
Abstract
Work-family conflict can lead to irreparable losses to individuals, families and organizations. This matter is especially important for married working women who cannot eschew home responsibilities. To consider an appropriate intervention for this issue, we investigated the effect of a one-month intervention on support from the workplace and the family, individual characteristics and work-family conflict. This quasi-experimental longitudinal study includes an intervention group and a control group, and uses a pre-test, post-test and 6-months follow up design. Participants were 120 married women working in healthcare services, recruited from two cities in South Iran. The web-based multimedia educational program comprised four modules: one for each of the women participants, their spouses, their co-workers, and their workplace supervisors. Data collection tools included a demographic information form, and co-worker support, supervisor social support, spouse support, core self-evaluation and work-family conflict questionnaires. The effect of the intervention was examined at two post-intervention time points. A comparison of changes in mean scores between the intervention and control groups indicated that scores of supervisor support, spouse support, core self-evaluation and work-family conflict in the intervention group one month and six months after the intervention were all significantly improved compared to before the intervention. There was no benefit of the intervention in terms of a change in co-worker support. There was no significant difference across the three time points in the control group. These results confirm that online educational methods can enable health promotion professionals to reduce work-family conflict to the benefit of both employees and organizations.
Similar content being viewed by others


Introduction
Work and family are two important parts of people’s lives. Most organizational behavior experts believe that an imbalance or conflict between one’s working life and family life brings on a set of factors which mutually intensify each other. Work-life imbalance, and associated stressors have become a major challenge for those concerned with good working conditions and quality of life in general (Guest, 2002). Work-family conflict – which includes interference of work with family life (WIF) and family interference with work (FIW) – can cause undesirable individual, family and occupational outcomes (Guest, 2002; Lallukka et al., 2013). Negative outcomes of work-family conflict include: extreme fatigue, depression, feelings of guilt and stress, dissatisfaction with family and married life, an increase in occupational injuries, a reduction in physical health, decline in productivity, less commitment to the organization and absenteeism (Farhadi et al., 2013; Hashim et al., 2012; Lallukka et al., 2013). These harmful outcomes of work-family conflict indicate that there is an urgent need for an intervention to manage this challenge for women who are exposed to work-family conflict. Although work-family conflict can affect all employees, it is particularly important for married women due to their roles as wife and mother, as well as worker. Previous research has indicated that when a couple both work full time, women perform twice as much housework as men (Beutell, 2010). Similarly, there are studies which indicate that working women who get married can anticipate some degree of work-family conflict (Farhadi et al., 2013; Hashim et al., 2012; Lallukka et al., 2013). As such, factors affecting work-family conflict and strategies which can reduce this conflict in this population should be investigated.
There is research which shows that social support provided by the workplace and the family environment can reduce work-family conflict (Adame-Sánchez et al., 2016; Cahill et al., 2015; Shakeri et al., 2021). Family support is considered as support from both spouse and family members, and it can be offered as emotional support (love, sympathy, trust, understanding the concern) and instrumental support (time, money, goods and services) (Namayandeh et al., 2010). Both can help improve job performance and mood (Selvarajan et al., 2013; Yang et al., 2019; Pluut et al., 2018) reported that emotional fatigue and work-family conflict are reduced through spouse’s emotional support. Similarly, Jin (2017) found that spousal support is negatively related to work-family conflict, and that high levels of spousal support can serve to increased job satisfaction and limit job burnout, even when work-family conflict is evident. Jin argued that ways to enhance spousal support should be found for improving work-family conflict. This research included an intervention designed to increase spouse support.
Occupational management support benefits both work and family life by creating learning opportunities, improving decision-making, and increasing problem solving skills, and developing leadership in individuals (Adame-Sánchez et al., 2016; Cahill et al., 2015; Shakeri et al., 2021). Workplace social support systems – such as family-friendly organizational policies, and a supportive organizational atmosphere with perceived supervisor and co-worker support – have been found to reduce work-family conflict (Selvarajan et al., 2013). Studies which have examined the effect of coworker support on reducing the impact of work-family conflict have contradictory findings. Although some studies have been indicated a significant negative correlation between co-worker support and work-family conflict (Shakeri et al., 2021; Yang et al., 2019), there are other studies which have reported a relatively weak correlation or even no correlation with work-family conflict (Namayandeh et al., 2010).
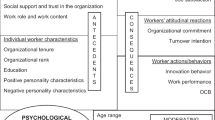
Only one fifth of workers have the flexibility they require to properly manage their occupational and family roles (Selvarajan et al., 2013). Whilst it could be argued that things have improved since this 1997 US National Study of Changing Workforce, there is little evidence that this is so, and anecdotal reports indicate there remains much room for improvement (e.g. Galinsky et al., 2021; Lewis 2020). Moreover, given that many workers with children are part of a dual-income family, it can be appreciated that organizational and family social support for working wives is vital (Selvarajan et al., 2013). A review of the extant literature on social support to reduce work-family conflict is unilluminating in terms of understanding how social support can reduce work-family conflict beyond appreciating that the difference in study outcomes may be due to the demographic and individual differences. In their study of 380 US employees, Michel & Clark (2013) found that 25–28% of the variance in work-family conflicts was explained by individual differences. Other research findings indicate that neuroticism (Lachowska, 2014), locus of control (Fridayanti et al., 2019; Michel & Clark, 2013), self-esteem (Gliwny, 2020), and self-efficacy (Deuling & Burns, 2017) are all involved in work-family conflict. These features are highly interdependent and affect each other. They are a set of these features are recognized as core self-evaluation (Chang et al., 2012). Core self-evaluation reflects an individual’s evaluation of their aptness, competence and ability (Karatepe & Azar, 2013). Individuals who have a high core self-evaluation believe in themselves and their abilities to manage their environment; they have a positive outlook on challenging situations and are expected to seek more social support in their life (St-Onge et al., 2020). Core self-evaluation moderates the negative effect of role overload on satisfaction with work-family balance (Wang & Li, 2019), and if a person does not have sufficient social support in the workplace or at home, then high core self-evaluation can help compensate and reduce the work-family conflict (Haines et al., 2013).
