
Abstract
The World Health Organization predicted that depression will become the second greatest disease burden after coronary heart disease by 2020. However, there are few quantitative studies on the spatial relationship between environmental factors and characteristics of patients with depression. In this paper, mathematical statistics, geographical information system and regression methods were used to conduct a quantitative analysis of the individual attributes of hospitalized patients with depression in a Class 3A hospital in Shanghai from 2013 to 2019 and to explore the relationship between individual attributes and circumjacent environmental factors. The results show that (1) the total number of patients with depression has increased in recent years, and the proportion of women was increased 2.5-fold compared with that of men. The risk was significantly increased in middle-aged and young adults aged 45–69 years compared with other age groups. The average hospitalization time was 20–30 days. The lower the level of education, the greater the risk of depression. (2) Within a certain spatial range, the closer to city parks and coffee shops, the lower the distribution density of depressed patients. (3) Medical insurance for patients with depression needs to implement a “people-oriented” differentiation policy. (4) Expanding urban public space, improving urban leisure and entertainment infrastructure, and introducing coffee shops into large-scale residential communities are three important strategies to prevent and treat depression.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Depression is a common mental disorder mainly manifested by sustained negative affect and anhedonia. Depression has become one of the most serious psychiatric diseases affecting human health in modern and stressful social environments (Bongiorno, 2012; Drysdale et al., 2017; Katon et al., 2002; Mathers & Loncar, 2006; Watzke et al., 2020). Depression and Other Common Mental Disorders reports that greater than 300 million individuals suffered from depression worldwide, and the average incidence rate was approximately 6.66% in 2019 (https://app.mhpss.net). Depression affects 20 million people in the US, and approximately 10% of American adults are projected to have depression with a prevalence of 7:100 males and 12:100 females. Depression is one of the largest and costliest medical health problems in the United States, accounting for > US$46.5 billion in total costs annually (Bongiorno, 2012; Quilala, 2017). In China in 2009, 4.2% of the total population (approximately 54 million people) experienced depression. In addition, depression leads to an annual economic burden of greater than 51.37 billion Chinese yuan (https://app.mhpss.net). By 2030, depression will become a major global public health issue and the leading cause of death globally, causing a significant negative effect on productivity.
In recent years, many cities, such as Shanghai and Shenzhen, have advocated for the inclusion of depression and psychosis in universal health coverage (UHC), aiming to increase affordability for patients. Drug therapy and psychological interventions represent key defenses for preventing suicide and have been studied extensively (Hasin et al., 2005; Weinberger et al., 2018). Although substantial progress has been made in the pharmacology and psychotherapy fields of depression, most patients do not receive the correct treatment in a timely manner due to many factors, such as stigma (Riolo et al., 2005; Whiteford et al., 2013). With considerable attention given to mental illnesses, especially major depression, research on depression has been increasingly performed. An increasing number of studies suggest that depression prevalence has increased progressively over time and that individual attributes vary significantly among patients with depression (Hidaka, 2012). In terms of gender, depression affects more women than men (Kuehner, 2017); patients with multiple chronic diseases have a higher prevalence of depression (Altun & Yazici, 2015), and the prevalence of depression in middle-aged individuals was increased compared with that in younger people (Pratt & Brody, 2014). Regarding influencing factors, harmonious family relationships, social support and the amount of financial assets owned by the elderly are inversely associated with the prevalence of depression (Horita & Otsuka, 2014; Jin, 2019; Koizumi, 2005; Ma et al., 2020).
Scholars generally believe that several factors are related to depression, mainly including age, gender, genetic factors, personal factors, and family and social factors (Bongiorno, 2012; Altun & Yazici, 2015; Pratt & Brody, 2014; Wang, 2020; Su, 2019; Ji et al., 2020). Additionally, some interesting phenomena are also present from the perspective of spatial patterns. As scholars have noted, greening urban space can improve the mental health of surrounding residents and alleviate negative emotions, such as depression (Zhu et al., 2019). In addition, coffee has a preventive effect against depression (Guo et al., 2014; Kim & Kim, 2018; Kimura et al., 2020).
