
Abstract
Introduction
Positive psychological variables, such as meaning in life and the capacity for enjoyment, are important resilience factors against negative behaviors and symptoms. These constructs are related to better emotional regulation strategies, a greater perception of control over one’s life, and better mental health in general. Adjustment disorder (AjD) is a prevalent condition defined as the failure to adapt to a stressful event.
Objective
This study presents secondary analysis data on the effect of an Internet-delivered cognitive-behavioral therapy intervention (iCBT) for AjD on meaning in life and capacity for enjoyment, compared to a control group.
Method
The sample consisted of 68 participants with AjD. 34 in the iCBT condition and 34 in the control group). Meaning in life was assessed by the Purpose-in-Life Test-10, and the Environmental Rewards Observation Scale was used to assess the capacity for enjoyment. The iCBT intervention focused on acceptance and processing of the stressful event. Intent-to-treat mixed-model analyses without any ad hoc imputations and using Cohen’s d effect comparisons were conducted.
Results
The results revealed a significant main effect of time and a significant group x time interaction in all the measures. Significantly higher pre-post score differences were found in the treatment condition.
Discussion
Meaning in life and capacity for enjoyment can change after an iCBT intervention for AjD. Therapeutic implications of the results and future lines of research about the role of meaning in life in AjD are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Positive psychological variables, such as meaning in life and the capacity for enjoyment, are important resilience factors against negative behaviors and symptoms (e.g., Hopko et al., 2003). These constructs are related to better emotional regulation strategies, a greater perception of control over one’s life, and better mental health in general. Adjustment disorder (AjD) is a prevalent condition that is defined as failure to adjust to a stressful event or major change in life circumstances (e.g., migration) and is characterized by low mood, insomnia, frequent crying, poor concentration, poor appetite, and concerns about major changes (Puri et al., 2013). Studies focusing on assessing the influence of meaning in life and enjoyment on AjD treatment. Although currently there is no evidence-based treatment of choice for AjD (O’Donnell et al., 2018), cognitive-behavioural therapy (CBT) is the most frequent form of treatment, and also the most recommended by authors (e.g., Benton & Lynch, 2005). Recently, some studies have shown positive outcomes in the treatment of this problem with brief Internet-delivered CBT interventions (e.g., Rachyla et al., 2020). This paper examines the effect of a brief iCBT on meaning in life and enjoyment.
Meaning in Life
Frankl introduced the concept “meaning in life” in psychology and psychiatry in his existential theory. According to Frankl (1973), meaning in life is the primary motive for human behavior and the condition of personal self-fulfillment, and he emphasized the role of creative, experimental, and attitudinal values in the development of the sense of existential fulfillment.
To understand this definition of meaning in life, it is important to know that, although life has meaning in all situations and circumstances, it has to be experienced as meaningful (King et al., 2016). Therefore, when the search for meaning in a person's life is constantly hampered, it can be psychologically damaging. When this happens, and a sense of meaning is not found, a negative cognitive-motivational state emerges. This state, which is accompanied by a set of symptoms such as boredom, depression, aggressive behavior, perception of lack of control over one's life, and absence of life goals, is called an “existential vacuum”.
Frankl (1959) suggested that life never ceases to be potentially meaningful, and that human beings have the need to live oriented towards someone or something (a purpose), which allows them to build a meaningful life in any circumstance. Frankl suggested that there were three main sources of meaning: doing something (career, work, etc.), loving someone (authentic interpersonal relationships) and through the attitude with which we face suffering. These sources of meaning proposed by Frankl, has been confirmed in a study carried out with patients with suicidal ideation indicate that they indicated that the main sources of meaning are: Interpersonal / affective relationships (mainly family), profession / education, intellectual / non-intellectual pleasures, and transcendental dimension (religiosity / spirituality) (Costanza et al., 2020).
In this sense, previous research shows that low meaning in life levels is related to substance abuse, lack of hope in life, and suicidal ideation (Costanza et al., 2019; Marco et al., 2017; Vos & Vitali, 2018), and it may have an influence on personal relationships, leading to social rejection or disturbances (Ho et al., 2010).
By contrast, higher scores on meaning in life are related to the experience of freedom, a positive view of life and the future, purpose and success of life goals, coping, satisfaction in life, and self-realization (García-Alandete et al., 2009). Moreover, people with the experience of meaning in life have a greater sense of autonomy, self-determination, and purpose in life, with clear and definite personal life goals (Frankl, 1956).
Therefore, meaning in life has been positively associated with some psychological well-being variables and negatively associated with psychopathology, and so it seems to serve as a mediator factor in psychological health (Gongora, 2014; Halama & Dedova, 2007). Specifically, studies show that people with higher meaning in life have a lower incidence of psychological disorders such as depression (Kleftaras & Psarra, 2012). Moreover, meaning in life is an important factor in maintaining not only emotional well-being, but also physical and functional health (e.g., Czekierda et al., 2017; Glaw et al., 2017).
The role of meaning in life has been associated with higher positive emotions (Feder et al., 2013) and with acceptance and less fear of death (Routledge & Juhl, 2010). In addition, meaning in life has been shown to be a resilience factor against the development of burnout (Chan, 2009) and negative behaviors or symptoms such as hopelessness (García-Alandete et al., 2019).
Moreover, it seems that people who can find meaning in life in hostile experiences, such as a disease like cancer or HIV (Guerrero-Torrelles et al., 2017), the loss of a child (Williams et al., 1998), or traumatic situations in military veterans (Park, 2010), are able to cope better with the situation than those who cannot find meaning.
In sum, studies show that higher meaning in life has been associated with positive psychological variables such as emotional regulation strategies, a greater perception of control over one's life, and a greater capacity to face adversity or problems (Shin et al., 2005).
Adjustment Disorder
Adjustment disorder (AjD) is characterized by the failure to adapt to a stressful event, and the inability to face problems is a key symptom of the disorder (Maercker et al., 2013). For this reason, understanding the relationship between psychological variables such as meaning in life and AjD could be of clinical interest. In fact, AjD is one of the most common psychological disorders in clinical practice (Evans et al., 2013). It is characterized by marked distress, and it causes a significant impairment in different functional areas of patients’ lives, such as family, relationships, work, and studies. In addition, AjD may increase the risk of suicidal thinking and behavior (Casey et al., 2015).