Various studies (O’Mera, 2017; Rathi & Barath, 2013; Wattoo et al., 2018) have indicated a significant relationship between social support and work-family conflict, and work-family conflict with core self-evaluation indices (Haines et al., 2013; Pluut et al., 2018; Yang et al., 2019). Interventions based on education to reduce the impact of these predictors of work-family conflict for working women are limited. To date, studies that have tested a remedial intervention have used traditional in-person methods (Poms et al., 2016; Zarei & Kazemipour, 2020). Another issue is that there are limited interventions in the field of spouse support in Iran. This can be related to the cultural context of the society. There is typically a strict division of labor in the home, and families expect a large contribution from women, with little contribution from other family members (Khosravan et al., 2018). It should also be noted that this is women’s experiences in many other societies to some degree. Social values and norms in a given culture can form the nature and intensity of experiences in the family and the occupational scope for women and men (Powell et al., 2009). Therefore, work-family conflict, the factors affecting it and the strategies which decrease it should be evaluated in different societies. Nevertheless, it is important to examine the effect of social support-based educational interventions and the effect of personality, including core self-evaluation features to identify ways to reduce work-family conflict.
It is possible that working women are not be able to appropriately engage with in-person educational methods which requires precise and invariable scheduling due to the lack of enough time. This is especially so in the current situation, as we are still living in the COVID-19 pandemic. The requirement for social distancing has limited the potentials of in-person programs, and raised a need to provide remote interventions. Moreover, it has been suggested that the pandemic has created new work-related challenges (Rudolph et al., 2021), particularly for women workers (Lewis, 2020). Remote educational programs can be more accessible to working women and provide a realistic opportunity to study the contents even when they have very little leisure time.
The Current Study
Based on the discussion above, the aim of this study was to evaluate a multimedia educational program in terms of its efficacy to reduce work-family conflict – specifically with respect to increased use of social support, and increased core self-evaluation. We hypothesized the following:
-
There will be a mean change indicating improvement in social support scores in the organizational dimension (perceived responsible support and peer support) for the intervention group, but not the control group following the intervention (both post-test and at 6-months follow-up.)
-
There will be a mean change indicating improvement in social support scores in the family dimension (spouse support) for the intervention group, but not the control group following the intervention (both post-test and at 6-months follow-up.)
-
There will be mean changes indicating improvement of core self-assessment (neuroticism, self-esteem, self-efficacy and source of control) for the intervention group, but not the control group following the intervention (both post-test and at 6-months follow-up.)
-
There will be a mean change indicating improvement in work-family conflict scores for the intervention group, but not the control group following the intervention (both post-test and at 6-months follow-up.)
Method
Location of Study and Participants
The study setting was in two cities – Bushehr and Borazjan – located in South Iran. The two cities are culturally close to each other, yet at a distance of about 60 km, hence minimizing the possibility of participants communicating and exchanging the information about the study. Participants from one city (Borazjan) were designated as the control group and the other (Bushehr) as the intervention group by a simple randomization method (drawing lots).
Informed consent was provided by participants’ spouses and co-workers, as well as supervisors of the integrated healthcare services of the two cities in the study where recruitment took place. Volunteers were incentivized to join and complete the study by including a cash prize draw for each group at the end of the study. Inclusion criteria for participation were: married female employees working in integrated healthcare services (of the given cities) who consented to participate in the study; at least 3-years or more work experience; married for 3 years or more; at least one child; and educated to at least a higher education diploma level. Exclusion criteria for the data analyses were those who: withdrew from the study after consent; did not complete the questionnaires; became ill or pregnant during the study; or did not have the consent of their spouse. According to Alavi Arjmand et al., (2013), for sufficient power to detect a difference at the p < 0.05 level the sample size needed was n = 51 in each group. We recruited 60 persons into both groups to accommodate a drop-out rate of nearly 20% in each group.
223 female employees from Bushehr and Borazjan centers for integrated healthcare services were invited to participate in this study (88 from Borazjan and 135 from Bushehr). From the 195 volunteers who met the study inclusion criteria (78 in Borazjan and 117 in Bushehr), 30 people did not consent to participate in the study. Finally, out of 165 people who met the inclusion criteria and were willing to participate in the study, 60 volunteers from each of the two cities were randomly selected to participate in the study. 58 and 57 people completed the study in the intervention and the control group, respectively. (See Fig. 1.)

Consort flow chart of participants
Procedure
The study used a quasi-experimental design which compared an intervention group with a control group before the intervention, one month after the start of the intervention study (post-test), and again in a follow-up after six-months. The intervention group followed a web-based multimedia educational program. During the study period the control group had not have access to the educational programme. This was available to them after the study, in line with good ethical practice. At the post-test and six-month follow-up data collection points, the effect of the educational intervention on the variables of supervisor support, co-worker support, spouse support, core self-evaluation, and work-family conflict was assessed.
Intervention
The educational content was prepared and validated based on a literature review of research related to work-family conflict, and two workshops with five experts in the fields of health promotion and education to discuss the proposed educational content of the intervention in terms of adequacy, importance and necessity. After applying the experts’ qualitative comments, the educational content was presented to 15 members of the target group (5 supervisors, 5 co-workers, 5 employees’ spouses) to be examined in terms of clarity and understanding. Finally, after eliminating ambiguities, the educational content was provided in the form of multimedia on the Salamooz platform (plus.salamooz.com).
Before the intervention, the questionnaires were completed by all participants in the two groups. Then, the initial information on how to enter the educational programs was sent to the mobile phone of each participant in the intervention group. That is, the participants, their spouses, supervisors, and co-workers were each given a dedicated, confidential username and password to log into the multimedia educational program. The intervention commenced with information on how to use the educational packages, according to participatory role. A WhatsApp group was also created to resolve any ambiguities about logging into the website and how to use the educational packages. The time allocated to see the educational programs was one month. Engagement with the intervention was monitored during the month through the website administration panel, and weekly reminders to engage in the intervention were sent to workplaces and through the WhatsApp group, to promote participation.
At the end of the one-month educational program intervention, the study questionnaires were resent to all participants for the post-test analysis, and they were also sent again for the six-month follow-up. At the end of the study, the educational packages were also made available to the control group in order to observe good ethical practice, and the cash prizes were awarded to both groups by drawing lots.
