
Abstract
The main objective of this study was to examine the use of protection motivation theory (PMT) in explaining smokers’ quitting intentions among Chinese adults with the goal of providing valuable evidence to promote theory-guided and culturally appropriate cessation interventions. This cross-sectional study included 613 participants randomly selected from 26 provinces in Mainland China. Cronbach’s alpha and interclass correlation coefficients (ICC) were used to assess the reliability of individual PMT constructs. A multiple linear regression was used for the multivariable analysis. Cronbach’s alpha coefficient of the 23 items was 0.74. Cronbach’s alpha coefficient of all the subscales varied from 0.71 to 0.74. Stronger quitting intentions were significantly associated with higher perceived vulnerability (Coef. = 0.13, P < 0.01), self-efficacy (Coef. = 0.28, P < 0.01), and response efficacy (Coef. = 0.23, P < 0.01) but inversely associated with intrinsic rewards (Coef. = −0.15, P < 0.01). Greater quitting intentions were significantly associated with higher threat (Coef. = 0.19, P < 0.01) and coping appraisals (Coef. = 0.25, P < 0.01). Regarding behaviour, longer quitting attempts were significantly associated only with self-efficacy (Coef. = 0.13, P < 0.01) and response cost (Coef. = −0.18, P < 0.01) Our results confirmed the applicability of PMT for predicting the quitting intention in Chinese adults. Self-efficacy is the only factor that has a predictive effect on both the intention and behaviour. To improve the effectiveness of smoking-cessation interventions, specific attention should be directed during their design to the more influential PMT constructs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The tobacco epidemic is one of the biggest public health threats China has ever faced, as tobacco use causes more than one million deaths in China each year (Lin, Chun, Zhao, et al., 2019a). Although many smoking-cessation programmes have been implemented, researchers have found limited success in reducing smoking rates (China Disease Control and Prevention Center, 2016; China Disease Control and Prevention Center, 2019). According to the Chinese Adult Tobacco Survey, the smoking prevalence among males was 52.9% in 2010 (Yang, Li, Wang, et al., 2010), 52.1% in 2015 (China Disease Control and Prevention Center, 2016), and 50.5% in 2018 (China Disease Control and Prevention Center, 2019). One of the most important reasons for these rates is that most tobacco prevention and smoking-cessation activities are not grounded in or guided by theory. Karen et al. conducted a review and found that health intervention research has largely been implemented in China without a theoretical framework (Macdonell, Chen, Yan, et al., 2013). Yan et al. also found that few studies on smoking prevention in the Chinese population were theory guided. Even in intervention trials based on behavioural change theory, some obvious problems have always rendered the results problematic; for example, no detailed information was provided about how to integrate the theories into specific intervention measures, and no effective information was reported to support the role that the theories played in the intervention or how to contribute to a persistent enhancement of motivation (Yan et al., 2014).
In China, most health educators recognize the importance of integrating behavioural change theory into their routine smoking-cessation activities, but several barriers must be addressed. One is the lack of available measurement scales to evaluate the quitting intention and to further guide intervention activities. Protection motivation theory (PMT) is a well-known theory of behavioural change and is especially useful for addressing smoking behaviour (Lin, Liu, Chang, et al., 2019b; Sabzmakan, Ghasemi, Asghari Jafarabadi, Kamalikhah, & Chaleshgar, 2018).
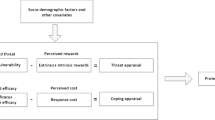
PMT is a systematic theory that states that intention, as the most significant predictor of behaviour, is determined by two appraisal processes: threat and coping (Webb, Sniehotta, & Michie, 2010a). As shown in Figure 1, PMT has seven elements: perceived severity, perceived vulnerability, intrinsic and extrinsic rewards, response efficacy, self-efficacy, and response costs. Greater motivation for specific health behaviours (such as quitting intention) can be expected if the perceived severity and vulnerability are high and rewards are low. Response efficacy and self-efficacy are expected to enhance motivation, whereas response costs are expected to reduce it (Bashirian, Barati, Mohammadi, et al., 2019; Brooks Stephanie, 2020; Malmir, Barati, Khani Jeihooni, Bashirian, & Hazavehei, 2018).