Regarding the specific relationship between meaning in life and the severity and response to treatment in patients with AjD, some preliminary results found that a lower meaning in life score was related to higher depressive symptoms and low positive affect in patients with AjD (Mor et al., 2018). Moreover, low meaning in life has been shown to predict a variety of psychosocial adjustment problems (Park, 2010). Grimaldos et al. (2019) carried out the first study that analyzed the predictive capacity of meaning in life as a treatment outcome for AjD after receiving a ICBT program that aimed to change the meaning of stressful life events. They found that meaning in life predicted the change in depressive symptoms. Moreover, Quero et al. (2018) found that the meaning in life level could predict some studied psychological variables, such as coping strategies, post-traumatic growth, and capacity for enjoyment, in patients with AjD before treatment. More recently, Marco et al. (2020a) found that meaning-making during face-to-face CBT was a mediator between anxiety symptoms and depressive symptoms before and after treatment. Thus, these studies suggest that meaning in life could be an important variable in the treatment of AjD.
Enjoyment
In this line, other positive variables, such as self-esteem, optimism, and life satisfaction, have been found to have an influence on the prevalence and greater severity of symptoms in patients with AjD (Vallejo-Sánchez & Pérez-García, 2015). Specifically, capacity for enjoyment is one of the most commonly studied positive variables. For several decades, studies have found support for the importance of the individual-environment fit in the development of positive life rewards (Battista & Almond, 1973). This fit seems to be related to statements that have to do with deriving pleasure, enjoyment, or satisfaction from life activities and experiences. The relationship between positive reinforcement and emotional distress has been established (Cuijpers et al., 2007). In general, low levels of enjoyment is accompanied by unusual goal-directed behavior (Manos et al., 2010). Barraca and Pérez-Álvarez’s (2010) results showed that the average enjoyment score was lower in caregivers compared to the non-clinical Spanish population. In addition, facilitating greater access to rewards decreases the intensity and frequency of punishment events, as occurs in cancer survivors (Lewinsohn et al., 1980), and contact with enjoyment increases positive affect (Hopko et al., 2003). Therefore, given the positive relationship between the presence fo enjoyment in one’s life and positive affect, which is related to the severity of AjD symptoms, enjoyment could be another important variable to consider in its treatment. However, to our knowledge, there are no available studies that focus on assessing the influence of enjoyment on AjD treatment.
Cognitive Behavioral Therapy
Currently there is no evidence-based treatment of choice for AjD (Casey, 2014). In addition, many of the intervention studies published have methodological limitations (O'Donnell et al., 2018). In the meta-analysis of O'Donnell et al., which included 29 articles addressing the treatment of AjD, the quality of the studies was classified as low to very low. According to this author, there is a wide diversity of psychological treatments for AjD (psychodynamic, relaxation techniques, behavioural therapy…) but the most frequent form of treatment is the cognitive-behavioural one.
The need to develop brief treatments that reach as many people as possible has led to the incorporation of Information and Communication Technologies, such as the Internet, in the treatment of AjD. To the author’s knowledge several randomized control trials have been conducted for assessing the efficacy of self-applied Internet-delivered interventions for AjD (Bachem & Maercker, 2016; Eimontas et al., 2018; Lindsäter et al., 2018; Moser et al., 2019; Rachyla et al., 2020), as well as for the treatment of psychiatric symptoms such as insomnia (Soh et al., 2020). The treatments tested are brief, ranging from 4 to 6 modules, except for the study of Lindsäter et al. (2018) which includes 12 modules. All of these articles found clinical improvement in patients who received the treatment. The internet CBT (iCBT) intervention developed by Rachyla et al. (2020) was effective in reducing negative affect and symptoms in patients with AjD. In addition, the implementation of open source learning platforms such as Moodle for an Internet-based program has shown that it could be used as a cost-effective method to implement and deliver these types of therapies which could further reduce associated costs (Takano et al., 2016; Zhang & Ho, 2017).
In this line of research, and given the growing interest in learning about the role of some related positive psychological variables in AjD, the main objective of this study was to test the effect of the iCBT intervention aforementioned that has been shown to be effective for treating AjD (Rachyla et al., 2020) on meaning in life. The secondary objective was to analyze the effect of this intervention on the level of enjoyment in one’s life.
Method
Study Design
This study consisted of a secondary analysis of data collected as part of a two-armed, single-blind, parallel group randomized controlled trial (RCT) with two independent groups: an intervention group receiving an Internet-delivered cognitive therapy (iCBT) intervention and a control group (participants completed the intervention program after the seven-week waiting-list time for ethical reasons). The trial was registered at the ClinicalTrial.gov database (NCT02758418, 2 May 2016). More details about this intervention can be found in the published study protocol (Rachyla et al., 2018) and will be described later. The main efficacy data are available in the original study published elsewhere (Rachyla et al., 2020).
The study was conducted following the Consolidated Standards of Reporting Trials (CONSORT) (Moher et al., 2010) and the SPIRIT guidelines (Chan et al., 2013). The protocol for the current RCT was approved by the Ethical Committee of Universitat Jaume I. The online informed consent form was signed before the randomization of the participants.
In this study, we present the outcome measures assessed at pre- and post-intervention and the 3-, 6-, and 12-month follow-ups, in order to provide data on intervention effectiveness and maintenance of the improvements over time.
Participants, Recruitment, Randomization, Flow and Attrition
The research took place at the Emotional Disorders Clinic at Universitat Jaume I in Castellón (Spain). Participants recruitment was carried out through advertisements on local media (radio, TV and newspaper) and the website of Universitat Jaume I, and disseminated through social networks (Facebook, Instagram and Twitter).
People interested in the study sent an e-mail to tao@uji.es or called the clinic. Then, the clinical team had a telephone interview with them. The purpose of the interview was to explain the research terms and check the fulfillment of the eligibility criteria. These telephone interviews were recorded with the patient´s consent. All participants underwent a semi-structured Diagnostic Interview for AjD, based on DSM-5. The clinical team were 2 PhD students with a master's degree in clinical psychology and were trained in cognitive behavioral therapy.