Multimedia Educational Content
The multimedia educational content was provided in 4 educational packages to improve core self-evaluation features in the female employees, and to reinforce social support provided by coworkers, officials and spouses. These educational packages included the following parts:
-
Female Employees (The role of individual characteristics in reducing work-family conflict). This package comprised five elements: Definition of work-family conflict and problems caused by it; self-esteem and ways to improve it; self-efficacy and ways to increase it; locus of internal control and ways to reinforce it; and neuroticism and ways to deal with it.
-
Co-workers (The role of co-worker support in reducing work-family conflict). This package had three parts: Definition of work-family conflict and problems caused by it; definition of social support and its advantages; how social support provided by co-workers can reduce work-family conflict and ways to increase positive relationships.
-
Supervisors (The role of supervisor support in reducing work-family conflict). This package consisted of three parts: Definition of work-family conflict and problems caused by it; definition of social support and its advantages; how social support provided by a supervisor can reduce work-family conflict and ways to increase it.
-
Spouses (The role of spouse support in reducing work-family conflict). This package had three parts: Definition of work-family conflict and problems caused by it; definition of social support and its advantages; how social support provided by spouse can reduce work-family conflict and ways for men to support their wives.
Tools for Gathering Data
-
Demographic information: A self-report form that asked for age, education, work experience, type of employment status, number of children, age of children, caregiving for other family members (e.g. elderly parents), duration of marriage, income, and organizational position.
-
Work-Family Conflict Scale (Carlson et al., 2000). An 18-item questionnaire with two subscales, each with 9 items. These investigate interference of work with family life (WIF), and family life interference with work (FIW). Each subscale examines three aspects of the concept – time-based conflict, energy-based conflict, and behavior-based conflict. Examples of items in this scale are “My job keeps me away from my family activities more than usual” and “Because of the stress I endure at home, I am more involved in work issues at work.” Items were scored using a 5-point Likert scale ranging from strongly disagree (1) to strongly agree (5), and higher scores indicated higher levels of work-family conflict (WFC). Good reliability was affirmed by Carlson et al., (2000): Cronbach’s alphas = 0.78 to 0.87. In the current study, Cronbach’s alphas for WIF and FIW and total WFC were 0.89, 0.89 and 0.91, respectively.
-
Supervisor social support. A 5-item subscale from the Job Content Questionnaire (Karasek et al., 1998) was used to evaluate perceived supervisor social support. The measure included items such as: “My Supervisor pays attention to my family problems” and “My Supervisor pays attention to what I say” and used a 4-level response scale from strongly disagree to strongly agree (1 to 4), where higher scores represented more support from the supervisor. Choobineh et al., 2011) affirmed the reliability of this scale: Cronbach’s alpha 0.90. In the present study, internal consistency was confirmed: Cronbach’s alpha = 0.86.
-
Coworker social support. This variable was measured with a modified version of the 10-item work support subscale (Deeter-Schmelz & Ramsey, 1997). Examples of items are “My coworkers listen to my work problems” and “My coworkers advise me on my family matters”. A 5-point response scale from rarely to always (1 to 5) was used, and higher scores represented more support from coworkers. (Aslani et al., 2014) affirmed the reliability of the coworker support scale (Cronbach’s alpha 0.9). In the current study, the internal consistency was confirmed: Cronbach’s alpha = 0.87.
-
Spouse support. Social support provided by the participant’s spouse was assessed using three items used by Selvarajan et al., (2013). These questions asked who was responsible for: household chores including cleaning the house; cooking; and taking care of children. Responses have been scored using 3-point scale from 1 (I do), 2 (this responsibility is equally shared with my spouse), and 3 (my spouse has this responsibility). Higher scores represented more support. In the original study Cronbach’s alpha was 0.8. In the current study, Cronbach’s alpha = 0.64.
-
Core self-evaluation scale (Judge et al., 2003). This is a 12-item questionnaire which measures four specific core traits (self-esteem, generalized self-efficacy, neuroticism, and locus of control). It is strongly associated with job performance, job satisfaction and life satisfaction, making it an appropriate dispositional measure for this research. Examples of items are “I do my job successfully” and “I do not feel in control of the success of my work”. A 5-point Likert scale was used ranging from strongly disagree (1) to strongly agree (5), and to maintain higher scores representing higher core self-evaluation items 2, 4, 6, 7, 10 and 12 were reversed. A Cronbach’s alpha of 0.9 has been reported (O’Mera, 2017). In the present study Cronbach’s alpha = 0.78.
Data Analysis
First, quantitative data distribution was examined by the Shapiro-Wilk test in both groups. Mann-Whitney U-tests and Independent T-tests were used to compare the quantitative demographic variables between the intervention and control groups. Chi-square and Fisher’s exact tests were used to compare categorical demographic variables. Repeated measures analysis of variance and Independent T-tests were used to compare the changes in the mean of results in the three time points (pre-test, post-test and at follow-up) and to compare the changes in the mean of both groups, respectively. The effect of time and the interaction between time point and group were examined for all the study variables (supervisor support, co-worker support, spouse support, work-family conflict, family-work conflict, and core self-evaluation). If the interaction between the time and the group for a given variable was significant, then an intra-group comparison was conducted separately, sorted by the intervention and control group as well as a pairwise comparison of time point. The mean of changes in the score of the perceived supervisor, co-worker, and spouse support, core self-evaluation and work-family/family-work conflict between both groups of intervention and control was also compared during the study according to time point (before intervention, one-month and six-months after the intervention). Data were analyzed using SPSS software version 24, and significance determined at the conventional level p ≤ 0.05.
Results
Data from 115 married female employees of integrated healthcare services in two cities were analyzed. 58 of the 60 participants in the intervention group and 57 of the 60 participants in control group completed the study. The majority of participants in both groups were family health experts (43.1% intervention and 36.8% control). The average age in the intervention group and the control group was 38.57 ± 5.79 and 36.32 ± 6.61 years respectively. Most participants had a bachelor’s degree (62.1% intervention and 61.4% control). The intervention and control groups were compared with respect to the distribution of demographic variables. As seen, Table 1, the two groups were very similar. The only difference seen was in age and income.
Supervisor Support
Time since intervention and the interaction between time and group was statistically significant for supervisor social support (F = 12.90, p < 0.001). Intra-group comparisons indicated that in the intervention group, there was a significant difference in mean supervisor support in the three time points (F = 22.82, p < 0.001) (See Table 2). Pairwise comparison of times in the intervention group indicated that post-test and at six-months follow-up there was a statistically significant increase in supervisor support than before the intervention (p < 0.001) (See Table 3). Comparisons between the two groups showed that the mean of changes in supervisor support score was significantly different one-month and six-months after the intervention than before the intervention (p = 0.002, and p < 0.001) (See Table 4).