The theoretical framework of protection motivation theory
Evidence Prior to this Study
In recent years, PMT has received some attention in predicting behavioural change and designing interventions. Zahra et al. successfully used PMT to assess fall-protective behaviours among older adults. Patty et al. used PMT to understand how experiencing a fire in an immersive virtual environment motivates prevention behaviour (Brooks & Bubela, 2020; Jansen, Snijders, & Willemsen, 2020; Taheri-Kharameh et al., 2020). One systematic review published in the Journal of Applied Social Psychology found that such a theory is a useful tool in predicting health intentions and concurrent behaviour but has less utility for assessing future behaviour (Milne, Sheeran, & Orbell, 2000).
With regard to smoking behaviour, some studies have been conducted among adolescents based on constructs of PMT, such as that by Johannes et al., who found that only one part of PMT (self-efficacy) had predictive validity in predicting adolescents’ smoking intentions and related behaviours (Thrul, Stemmler, Bühler, & Kuntsche, 2013). Karen et al. found that two of seven PMT factors were significantly correlated with the smoking intention among adolescents (Macdonell et al., 2013). Other researchers found that PMT was an effective conceptual framework for studying tobacco use. This theory can significantly predict smoking behaviour after controlling for covariates (Xu & Chen, 2016). Surprisingly, little research has used PMT to examine adults’ quitting intentions. However, PMT has been widely used in alcohol abstinence programmes. An intervention developed based on PMT has proven effective in strengthening the intention to limit alcohol consumption in a large number of studies (Ben-Ahron, White, & Phillips, 1995; Milne et al., 2000; Stainback & Rogers, 1983).
Theoretical Framework and Hypotheses
PMT proposes that protection motivation relies on a threat appraisal and an assessment of possible options to cope with specific threats (Rogers, 1983). Based on the literature, we identified four psychological determinants that have an important role in influencing individuals’ threat appraisal: perceived severity, perceived susceptibility, and intrinsic and extrinsic rewards. Three determinants are related to coping appraisal: response efficacy, self-efficacy, and response costs. The direction of severity depends on the expected consequence of a behaviour or habit. The vulnerability is the likelihood that a consequence will occur. Significant predictive effects were reported for severity and vulnerability on smoking behaviour in a previous study (Greening, 1997). In addition, some researchers have found that vulnerability is more significantly correlated with subsequent behaviour (Milne et al., 2000). Therefore, we posit our first hypothesis: Severity and vulnerability to smoking-related threats are positively associated with the quitting intention.
Intrinsic and extrinsic rewards and response costs are another dimension of threat appraisal. Intrinsic rewards consist of the perceived positive effect of a behaviour. Extrinsic rewards consist of the perceived positive social reactions or consequences. A study conducted in Iranian adolescents showed that intrinsic rewards had a significant inverse relationship between protection motivation and tobacco use (β = −0.285, P < 0.001) (Sabzmakan et al., 2018). Although a few studies have reported different results for extrinsic rewards when predicting smoking behaviour, most studies have identified a high correlation between extrinsic rewards and intrinsic rewards (covariate coefficient = 0.98) (Macdonell et al., 2013; Sabzmakan et al., 2018; Thrul et al., 2013). Response costs concern beliefs about how costly performing the recommended response will be to the individual and are significantly correlated with subsequent behaviour. However, such associations were small to medium and unstable in a previous study (Abraham Charles, Paschal, Dominic, et al., 1994). Therefore, we posit our second hypothesis: Intrinsic and extrinsic rewards and response costs are negatively associated with the quitting intention.