To participate in the study, inclusion criteria were: being 18 years old or more; meeting DSM-5 criteria for AjD (APA, 2013); being able to use a computer and having access to the Internet; being able to understand and read Spanish; and having an e-mail address. Exclusion criteria were: receiving another psychological treatment for AjD; current alcohol or drug dependence or abuse; meeting criteria for psychosis or a severe personality disorder; a severe organic illness that makes it impossible to apply the treatment program; and risk of suicide or self-destructive behaviors. Receiving pharmacological treatment was not an exclusion criterion, but any increase in the medication during the study period led to the participant’s exclusion.
Once the online informed consent had been signed, participants were randomly assigned to one of the groups (intervention group or control group). Participants signed their participation agreements without knowing their group assignment. In addition, study researchers were blind to the group to which the assessed participants belonged. An independent researcher performed the randomization. This assignment was carried out by the Epidat 4.1 program, which generates a sequence of random numbers. Participant recruitment was carried out between May 2015 and March 2018.
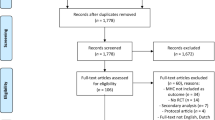
After reviewing the literature and adopting a more conservative approach, an effect size of 0.70 was assumed in the original work. Considering a significance level of 5% and a power of 80%, 26 participants in each group would be sufficient to detect the assumed difference. Because the literature reveals dropout rates from iCBTs of around 30%, a sample of 68 participants was recruited: 52 were women (76.5%) and 16 men (23.5%). They were randomized in two groups: 34 participants with AjD were in the intervention group, and 34 were in the control group.
Of the 68 participants, all were between the ages of 18 and 58, with a mean age of 33.21 (SD = 10.60), and 76.5% were women. Regarding marital status, 51.5% of the participants were single, 33.8% were married or had a partner, 13.2% were separated or divorced, and 1.5% were widowers. In the case of the educational level, most of the participants had higher education (73.5%), some had secondary education (19.1%), and the rest had primary education (7.4%). Break-up, separation, or divorce was the most frequently reported stressor (29.4%), followed by conflicts with family members (19.1%), problems in work or academic areas (19.1%), their own disease (11.8%), illness of a relative (4.4%), economic problems (10.3%,), change of city or country of residence (2.9%), and life change (2.9%). In most cases, the distress symptoms had been present for at least six months (48.5%), but only eight participants were receiving medication at the time of assessment (14.7%).
Of the 34 participants in the first group, 30 completed the PIL-10 assessment before the intervention, 22 completed it at the post-intervention evaluation, and 17, 12, and 8 participants completed it at the 3-, 6-, and 12-month follow-ups, respectively. In the control group, 26 of the 28 participants completed the post-waiting list assessment. Regarding the EROS assessment, 34 completed the questionnaire before the intervention, 25 answered the post-treatment evaluation, and 20, 16, and 9 participants completed the questionnaire at the 3-, 6-, and 12-month follow-ups, respectively. In the control group, 26 of the 29 participants completed the post-waiting list assessment.
Because the post-intervention assessment was performed only when the last iCBT module had been completed, participants who did not finish the whole program were considered dropouts.
Measures
Purpose-in-Life Test-10 Items (PIL-10; García-Alandete, Martinez & Nohales, 2013). This scale is a reduced version of the PIL (Crumbaugh & Maholick, 1969) and of the Spanish adaptation (Noblejas de la Flor, 1994). The PIL is a commonly used instrument to measure meaning and purpose in life. It is comprised of 10 items that are answered on a Likert scale with 7 response categories (1 and 7 have specific labels, and category 4 indicates neutrality). The PIL-10 includes two subscales: 1) Satisfaction and meaning in life (composed of items 1, 2, 5, 6, 9, and 11 of the original PIL) (e.g., “When thinking about my own life: I often wonder why I exist / I always find reasons to live” or “Life to me seems: Completely routine/Always exciting”) and, 2) Life goals and purposes (composed of items 3, 7, 17, and 20) (e.g., “In my Life I have: No goals or aims at all/ Very clear goals and aims” or “I regard my ability to find a meaning, a purpose, or mission in life as: Practically none/Very great”. The total score ranges between 10 and 70, and higher scores indicate greater meaning in life. The PIL-10 offers good psychometric properties (e.g., García-Alandete et al., 2013). A good internal consistency (Cronbach’s alfa = 0.88) was obtained for the current sample, being the Cronbach’s alpha for the Satisfaction and meaning in life subscale = 0.89 and for the Life goals and purposes = . 67.
The Environmental Rewards Observation Scale (EROS; Armento & Hopko, 2007). This is a 10-item scale that assesses enjoyment and response-contingent positive reinforcement, measured on a Likert scale with 4 response categories (1, “strongly disagree” to 4, “strongly agree”). Items include increased goal-directed behavior and positive affect from obtaining reinforcements from the environment; half of the items are reverse scored (e.g., “A lot of activities in my life are pleasurable” or “Lately I have found that many experiences make me unhappy”). Scores range from 10 to 40, with higher scores indicating increased enjoyment. The Spanish adaptation of the instrument (Barraca & Pérez-Álvarez, 2010) presents good internal consistency (Cronbach’s alfa = 0.86). For the current sample a Cronbach’s alfa of 0.77 was obtained.
Demographics: We reported the sociodemographic measures (see Table 1) commonly included in clinical trials (gender, age, marital status, level of education, employment status, and ICT proficiency level) and other clinical measures (medication, number of stressors, duration of symptoms, global interference level, and main stressor).
Intervention
Detailed summaries of the treatment content are provided in the study protocol (Rachyla et al., 2018). Briefly, Adjustment Disorders Online is a self-applied iCBT based on a manualized protocol for AjD, supported by a 10-min weekly phone call. It focuses on acceptance and processing of the stressful event, with the aim of improving the capacity to face problems and learn from them after the events, which is achieved through acceptance, confrontation, and developing a new meaning for the stressful event.
The aim of the phone calls was to clarify doubts about the use of the platform, remind patients of the importance of continuing to work on the contents, and congratulate them for their effort and achievements. Patients received one telephone call per week over a 7–10-week period, and each call had a maximum duration of 10 min. In the call, no additional clinical content or counselling was provided.
