcomes, where lower values imply longer-lasting memories of the past choices; win perseverance (BF), i.e., whether people persist in choosing decks with higher win rates [here, values below 0 represent perseverance with decks with lower win rates (A and C) and values above 0 represent perseverance with decks with higher win rates (B and D)]; and deck perseverance (BP), i.e., whether people prefer one deck or switch between decks [here, values below 0 imply a preference to switch (sometimes in a random manner) and values above 0 imply perseverance with the same decks]. The ORL model outperformed past learning reinforcement models (such as the Prospect Valence Learning and Value-Plus- Perseverance models) in terms of prediction accuracy and parameter recovery (Haines et al., 2018).
As we explained before, the fact of eating something with more or less calories may be considered a decision; as well as the fact of eating a larger or smaller quantity is another decision. Indeed, people with problems such as overweight, obesity or binge eating show greater levels of food addiction, which is highly related to decisions guided by reward seeking. In this sense, people with higher values of reward learning (Arew) may be more vulnerable to food addiction, and in consequence, more vulnerable to excess weight and obesity. To improve understanding of this altered process, using computational models based on value-based decision-making, such as ORL, help us to determine not only whether people exhibit good or bad decision-making performance, but also how is the feedback processing (reward seeking and punishment avoidance) during the process. Thus, by applying this model to the study of eating behavior and, in particular, to the study of subjective hedonic experience, we can better understand why appetite regulation may be compromised in adolescents, whose food decision-making process is biased towards the most rewarding choices. As also discussed above, adolescence is a critical period in terms of brain development, particularly as it pertains to executive function (i.e., decision-making) and reward/sensation seeking. In the ORL model, random choices between decks, measured by values lower to 0 in deck perseverance (BP), implies that decisions are guided by greater sensation seeking. Thus, adolescents with higher reward sensitivity and sensation seeking may be more vulnerable to compulsive overeating. Therefore, we consider that given the relevance of the problem and the fact that alterations in decision-making seem to contribute not only to the progression of obesity, but also to significant limitations in weight control efficacy (Biddle & Dovey, 2009), it seems truly urgent to deepen the knowledge of the decision-making process in this population.
Aim and hypotheses
Thus, this study is the first one to use a novel reinforcement learning model –the ORL model- to analyze the cognitive processes underlying decision-making in adolescents with excess weight during performance of the IGT. Based on the value-based decision-making model (Rangel et al., 2008), we hypothesize that, for overweight adolescents, the salience of disadvantageous choices will be increased, in association with enhanced learning of these disadvantageous selections due to their higher short-term rewarding value. In agreement with previous studies (Verbeken et al., 2014; Verdejo-García et al., 2010), this will lead to greater reward learning and poorer performance during the IGT in overweight compared to normal weight adolescents. Furthermore, since adolescents with excess weight seem to show higher short-term reward-related sensation seeking scores (Delgado-Rico et al., 2012), we also hypothesize lower perseverance decks scores in our overweight sample, which may also imply a more random strategy, in turn linked to a more extensive search for novel task outcomes in this sample.
Methods
Participants
A total of 57 adolescents (35 females, age range: 13 to 18 years, mean ± SE = 15.40 ± 0.21) were recruited from high schools located in Jaén (Spain). The researchers visited all the high schools in Jaén, asked the director for permission to enter the classrooms and give the relevant information of the study (characteristics of the study and contact data to participate) to the students. Adolescents who wanted to participate contacted to us and were divided into two groups (normal and excess weight) according on their age-adjusted body mass index (BMI) percentile, in accordance with the guidelines of the International Obesity Task Force (Cole & Lobstein, 2012). The groups were balanced according to age and gender. The normal weight group was composed of 28 participants, with age-adjusted percentiles between the 5th and 84th. The excess weight group was composed of 29 participants, with age-adjusted percentiles ≥ 85th. The inclusion criteria were: (i) aged between 13 and 18 years; and (ii) no current or history of neurological disorders, psychiatric disorders or drug/alcohol dependence or abuse; and (iii) no history of eating disorders (measured using the Eating Disorder Inventory [EDI-2]). All participants had normal or corrected to-normal vision.