Self-efficacy is also a potential pathway for motivation. It is the belief in one’s competence to cope with adversity in specific demanding situations. A branch of the literature suggests that self-efficacy plays an important role in determining health behaviour (Schwarzer & Fuchs, 1996; Seyde, Taal, & Wiegman, 1990), as exemplified by a study conducted in Germany that found that self-efficacy was the strongest predictor of a concurrent smoking-related behavioural intention (Thrul et al., 2013).
Another important determinant to taking preventive measures is response efficacy, which assesses the effectiveness of protective behaviour in lessening health threats. Sarah et al. conducted a meta-analytic review and found that response efficacy had a small-to-medium association with concurrent behaviour. The remaining coping appraisal components had medium-to-large associations (Milne et al., 2000). Therefore, we posit our third hypothesis: Response efficacy and self-efficacy are positively associated with the quitting intention.
Overall, the balance between the two appraisal pathways (threat and coping appraisals) determines the likelihood of a risk behaviour. Therefore, we posit our fourth hypothesis: Both coping and threat appraisal variables are significant predictors of the quitting intention.
In addition, many studies have left the relation between psychological determinants and behaviour untested, because effects on behaviour are often difficult or even impossible to measure (Macdonell et al., 2013). We believe it is worthwhile to test psychological determinants and the target behaviour simultaneously. Therefore, we also examined the predictive effect of the quitting intention and PMT constructs on behaviour. Previous studies found that PMT is useful in predicting health-related intentions and concurrent behaviour and have proven the direct association between motivation and behaviour (Milne et al., 2000; Sabzmakan et al., 2018). Therefore, our final hypothesis is that the smoking intention is a sound variable that can predict quitting behaviour.
The main objective of this study was to examine the use of PMT to explain smokers’ quitting intentions among Chinese adults with the goal of providing valuable evidence to promote theory-guided and culturally appropriate cessation interventions. First, we tested the fit of the PMT structure to the population samples. Second, we assessed how well the different constructs of this theory predicted the quitting intention and behaviour.
Methods
Study Design and Participants
This was a cross-sectional study conducted in July and August, 2020. The School of Public Health, Peking University Health Science Centre sent investigators to 26 provinces in Mainland China. Participants were randomly selected on public streets. Data were collected with questionnaires administered in the form of face-to-face interviews. Interviews lasted for approximately 15–20 min for each participant. We recruited participants based on the following criteria: (1) age between 18 and 70 years old; (2) daily smokers with ≥1 year of smoking duration; (3) local residents ≥5 years; and (4) consent to participate in the programme.
This study received ethical review and approval from the Peking University Health Science Centre. Before data collection, the interviewers conducted eligibility confirmation and obtained informed consent. The Peking University Health Science Centre conducted online trainings for all interviewers in three areas: (1) method of obtaining informed consent, i.e., interviewers should introduce the content and purpose of the survey according to specific criteria, obtain verbal informed consent from all participants, and let all the participants know that all statistical analyses would be conducted anonymously and their information would be used for research purposes and published; (2) valuable skills when conducting interviews, such as how to question effectively and how to make participants comfortable; and (3) other skills, such as how to approach more participants, keep themselves safe and deal with problems if participants were unhappy.
Data Collection Procedure
A four-stage method was applied in this survey. In the first stage, experts at Peking University designed the standardized questionnaires. In the second stage, an online survey system was developed, and a unique URL was generated. The self-check function of the online survey system automatically identified missing data, logical errors, and illegal characters. In the third stage, all the investigators input the information through the internet after they completed the face-to-face interviews. In the last stage, the submitted questionnaires were reviewed by staff at Peking University, and the respondents were contacted for clarification if any problems were detected.
Measurements
We used a questionnaire with four sections, as follows:
-
1.
Sociodemographic information—including sex, age, body mass index, marital status, ethnicity, education, yearly income, chronic diseases, and occupation—was assessed in the first section of the questionnaire.
-
2.
Smoking status—including the number of cigarettes per day, smoking duration, withdrawal symptoms, smoking harm awareness, and e-cigarette usage—was assessed in the second section of the questionnaire.
-
3.
Smoking-cessation information—including quitting attempts, quitting methods, and the quitting intention—was assessed in the third section of the questionnaire.