The internet-based system has a database with media contents (videos, images, audio, and text). It includes several therapeutic components such as psychoeducation, negative emotion management techniques (slow breathing and behavioral activation), exposure, problem-solving techniques, mindfulness, acceptance and elaboration techniques of the negative event, and positive psychology strategies that try to increase the natural human capacity to resist and grow in the face of adversity and prevent relapse. The positive psychology strategies are exercises used to extract positive aspects from experiences (Neimeyer, 2000) to cope with problems, following also the guidelines by Karl Popper (1995) about the role of solving problems to the progress of the human being. It is the optimized version of the original intervention protocol for AjD developed by Botella et al. (2008).
The program is structured in 7 modules and lasts approximately 7 to 10 weeks. Completing one module per week is recommended, although it might be useful to spend more time with some, depending on how much each person needs to advance. The modules are:
-
0- Starting the program: The objectives are to provide the participants information about the treatment program and the contents included in it and to promote their adherence and the importance of evaluation, the use of records and tasks for treatment and to promote motivation for change.
-
1- Understanding emotional reactions: The objectives of this module are to provide the participant with information about AjD and common reactions to stressful events and teach participants two strategies to manage negative emotions (behavioral activation and slow breathing technique).
-
2- Learning to deal with negative emotions: With this module it is intended that the participant face avoided situations that contribute to the maintenance of the problem, improving the ability to face daily challenges through the exposure technique and learn to solve problems using problem solving technique.
-
3- Accepting the problems: In this module it is intended that the participant becomes aware of personal experiences related to stressful situations, learning the logic of elaboration and mindfulness to elaborate and process stressful situations in order to accept them and reflect on the new meaning the problems may have.
-
4- Learning from problems: The objectives of this module are for participants to be able to reflect on the learning that we can extract from problems, to agree on the elaboration to face their experiences and to be able to learn from them, and to learn to identify their own psychological strengths.
-
5- Changing the meaning of the problems: The objectives are for the participants to be able to elaborate and process the stressful event by developing a new meaning for the problem situation and to develop a new attitude towards the problems by making a forward-looking letter and choosing a personal life motto.
-
6- Relapse prevention: Participants evaluate the achievements made with the treatment and review the techniques and skills learned. In addition, they learn to identify problem situations and develop a plan to deal with them. The need to continue working on their own improvement is also addressed.
Participants in the control group were assessed by the intervention program before and after a waiting period of 7 weeks. They were told to wait for this period and then, after completing the second assessment, they received the treatment. During the waiting period this group did not receive any treatment or instructions on their adjustment process.
Statistical Analyses
Baseline differences between the study groups were examined using independent sample t-tests and chi-square tests (χ2) for continuous and categorical variables, respectively.
Intent-to-treat (ITT) mixed-model analyses without any ad hoc imputations were conducted to handle missing data due to participant dropout. This analysis compares the study groups based on the treatment to which they were randomly allocated. It does not assume that the last measurement is stable, it does not involve any substitution of missing values with supposed or estimated values, it is conducted using all available observations, thus reducing the biases and loss of power caused by the simple deletion or random imputation of incomplete data. Mixed-model analyses are appropriate for RCTs with multiple time points and pre-post designs, and it is robust to violations of distributional assumptions (Salim et al., 2008; Schielzeth et al., 2020).
For all the outcomes, time (pre, and post) was treated as within-group factor and group (intervention and control group) as a between-group factor. A separate mixed-model analysis was conducted to explore changes in the intervention group from baseline to follow-up (3-, 6-, and 12-month). Significant effects were followed up with pairwise comparisons (adjusted by Bonferroni correction). These statistical tests have shown their robustness regardless of violations of the required assumptions when group sizes are equal (Schmider et al., 2010). Effect sizes (Cohen’s d) were calculated for within-group and between-group comparisons (Cohen, 1988; Cumming & Calin-Jageman, 2016). Moreover, sensitivity (parametric and non-parametric) analyses were performed to explore the adequacy and robustness of the findings in terms of the methods different methods for handling missing data (Thabane et al., 2013).
All statistical analyses were conducted using IBM SPSS Statistics, version 25.0 for Windows (IBM Company, Madrid, Spain).
Results
Baseline Characteristics
The majority of the participants who performed the pre-intervention evaluation were Spanish (n = 56), but there were also participants from Romania (n = 1), Brazil (n = 2), Colombia (n = 2), El Salvador (n = 1), Ecuador (n = 1), Argentina (n = 1), Chile (n = 1), and Portugal (n = 1). All participants understood the study instructions, regardless of their nationality or country of residence. All of them were asked about their level of proficiency in ICTs; 51.5% had an advanced level, 35.3% a medium level, 7.4% a basic level, and 5.9% an expert level.
No baseline differences in demographic or clinical characteristics were found between groups. All these data are presented in Table 1. Furthermore, no differences in pre-test scores were found between participants who dropped out and those who remained in the study: Satisfaction and meaning in life (t (56) = -0.30. P = 0.775); Life goals and purposes (t (56) = 1.23, p = 0.184); Total PIL-10 (t (56) = 0.34, p = 0.736); and EROS (t (61) = 0.819, p = 0.416).
Treatment Effect at Post-Treatment
Table 2 presents the effects of the intervention outcomes at post-treatment. A significant interaction effect of time of assessment (pretreatment and post-treatment) and experimental condition (intervention group and control group) was found, indicating a different pattern of change between groups over time on the total PIL-10 score [F (1, 47.94) = 19.83; p < 0.00], the Satisfaction and meaning in life subscale [F (1, 47.88) = 17.89; p < 0.00], the Life Goals and Purposes subscale [F (1, 47.47) = 12.01; p < 0.01], and the EROS total score [F (1, 51.18) = 11.47; p < 0.01].
Within-group comparisons showed significant improvements over time in the TAO condition on all the measures (ps < 0.001), indicating significant mean differences from pre to post, with large effect sizes (Cohen’s d values) ranging from 0.70 to 1.03. No significant pre-to-post changes were found in the control group.