The Iowa Gambling Task
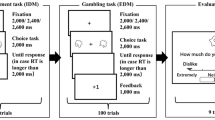
Participants completed a computerized version of the IGT (Bechara, 2007). This task evaluates decision- making under uncertain conditions. Participants start with 2000 € and should gain as much money as possible. For this purpose, they must choose among four decks of cards: two disadvantageous decks (Decks A and B) that provide short-term rewards but greater future losses (long-term loss), and two advantageous decks (Decks C and D) that provide short-term lower rewards but smaller future losses (long-term gain). The B and D decks provide a high percentage of small wins (90%) and a low percentage (10%) of big punishments, while decks A and C provides moderate wins and losses (both 50%). After each trial (n = 100 in total), the software provides monetary feedback to the participants. IGT performance was determined using the Iowa Gambling (IG) index, as the difference between the number of trials with a card chosen from the advantageous decks minus the number of trials with a card chosen from the disadvantageous decks (CD − AB). The IG index is calculated for blocks of 20 trials, to determine whether participants show progressive learning during the task, and for all 100 trials. The total number of occasions on which each deck was chosen was also calculated.
The outcome-representation learning model
The ORL (Haines et al., 2018) was used to decompose decision-making during the IGT into five components: i) reward learning (Arew; from 0 to 1), where higher values represent faster reward outcome learning; ii) punishment learning (Apun; from 0 to 1), where higher values represent faster learning about punishment outcomes; iii) forgetfulness (K; from 0 to 242) is a decay parameter indexing how quickly people forget their past deck choices, where higher and lower values represent relatively shorter and long memories, respectively, of their own choices; iv) perseverance in wins (BF; from—∞ to + ∞), where mostly negative values (below 0) indicate greater perseverance for decks with a low win frequency (Decks A and C), while mostly positive values (above 0) indicate greater preference for decks with a high win frequency (Decks B and D); and v) deck perseverance (BP; from—∞ to + ∞), where mostly negative results (below 0) imply a preference for switching decks (more random responses), and mostly positive results (above 0) imply a perseverance for the same deck.
Procedure
After obtaining permission from the high school’s directors, the study was presented to each class of students and their participation was requested. Those who were interested in participating sent us their informed consent form after it had been signed by their parents. Height and weight were self- reported by participants and they were assigned to a group depending on their BMI. Then, an experimental session was scheduled for each participant. Sessions started at 4 p.m. BMI was calculated again in the laboratory, based on the exact height and weight data collected on arrival. Body composition measures were also collected using the Bodystat®1500 monitoring unit. The EDI-2 (Garner, 1998), validated for use in young people, was administered to rule out eating disorders (binge eating, anorexia nervosa, and bulimia nervosa). Subsequently, the participants completed a computerized version of the IGT. The computer screen size was 15.4 inches, and each participant was located at a distance of 65-70 centimetres from the screen to guarantee good visual acuity. The Ethics Committee for Human Research of the Universidad de Jaén approved the study.
Statistical analyses
The Chi-square test (for qualitative variables) and Student’s t-test (for quantitative variables) were applied to determine if there were differences between groups in age, gender, BMI and body fat percentage. To analyze the behavioral data (results of the IGT), a growth model was used with the IG index as the dependent variable, fixed effects of Block (Block 1 to Block 5), Group (Excess weight / Normal weight) and the Block*Group interaction, and the intercept as a random effect. Fixed effects omnibus test degrees of freedom were corrected using the Satterthwaite method. Simple effects for polynomials were tested by Group in order to understand the learning curve for each group. Post-hoc comparisons were adjusted based on the false discovery rate (FDR).
As no previous study using computational models has been conducted on the IGT performance of excess weight adolescents, we first compared four existing computational models available in the hBayesDM package using hierarchical Bayesian analysis (HBA) (Ahn et al., 2017), in order to determine whether the ORL model has the best fit. The four models were as follows: the “Prospect- Learning Valence with the Delta rule” (PVL-Δ) model, the “Prospect-Learning Valence with the Decay rule” (PVL-D) model, the “Value-Plus-Perseverance” (VPP) model and the ORL model. To perform HBA, we used the R package hBayesDM with RStan 2.19.3 for sampling the posterior distribution. The Markov chain Monte Carlo (MCMC) sampling algorithm used by Stan is the Hamiltonian Monte Carlo (HMC). A total of 20,000 samples were used after 10,000 burn-in samples were obtained for four chains (10,000 × 4 chains = a total of 40,000 samples; with 40,000 burn-in samples) for each model. For each parameter, the Gelman-Rubin test (Gelman & Rubin, 1992) was used in order to check the convergence of the chains (aka. Ȓ). All model parameters had Ȓ values of 1.00, here Ȓ values close to 1.00 indicate that the MCMC chains converge to the target distribution. We also performed a visual inspection of the chains in order to corroborate convergence to the target distribution. Model comparison was performed using the leave-one-out information criterion (LOOIC), to determine the model with the best fit to the data (Vehtari et al., 2017). Parameters for the best-fitting model were estimated for each individual to compare the excess weight and normal weight groups. The posterior distribution mean and standard deviation of the parameters were calculated for each group. We used the posterior highest density interval (HDI), which is the range of parameter values having higher probability to be at 95%, in order to make decisions regarding the group comparisons. If the HDI posteriors exclude 0, the comparison is considered significant. All statistical analyses were performed using R 3.4.2 software.