-
4.
The PMT constructs were assessed using the PMT scale, which was based on the work of Xu et al. (Jansen et al., 2020). These measures have previously been shown to have good psychometric properties. We also improved and adjusted some of the questions to make them fit for the measures of the quitting intention. Specifically, the scale consisted of 23 items using a 7-point Likert-type response scale from 1 (‘definitely disagree’) to 7 (‘definitely agree’). Each construct subscale included three items (except the quitting intention), and we computed the mean as the subscale score.
Perceived severity was measured by three items: ‘The earlier a person starts smoking, the greater the harm’, ‘More smokers get sick than nonsmokers’, and ‘Smokers die earlier than nonsmokers’.
Perceived vulnerability was measured by three items: ‘I would become addicted if I smoked’, ‘I would get sick if I smoked’, and ‘If I smoke, I may die earlier’.
Intrinsic rewards were measured by three items: ‘Smoking makes people feel comfortable’, ‘Smoking helps people concentrate’, and ‘Smoking enhances brainwork’.
Extrinsic rewards were measured by three items: ‘Smokers look cool and fashionable’, ‘Smoking is good for social networking’, and ‘The life of a smoker is happier than that of a nonsmoker’.
Self-efficacy was measured by three items: ‘I am confident that I can quit smoking successfully’, ‘I have the ability to stop smoking’, and ‘I think stopping smoking is easy for me’.
Response efficacy was measured by three items: ‘People will feel good by not smoking’, ‘People will be less likely to get disease if they do not smoke’, and ‘Quitting smoking is good for disease recovery’.
Response cost was measured by three items: ‘A person may be isolated if they quit smoking’, ‘Refusing a cigarette offer is very impolite’, and ‘One will miss the enjoyment if he or she quits smoking’.
The intention to quit smoking was assessed with ‘I plan to stop smoking in the next month’ and ‘I expect to stop smoking in the next month’.
Quitting behaviour was measured by two questions. First, the respondents were asked, ‘Have you ever tried to quit? A: Yes, B: No’. The respondents who answered ‘A’ were then asked the second question: ‘What is the longest amount of time you have abstained from smoking? A: 1–30 days, B: 1–6 months, C: 6–12 months, D: more than 12 months’.
Data Analysis
Our data analysis was conducted in three steps. First, we examined the distribution of the categorical and continuous variables. Second, Cronbach’s alpha and interclass correlation coefficients (ICC) were used to assess the reliability of the individual PMT constructs. Third, we performed a multiple linear regression for a multivariable analysis. To examine the association between the PMT constructs, on the one hand, and the quitting intention and quitting behaviour, on the other hand, three sets of regression models were constructed and used in the analysis based on the procedures outlined by Yan et al. (Yan et al., 2014).
We created four perception scores based on the seven PMT constructs. The perceived threat was computed as the mean of the vulnerability and severity items, perceived rewards were computed as the mean of the extrinsic and intrinsic rewards items, the perceived efficacy of not smoking was computed as the mean of the response efficacy and self-efficacy items, and the perceived cost of not smoking was equal to the response cost construct score.
Then, we created two additional PMT pathway scores based on the four PMT perceptions described above. The threat appraisal pathway was computed as the difference between the perceived threat and perceived rewards. The coping appraisal pathway was computed as the difference between the perceived efficacy and perceived cost.
-
(1)
Model 1 included the seven PMT constructs simultaneously.
-
(2)
Model 2 contained the four PMT perceptions simultaneously.
-
(3)
Model 3 involved the two PMT pathways simultaneously.
We also include the quitting intention in each model when predicting quitting behaviour. Age, sex, education, and life satisfaction were included as control variables. We used SPSS 24.0 statistical software (SPSS Inc., Beijing, China) to conduct all the analyses.