Caffeine intake was negatively correlated with depression and depressive symptoms and may prevent depressive symptoms, which has been verified in studies conducted by researchers in the United States (Guo et al., 2014), South Korea (Kim & Kim, 2018) and Japan (Kimura et al., 2020). Coffee is a major contributor to dietary caffeine among adults. Appropriate physical activity not only obviously alleviates symptoms of depression and ameliorates anxiety but also improves quality of life (Kvam et al., 2016). Additionally, access to green spaces and proximity to parks are linked to positive health outcomes for urban residents, including reduced risk of cardiovascular disease and diabetes and less stress (Orstad et al., 2020). Urban parks offer opportunities for improving physical health and contact with nature, which can reduce loneliness and improve psychological well-being (Kowitt et al., 2020).
Notably, most of the previous studies regarding factors associated with depression presented qualitative analysis results of internal environmental factors, such as individual attributes and family relationships, whereas relatively little attention has been given to the external environmental factors around residential areas.
For instance, urban green space and infrastructure construction can impact surrounding residents’ psychological health. Therefore, this paper attempts to present a quantitative analysis of the external environmental factors in patients with depression. Additionally, the spatial epidemiology approach of integrating geographical information system (GIS) analysis and data mining methods contrasts with traditional methods of pathology and clinical research, which links incidence data, geographical data and spatial information to discover the spatial characteristics affecting the occurrence of diseases in a more intuitive and simplified manner.
The remainder of the study is arranged as follows. Section 2 describes materials and methods. Section 3 presents the attribute characteristics of patients with depression. Section 4 investigated the relationship between the surrounding environmental factors and the distribution density of depression patients. The discussion is given in Section 5. Finally, the conclusions and recommendations are given in Section 6.
Materials and Methods
Data Sources
As a typical city in China, Shanghai represents the direction of economic and healthy development in China. Shanghai had approximately 24.87 million resident population (China seventh national census, 2020) and included 16 districts of which 7 districts in the downtown and 9 in the suburbs (Fig. 1). Besides, the Shanghai Municipal Health Commission Annual Data Report indicated that shanghai had 387 hospitals, 105 beds and 53 doctors per 10, 000 population in 2019.

Study area and sample X hospital
This study was approved by the Shanghai Medical Insurance Association and a Class 3A hospital in Shanghai and complied with all relevant ethical regulations. Patient data were obtained retrospectively from the hospital registry data. The psychiatric discipline of this hospital is a characteristic discipline in Shanghai. The hospital is one of only two training bases for psychiatric specialists in Shanghai and professional departments with national qualifications for clinical trials of psychotropic drugs. Thus, as the research objects in this study, patients with depression in this hospital can represent the overall situation of patients with depression in Shanghai to some extent. Hospital inpatients with depression data, including age, sex, street address, length of stay, and hospitalization expenses, from 2013 to 2019 were acquired from the hospital information system. Point of interest (POI) data mainly reflect the macroscopic distribution of geographic datasets. Spatial location data of urban parks and coffee shops were obtained from the points of interest (POIs) of Baidu Maps in 2019. Figure 1 shows the study area and hospital X which is located in the Putuo district of Shanghai.
Methods
The present paper aims to quantitatively investigate the relationship between geospatial factors and depression. To accomplish this goal, a combination of mathematical statistics, kernel density estimation, Euclidean distance and linear regression were applied.
-
(1)
Kernel density estimation (KDE) is widely used in spatial clustering analysis of point data, which reflects the relative concentration degree of the spatial point distribution. We used KDE to analyze the spatial distribution of hospitalized patients with depression (Wang, 2020;Okabe et al., 2009). The points falling into the search area have different weights. Points near the center of the search area are given higher weights. As the distance increases, the weight value will decrease (Shi et al., 2021). The kernel density function f(x) at spatial position x can be calculated as follows:
In Formula (1), r is the distance attenuation threshold; n is the number of points that are less than or equal to r from position x; and the k function represents the spatial weight function.