Spouse Support
For the intervention group, social support from spouses did not differ at either time point after the intervention (F = 1.96, p = 0.149). There was, however, a significant interaction between time and group (F = 12.14, p < 0.001). Intra-group comparisons indicated that there was a significant decrease in spouse support in the three time points in control group (F = 9.27, p < 0.001) (see Table 2). That is, in the control group the post-test and follow-up measures were significantly different to the pre-test baseline measure (p = 0.001, p = 0.004) (see Table 3). A comparison of the mean changes between the two groups showed that spouse support in the intervention group increased, whereas in the control group it decreased both one-month and six-months after the intervention compared to baseline (p = 0.001, and p < 0.001) (see Table 4).
Co-worker Support
There was a significant time effect for co-worker support (F = 16.69, p < 0.001), but no interaction between time and group (F = 0.38, p = 0.68). Comparisons of the average of the mean changes between the intervention and control groups did not reach statistically significant difference (p ≥ 0.05) (see Table 4).
Core Self-evaluation
There was a time effect (F = 6.34, p = 0.007) and a time-group interaction (F = 8.69, p ≤ 0.001) for the core self-evaluation variable. Intra-group comparisons indicated a significant difference only in the intervention group (F = 13.85, p < 0.001) (see Table 2). Pairwise comparisons of times in the intervention group indicated a significant increase in core self-evaluation post-test and at six-months follow-up compared to pre-test (p < 0.001, and p = 0.005) (see Table 3). Comparing the average changes between two groups showed that one-month and six-months after the intervention core self-evaluation score in the intervention and control group had increased and decreased, respectively and there was a significant difference in changes between two groups (p = 0.001, and p = 0.006) (see Table 4).
Work-family Conflict
There was a time effect (F = 22.43, p < 0.001) and a time-group interaction (F = 23.50, p < 0.001) for work-family conflict. Intra-group comparisons showed that the mean score of work-family conflict in the three test times was significantly different only in the intervention group (F = 1.29, p = 0.270) (see Table 2). Pairwise comparisons in the intervention group indicated that there was a significant decrease in work-family conflict one-month and six-months after the intervention than before it (p < 0.001). There was also a significant improvement in work-family conflict score at six-months compared to one-month after the intervention (p ≤ 0.001) (see Table 3). A comparison of the average changes in work-family conflict score between the two groups one-month and six-months after the intervention revealed that for the control group work-family conflict had increased at both time points, and the difference between the two groups was significant. (P < 0.001) (See Table 4).
Family-work Conflict
Time effect (F = 12.48, p < 0.001) and time-group interaction (F = 7.98, p ≤ 0.001) were significant for the family-work conflict variable. Intra-group comparisons indicated a significant difference in mean family-work conflict only in the intervention group (F = 15.34, p < 0.001) (see Table 2). Pairwise comparisons of times in the intervention group indicated that the mean score of family-work conflict was significantly decreased post-test and at follow-up six-months after the intervention than before it (p < 0.001, and p = 0.01) (see Table 3). Family-work conflict scores in the two groups one-month and six-months after the intervention were improved more in the intervention group than in the control group and the difference between two groups was statistically significant (F = 2.49, p = 0.014) (see Table 4).
Total Work-family Conflict
Time effect (F = 22.09, p < 0.001) and time-group interaction (F = 19.22, p < 0.001) were significant for total work-family conflict. Intra-group comparisons indicated that the mean total work-family conflict score was statistically different across the three time points only in the intervention group (F = 31.14, p < 0.001) (see Table 2). Pairwise comparisons of times in the intervention group indicated that there was a significant decrease in mean total work-family conflict one-month and six-months after the intervention (p < 0.001, p < 0.001) (see Table 3). Comparing the average changes between two groups showed that one-month and six-months after the intervention, the decrease in total work-family conflict scores in the intervention group were significantly greater than in the control group (p < 0.001, p < 0.001) (see Table 4).
Discussion
This study investigated the effect of a four-part multimedia educational intervention to improve family and organizational social support and core self-evaluation towards reciprocally reducing work-family conflict in married female employees. We found that the multimedia educational intervention significantly increased core self-evaluation, supervisor and spouse support and there was a reciprocal reduction in work-family conflict, and family-work conflict in the intervention group at the one-month and six-month follow-up time points, when compared to a control group. There was no impact of the co-workers education on reducing work-family conflict for participants.
On interesting aspect of our findings was that whilst the intervention clearly had a significant impact post-test, and the improvement was maintained at follow-up, there was generally a lack of significant difference between post-test and follow-up (1 month and 6 months after the intervention). So, whilst an improvement was quickly seen and to some extent sustained, there was no further improvement. A hard look at the data indicated some reduction in support, if minor after six months. This was not expected. Essentially, this can be due to forgetting the education provided due to the long distance between the test post and follow-up, and an even longer time in previous levels of support. Altogether, these findings indicate the importance of the education and a need to repeat the education until the required levels of support become the social norm. Sustainability is an important aspect that should be considered in all intervention programs.
The multimedia educational program increased the social support provided to the female participants by their supervisors. We suggest this increase was due to a change in supervisor’s attitudes and perceptions as a result of engaging with the premises of the education. The educational program led them to understand the benefit of supporting employees who have family responsibilities as well as work demands, and the negative consequences of work-family conflict. This finding is in accord with a study performed by Odle-Dusseau et al., (2016) which indicated that educating work supervisors on matters of family-centred support is effective. This in turn had organizational benefits as increased support also improved employees’ job performance, organizational commitment and job satisfaction. Similarly, Kelly et al., (2014) conducted a randomized trial which showed that their ‘STAR’ intervention (supervisor family-centred support education and individual education in order to augment control over optimal working time) increased supervisor support and control over working time by employees.