Results
Demographic and Smoking Behaviour Information for the Entire Sample
We approached 738 smokers. After screening, 613 were identified as eligible for interviews. The participants were from 26 provinces in Mainland China. Table 1 shows the descriptive statistics for the overall sample. Approximately 46.8% of the respondents were in their 40s or older, with an average age of 37.95 ± 14.31 years. Of the respondents, 58.7% had an educational level of college or higher. Most smokers reported smoking 1–50 cigarettes per week. Approximately 48% intended to quit (i.e., stated that they wanted to quit within 6 months).
Item Responses and the Reliability of the PMT Constructs
The mean scores, Cronbach’s alpha coefficient, and ICC of the PMT constructs are summarized in Table 2. The mean score (SD) of the 23 items varied from 6.19 (1.48) for Item 1 (‘The earlier a person starts smoking, the greater the harm’) to 2.75 (1.82) for Item 10 (‘Smokers look cool and fashionable’). Cronbach’s alpha coefficient of the 23 items was 0.74. Cronbach’s alpha coefficient of all the subscales varied from 0.71 to 0.74.
Multiple Regression Models for the Quitting Intention
The first three columns of Table 3 present the standardized estimates for the multiple regression models predicting the quitting intention from the PMT variables (columns 1–3). Model 1 incorporated seven of the PMT constructs. Stronger intentions were significantly associated with higher perceived vulnerability (Coef. = 0.13, P < 0.01), self-efficacy (Coef. = 0.28, P < 0.01), and response efficacy (Coef. = 0.23, P < 0.01) but were inversely associated with intrinsic rewards (Coef. = −0.15, P < 0.01). Model 2 incorporated the four PMT perceptions. Only perceived threat (Coef. = 0.16, P < 0.01) and perceived efficacy (Coef. = 0.43, P < 0.01) were positively associated with the quitting intention. In Model 3, the quitting intention was regressed onto the two appraisal pathways. Greater intentions were significantly associated with higher threat (Coef. = 0.19, P < 0.01) and coping appraisals (Coef. = 0.25, P < 0.01).
Multiple Regression Models for Quitting Behaviour
To examine the predictive effect of PMT variables on quitting behaviour, we changed the dependent variable to quitting behaviour and reconducted the regressions. The last three columns of Table 3 present the results. In all models, intention is a highly significant variable associated with quitting behaviour. Specifically,
in Model 1, longer quitting attempts were significantly associated with self-efficacy (Coef. = 0.13, P < 0.01) and response cost (Coef. = −0.18, P < 0.01). In Model 2, perceived efficacy (Coef. = 0.13, P < 0.01) and perceived cost (Coef. = −0.20, P < 0.01) were associated with longer quitting attempts. In Model 3, coping appraisal was significantly associated (Coef. = 0.24, P < 0.01) with longer quitting attempts.
Discussion
To the best of our knowledge, our study is the first to test PMT constructs in explaining the quitting intention in the Chinese population. Overall, our results confirmed the applicability of PMT for predicting the quitting intention among Chinese adults. However, the results of this study provide only partial support for our hypotheses. This finding is consistent with those reported by other researchers that not all PMT measures had the same strength in predicting behaviour (Ruiter, Abraham, & Kok, 2001; Ruiter, Verplanken, Kok, & Werrij, 2003). Consistent with our hypotheses, both coping and threat appraisals exhibited significant predictive values for the quitting intention, suggesting that at least some of the seven PMT constructs act as stable factors influencing quitting behaviour.
Specifically, we obtained partial support for our first hypothesis: Among the threat appraisal constructs, vulnerability to the health threat was confirmed as a predictor of the quitting intention, but the severity of the threat was not, even though the items related to perceived severity had the highest mean score among all the items. A possible explanation for this ineffective predictive relationship is that people may know that smoking is harmful but are not truly motivated to quit. On the other hand, the higher vulnerability is a sign that smokers realize how they could be influenced by the negative consequences of smoking behaviour. However, currently, the most common tobacco control programmes and activities in China focus on teaching that smoking is harmful. Our results may challenge ongoing tobacco control programmes that solely prioritize assisting people in identifying the potential harms of smoking.