-
(2)
The Euclidean distance (ED) calculates the distance between each pixel and the nearest source and is a commonly used definition of distance. ED is the true distance between two points in m-dimensional space. The calculation is presented in the following equation:
where x1 and y1 are the coordinate values of the pixels to be measured; x2 and y2 are the coordinate values corresponding to the target pixel; and D is the shortest straight-line distance between the selected pixel and the nearest pixel.
-
(3)
Univariate linear regression analysis was selected to determine the coefficients of relationships between the density of depressed patients and ED from city parks and coffee shops to identify the influence of urban spatial facilities on the incidence of depression. The model was established as follows:
where a and b are the parameters to be solved; yi is the kernel density value of depression; and xi is the ED between the city park and the coffee shop.
Attribute Characteristics of Hospitalized Patients with Depression
In this paper, a total of 1735 inpatient records were selected from 2013 to 2019. Each appearance of an inpatient constitutes one visit record in the raw data. Each record contains inpatients name, age, gender, education background, address, hospitalization frequency and hospitalization expenses. Therefore, the records should be properly preprocessed and excluded according to various attribute characteristics. For example, male patient Tom who has multiple hospitalizations in one year, it can only be counted as one male record in gender statistics. Following the plenary discussion, to avoid double-counting, we designed the excluded rules as follows: for patients with multiple hospital admissions, we counted only one sex, one age, one education background and one duplication by excluding the previous records and retaining only the latest record of each patient in a year. With respect to the hospitalization frequency and expenses, we opted to make no adjustments on original recordings.
Gender Characteristics
A total of 1440 records were kept in the gender statistics. In general, the number of patients with depression has experienced periods of growth during 2013–2019 in a Class 3A hospital in Shanghai (Fig. 2) with approximately 77.7% growth over the past 7 years. In fact, the number of female patients with depression grew 78.4% from 111 to 198 persons. The number of male patients with depression grew 86% from 43 to 80 persons, whereas the number of female patients was approximately 2.5 times that of men in Shanghai. According to the demographic data in Shanghai Statistical Yearbook 2019, the male to female sex ratio is 1:1.02 in Shanghai, demonstrating that women in Shanghai are more likely to suffer from depression.

The number and proportion of hospitalized patients with depression in X Hospital from 2013 to 2019
Age Distribution
The age of depression patients is classified into 6 classes, i.e., young people under 30 years old, young-middle aged 30–44 years, middle-aged between 45 and 59, young-elderly between 60 and 69, middle-elderly between 70 and 79 and elderly people over 80 years old. In both males and females, depression occurs more frequently in young-middle and young-elderly patients in the age range of 45–69 years (Fig. 3), and a low proportion of depression is noted among in young and elderly people.

The proportion of hospitalized patients with depression based on different age groups and gender in X Hospital from 2013 to 2019
Education Background Distribution
The available data sets can be broadly divided into three categories: ‘junior college degree and above’ (27.18%), ‘primary education and below’ (12.46%) and ‘secondary and technical secondary education’ (60.36%). Among patients with a junior college degree and above, patients with undergraduate education had the highest probability (approximately 15%) of having depression, patients with master’s education had the second highest probability (1.07%), and patients with doctoral education had the lowest probability (0.13%). Among patients with junior college degrees and below, patients with secondary education represent the greatest proportion (approximately 55%) of subjects with depression. Overall, research has shown a higher probability of depression in individuals with lower levels of education (Fig. 4).

Educational distribution of hospitalized patients with depression in X Hospital
Statistics of Hospitalization Frequency
Statistical analysis of the medical records of 1735 patients with depression revealed that 952 patients with depression were admitted for the first time, accounting for 54.87% of the total inpatients with depression. Depression patients who were hospitalized 2–10 times accounted for 37.52% of the total depression patients, and 7.61% of patients with depression were hospitalized more than 10 times (Fig. 5).