Results
Demographic and anthropometric variables
Comparison of the demographic characteristics (Table 1) did not reveal differences in age or gender between groups. Conversely, BMI and body fat percentage were, as expected, significantly higher in the excess weight group.
IGT behavioural results
The omnibus test showed a significant main effect of Group (β (SE) = - 2.85 (1.26), F1, 55 = 5.14, p < .027), in which excess weight adolescents displayed lower scores for the IG index (mean ± SE = - 2.98 ± .88) than normal weight adolescents (mean ± SE = - .13 ± .89), indicating a preference for disadvantageous decks in the excess weight group. Moreover, a trend in the Block*Group interaction was observed (F1, 220 = 2.27, p = .062). The difference between groups in linear growth was significant (β (SE) = - 2.82 (1.33), p < .035); the quadratic, cubic and quartic trend differences were not significant (all ps > .05). Simple effects analysis showed positive linear growth in the normal weight group (β (SE) = 2.67 (.95), p < .005); however, linear growth was not significant in the excess weight group (p > .05). Post-hoc comparisons showed poorer performance in the excess weight compared to the normal weight group in the second part of the IGT, with significant group differences in block 5 (β (SE) = - 3.07 (1.48), p < .027) and a trend in block 4 (β (SE) = - 2.89 (1.53), p < .054). All other blocks showed no significant group differences (all ps > .05) (Fig. 1). Therefore, normal weight adolescents learned the contingencies of IGT, increasing their preference for advantageous decks, but, excess weight adolescents show the same preference for disadvantageous decks thorough the task.

IG index of the five blocks of 20 trials/each (mean ± SE) for the two groups: excess weight and normal weight adolescents. Note: * = p < 0.050;.t = p < 0.070
IGT computational models
The comparisons between the four computational models showed that ORL model has the best fit (Table 2). Thus, we used the ORL model to examine group differences in the parameters of interest.
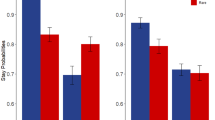
After sampling the posterior distributions, comparison of the ORL model components between groups indicated that reward learning (Arew) values were significantly higher in the excess weight group than in the normal weight group (Table 3). Conversely, excess weight adolescents had significantly lower values for forgetfulness (K) and perseverance (Bp) than normal weight adolescents. Table 3 shows the posterior mean ± SD for each group and the 95% HDI values. Figure 2 shows the posterior distributions of the five parameters in each group. Thus, excess weight adolescents learned faster about the rewards of IGT, remember longer memories of their own choice and made more random decisions during the task than normal weight adolescents.

Posterior distributions for each group (Excess weight; Normal weight) of the five components estimated from the IGT using the ORL model: ARew = Reward learning, APun = Punishment learning, K = forgetfulness, βF = Win perseverance, βP = Deck perseverance
Discussion
Adolescents with excess weight displayed deficits in decision-making. On the one hand, their IGT total score was lower compared with normal weight adolescents. On the other hand, the ORL (the model with the best fit) components showed that excess weight adolescents have greater reward learning (Arew) and lower forgetfulness (K) and perseverance (Bp) than the normal weight adolescents.
Regarding IGT score, a trend towards poorer performance was also observed in the second part of IGT in excess weight group. In the first part of the IGT, participants have to make decisions under ambiguity (i.e., without knowledge of the contingencies of the different options) whereas decisions under risk (i.e. with knowledge of such contingencies) have to be made in the second part of the task. These results are in agreement with previous studies showing similar impairments and riskier decisions in the IGT in excess weight adolescents (Verbeken et al., 2014; Verdejo-García et al., 2010). Furthermore, a recent meta-analysis (Rotge et al., 2017) reported that decisions under risk, but no decisions under ambiguity, were affected in the obesity group in comparison to the control group. In this line, Moreno-Padilla et al. (2018a) reported higher risk-taking in excess weight adolescents in the Balloon Analogue Risk Task.