Furthermore, at post-treatment, the intervention group revealed greater improvements on all measures, compared to the control group, showing significant between-group differences (all ps < 0.05) corresponding to significant moderate effect sizes (ranging from 0.68 to 0.76), except for the Life Goals and Purposes subscale (d = 0.54).
Stability of Treatment Effects During the Follow-up
Regarding the effects of the intervention at the follow-up assessments, the main effect of time was found to be non-significant at the 3-, 6-, and 12-month follow-ups, compared to post-intervention, on the total PIL-10 score [F (3, 39.55) = 0.49; p > 0.05], the Satisfaction and meaning in life subscale [F (3, 42.41) = 0.42; p > 0.05], the Life Goals and Purposes subscale [F (3, 34.95) = 0.62; p > 0.05], and the EROS total score [F (3, 50.55) = 0.25; p > 0.05], suggesting the stability of the treatment gains at post-treatment.
In Table 3, results of a separate linear mixed-model analysis comparing pre-intervention and follow-ups in the treatment group are presented for each outcome. A significant main effect of time was found for all measures (p < 0.05), indicating the maintenance of the treatment gains. In addition, within-group comparisons showed significant improvements over time in the treatment condition on all measures (p < 0.01), with moderate and large effect sizes (ranging from 0.59 to 1.25) at 3- and 6-month follow-ups, but these gains were not significant at the 12-month follow-up.
Discussion and Conclusions
The aim of this study was to carry out an RCT to test the effect of an iCBT for AjD on meaning in life, assessed by the PIL-10, and on the capacity for enjoyment, assessed by the EROS questionnaire, compared to a control group. Results obtained in the present study showed that the internet-based system was effective in increasing meaning in life in the intervention group, which was observed on the PIL-10 total score and on the two subscales: Satisfaction and meaning in life and Life Goals and Purposes. The intervention also significantly enhanced the capacity for enjoyment measured by the EROS. However, no significant changes were obtained in the control group. Within-group effect sizes were large on all measures, except on the Life Goals and Purposes subscale, which had a moderate effect size. Furthermore, differences were found between the two groups. The intervention group presented significantly larger improvements on all the measures, with moderate effect sizes, except Life Goals and Purposes.
In addition, results showed that the effects on PIL-10 and EROS were maintained over time in the medium and longer term (3- and 6- and 12-month follow-ups). However, the effect size for the 12-month follow up was not significant, which might be due to loss of data in the 12-month follow-up.
These results are consistent with those found in the original study (Rachyla et al., 2020), which showed that the internet-based system intervention was effective not only in decreasing negative affect and depressive, anxiety, and AjD symptoms, but also in promoting positive variables such as posttraumatic growth, positive affect, and quality of life. This is not surprising because the intervention includes positive psychology strategies that try to increase the natural human capacity to resist and grow in the presence of adversity. Specifically related to meaning in life, the main component of the program (techniques for acceptance and elaboration of the negative event) is designed to revise and rebuild the meaning of the stressful event in the patient’s life, which implies an elaboration of meaning-making Furthermore, the program also includes the behavioral activation technique, which might have helped to increase satisfaction with life experiences.
Our findings are also in line with previous studies showing the predictive role of meaning in life in the therapeutic change in depressive symptoms (Grimaldos et al., 2019) and the mediating role of meaning-making in anxiety symptoms and depressive symptoms before and after face-to-face CBT treatment (Marco et al., 2020a), suggesting that treating meaning in life could be an important variable in the treatment of AjD.
As far as we know, this is the first study to examine the effect of an iCBT on meaning in life. The results show that a self-applied iCBT treatment is effective in increasing meaning in life in AjD, which is a condition that, despite its relevance, has received little attention from researchers. In addition, we should consider the important advantages that internet-delivered interventions offer in terms of reach, flexibility, cost saving, and confidentiality (Griffiths et al., 2006; Musiat & Tarrier, 2014), compared to traditional face-to-face CBT.
All these results may have therapeutic implications. The finding that future-oriented meaning in life plays a key role in reducing AjD symptoms should lead to interventions focused on building future goals and the search for meaning in life in these patients specifically, in order to increase their effectiveness. These results also highlight the importance of including this construct in prevention programs in order to strengthen positive psychological variables such as affect and promote resilience and reduce the development of clinical symptoms in high-risk people, for example, people who have experienced a stressful event. Because this factor has been related to resilience and a greater ability to face adversities (Marco et al., 2020b), the improvement in meaning in life could prevent future relapses in these patients and help them to face future stressful events in a more adaptive way. Finally, the findings also show the advantages of including strategies that enhance this protective variable in prevention programs for the general population.
The present study has some limitations that should be considered in future studies. The foremost limitation is that we cannot know from this study whether the heightened levels in meaning and enjoyment resulted from reading about the topics in the seven modules, from doing the exercises included, from reflection on the stressful event, or something else due to the fact that the control group was not instructed to do anything but wait. All that can be learned from this study is that the whole package of this intervention was helpful for meaning and enjoyment, compared to participants who were not instructed to do anything. Future studies with active control groups are needed to withdraw firmer conclusions in this regard. Second, our sample was composed mainly of volunteers who showed an interest in an online intervention, and it is unclear whether the adherence and treatment outcomes could have been affected. Third, most of the participants had university studies, thus compromising the generalizability of the results to other populations. A fourth limitation, pointed out above, is the loss of data from the post-treatment to follow-up assessments that may affect the statistical power. Nevertheless, sensitivity analyses and one of the most robust methods to handle missing data (i.e., ITT mixed model analyses without any ad hoc imputation), reducing this possible bias and loss of power, has been conducted in this study.
Another important line of research would be the study of meaning-making mechanisms and their mediator role in psychological wellbeing, specifically in depressive and anxious symptomatology (Marco & Alonso, 2019). As described in the introduction, in some studies, meaning in life seems to have a direct influence on health and psychological adjustment (e.g., Smith & Zautra, 2004), whereas in others it acts as a mediator (e.g., Heisel & Flett, 2004).