Statistics on the admission frequency of depression patients in X Hospital
Composition of Average Hospitalization Expenses
After the medical records acquisition step, the medical expenses of patients with depression comprise seven diverse, including the treatment category, diagnosis category, comprehensive medical service category, consumable category, traditional Chinese medicine category, nursing category and Western medicine category. Regarding hospitalization expenses for depression, the treatment and diagnosis expenses are the two highest costs among all items in each year, whereas the proportion of pharmaceutical expenses gradually decreases, indicating that timely and scientific consultation and treatment and a direct treatment path for depression are important measures to reduce the cost of treatment for depression. In addition, a significant reduction in drug costs occurred in 2016 that was related to the efforts of relevant departments to control drug costs. In 2017, medicine markups were cancelled in the comprehensive reform of public hospitals, which produced obvious effects on drug costs. In addition, the proportion of nursing expenses is at a low level, but a gradual increasing trend is noted. Based on public attention to depression in recent years, clinical nursing has become increasingly important. In summary, nursing care should be provided to depressed patients to provide psychological relief, drug advice and safety. In addition, the cost of consumables is less than 1% because depression is a psychological disease and does not require surgical treatment (Fig. 6).

The cost structure and its changes in patients with depression discharged from X Hospital from 2013 to 2019
Patterns of Spatial Association of Patients with Depression and Surrounding Environmental Factors
Urban parks represent green spaces, and these studies focus on the spatial relationship between the natural environment and patients with depression. Coffee shops represent social spaces, and these studies focus on the spatial relationship between the human environment and patients with depression.
Spatial analysis requires accurate patient addresses. Thus, sample points with multiple visits and unclear addresses were excluded, and a total of 900 valid sample data points were finally obtained. The analysis results show as the distance from the hospital increased, the area contained in the spatial range increases exponentially. However, the number of samples corresponding to patients gradually decreases as the area increases (Table 1, Fig. 7). Considering that the principle of nearby treatment of patients in hospitals has a significant influence on the spatial distribution of cases, an appropriate range was selected as the study area based on factors, such as sample points and hospital service coverage area. As a result, the study area was obtained by setting 10 km as the buffer radius centered on X Hospital. In total, 681 sample points were noted in the study area, accounting for 75.67% of the total area of Shanghai (Table 1).

Schematic diagram of sample points graded by distance
Spatial Distribution Relationship between Urban Parks and Depressed Patients
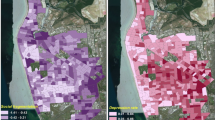
The spatial distribution density of depression patients was obtained by kernel density analysis. The greater the density, the greater the number of patients diagnosed at this point in spatial distribution. The results showed that the spatial distribution of depression inpatients in Shanghai presented a block-like clustering pattern with “one main and many secondary” (Fig. 8).

Kernel density distribution in patients with depression
First, we used resampling to obtain the distance value and kernel density value at the location of the sampling point by ArcGIS. The sampling density was 200 m *200 m. The sampled density value served as the Y-axis, and the distance value served as the X-axis to generate a scatter plot. When the distance from the park is greater than 2000 m, the data are highly discrete. Thus, data within 2000 m were selected for analysis. The linear regression results between the distance to park and density of depressed patients are presented in Fig. 9.

Linear regression results between the density of depressed patients and the distance from urban parks
Remarkably, a positive correlation between the density of depressed patients and park distance within 2 km was established with a goodness of fit (GOF) parameter of 0.63, equation y = 0.0003x + 1.9735 and correlation coefficient of 0.7928. In Fig. 9, we can observe that the density of patients increased with increasing distance from the park within 10 km of the hospital buffer zone and 2 km from the park. Thus, the farther the distance from the park, the higher the distribution density of patients with depression, indicating that urban parks have a soothing effect on patients with depression. This finding is consistent with the research results of Kvam et al., who found that “greening urban open space can improve the mental health of surrounding residents and alleviate negative emotions, such as depression” (Kvam et al., 2016).