Regarding the second hypothesis, we found that, among the threat appraisal constructs, intrinsic rewards are one of the important predictors for the quitting intention, but extrinsic rewards and response costs may be less important in influencing this behaviour. The significant inverse association between intrinsic rewards and the quitting intention was also confirmed by other researchers. Yan et al. found that, despite having thorough knowledge of the harmful outcomes of smoking, students do not have the ability to quit cigarettes because they simply enjoyed smoking. The rewards included feeling good, enjoying the company of friends, and having a feeling of comfort (Yan et al., 2014). Therefore, encouraging smokers to correct their misperceptions of such intrinsic rewards from smoking will have better tobacco control effects than addressing the extrinsic rewards of smoking.
Consistent with our third hypothesis, response efficacy and self-efficacy were the strongest predictors of the quitting intention. Hypothesis 3 is also proven as perceived efficacy is the main predictor of the quitting intention among all four perceptions (perceived threat, perceived rewards, and perceived cost). This finding points to the importance of enhancing smokers’ perceived self-efficacy in quitting smoking and refusing cigarettes. Some potential techniques to improve self-efficacy, such as mastery and vicarious experiences, have been tested in other studies (Webb, Sniehotta, & Michie, 2010b). Therefore, activities with the goal of smoking intervention and cessation efforts should recognize the importance and effectiveness of incorporating evidence-based methods to promote perceived efficacy related to quitting.
Our data suggest that individual PMT components differ in the significance of their ability to predict the quitting intention. Therefore, to achieve better effects, specific attention should be directed to the more influential PMT constructs when designing smoking-cessation interventions. Furthermore, our study supports the hypothesis that the different constructs of threat and coping appraisals can cross-sectionally predict smoking-related behavioural intentions. Thus, how do these factors interact with each other? Is there any potential mediator? All these questions warrant further research. In addition, future research would also benefit from using longitudinal data to prospectively determine the predictive value of the different components of PMT.
As stated in the introduction, the ultimate goal of intervention is to affect individuals’ behaviour; however, many studies assess only mental effects. We recognize that intentions are important, as they ‘get the ball rolling’, but, given that many people fail in their pursuit of smoking cessation, measuring the intention alone provides only a partial picture. We advance our results by measuring the psychological determinants and the target behaviour simultaneously. The results show that the quitting intention is significantly associated with quitting behaviour in all models. Self-efficacy and response cost are significantly related to quitting behaviour (last hypothesis). Self-efficacy is the only factor that has a predictive effect on both the intention and behaviour; it extends from the quitting intention to quitting behaviour. This finding is consistent with early research suggesting that coping appraisal—and, within this construct, especially self-efficacy—is a better predictor of health behaviour than threat appraisal (Ruiter et al., 2003; Thrul et al., 2013), thus reaffirming that threat communication may be less important for smoking-cessation-related health education.
Our study has several limitations. First, we used only cross-sectional data for this estimation. As a result, we cannot infer a causal relationship. Second, most of our participants were male. A study including females might lead to different results. Third, all the information we collected was self-reported without verification, and the respondents’ interpretations of some questions might have varied. Fourth, most of the interviewers were students at the Peking University Health Science Centre; to ensure their safety, data collection mostly took place in large business districts and large residential areas in urban regions. Therefore, the surveys could have been biased because we concentrated on certain areas.
Despite these limitations, our findings have theoretical implications. First, although PMT is a widely used theory and especially useful for addressing smoking behaviour, most well-designed previous studies have focussed on smoking prevention or smoking motivation analyses. Our research is an extension of the theory for smoking-cessation motivations. Second, as the literature suggests, PMT has been used to explain various motivations in Western countries. This is the first study to extend the application of such theory in Chinese adults. Therefore, our research also demonstrates the cross-cultural generalization of the theory as an additional contribution.