The ORL components showed that excess weight adolescents have greater reward learning (Arew). Associations between sensitivity to reward and eating behavior have been widely reported (Davis et al., 2004; Franken & Muris, 2005; Loxton & Dawe, 2001). Specifically, sensitivity to reward was significantly related to greater food craving and BMI in adult women (Davis et al., 2004; Franken & Muris, 2005). Regarding adolescents, a study found that adolescent girls with greater sensitivity to reward cues were more likely to engage in binge-eating behaviors, thus predicting dysfunctional eating (Loxton & Dawe, 2001). Furthermore, exposure to high-calorie food cues in adolescents with overweight is associated with greater striatal-limbic activation relative to normal weight adolescents, suggesting the importance of the motivational-reward system in their eating behavior (Jastreboff et al., 2014; Moreno-Padilla et al., 2018b; Stice et al., 2008). In line with this, Moreno-Padilla et al. (2018b) found that excess weight adolescents showed greater striatal-limbic system activation than normal weight adolescents when choosing between appetizing and standard food cues. This pattern of activation correlated with food craving and behavioral food choices in the context of appetizing foods. This is the first study of excess weight adolescents to analyze reward sensitivity in terms of learning during decision-making in the IGT. According to the value-based decision-making model (Rangel et al., 2008), alterations in this process can enhance reward learning, which may increase the preference for disadvantageous decks.
Adolescents with excess weight also showed lower levels of forgetfulness (K) in their IGT performance. There is no previous literature on the role of this cognitive process in decision-making in excess weight samples. The lower levels of forgetfulness in the IGT, in the context of better learning of reward contingencies in this population, indicated a tendency to prioritize rewards over punishments and, consequently, remembrance of winnings rather than losses. This bias involves a persistent preference for disadvantaged decks that bring immediate rewards but with detrimental long-term consequences. In the eating behavior context, there would be a higher likelihood of memorizing highly rewarding rather than healthy food, which together with the increased reward learning would lead to choosing food high in fat and/or sugar more frequently, thus favoring additional weight gain.
Finally, overweight adolescents showed a strong preference toward switching in the IGT, as opposed to perseverating (Bp) on specific decks. In this line, our group of excess weight adolescents may show riskier choices on the IGT not only because of their greater reward sensitivity, but also because of their tendency to seek novelty. Although our excess weight adolescent learnt about reward contingencies more rapidly, they seemed to choose the decks more randomly, which may be explained by their greater engagement in exploratory and sensation seeking behaviors. Delgado-Rico et al (2012) also reported greater short-term reward-related sensation seeking in adolescents with excess weight. This bias implies that they fail to understand the game's strategy, relying more on short-term rewards and novelty seeking and, ultimately, showing increased risk-based, impulsive decision-making. Furthermore, this lack of perseveration and the tendency toward switching on the IGT could also explain their difficulties in following a strict healthy diet, and their higher likelihood to switch their food choices and give up demanding diets. To sum up, the observed cognitive processes in excess weight adolescents (greater reward learning, and less forgetfulness and perseveration) converge to promote riskier choices, which could translate to harmful eating behaviors and increased risk of developing or maintaining obesity.
Haines et al (2018) applied the ORL model to the data of 393 substance abusers, collected across multiple research sites, and found similar results to ours. Chronic cannabis users were more sensitive to rewards (reflected in higher reward learning rates) and showed less perseveration (irrespective of the value of each deck) than healthy controls. These similar decision-making results between overweight and substance-using samples are consistent with the growing evidence supporting the concept of “food addiction” (Volkow et al., 2013). According to this perspective, obesity and drug addiction can be defined as conditions in which the saliency of a specific type of reward (food and drugs, respectively) becomes overstated relative to, and at the expense of, other rewards.
Regarding the limitations of this study, there are a number of issues that need to be addressed in future studies, including differentiating among obese (≥ 95th age-adjusted percentile), excess weight (≥ 85th and ≤ 95th age-adjusted percentile) and normal weight (5th to 84th age-adjusted percentile) participants, to analyse possible differences according to the degree of overweight. It will also be necessary to analyse differences in decision-making between adolescents and adults with excess weight, to discern if the observed deficits are attenuated with the development of the frontal lobes in adulthood. Finally, our study lacks of a longitudinal analysis which evaluates the long-term influence of these decision- making deficits on weight gain in these adolescents. These long-terms effects are very important in order to determine whether adolescents with overweight eventually become adults with obesity.