Our results show that a cognitive behavioral intervention focused on teaching people how to search for meaning in life better after experiencing a stressful event is capable of increasing meaning in life and variables such as the capacity for enjoyment in the participants. Future studies should find out whether there is a relationship between the increase in meaning in life after the application of the treatment and the increase in the capacity for enjoyment, or whether they are independent variables, in addition to studying the relationship between meaning in life and other psychological variables after the application of an iCBT.
Finally, our study found that the dimension of satisfaction and meaning in life improved more than the dimension of life goals and purposes. Therefore, future research should analyze which dimension of meaning is responsible for meaning-making: coherence (comprehensibility and making sense of one's life), purpose (one's core aims and aspirations for life and direction in life), or satisfaction (having a life worth living and a sense of life's inherent value) (Martela & Steger, 2016).
In conclusion, it seems important to foster meaning in life and carry out more research in this field, focusing on its relationship with other positive variables that have been relevant in the scientific literature. Hence, it would be possible to replicate the results obtained in the present study, test the effectiveness of CBT in increasing meaning in life, and evaluate whether including a specific meaning in life component in these treatments would enhance meaning in life and treatment effectiveness.
Data availability
The dataset used in the current study is available from the corresponding author on reasonable request.
Code availability
Not applicable.
References
American Psychiatric Association (APA). (2013). Diagnostic and statistical manual of mental disorders DSM-V (5th ed.). APA.
Armento, M. E., & Hopko, D. R. (2007). The environmental reward observation scale (EROS): Development, validity, and reliability. Behavior Therapy, 38(2), 107–119.
Bachem, R., & Maercker, A. (2016). Self-help interventions for adjustment disorder problems: A randomized waiting-list controlled study in a sample of burglary victims. Cognitive Behaviour Therapy, 45(5), 397–413.
Barraca, J., & Pérez-Álvarez (2010). Adaptación española del Environmental Reward Observation Scale (EROS).
Battista, J., & Almond, R. (1973). The development of meaning in life. Psychiatry, 36(4), 409–427.
Benton, T. D., & Lynch, J. (2005). Adjustment disorders [web page]. Retrieved from www.emedicine.com/Med/topic3348.htm
Botella, C., Baños, R. M., & Guillén, V. (2008). Creciendo en la adversidad. Una propuesta de tratamiento para los trastornos adaptativos. Psicología Positiva Aplicada. DDB.
Casey, P. (2014). Adjustment disorder: New developments. Current Psychiatry Reports, 16(6), 451.
Casey, P., Jabbar, F., O’Leary, E., & Doherty, A. M. (2015). Suicidal behaviours in adjustment disorder and depressive episode. Journal of Affective Disorders, 174, 441–446. https://doi.org/10.1016/j.jad.2014.12.003
Chan, D. W. (2009). Orientations to happiness and subjective well- being among Chinese prospective and in-service teachers in Hong Kong. Educational Psychology, 29, 139–151.
Chan, A. W., Tetzlaff, J. M., Altman, D. G., Laupacis, A., Gøtzsche, P. C., Krleža-Jerić, K., ... & Doré, C. J. (2013). SPIRIT 2013 statement: defining standard protocol items for clinical trials. Annals of Internal Medicine, 158(3), 200–207.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Lawrence Erlbaum Associates.
Costanza, A., Prelati, M., & Pompili, M. (2019). The meaning in life in suicidal patients: The presence and the search for constructs. A systematic review. Medicina, 55, 1–18. https://doi.org/10.3390/medicina55080465
Costanza, A., Amerio, A., Odone, A., Baertschi, M., Richard-Lepouriel, H., Weber, K., … & Canuto, A. (2020). Suicide prevention from a public health perspective. What makes life meaningful? The opinion of some suicidal patients. Acta Biomed, 91(3-S), 128–134.
Crumbaugh, J., & Maholick, L. (1969). Manual de instrucciones para el Test de Sentido de Vida (PIL). Viktor Frankl Institute for Logotherapy.
Cuijpers, P., Van Straten, A., & Warmerdam, L. (2007). Behavioral activation treatments of depression: A meta-analysis. Clinical Psychology Review, 27(3), 318–326.
Cumming, G., & Calin-Jageman, R. (2016). Introduction to the new statistics: Estimation, open science, and beyond. Routledge.
Czekierda, K., Banik, A., Park, C. L., & Luszczynska, A. (2017). Meaning in life and physical health: Systematic review and meta-analysis. Health Psychology Review, 11(4), 387–418. https://doi.org/10.1080/17437199.2017.1327325
Eimontas, J., Rimsaite, Z., Gegieckaite, G., Zelviene, P., & Kazlauskas, E. (2018). Internet-based self-help intervention for ICD-11 adjustment disorder: Preliminary findings. Psychiatric Quarterly, 89(2), 451–460.
Evans, S. C., Reed, G. M., Roberts, M. C., Esparza, P., Watts, A. D., Correia, J. M., … & Saxena, S. (2013). Psychologists' perspectives on the diagnostic classification of mental disorders: results from the WHO‐IUPsyS Global Survey. International Journal of Psychology, 48(3), 177–193. https://doi.org/10.1080/00207594.2013.804189
Feder, A., Ahmad, S., Lee, E. J., Morgan, J. E., Singh, R., Smith, B. W., … & Charney, D. S. (2013). Coping and PTSD symptoms in Pakistani earthquake survivors: Purpose in life, religious coping and social support. Journal of affective disorders, 147(1-3), 156–163. https://doi.org/10.1016/j.jad.2012.10.027
Frankl, V. E. (1959). Man’s search for meaning: From death camp to existentialism (1ª). Beacon.
Frankl, V. E. (1956). Theorie und Therapie der Neurosen: Einführung in Logotherapie und Existenzanalyse.
Frankl, V. E. (1973). Psychotherapy and existentialism selected papers on Logotherapy.
García-Alandete, J., Gallego-Pérez, J. F., & Perez-Delgado, E. (2009). Purpose in life and hopelessness: An empirical study. Universitas Psychologica, 8(2), 447–454.
García-Alandete, J., Martínez, E. R., & Nohales, P. S. (2013). Factorial structure and internal consistence of a Spanish version of the Purpose-In-Life Test. Universitas Psychologica, 12(2), 517–530.