Spouse support for female workers was seen to be most resistant to improvement in our multimedia educational intervention study. Intragroup comparisons showed that there was no change in spouse support post-test or at follow-up in the intervention group, and in the control group where there was a difference over time, this was not in the right direction. That is, during the period of the study spouse support did not improve for the intervention groups, and significantly decreased for the control group. This is not an obvious reason. Nevertheless, we can make some assumptions from the timing of this research – during the COVID-19 pandemic – which work demands increased for these female healthcare workers, who were also wives and mothers, and that family support from the husband did not change. Or at least, the improvement provided by the intervention was not sufficient to mitigate the increase in work demands and improve WFC. Likewise, for the female healthcare workers, who were also wives and mothers in the control group without any change in family support during the challenging time for healthcare workers, there was a perceived decrease in support because of the increase in work demands. We acknowledge this is speculative, but plausible. To date there is a dearth of peer-reviewed empirical studies that have looked at spousal support for healthcare workers during the COVID-19 pandemic.
It remains, that we suggest that our multimedia educational program the potential to increase the spouse support for female employees. Certainly, previous studies have indicated that instrumental support provided by a spouse can be important for the well-being of women, especially in cultures with little gender equality (Bayhan Karapinar et al., 2020). For example, Cooper et al., (2021) used an intervention program called RE-AIM (reach, effectiveness, adoption, implementation and maintenance) to increase exclusive breastfeeding and family planning in Tanzania, and found that including male spouses in household education was important for effectiveness. Similarly, a couples support-centred intervention led to an understanding in men that supporting one’s spouse creates increased affection and interest between the mother and infant in postpartum women when compared to a control group (Khanzadeh & Mogaddam Tabrizi, 2020). In cultures such as Iran, where men and women internalize their traditional gender roles, and believe that their family life and work are affected by a woman’s work outside the home, the participation of spouses in household chores is typically inadequate, and their expectations of women a cause of conflict (Pourmeidani et al., 2014). In our study, spouse support education may have increased the support by changing the men’s traditional outlook about the role division.
Our study also incorporated education to increase supervisor support for the employee which was effective, and support from managers which was effective, but the education to increase co-worker support in our study did not contribute to reducing work-family conflict. The intervention we utilized to increase co-worker support did not lead to significant changes in the intervention group compared to the control group. It is difficult to fully appreciate the reason why this was so, although the few previous intervention studies in the literature have not measured changes in the extent of co-worker support, and just the results obtained from coworker support are provided. Jungert et al., (2018), for example, indicated that a short-term supportive intervention provided by coworkers can be effective in creating support for the essential needs of the employees and increasing their incentive, but did not overtly measure change. Chiaburu (2010) argued that co-workers could be more significant in the professional development of employees than organization and supervisor support, but in Chiaburu’s study, unlike our study, the focus was on the transfer and retention of the educational provided for workplace effectiveness per se, rather than the relationships among co-workers for social support to ameliorate work-family conflict. Critically, the two studies together both indicate difficulties in harnessing co-worker social support to reduce work-family conflict. It remains, however, that the lack of influence of the multimedia educational program we provided to improve co-worker support could be due to the specific conditions caused by prevalence of the Covid-19 pandemic raging at the time of the study. Teleworking, and a reduction in the presence of co-workers clearly reduced opportunities to provide support at times of need. Similarly, the requirement to keep a ‘social distance’ reduced the interaction of people who were working in the workplace. Together, this situation prevented consideration of the demand and provision of the support that could have been expected – at least pre-Covid-19. Consequently, we have to recognize that the supportive educational provided to co-workers in this study was not been fully implemented in the current context. It is difficult to say that there was no effect. We can only consider that the conditions were not conducive to test that aspect of the program.
Of interest to the question of the value of coworker support to the management of work-family conflict, are the results of a facilitator-led 4-month educational intervention by Marino et al., (2016). This intervention used the aforementioned STAR support education (Kelly et al., 2014) for the staff and managers of a US nursing home towards a reduction in employee’s sleep problems over a 12-month follow-up. The rationale was that the educational intervention would improve support in the workplace, and in turn, work-family conflict which causes sleep problems. However, the educational intervention did not improve work-family conflict compared to a control group, nor sleep problems. Marino et al., (2016) suggest there are challenges in reducing work-family conflict in those working shifts in a nursing home context. However, we suggest the different outcomes may be more apparent than real.
The self-development block in the multimedia educational program focused on core self-evaluation – reinforcing the self-efficacy, locus of control and self-esteem and coping with neuroticism. This successfully increased participant’s core self-evaluation after the intervention compared to before the intervention. This is an original finding. There are no previous educational health promotion intervention studies in this area, to our knowledge, in the extant literature. There are studies that have used the component parts of this concept to suggest our finding was to be expected. For example, (Jahani Eftekhari et al., 2020) ran a randomized clinical trial in which the intervention was based on self-efficacy theory and health literacy to enhance health promotion behaviours of female volunteers from health centers. They found significantly increased self-efficacy, health literacy and health promotion behaviours in the intervention group, relative to a control group. Also, a semi-empirical intervention that involved nursing students indicated that a self-esteem reinforcement intervention had considerable effect on improving levels of self-esteem and self-efficacy (Ribeiro et al., 2020). The increase in core self-evaluation in the present study can be explained as the reciprocal effect of the elements of self-efficacy, self-esteem and locus of control on each other and the synergy in the final results. The multimedia educational program may also have helped participants identify their individual resources and reinforce them. That is, the intervention may work because it supports people to investigate their neuroticism and perceive stressors more as a challenge and less as a threat.
The multimedia educational packages provided in the field of the workplace/family support and core self-evaluation modified and reduced work-family conflict and family-work conflict. The impact of the supportive intervention for improving work-family conflict and its consequences has been examined in evaluations of other studies (Bray et al., 2018; Hammer et al., 2011; Kelly et al., 2011), but none of these used a multimedia approach. Bray et al., (2018) conducted a semi-empirical study to investigate the effects of supportive and flexibility interactions on employees’ work performance. They found that supervisor support which decreased working hours by one hour per week reduced work-family conflict. Two intervention studies based on the provision of family-centred support found an increase in job satisfaction, physical health, as well as sleep status improvement and reduced work-family conflict (Hammer et al., 2011; Kelly et al., 2011).
Our multimedia educational programs may augment social support and consequently reduce work-family conflict among female employees by changing the gender roles views’ of men, and by providing an understanding of family and work roles of female employees to work supervisors.