In summary, our findings confirmed greater reward sensitivity during decision-making (IGT) in adolescents with excess weight compared to normal weight adolescents. Furthermore, the lower forgetfulness and perseveration in excess weight adolescent corroborated their poorer performance on the IGT. Adolescents with excess weight seem to remember rewarding experiences more readily and use maladaptive strategies in the IGT, including more random and novelty seeking-focused ones, thus leading to reduced task performance. These innovative results deepen knowledge of the cognitive processes that underlie IGT performance in excess weight adolescents and confirm the essential role of reward sensitivity in decision-making strategies. Excess weight in adolescence is a risk factor for the development of future health problems and obesity. Furthermore, alterations in decision-making seem to contribute not only to the progression of obesity, but also to significant limitations in weight control efficacy. For instance, Biddle and Dovey (2009) reported that decision-making deficits may lead to failure of weight loss interventions. Therefore, in our modern societies, given the high availability of, high-calorie foods, decision-making plays an essential role in maintaining healthy eating behaviors. Thus, designing interventions aimed at reducing reward sensitivity and increasing inhibitory control to improve decision-making process in this population is advisable.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Code availability
Code generated are available from the corresponding author on reasonable request.
References
Ahima, R. S., & Antwi, D. A. (2008). Brain regulation of appetite and satiety. Endocrinology and Metabolism Clinics of North America, 37(4), 811–823. https://doi.org/10.1016/j.ecl.2008.08.005
Ahn, W.-Y., Haines, N., & Zhang, L. (2017). Revealing neurocomputational mechanisms of reinforcement learning and decision-making with the hBayesDM package. Computational Psychiatry, 24-57. https://doi.org/10.1162/CPSY_a_00002
Ahn, W. Y., Busemeyer, J. R., Wagenmakers, E. J., & Stout, J. C. (2008). Comparison of decision learning models using the generalization criterion method. Cognitive Science, 32, 1376–1402. https://doi.org/10.1080/03640210802352992
Arnett, J. (1992). Reckless behavior in adolescence: A developmental perspective. Developmental Review, 12(4), 339–373. https://doi.org/10.1016/0273-2297(92)90013-R
Bechara, A. (2007). Iowa Gambling Task Professional Manual. Psychological Assessment Resources, Inc.
Bechara, A., Damasio, A. R., Damasio, H., & Anderson, S. W. (1994). Insensitivity to future consequences following damage to human prefrontal cortex. Cognition, 50, 7–15. https://doi.org/10.1016/0010-0277(94)90018-3
Biddle, S., & Dovey, T. (2009). Obesity - is physical activity the key? Psychologist, 22(1), 32–35.
Blakemore, S. J., & Robbins, T. W. (2012). Decision-making in the adolescent brain. Nature Neuroscience, 15(9), 1184–1191. https://doi.org/10.1038/nn.3177
Blumenthal, D. M., & Gold, M. S. (2010). Neurobiology of food addiction. Current Opinion in Clinical Nutrition & Metabolic Care, 13(4), 359–365. https://doi.org/10.1097/MCO.0b013e32833ad4d4
Brogan, A., Hevey, D., O’Callaghan, G., Yoder, R., & O’Shea, D. (2011). Impaired decision making among morbidly obese adults. Journal of Psychosomatic Research, 70(2), 189–196. https://doi.org/10.1016/j.jpsychores.2010.07.012
Brogan, A., Hevey, D., & Pignatti, R. (2010). Anorexia, bulimia, and obesity: Shared decision making deficits on the Iowa Gambling Task (IGT). Journal of the International Neuropsychological Society, 16(4), 711–715. https://doi.org/10.1017/S1355617710000354
Busemeyer, J. R., & Stout, J. C. (2002). A contribution of cognitive decision models to clinical assessment: Decomposing performance on the Bechara gambling task. Psychological Assessment, 14(3), 253. https://doi.org/10.1037/1040-3590.14.3.253
Chen, R., Li, D. P., Turel, O., Sørensen, T. A., Bechara, A., Li, Y., & He, Q. (2018). Decision making deficits in relation to food cues influence obesity: A triadic neural model of problematic eating. Frontiers in Psychiatry, 9, 264. https://doi.org/10.3389/fpsyt.2018.00264