Spatial Distribution Relationship between Coffee Shops and Depressed Patients
Using the same approach, when the distance from the coffee shop is greater than 1500 m, the data are highly discrete. Thus, we select the data within 1500 m for coffee shop analysis. The linear regression results between the distance to coffee shops and the density of depressed patients are shown in Fig. 10.

Linear regression results between the density of depressed patients and the distance from coffee shops
The results reveal a well-established positive association between depressed patients and the distance from coffee shops within 1500 m with a GOF parameter of 0.79, equation y = 0.0012x + 1.6491 and correlation coefficient of 0.89. Moreover, as the distance from coffee shops increases, the density of patients with depression becomes increasingly high. Overall, these results further indicate that coffee shops may be an important factor mitigating depression to a limited extent.
Discussion
The goal of current study was to examine characteristics of hospitalized patients with depression and their relationship with the surrounding environment. With respect to gender, it is worth noting that more women than men report depression in the present study, which is in accordance with many previous studies (Hasin et al., 2005; Pratt & Brody, 2014; Williams et al., 2007). We found that both women and men demonstrate increasing depression prevalences over time with no differences in the rate of increase by gender. Weinberger et al. (2018) found that the female: male was 2:1 in USA, which may vary with our conclusion 2.5:1. This is because our data are only hospitalization patients and do not include outpatient records. There are also noticeable differences in terms of age and education distribution. Like our research on age distribution, Pratt and Brody (2014) found that younger and older adults report lower prevalences of depression than middle age groups. However, Weinberger et al. (2018) came to a different conclusion on education distribution. They concluded that the rates of increase in depression did not significantly differ by income or education among those in the highest education groups (some college or college degree and above). Our findings suggest that nearly half (45%) of depression patients have revisited the hospital in Shanghai. Another research was also done in Beijing (Han et al., 2021). They concluded that hospitalization days per year decreased for patients in the short stay and repeated long stay clusters, which is different from this study. It is necessary to take in account local contexts to interpret the data and evidence. From the expenses perspective, National US spent $22.8 billion on treatment for depression (Wu et al., 2016). Although the total cost is important for depression, few studies have described the composition of expenses. In this study, the cost composition is analyzed in detail, which discovered that treatment and diagnosis category are the most expensive items.
The positive relationship between urban park distance and density of depression also confirms the importance of the urban public space. The results indicate that within a certain distance, closer to the park, the lower the risk of depression appear. Again, Lin et al. (2017) found that distance to and the accessibility of parks was a key condition for park use among individuals and pocket parks play important roles in shaping the city. On one hand, people who live close to a park are more likely to exercise than those who do not. On the other hand, closer to parks represents more vegetation that could improve air quality (Du et al., 2021). Interestingly, the prevalence of depression in frequent coffee drinkers was 32% lower than in coffee non-drinkers (Kim & Kim, 2018). Similarly, significantly positive correlation between density of depression and the distance from coffee shops indicates that the low depression density still benefit from coffee shops.
Ultimately, the results of the present study should be interpreted with some caution because of limitations. Spatial accessibility to healthcare facilities is an equitability index measuring the evenness of public service facilities and has drawn much attention in recent years. For example, Yang et al. (2020) found significant inequality of spatial accessibility to healthcare facilities in Shanghai, with Huangpu, southern Jing ‘an and northern of Xuhui district showed higher traffic accessibility. However, this study did not consider transportation modes of residents and just chose surrounding infrastructures within a fixed radius buffer. Furthermore, we only focused on urban parks and coffee shops, the two public service facilities. Over the following research, we will plan incorporate road network, and more surrounding facilities such as bars into our dataset so we can adapt our explanation model to be more comprehensive and accurate. Despite these limitations, this study’s findings provided important implications for health professionals and policy makers.