According to the Conservation of Resources model (Grandley & Cropanzano, 1999) and the Selection, Optimization and Compensation model (Baltes & Baltes, 1990), people are capable of accessing and improving using their available resources of social support. When people access these resources, they may optimally allocate their available social support to support their well-being (Hobfoll, 2001). Therefore, individuals with a higher level of social support at work (or at home) can consume less of their personal resources in the work (family) scope and they can thrive. That is, social support provides personal resources that can be invested in one’s work (family) which then allows them to be effective in this field. This also translates to high level of social support at work (family) can reduce work-family conflict and accordingly reduce family-work conflict (Baltes & Baltes, 1990). In the field of core self-evaluation, those individuals who have a keen awareness of their personal resources and use of them improved their understanding on combining their roles and this led to a more positive experience in combining occupational and family roles.
Strengths and Limitations
This study is the first simultaneous intervention of individual education and family/organizational support in the area of work-family conflict among Iranian female employees. This study also has some limitations like all studies, despite our efforts to provide a developed intervention in the area of work-family conflict. The possibility of individual randomization and using randomized controlled test (RCT) which is considered as a gold standard method for investigating interventions, was not possible due to the particular conditions of the studied samples and their close relationships with each other. Nevertheless, we are confident that our design, and sample size mitigated for this limitation.
The participants in the current study were public sector employees, where salaries and wages are the same regardless of gender and their work schedules are more flexible than many private sector employees, so the results obtained cannot be generalized to the private sector. Similarly, because recruitment was limited to married women working for a healthcare organization in a specific province of Iran, generalizing the results to other jobs and provinces becomes problematic. We also acknowledge that the effect of supportive interventions for men in terms of reducing work-family conflict may be different. We recruited female employees with children in the study regardless of the age range of their children to avoid a limitations in sample size. It is possible, however, that working mothers with children at primary school and younger benefit more from the intervention due to the more conflicts in both aspects of work and family (Kelly et al., 2014). This issue should be considered in future studies.
Conclusions
Work-family/family-work conflict can be reduced using multimedia educational program that reinforces core self-evaluation, and increases supervisor and spouse support to working women. These changes can be retained for at least six months after the intervention. Health promotion specialists, work and family psychologists, organizations and all who try to reduce work-family conflict and family-work conflict should pay attention to individual, family and organizational aspects as these are all influential when intervention to ameliorate work-family conflict is needed.
Data Availability
Data is available on written request to the corresponding author.
References
Adame-Sánchez, C., González-Cruz, T. F., & Martínez-Fuentes, C. (2016). Do firms implement work–life balance policies to benefit their workers or themselves? Journal of Business Research, 69(11), 5519–5523. https://doi.org/10.1016/j.jbusres.2016.04.164
Alavi Arjmand, N., Kashaninia, Z., Hosseini, M. A., & Rezasoltani, P. (2013). Effect of stress management on job stress and work-family conflict among nurses. Hayat Journal, 18(4), 81–91. Retrieved from http://hayat.tums.ac.ir/article-1-16-en.html
Aslani, K., Amanalahi, A., Saidi, Z., & Sardari Nasab, K. (2014). The relationship between work engagement, self-efficacy for work/family conflict management, family and work support with job burnout among administrative office personnel’s in Ahvaz. Biannual Journal of Applied Counseling, 3(3), 79–92
Baltes, P. B., & Baltes, M. M. (1990). Psychological perspectives on successful aging: The model of selective optimization with compensation. In P. B. Baltes, & M. M. Baltes (Eds.), Successful aging: Perspectives from the behavioral sciences (pp. 1–34). Cambridge University Press. https://doi.org/10.1017/CBO9780511665684.003
Bayhan Karapinar, P., Metin Camgoz, S., & Tayfur Ekmekci, O. (2020). Employee wellbeing, workaholism, work–family conflict and instrumental spousal support: A moderated mediation model. Journal of Happiness Studies, 21(7), 2451–2471. https://doi.org/10.1007/s10902-019-00191-x
Beutell, N. J. (2010). Work schedule, work schedule control and satisfaction in relation to work-family conflict, work‐family synergy, and domain satisfaction. Career Development International. https://doi.org/10.1108/13620431011075358
Bray, J. W., Hinde, J. M., Kaiser, D. J., Mills, M. J., Karuntzos, G. T., Genadek, K. R. … Hurtado, D. A. (2018). Effects of a flexibility/support intervention on work performance: Evidence from the work, family, and health network. American Journal of Health Promotion, 32(4), 963–970. https://doi.org/10.1177/0890117117696244
Cahill, K. E., McNamara, T. K., Pitt-Catsouphes, M., & Valcour, M. (2015). Linking shifts in the national economy with changes in job satisfaction, employee engagement and work–life balance. Journal of Behavioral and Experimental Economics, 56, 40–54. https://doi.org/10.1016/j.socec.2015.03.002
Carlson, D. S., Kacmar, K. M., & Williams, L. J. (2000). Construction and initial validation of a multidimensional measure of work–family conflict. Journal of Vocational Behavior, 56(2), 249–276. https://doi.org/10.1006/jvbe.1999.1713
Chang, C. H., Ferris, D. L., Johnson, R. E., Rosen, C. C., & Tan, J. A. (2012). Core self-evaluations: A review and evaluation of the literature. Journal of Management, 38(1), 81–128. https://doi.org/10.1177/0149206311419661
Chiaburu, D. S. (2010). The social context of training: coworker, supervisor, or organizational support? Industrial and Commercial Training, 42(1), 53–56. https://doi.org/10.1108/00197851011013724