García-Alandete, J., Hernández, G., de Tejada, B., Pérez Rodríguez, S., & Marco-Salvador, J. H. (2019). Meaning in life among adolescents: Factorial invariance of the purpose in life test and buffering effect on the relationship between emotional dysregulation and hopelessness. Clinical Psychology & Psychotherapy, 26(1), 24–34. https://doi.org/10.1002/cpp.2327
Glaw, X., Kable, A., Hazelton, M., & Inder, K. (2017). Meaning in life and meaning of life in mental health care: An integrative literature review. Issues in Mental Health Nursing, 38(3), 243–252. https://doi.org/10.1080/01612840.2016.1253804
Gongora, V. (2014). Satisfaction with life, well-being, and meaning in life as protective factors of eating disorder symptoms and body dissatisfaction in adolescents. Eating Disorders: The Journal of Treatment & Prevention, 22, 435–449. https://doi.org/10.1080/10640266.2014.931765
Griffiths, F., Lindenmeyer, A., Powell, J., Lowe, P., & Thorogood, M. (2006). Why are health care interventions delivered over the internet? A systematic review of the published literature. Journal of Medical Internet Research, 8(2), 1–15. https://doi.org/10.2196/jmir.8.2.e10
Grimaldos, J., Mor, S., Palau-Batet, M., Rachyla, I., & Quero, S. (2019). El sentido de la vida como variable preditiva del cambio clínico tras un Tratamiento cognitivo-conductual basado en Internet para los trastornos adaptativos. Communication presented at V Jornadas de Investigación de la Facultad de Ciencias de la Salud, Universitat Jaume I, Castellón (Spain)
Guerrero-Torrelles, M., Monforte-Royo, C., Rodríguez-Prat, A., Porta-Sales, J., & Balaguer, A. (2017). Understanding meaning in life interventions in patients with advanced disease: A systematic review and realist synthesis. Palliative Medicine, 31(9), 798–813. https://doi.org/10.1177/0269216316685235
Halama, P., & Dedova, M. (2007). Meaning in life and hope as predictors of positive mental health: Do they explain residual variance not predicted by personality traits? Studia Psychologica, 49, 191–200.
Heisel, M. J., & Flett, G. L. (2004). Purpose in life, satisfaction with life, and suicide ideation in a clinical sample. Journal of Psychopathology and Behavioral Assessment, 26(2), 127–135.
Ho, M. Y., Cheung, F. M., & Cheung, S. F. (2010). The role of meaning in life and optimism in promoting well-being. Personality and Individual Differences, 48, 658–663. https://doi.org/10.1016/j.paid.2010.01.008
Hopko, D. R., Lejuez, C. W., Ruggiero, K. J., & Eifert, G. H. (2003). Contemporary behavioral activation treatments for depression: Procedures, principles, and progress. Clinical Psychology Review, 23(5), 699–717.
King, L. A., Heintzelman, S. J., & Ward, S. J. (2016). Beyond the search for meaning: A contemporary science of the experience of meaning in life. Current Directions in Psychological Science, 25(4), 211–216. https://doi.org/10.1177/0963721416656354
Kleftaras, G., & Psarra, E. (2012). Meaning in life, psychological well-being and depressive symptomatology: A comparative study. Psychology, 3(4), 337–345.
Lewinsohn, P. M., Sullivan, J. M., & Grosscup, S. J. (1980). Changing reinforcing events: An approach to the treatment of depression. Psychotherapy: Theory, Research & Practice, 17(3), 322.
Lindsäter, E., Axelsson, E., Salomonsson, S., Santoft, F., Ejeby, K., Ljotsson, B., … & Hedman-Lagerlöf, E. (2018). Internet-based cognitive behavioral therapy for chronic stress: A randomized controlled trial. Psychotherapy and Psychosomatics, 87(5), 296–305.
Maercker, A., Brewin, C. R., Bryant, R. A., Cloitre, M., van, Ommeren., Jones, L. M., … Reed, G. M. (2013). Diagnosis and classification of disorders specifically associated with stress: Proposals for ICD-11. World Psychiatry: Official Journal of the World Psychiatric Association, 12(3), 198–206. https://doi.org/10.1002/wps.20057
Manos, R., Kanter, J., & Busch, A. (2010). A critical review of assessment strategies to measure the behavioral activation model of depression. Clinical Psychology Review, 30, 547–561.
Marco, J. H., & Alonso, S. (2019). Meaning in life buffers the association between clinical anxiety and global maladjustment in participants with common mental disorders on sick leave. Psychiatry Research, 271, 548–553. https://doi.org/10.1016/j.psychres.2018.12.027
Marco, J. H., Cañabate, M., Pérez, S., & Llorca, G. (2017). Associations among meaning in life, body image, psychopathology, and suicide ideation in Spanish participants with eating disorders. Journal of Clinical Psychology, 73(12), 1768–1781. https://doi.org/10.1002/jclp.22481
Marco, J. H, Alonso, S., & Baños, R. (2020a). Meaning-making as a mediator of anxiety and depression reduction during cognitive behavioral therapy intervention in participants with adjustment disorders. Clinical Psychology & Psychotherapy, 1–9. https://doi.org/10.1002/cpp.2506
Marco, J. H., Cañabate, M., Llorca, G., & Pérez, S. (2020b). Meaning in life moderates hopelessness, suicide ideation, and borderline psychopathology in participants with eating disorders: A longitudinal study. Clinical Psychology & Psychotherapy, 27(2), 146–158. https://doi.org/10.1002/cpp.2414
Martela, F., & Steger, M. F. (2016). The three meanings of meaning in life: Distinguishing coherence, purpose, and significance. The Journal of Positive Psychology, 11(5), 531–545. https://doi.org/10.1080/17439760.2015.1137623
Moher, D., Hopewell, S., Schulz, K. F., Montori, V., Gøtzsche, P. C., Devereaux, P. J., … Altman, D. G. (2010). CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ (Clinical Research Ed.), 340, c869. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2844943&tool=
Mor, S., Quero, S., Rachyla, I., Tur, C., & Marco, J. H. (2018). Meaning in life as a predictive variable for clinical symptoms in patients with adjustments disorder. Poster presented at 52nd Annual ABCT Convention, Washington (USA).