Cole, T. J., & Lobstein, T. (2012). Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatric Obesity, 7(4), 284–294. https://doi.org/10.1111/j.2047-6310.2012.00064.x
d’Acremont, M., Lu, Z. L., Li, X., Van der Linden, M., & Bechara, A. (2009). Neural correlates of risk prediction error during reinforcement learning in humans. NeuroImage, 47(4), 1929–1939. https://doi.org/10.1016/j.neuroimage.2009.04.096
Davis, C., & Carter, J. C. (2009). Compulsive overeating as an addiction disorder. A review of theory and evidence. Appetite, 53(1), 1–8. https://doi.org/10.1016/j.appet.2009.05.018
Davis, C., Patte, K., Curtis, C., & Reid, C. (2010). Immediate pleasures and future consequences. A neuropsychological study of binge eating and obesity. Appetite, 54(1), 208–213. https://doi.org/10.1016/j.appet.2009.11.002
Davis, C., Strachan, S., & Berkson, M. (2004). Sensitivity to reward: Implications for overeating and overweight. Appetite, 42(2), 131–138. https://doi.org/10.1016/j.appet.2003.07.004
De Cock, N., Van Lippevelde, W., Vervoort, L., Vangeel, J., Maes, L., Eggermont, S., et al. (2016). Sensitivity to reward is associated with snack and sugar-sweetened beverage consumption in adolescents. European Journal of Nutrition, 55(4), 1623–1632. https://doi.org/10.1007/s00394-015-0981-3
Delgado-Rico, E., Río-Valle, J. S., González-Jiménez, E., Campoy, C., & Verdejo-García, A. (2012). BMI predicts emotion-driven impulsivity and cognitive inflexibility in adolescents with excess weight. Obesity, 20(8), 1604–1610. https://doi.org/10.1038/oby.2012.47
Ernst, M., & Fudge, J. L. (2009). A developmental neurobiological model of motivated behavior: Anatomy, connectivity and ontogeny of the triadic nodes. Neuroscience and Biobehavioral Reviews, 33(3), 367–382. https://doi.org/10.1016/j.neubiorev.2008.10.009
Fagundo, A. B., De la Torre, R., Jiménez-Murcia, S., Agüera, Z., Granero, R., Tárrega, S., ... & Fernández-Aranda, F. (2012). Executive functions profile in extreme eating/weight conditions: from anorexia nervosa to obesity. PLoS One, 7(8): e43382. https://doi.org/10.1371/journal.pone.0043382
Franken, I. H. A., & Muris, P. (2005). Individual differences in decision-making. Personality and Individual Differences, 39(5), 991–998. https://doi.org/10.1016/j.paid.2005.04.004
Galvan, A. (2010). Adolescent development of the reward system. Frontiers in Human Neuroscience, 4, 6. https://doi.org/10.3389/neuro.09.006.2010
Galvan, A., Hare, T. A., Parra, C. E., Penn, J., Voss, H., Glover, G., & Casey, B. J. (2006). Earlier development of the accumbens relative to orbitofrontal cortex might underlie risk-taking behavior in adolescents. Journal of Neuroscience, 26(25), 6885–6892. https://doi.org/10.1523/JNEUROSCI.1062-06.2006
Garner, D. M. (1998). EDI-2: Inventario de Trastornos de la Conducta Alimentaria. TEA.
Gelman, A., & Rubin, D. B. (1992). Inference from Iterative Simulation Using Multiple Sequences. Statistical Science, 7(4), 457–472. https://doi.org/10.1214/ss/1177011136
Giedd, J. N., Blumenthal, J., Jeffries, N. O., Castellanos, F. X., Liu, H., Zijdenbos, A., ... & Rapoport, J. L. (1999). Brain development during childhood and adolescence: a longitudinal MRI study. Nature Neuroscience, 2(10), 861-863. https://doi.org/10.1038/13158
Greene, K., Krcmar, M., Walters, L. H., Rubin, D. L., Jerold, & Hale, L. (2000). Targeting adolescent risk-taking behaviors: The contributions of egocentrism and sensation-seeking. Journal of Adolescence, 23(4), 439–461. https://doi.org/10.1006/jado.2000.0330
Haines, N., Vassileva, J., & Ahn, W. Y. (2018). The outcome-representation learning model: A novel reinforcement learning model of the Iowa gambling task. Cognitive Science, 42(8), 2534–2561. https://doi.org/10.1111/cogs.12688
Harden, K. P., & Tucker-Drob, E. M. (2011). Individual differences in the development of sensation seeking and impulsivity during adolescence: Further evidence for a dual systems model. Developmental Psychology, 47(3), 739. https://doi.org/10.1037/a0023279