Choobineh, A., Ghaem, H., & Ahmedinejad, P. (2011). Validity and reliability of the Persian [Farsi] version of the Job Content Questionnaire: A study among hospital nurses. Eastern Mediterranean Health Journal, 17(4), 335–341
Cooper, C. M., Drake, M., Kavle, J. A., Nyoni, J., Lemwayi, R., Mabuga, L. … George, J. (2021). Implementing a novel facility-community intervention for strengthening integration of infant nutrition and family planning in Mara and Kagera, Tanzania. International Journal of Environmental Research and Public Health, 18(8), 4105. https://doi.org/10.3390/ijerph18084105
Deeter-Schmelz, D. R., & Ramsey, R. P. (1997). Considering sources and types of social support: A psychometric evaluation of the House and Wells (1978) instrument. The Journal of Personal Selling and Sales Management, 17(1), 49–61. https://www.jstor.org/stable/40471654
Deuling, J. K., & Burns, L. (2017). Perfectionism and work-family conflict: Self-esteem and self-efficacy as mediator. Personality and Individual Differences, 116(1), 326–330. https://doi.org/10.1016/j.paid.2017.05.013
Farhadi, A., Movahedi, Y., Nalchi, M., Daraei, M., & Mohammadzadegan, R. (2013). The relationship between Work-family conflict, burnout dimensions and intention to leave among female nurses. Iran Journal of Nursing, 26(84), 34–43. Retrieved from http://ijn.iums.ac.ir/article-1-1638-en.html
Fridayanti, H., Indyastuti, D. L., & Anggraeni, A. I. (2019). The effect of Work-Family Conflict on Job Stress of Country Civil Apparatus with Locus of Control as a moderation. ICORE, 5(1). ISBN: 978-623-7144-28-1
Galinsky, E., Kim, S. S., & Pal, I. (2021). An inclusive workplace and employee engagement: Surviving and thriving. Family and Work Institute. Available at: https://cdn.sanity.io/files/ow8usu72/production/37c37190696a1cab57046c1f65f3d
Gliwny, M. (2020). The relationship between work-family conflict and family-work conflict, and self-esteem and emotional intelligence among managers. Zeszyty Naukowe Małopolskiej Wyższej Szkoły Ekonomicznej w Tarnowie, 45, 137–151. https://doi.org/10.25944/znmwse.2020.01.137151
Grandley, A. A., & Cropanzano, R. (1999). The conservation of resources model applied to work-family conflict and strain. Journal of Vocational Behavior, 54(2), 350–370. https://doi.org/10.1006/jvbe.1998.1666
Guest, D. E. (2002). Perspectives on the study of work-life balance. Social Science Information, 41(2), 255–279. https://doi.org/10.1177/0539018402041002005
Haines, V. Y., III., Harvey, S., Durand, P., & Marchand, A. (2013). Core self-evaluations, work–family conflict, and burnout. Journal of Marriage and Family, 75(3), 778–793. https://doi.org/10.1111/jomf.12026
Hammer, L. B., Kossek, E. E., Anger, W. K., Bodner, T., & Zimmerman, K. L. (2011). Clarifying work–family intervention processes: The roles of work–family conflict and family-supportive supervisor behaviors. Journal of Applied Psychology, 96(1), 134. https://doi.org/10.1037/a0020927
Hashim, N., Ishar, N. I. M., Rashid, W. E. W., & Masodi, M. S. (2012). Personality traits, work-family conflict and job satisfaction: Items validity using Rasch measurement approach. Procedia-Social and Behavioral Sciences, 65, 1013–1019. https://doi.org/10.1016/j.sbspro.2012.11.235
Hobfoll, S. E. (2001). The influence of culture, community, and the nested-self in the stress process: Advancing conservation of resources theory. Applied Psychology, 50(3), 337–421. https://doi.org/10.1111/1464-0597.00062
Jahani Eftekhari, M., Peyman, N., & Doosti, H. (2020). The effect of educational intervention based on the self efficacy and health literacy theory on health promoting lifestyles among female health volunteers of Neyshabur, Iran. Health and Development Journal, 6(4), 302–313. https://doi.org/10.22062/JHAD.2018.91267
Jin, X. (2017). The relationship of work-family conflict to job burnout and job satisfaction in information technology employees in Korea: The moderating effects of spousal support. International Journal of Applied Engineering Research, 12(20), 9739–9745
Judge, T. A., Erez, A., Bono, J. E., & Thoresen, C. J. (2003). The core self-evaluations scale: Development of a measure. Personnel Psychology, 56(2), 303–331. https://doi.org/10.1111/j.1744-6570.2003.tb00152.x
Jungert, T., Van den Broeck, A., Schreurs, B., & Osterman, U. (2018). How colleagues can support each other’s needs and motivation: An intervention on employee work motivation. Applied Psychology, 67(1), 3–29. https://doi.org/10.1111/apps.12110
Karasek, R., Brisson, C., Kawakami, N., Houtman, I., Bongers, P., & Amick, B. (1998). The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. Journal of Occupational Health Psychology, 3(4), 322
Karatepe, O. M., & Azar, A. K. (2013). The effects of work–family conflict and facilitation on turnover intentions: The moderating role of core self-evaluations. International Journal of Hospitality & Tourism Administration, 14(3), 255–281. https://doi.org/10.1080/15256480.2013.809987
Kelly, E. L., Moen, P., Oakes, J. M., Fan, W., Okechukwu, C., Davis, K. D., & Hanson, G. C. (2014). Changing work and work-family conflict: Evidence from the work, family, and health network. American Sociological Review, 79(3), 485–516. https://doi.org/10.1177/0003122414531435
Kelly, E. L., Moen, P., & Tranby, E. (2011). Changing workplaces to reduce work-family conflict: Schedule control in a white-collar organization. American Sociological Review, 76(2), 265–290. https://doi.org/10.1177/0003122411400056
Khanzadeh, Z., & Mogaddam Tabrizi, F. (2020). The effect of supportive couple-centered counselling on perception of support for spouse and maternal attachment in parturients referring to health centers of Urmia University of Medical Sciences in 2018-19. Avicenna Journal of Nursing and Midwifery Care, 28(2), 112–126. Retrieved from http://nmj.umsha.ac.ir/article-1-2087-en.html
Khosravan, S., Jar, A., Moghadam, S., L., & Mazlom, B. (2018). The impact of family-centered educational-support program on work-family conflicts of female nurses in the city of Zabol in 2017. Community Health Journal, 12(4), 1–10. Retrieved from http://chj.rums.ac.ir/article_87032.html
Lachowska, B. H. (2014). Neuroticism, work demands, work-family conflict and job stress consequences. Medycyna Pracy, 65(3), 387–398
Lallukka, T., Arber, S., Laaksonen, M., Lahelma, E., Partonen, T., & Rahkonen, O. (2013). Work–family conflicts and subsequent sleep medication among women and men: a longitudinal registry linkage study. Social Science & Medicine, 79, 66–75. https://doi.org/10.1016/j.socscimed.2012.05.011
Lewis, H. (2020). The coronavirus is a disaster for feminism. The Atlantic, 19(03)