Moser, C., Bachem, R., Berger, T., & Maercker, A. (2019). ZIEL: Internet-based self-help for adjustment problems: Results of a randomized controlled trial. Journal of Clinical Medicine, 8(10), 1655.
Musiat, P., & Tarrier, N. (2014). Collateral outcomes in e-mental health: A systematic review of the evidence for added benefits of computerized cognitive behavior therapy interventions for mental health. Psychological Medicine, 44(15), 3137–3150. https://doi.org/10.1017/S0033291714000245
Neimeyer, R. A. (2000). Searching for the meaning of meaning: Grief therapy and the process of reconstruction. Death Studies, 24(6), 541–558.
Noblejas de la Flor, M. A. (1994). Logoterapia. Fundamentos, principios y aplicación. Una experiencia de evaluación del logro interior de sentido. Tesis Doctoral, Universidad Complutense de Madrid, Madrid, España.
O’Donnell, M. L., Metcalf, O., Watson, L., Phelps, A., & Varker, T. (2018). A systematic review of psychological and pharmacological treatments for adjustment disorder in adults. Journal of Traumatic Stress, 31(3), 321–331.
Park, C. L. (2010). Making sense of the meaning literature: An integrative review of meaning making and its effects on adjustment to stressful life events. Psychological Bulletin, 136(2), 257–301. https://doi.org/10.1037/a0018301
Popper, K. (1995). Karl Popper: Philosophy and problems. Cambridge University Press.
Quero, S., Alegre, S., Mor, S., Rachyla, I., Lopez-Montoyo, A., Tur, C., & Marco, H. (2018). El rol predictivo del sentido de la vida en variables psicológicas positivas en pacientes con trastorno adapativo. Poster presented at 4th Congreso Español de Psicología Positiva, Madrid (Spain).
Rachyla, I., Pérez-Ara, M., Molés, M., Campos, D., Mira, A., Botella, C., & Quero, S. (2018). An internet-based intervention for adjustment disorder (TAO): Study protocol for a randomized controlled trial. BMC Psychiatry, 18(1), 161.
Rachyla, I., Mor, S., Cuijpers, P., Botella, C., Castilla, D., & Quero, S. (2020). A guided Internet‐delivered intervention for adjustment disorders: A randomized controlled trial. Clinical Psychology & Psychotherapy. https://doi.org/10.1002/cpp.2518
Routledge, C., & Juhl, J. (2010). When death thoughts lead to death fears: Mortality salience increases death anxiety for individuals who lack meaning in life. Cognition and Emotion, 24(5), 848–854.
Salim, A., Mackinnon, A., Christensen, H., & Griffiths, K. (2008). Comparison of data analysis strategies for intent-to-treat analysis in pre-test–post-test designs with substantial dropout rates. Psychiatry Research, 160(3), 335–345. https://doi.org/10.1016/j.psychres.2007.08.005
Schielzeth, H., Dingemanse, N. J., Nakagawa, S., Westneat, D. F., Allegue, H., Teplitsky, C., et al. (2020). Robustness of linear mixed-effects models to violations of distributional assumptions. Methods in Ecology and Evolution, 11, 1141–1152. https://doi.org/10.1111/2041-210X.13434
Schmider, E., Ziegler, M., Danay, E., Beyer, L., & Bühner, M. (2010). Is it really robust? Reinvestigating the robustness of ANOVA against violations of the normal distribution assumption. Methodology, 6, 147–151.
Shin, J. Y., Lee, Y. A., & Lee, K. H. (2005). The effects of life meaning and emotional regulation strategies on psychological well-being. Korean Journal of Counselling and Psychotherapy, 17, 1035–1057.
Smith, B. W., & Zautra, A. J. (2004). The role of purpose in life in recovery from knee surgery. International Journal of Behavioral Medicine, 11(4), 197.
Soh, H. L., Ho, R. C., Ho, C. S., & Tam, W. W. (2020). Efficacy of digital cognitive behavioural therapy for insomnia: A meta-analysis of randomised controlled trials. Sleep Medicine, 75, 315–325.
Takano, A., Miyamoto, Y., Kawakami, N., & Matsumoto, T. (2016). Web-based cognitive behavioral relapse prevention program with tailored feedback for people with methamphetamine and other drug use problems: Development and usability study. JMIR Mental Health, 3(1), e4875.
Thabane, L., Mbuagbaw, L., Zhang, S., Samaan, Z., Marcucci, M., Ye, C., … Goldsmith, C. H. (2013). A tutorial on sensitivity analyses in clinical trials: The what, why, when and how. BMC Medical Research Methodology, 13, 92. https://doi.org/10.1186/1471-2288-13-92
Vallejo-Sánchez, B., & Pérez-García, A. M. (2015). Positividad y afrontamiento en pacientes con trastorno adaptativo. Anales De Psicología, 31(2), 462–471.
Vos, J., & Vitali, D. (2018). The effects of psychological meaning-centered therapies on quality of life and psychological stress: A metaanalysis. Palliative & Supportive Care, 16(5), 608–632. https://doi.org/10.1017/S1478951517000931
Williams, B., Coyle, J., & Healy, D. (1998). The meaning of patient satisfaction: An explanation of high reported levels. Social Science & Medicine, 47(9), 1351–1359.
Zhang, M. W., & Ho, R. (2017). Moodle: The cost effective solution for internet cognitive behavioral therapy (I-CBT) interventions. Technology and Health Care, 25(1), 163–165.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. Ministerio de Economía y Competitividad (Spain; Plan Nacional I + D + I. PSI2013-41783-R).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The protocol for the current RCT was approved by the Ethical Committee of Universitat Jaume I.
Informed consent
Informed consent was obtained from all participants included in the study, following the guidelines of the Ethical Committee of Universitat Jaume I.
Conflicts of interest/competing interests
The authors declare no conflicts of interest that could have influenced the work reported in this paper.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Quero, S., Palau-Batet, M., Tur, C. et al. Effect of an internet-based intervention for adjustment disorder on meaning in life and enjoyment. Curr Psychol 42, 20543–20555 (2023). https://doi.org/10.1007/s12144-022-03177-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-03177-w