Conclusions and Recommendations
Studies that considered the spatial effect of the surrounding environment on patients with depression in cities are lacking. In this paper, the medical records of hospitalized patients with depression were used for spatiotemporal analysis. The results showed that the incidence of depression had obvious gender and age characteristics, and the hospital costs also varied and fluctuated by category. In terms of gender, females had an approximately 2.5-fold greater risk of suffering depression in Shanghai compared to males. Men and women aged 45–69 years who are classified as middle-aged and young-old individuals were overrepresented in this data set compared to young people under 30 and oldest old people over 80 from 2013 to 2019. In addition, our study demonstrated that urban parks (a type of open space) and coffee shops (a type of social and cultural space) are spatially correlated with the density of patients with depression. Specifically, within the 2-km range, the density of depressed patients decreases, whereas the distance from the park increases. The farther the distance from the coffee shops, the higher the distribution density of depressed patients at 1.5 km.
Therefore, there are three urgent tasks for the prevention and treatment of depression apart from strengthening public mental health education and encouraging patients with depression to actively seek medical treatment. Several key recommendations emerged.
First, additional work will be needed to further improve the “people-oriented” medical insurance policy. For example, the reimbursement rate of medical expenses for female patients with depression should be increased as appropriate. As aforementioned, With regard to gender, more women report depression than men. In addition, the reimbursement rate of medical expenses should be appropriately increased for patients with long-term severe depression and patients with multiple chronic diseases (Rubio et al., 2011).
Second, the urban government and department of land space planning and administration should further expand the urban public space and provide a well-established urban leisure and entertainment infrastructure. In densely populated urban residential areas, the current planning goal is that residents can see a large park 500 m away. However, we believe that by 2025, residents should see small and medium parks within 350 m and small parks or “pocket parks” within 250 m by 2030.
Third, it should be noted that coffee shops should be introduced to large-scale urban residential areas. The existing coffee shops are mainly located in business districts, and the primary target populations are the middle- and high-income groups with higher education, especially young adults who seek fashionable trends (Shi & Yang, 2018). However, patients with depression were more likely to be middle-aged and young-old people in the age range of 45–69 years old who had poorer access to coffee services. Consequently, the introduction of coffee shops into large residential communities is conducive to moderately promoting coffee consumption in middle-aged and elderly people.
Data Availability
The data used in the research cannot be shared with any person because of the ethical concerns relating to confidentiality and anonymity of the patients. The datasets used in the research cannot be publicly shared but are available upon reasonable request.
References
Altun, F., & Yazici, H. (2015). The relationships between life satisfaction, gender, social security, and depressive symptoms among elderly in Turkey. Educational Gerontology, 41(4), 305–314.
Bongiorno, P. (2012). How come They’re happy and I’m not? The complete natural medicine program for healing depression for good. Conari Press.
Drysdale, A. T., Grosenick, L., Downar, J., Dunlop, K., Mansouri, F., Meng, Y., Fetcho, R. N., Zebley, B., Oathes, D. J., Etkin, A., Schatzberg, A. F., Sudheimer, K., Keller, J., Mayberg, H. S., Gunning, F. M., Alexopoulos, G. S., Fox, M. D., Pascual-Leone, A., Voss, H. U., Casey, B. J., Dubin, M. J., & Liston, C. (2017). Resting-state connectivity biomarkers define neurophysiological subtypes of depression. Nature Medicine, 23(1), 28–38.
Du, H., Zhou, F., Cai, Y., et al. (2021). Research on public health and well-being associated to the vegetation configuration of urban green space, a case study of Shanghai, China. Urban Forestry & Urban Greening, 59(6), 126990.
Guo, X., Park, Y., Freedman, N. D., Freedman, N. D., Sinha, R., Hollenbeck, A. R., Blair, A., & Chen, H. (2014). Sweetened beverages, coffee, and tea and depression risk among older US adults. PLoS One, 9(4), e94715.