Marino, M., Killerby, M., Lee, S., Klein, L. C., Moen, P., Olson, R. ... Buxton, O. M. (2016). The effects of a cluster randomized controlled workplace intervention on sleep and work-family conflict outcomes in an extended care setting. Sleep Health, 2(4), 297–308. https://doi.org/10.1016/j.sleh.2016.09.002
Michel, J. S., & Clark, M. A. (2013). Investigating the relative importance of individual differences on the work–family interface and the moderating role of boundary preference for segmentation. Stress and Health, 29(4), 324–336. https://doi.org/10.1002/smi.2474
Namayandeh, H., Yaacob, S. N., & Juhari, R. (2010). The influences of work support and family support on work-family conflict (W-FC) among married female nurses in Shiraz-Iran. Journal of American Science, 6(12), 534–540
O’Mera, B. K. (2017). Interaction of social support and core self-evaluations on work-family conflict and burnout. Purdue university. ProQuest Dissertations Publishing. 10270942
Odle-Dusseau, H. N., Hammer, L. B., Crain, T. L., & Bodner, T. E. (2016). The influence of family-supportive supervisor training on employee job performance and attitudes: An organizational work–family intervention. Journal of Occupational Health Psychology, 21(3), 296. https://doi.org/10.1037/a0039961
Pluut, H., Ilies, R., Curşeu, P. L., & Liu, Y. (2018). Social support at work and at home: Dual-buffering effects in the work-family conflict process. Organizational Behavior and Human Decision Processes, 146, 1–13. https://doi.org/10.1016/j.obhdp.2018.02.001
Poms, L. W., Fleming, L. C., & Jacobsen, K. H. (2016). Work–family conflict, stress, and physical and mental health: a model for understanding barriers to and opportunities for women’s well-being at home and in the workplace. World Medical & Health Policy, 8(4), 444–457. https://doi.org/10.1002/wmh3.211
Pourmeidani, S., Noori, A., & Shafti, A. (2014). Relationship between life style and marital satisfaction. Journal of Family Research, 10(3), 331–344
Powell, G. N., Francesco, A. M., & Ling, Y. (2009). Toward culture-sensitive theories of the work–family interface. Journal of Organizational Behavior, 30(5), 597–616. https://doi.org/10.1002/job.568
Rathi, N., & Barath, M. (2013). Work-family conflict and job and family satisfaction: Moderating effect of social support among police personnel. Equality, Diversity and Inclusion: An International Journal, 32(4), 438–454. https://doi.org/10.1108/EDI-10-2012-0092
Ribeiro, R. M., Bragiola, J. V. B., Eid, L. P., Ribeiro, R. C. H. M., Sequeira, C. A. C., & Pompeo, D. A. (2020). Impact of an intervention through Facebook to strengthen self-esteem in nursing students. Revista Latino-Americana de Enfermagem, 28. https://doi.org/10.1590/1518-8345.3215.3237
Rudolph, C. W., Allan, B., Clark, M., Hertel, G., Hirschi, A., Kunze, F. … Zacher, H. (2021). Pandemics: Implications for research and practice in industrial and organizational psychology. Industrial and Organizational Psychology, 14(1–2), 1–35. https://doi.org/10.1017/iop.2020.48
Selvarajan, T., Cloninger, P. A., & Singh, B. (2013). Social support and work–family conflict: A test of an indirect effects model. Journal of Vocational Behavior, 83(3), 486–499. https://doi.org/10.1016/j.jvb.2013.07.004
Shakeri, M., Bafrooie, K. B., & Panahi, K. (2021). The effectiveness of training stress coping skills on work-life balance of the staff of Education Department in Yazd Province. The Journal of Tolooebehdasht
St-Onge, S., Haines, V. Y., III., Ballesteros-Leiva, F., & Poilpot-Rocaboy, G. (2020). Core self-evaluations, social support and life-domain conflicts. Personnel Review. https://doi.org/10.1108/PR-03-2020-0146
Wang, H., & Li, Y. (2019). Role overload and Chinese nurses’ satisfaction with work-family balance: The role of negative emotions and core self-evaluations. Current Psychology, 1–11. https://doi.org/10.1007/s12144-019-00494-5
Wattoo, M. A., Zhao, S., & Xi, M. (2018). Perceived organizational support and employee well-being: Testing the mediatory role of work–family facilitation and work–family conflict. Chinese Management Studies, 12(2), 469–484. https://doi.org/10.1108/CMS-07-2017-0211
Yang, T., Lei, R., Jin, X., Li, Y., Sun, Y., & Deng, J. (2019). Supervisor support, coworker support and presenteeism among healthcare workers in China: The mediating role of distributive justice. International Journal of Environmental Research and Public Health, 16(5), 817. https://doi.org/10.3390/ijerph16050817
Zarei, S., & Kazemipour, A. (2020). Effect of training work-family conflict management on increasing the quality of work life among the female employees of hospital. Journal of Occupational Hygiene Engineering Volume, 6(4), 34–40
Acknowledgements
This article was extracted from the Ph.D. thesis in Health Education and Health Promotion. It was financially supported by the Vice-Chancellor for Research, Shiraz University of Medical Sciences in Shiraz, Iran (research project no. 8-01-04-20316). We are grateful to the company directors, employees and their spouses who agreed to participate in the program.
Funding
This study was supported by Shiraz University of Medical Science.
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript. Farzaneh Noroozi, and Leila Ghahremani contributed to the Conceptualization. Farzaneh Noroozi Writing – original draft and Collection and assembly of data. Razieh Bagherzadeh contributed to the Formal analysis, review & editing. Rosanna Cousins contributed to the Methodology and Writing – review & editing. Leila Ghahremani contributed to Project administration, review & editing. Mahin Nazari contributed to review & editing.
Corresponding author
Ethics declarations
Consent to Participate
Written informed consent were obtained from the working women who acted as participants. Verbal informed consent was obtained from each participant’s spouse, co-workers, and officials of healthcare centers.
Competing Interest
Th authors declare that they have no competing interests.
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Ethical certification was received from the ethics committee of Shiraz University of Medical Sciences (IR.SUMS.REC.1398.1282). (IRCT code: 201310140150N20).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Noroozi, F., Bagherzadeh, R., Cousins, R. et al. Alleviating work-family conflict for female employees in Iran: The effect of a multimedia educational intervention. Curr Psychol 42, 18832–18845 (2023). https://doi.org/10.1007/s12144-022-03068-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-03068-0