Jastreboff, A. M., Lacadie, C., Seo, D., Kubat, J., Van Name, M. A., Giannini, C., et al. (2014). Leptin is associated with exaggerated brain reward and emotion responses to food images in adolescent obesity. Diabetes Care, 37(11), 3061–3068. https://doi.org/10.2337/dc14-0525
Konrad, K., Firk, C., & Uhlhaas, P. J. (2013). Brain development during adolescence: Neuroscientific insights into this developmental period. Deutsches Ärzteblatt International, 110(25), 425. https://doi.org/10.3238/arztebl.2013.0425
Koritzky, G., Yechiam, E., Bukay, I., & Milman, U. (2012). Obesity and risk taking. A male phenomenon. Appetite, 59(2), 289–297. https://doi.org/10.1016/j.appet.2012.05.020
Loxton, N. J., & Dawe, S. (2001). Alcohol abuse and dysfunctional eating in adolescent girls: The influence of individual differences in sensitivity to reward and punishment. International Journal of Eating Disorders, 29(4), 455–462. https://doi.org/10.1002/eat.1042
Luciana, M., & Collins, P. F. (2012). Incentive motivation, cognitive control, and the adolescent brain: Is it time for a paradigm shift? Child Development Perspectives, 6(4), 392–399. https://doi.org/10.1111/j.1750-8606.2012.00252.x
Ludwig, D. S., & Nestle, M. (2008). Can the food industry play a constructive role in the obesity epidemic? JAMA - Journal of the American Medical Association, 300(15), 1808–1811. https://doi.org/10.1001/jama.300.15.1808
Luppino, F. S., De Wit, L. M., Bouvy, P. F., Stijnen, T., Cuijpers, P., Penninx, B. W. J. H., & Zitman, F. G. (2010). Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Archives of General Psychiatry, 67(3), 220–229. https://doi.org/10.1001/archgenpsychiatry.2010.2
Mallorquí-Bagué, N., Fagundo, A. B., Jimenez-Murcia, S., De La Torre, R., Baños, R. M., Botella, C., ... & Fernández-Aranda, F. (2016). Decision making impairment: a shared vulnerability in obesity, gambling disorder and substance use disorders? PLoS One, 11(9), e0163901. https://doi.org/10.1371/journal.pone.0163901
Mamrot, P., & Hanć, T. (2019). The association of the executive functions with overweight and obesity indicators in children and adolescents: A literature review. Neuroscience & Biobehavioral Reviews, 107, 59–68. https://doi.org/10.1016/j.neubiorev.2019.08.021
Maxwell, A. L., Gardiner, E., & Loxton, N. J. (2020). Investigating the relationship between reward sensitivity, impulsivity, and food addiction: A systematic review. European Eating Disorders Review, 28(4), 368–384. https://doi.org/10.1002/erv.2732
Moreno-Padilla, M., Fernández-Serrano, M. J., & Reyes del Paso, G. A. (2018a). Risky decision-making after exposure to a food-choice task in excess weight adolescents: Relationships with reward-related impulsivity and hunger. PLoS One, 13(8), e0202994. https://doi.org/10.1371/journal.pone.0202994
Moreno-Padilla, M., Verdejo-Román, J., Fernández-Serrano, M. J., Reyes del Paso, G. A., & Verdejo-García, A. (2018b). Increased food choice-evoked brain activation in adolescents with excess weight: Relationship with subjective craving and behavior. Appetite, 131, 7–13. https://doi.org/10.1016/j.appet.2018.08.031
Moreno-Padilla, M. M., Fernández-Serrano, M. J., VerdejoGarcía, A., & Reyes Del Paso, G. A. (2019). Negative Social Evaluation Impairs Executive Functions in Adolescents with Excess Weight: Associations with Autonomic Responses. Annals of Behavioral Medicine, 53(4), 383–391. https://doi.org/10.1093/abm/kay051
Rangel, A., Camerer, C., & Montague, R. P. (2008). A framework for studying the neurobiology of value-based decision making. Nature Reviews Neuroscience, 9(7), 545e556. https://doi.org/10.1038/nrn2357
Rotge, J. Y., Poitou, C., Fossati, P., Aron-Wisnewsky, J., & Oppert, J. M. (2017). Decision-making in obesity without eating disorders: A systematic review and meta-analysis of Iowa gambling task performances. Obesity Reviews, 18(8), 936–942. https://doi.org/10.1111/obr.12549
Sahoo, K., Sahoo, B., Choudhury, A. K., Sofi, N. Y., Kumar, R., & Bhadoria, A. S. (2015). Childhood obesity: Causes and consequences. Journal of Family Medicine and Primary Care, 4(2), 187. https://doi.org/10.4103/2249-4863.154628
Shaw, P., Kabani, N. J., Lerch, J. P., Eckstrand, K., Lenroot, R., Gogtay, N., ... & Wise, S. P. (2008). Neurodevelopmental trajectories of the human cerebral cortex. Journal of Neuroscience, 28(14), 3586-3594. https://doi.org/10.1523/JNEUROSCI.5309-07.2008