Han, X., Jiang, F., Needleman, J., et al. (2021). A sequence analysis of hospitalization patterns and service utilization in patients with major psychiatric disorders in China. BMC Psychiatry, 21(1), 1–12.
Hasin, D. S., Goodwin, R. D., Stinson, F. S., & Grant, B. F. (2005). Epidemiology of major depressive disorder: Results from the national epidemiologic survey on alcoholism and related conditions. Archives of General Psychiatry, 62(10), 1097–1106.
Hidaka, B. H. (2012). Depression as a disease of modernity: Explanations for increasing prevalence. Journal of Affective Disorders, 140(3), 205–214.
Horita, Y., & Otsuka, Y. (2014). Relationships between workers' interpersonal helping behavior, social supports, job stressors, psychological stress responses, and vigor in manufacturing industry. Sangyō eiseigaku zasshi =. Journal of Occupational Health, 56(6), 259–267.
Ji, H., Du, L., Zhu, X., et al. (2020). Depression and its influence factors in the elderly with chronic disease in China. Modern Preventive Medicine, 47(16), 3002–3006 (In Chinese).
Jin, Y. (2019). The relationship between physical frailty and depressive symphoms: The mediating and moderating role of social support. Shandong University (In Chinese of Master Thesis).
Katon, W., Russo, J., Von Korff, M., Lin, E., Simon, G., Bush, T., Ludman, E., & Walker, E. (2002). Long-term effects of a collaborative care intervention in persistently depressed primary care patients. Journal of General Internal Medicine, 17(10), 741–748.
Kim, J., & Kim, J. (2018). Green tea, coffee, and caffeine consumption are inversely associated with self-report lifetime depression in the Korean population. Nutrients, 10(9), 1201.
Kimura, Y., Suga, H., Kobayashi, S., Sasaki, S., & the Three-Generation Study of Women on Diets and Health Study Group. (2020). Intake of coffee associated with decreased depressive symptoms among elderly Japanese women: A multi-center cross-sectional study. Journal of Epidemiology, 30(8), 338–344.
Koizumi, Y. (2005). Association between social support and depression status in the elderly: Results of a 1-year community-based prospective cohort study in Japan. Psychiatry and Clinical Neurosciences, 59(5), 563–569.
Kowitt, S. D., Aiello, A. E., Callahan, L. F., Fisher, E. B., Gottfredson, N. C., Jordan, J. M., & Muessig, K. E. (2020). Associations among neighborhood poverty, perceived neighborhood environment, and depressed mood are mediated by physical activity, perceived individual control, and loneliness. Health & Place, 62, 102278.
Kuehner, C. (2017). Why is depression more common among women than among men? The Lancet Psychiatry, 4(2), 146–158.
Kvam, S., Kleppe, C. L., Nordhus, I. H., & Hovland, A. (2016). Exercise as a treatment for depression: A meta-analysis. Journal of Affective Disorders, 202, 67–86.
Lin, P., Lau, S., Qin, H., et al. (2017). Effects of urban planning indicators on urban heat island: A case study of pocket parks in high-rise high-density environment. Landscape and Urban Planning, 168, 48–60.
Ma, J., Zhang, S., Liu, W., et al. (2020). Prevalence and associated factors of depression and anxiety in elderly patients with mild cognitive impairment in community: A cross-sectional study. Chinese General Practice, 23(33), 4246–4251 (In Chinese).
Mathers, C. D., & Loncar, D. (2006). Projections of global mortality and burden of disease from 2002 to 2030. PLoS Medicine, 3(11), e442.
Okabe, A., Satoh, T., & Sugihara, K. (2009). A kernel density estimation method for networks, its computational method and a GIS-based tool. International Journal of Geographical Information Science, 23(1), 7–32.
Orstad, S. L., Szuhany, K., Tamura, K., et al. (2020). Park proximity and use for physical activity among urban residents: Associations with mental health. International Journal of Environmental Research and Public Health, 17, 1–13.
Pratt, L. A., & Brody, D. J. (2014). Depression in the U.S. household population, 2009-2012. NCHS Data Brief, 172, 1–8.
Quilala, M. (2017) Depression and other common mental disorders: Global health estimates. https://app.mhpss.net/resource/depression-and-other-common-mental-disorders-global-health-estimates, (Online accessed: December18, 2020).
Riolo, S. A., Nguyen, T. A., Greden, J. F., et al. (2005). Prevalence of depression by race/ethnicity: findings from the National Health and Nutrition Examination Survey III. American Journal of Public Health, 95(6), 998–1000.
Rubio, J. M., Markowitz, J. C., Alegría, A., Pérez-Fuentes, G., Liu, S. M., Lin, K. H., & Blanco, C. (2011). Epidemiology of chronic and nonchronic major depressive disorder: Results from the national epidemiologic survey on alcohol and related conditions. Depression and Anxiety, 28(8), 622–631.
Shi, Y., & Yang, F. (2018). Features of spatial distribution and impacting factors of Starbucks in Shanghai. Economic Geography, 38(5), 126–132 (In Chinese).
Shi, Y., Tao, T., Cao, X., & Pei, X. (2021). The association between spatial attributes and neighborhood characteristics based on Meituan take-out data: Evidence from shanghai business circles. Journal of Retailing and Consumer Services, 58, 102302.
Su, Y. (2019). Analysis of depression and its influencing factors in middle and old people: An empirical study based on 2015 CHARLS. Liaoning University (In Chinese of Master Thesis).
Wang, Q. (2020). Research on the influence of social support on depression in the elderly--based on China family panel studies data in 2016. Shandong University (In Chinese of Master Thesis).
Watzke, B., Heddaeus, D., Steinmann, M., Daubmann, A., Wegscheider, K., & Härter, M. (2020). Does symptom severity matter in stepped and collaborative care for depression? Journal of Affective Disorders, 277, 287–295.
Weinberger, A. H., Gbedemah, M., Martinez, A. M., Nash, D., Galea, S., & Goodwin, R. D. (2018). Trends in depression prevalence in the USA from 2005 to 2015: Widening disparities in vulnerable groups. Psychological Medicine, 48(8), 1308–1315.
Whiteford, H. A., Harris, M. G., McKeon, G., Baxter, A., Pennell, C., Barendregt, J. J., & Wang, J. (2013). Estimating remission from untreated major depression: A systematic review and meta-analysis. Psychological Medicine, 43(8), 1569–1585.
Williams, D. R., González, H. M., Neighbors, H., Nesse, R., Abelson, J. M., Sweetman, J., & Jackson, J. S. (2007). Prevalence and distribution of major depressive disorder in African Americans, Caribbean blacks, and non-Hispanic whites: Results from the National Survey of American life. Archives of General Psychiatry, 64(3), 305–315.
Wu, J., Davis-Ajami, M. L., & Kevin Lu, Z. (2016). Impact of depression on health and medical care utilization and expenses in US adults with migraine: A retrospective cross sectional study. Headache: The Journal of Head and Face Pain, 56(7), 1147–1160.
Yang, W., Chen, N., Wang, H., et al. (2020). On the accessibility of medical facilities in the central area of Shanghai using improved 2SFCA. Geomatics World, 27(6), 75–79 (In Chinese).
Zhu, X., Fang, H. Q., Zhang, L. S., et al. (2019). Research progress on the health effects of coffee. Chinese Journal of Food Hygiene, 31(1), 93–98 (In Chinese).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflicts of interest.
Ethical Statement
Ethical approval for the study was obtained prior to this study from Shanghai Medical Insurance Association (No.YBXH-KT201901). All participants provided written informed consent.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tao, T., Shi, Y., Yang, Q. et al. Characteristics of hospitalized patients with depression and their relationship with the surrounding environment: A study in a class 3A hospital in Shanghai. Curr Psychol 42, 5910–5921 (2023). https://doi.org/10.1007/s12144-021-01940-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-021-01940-z