Smith, D. G., & Robbins, T. W. (2013). The neurobiological underpinnings of obesity and binge eating: A rationale for adopting the food addiction model. Biological Psychiatry, 73(9), 804–810. https://doi.org/10.1016/j.biopsych.2012.08.026
Stice, E., Spoor, S., Bohon, C., Veldhuizen, M. G., & Small, D. M. (2008). Relation of reward from food intake and anticipated food intake to obesity: A functional magnetic resonance imaging study. Journal of Abnormal Psychology, 117(4), 924. https://doi.org/10.1037/a0013600
Suchindran, C., North, K. E., Popkin, B. M., & Gordon-Larsen, P. (2010). Association of adolescent obesity with risk of severe obesity in adulthood. JAMA, 304(18), 2042–2047. https://doi.org/10.1001/jama.2010.1635
Van Leijenhorst, L., Moor, B. G., Op de Macks, Z. A., Rombouts, S. A. R. B., Westenberg, P. M., & Crone, E. A. (2010). Adolescent risky decision-making: Neurocognitive development of reward and control regions. NeuroImage, 51(1), 345–355. https://doi.org/10.1016/j.neuroimage.2010.02.038
Vehtari, A., Gelman, A., & Gabry, J. (2017). Practical Bayesian model evaluation using leave-one-out cross-validation and WAIC. Statistics and Computing, 27(5), 1413–1432. https://doi.org/10.1007/s11222-016-9696-4
Verbeken, S., Braet, C., Bosmans, G., & Goossens, L. (2014). Comparing decision making in average and overweight children and adolescents. International Journal of Obesity, 38(4), 547–551. https://doi.org/10.1038/ijo.2013.235
Verdejo-Garcia, A., Moreno-Padilla, M., Garcia-Rios, M. C., Lopez-Torrecillas, F., Delgado-Rico, E., Schmidt-Rio-Valle, J., & Fernandez-Serrano, M. J. (2015). Social stress increases cortisol and hampers attention in adolescents with excess weight. PLoS One, 10(4), e0123565. https://doi.org/10.1371/journal.pone.0123565
Verdejo-García, A., Pérez-Expósito, M., Schmidt-Río-Valle, J., Fernández-Serrano, M. J., Cruz, F., Pérez-García, M., et al. (2010). Selective alterations within executive functions in adolescents with excess weight. Obesity, 18(8), 1572–1578. https://doi.org/10.1038/oby.2009.475
Volkow, N. D., Wang, G. J., Tomasi, D., & Baler, R. D. (2013). Obesity and addiction: Neurobiological overlaps. Obesity Reviews, 14(1), 2–18. https://doi.org/10.1111/j.1467-789X.2012.01031.x
World Health Organization. (2020). Obesity and overweight.
Worthy, D. A., Pang, B., & Byrne, K. A. (2013). Decomposing the roles of perseveration and expected value representation in models of the Iowa gambling task. Frontiers in Psychology, 4, 640. https://doi.org/10.3389/fpsyg.2013.00640
Yang, Y., Shields, G. S., Guo, C., & Liu, Y. (2018). Executive function performance in obesity and overweight individuals: A meta-analysis and review. Neuroscience and Biobehavioral Reviews, 84, 225–244. https://doi.org/10.1016/j.neubiorev.2017.11.020
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception of the article. MMP contributed to data collection. AAC contributed to the statistical analysis. All authors contributed to the interpretation of the results. MMP and AAC drafted the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethical standards
The Ethics Committee for Human Research of the Universidad de Jaén approved the study. Participants sent us their informed consent for the study and publication signed by their parents.
Conflict of interest
The authors declare that they have no conflict of interest.
Implications and contributions summary
Excess weight in adolescence is a risk factor for the development of future health problems and obesity. Our study shows maladaptive decision making based on feedback in excess weight adolescents. Thus, designing interventions aimed at reducing reward sensitivity and increasing inhibitory control in this population is advisable.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Moreno-Padilla, M., Alacreu-Crespo, A., Guillaume, S. et al. The outcome-representation learning model: impairments in decision-making in adolescents with excess weight. Curr Psychol 42, 22404–22414 (2023). https://doi.org/10.1007/s12144-022-03299-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-03299-1