In addition, our study has policy implications. This study was the first to evaluate a scale measuring PMT constructs to understand quitting behaviour among Chinese adults. It provides a useful framework for investigating predictors of the quitting intention. This framework is essential for understanding quitting behaviour among Chinese adults to support a more effective tobacco control strategy. The findings could also encourage policymakers and health practitioners to implement theory-based behavioural interventions and thereby contribute to achieving better smoking-reduction outcomes.
Conclusion
In conclusion, the present study demonstrates that some PMT constructs—such as self-efficacy, response efficacy, intrinsic rewards, and perceived vulnerability—are useful in understanding quitting behaviours. Self-efficacy is the only factor that has a predictive effect on both the intention and behaviour. The lack of the predictive validity of the threat appraisal variables in predicting cessation-related behaviours provides further indication that threat communication as a means of promoting quitting attempts may not be the most effective strategy. Instead, it may be more fruitful to enhance adults’ self-efficacy to believe they can successfully quit smoking by strengthening their coping skills for how to remain abstinent. It provides new evidence supporting the utility of Western theories for advancing tobacco control in China. Taken together, we believe our research not only contributes to identifying the determinants of the quitting intention but also provides further evidence regarding smoking behaviour in a developing country and adds to earlier research on this topic.
Data Availability
The study data are accessible via Peking University, School of Public Health.
Abbreviations
- PMT:
-
protection motivation theory
- ICC:
-
interclass correlation coefficient
References
Abraham Charles, S., Paschal, S., Dominic, A., et al. (1994). Exploring teenagers' adaptive and maladaptive thinking in relation to the threat of hiv infection. Psychology & Health, 9, 253–272.
Bashirian, S., Barati, M., Mohammadi, Y., et al. (2019). An application of the protection motivation theory to predict breast self-examination behavior among female healthcare workers. Eur J Breast Health, 15, 90–97.
Ben-Ahron, V., White, D., & Phillips, K. (1995). Encouraging drinking at safe limits on single occasions: The potential contribution of protection motivation theory. Alcohol and Alcoholism, 30, 633–639.
Brooks, S. P., & Bubela, T. (2020). Application of protection motivation theory to clinical trial enrolment for pediatric chronic conditions. BMC Pediatrics, 20(1), 123.
Brooks Stephanie, P. (2020). Bubela Tania, Application of protection motivation theory to clinical trial enrolment for pediatric chronic conditions. BMC Pediatr, 20, 123.
China Disease Control and Prevention Center. (2016). 2015 China adult tobacco survey. Beijing: China CDC.
China Disease Control and Prevention Center. (2019). 2018 China adult tobacco survey. Beijing: China CDC.
Greening, L. (1997). Adolescents’ cognitive appraisals of cigarette smoking: An application of the protection motivation theory. Journal of Applied Social Psychology, 27, 1972–1985.
Jansen, P.C.P., Snijders, C.C.P., Willemsen, M.C. (2020). Playing with fire. Understanding how experiencing a fire in an immersive virtual environment affects prevention behavior [published correction appears in PLoS One. 2020 May 7;15(5):e0233123]. PLoS One, 15(3):e0229197.
Lin, H. X., Liu, Z., Chang, C., et al. (2019b). Design, development and randomised controlled trial of a smartphone application, 'QinTB', for smoking cessation in tuberculosis patients: study protocol. BMJ Open, 9(12), e031204.
Lin Haoxiang,Chang Chun,Liu Zhao et al. Subnational smoke-free laws in China. Tobacco Induced Diseases, 2019a, 17: 78.
Macdonell, K., Chen, X., Yan, Y., et al. (2013). A protection motivation theory-based scale for tobacco research among Chinese youth. J Addict Res Ther., 4, 154.
Malmir, S., Barati, M., Khani Jeihooni, A., Bashirian, S., & Hazavehei, S. M. M. (2018). Effect of an educational intervention based on protection motivation theory on preventing cervical cancer amongMarginalized women in West Iran. Asian Pacific Journal of Cancer Prevention, 19, 755–761.
Milne, S., Sheeran, P., & Orbell, S. (2000). Prediction and intervention in health-related behavior: A meta-analytic review of protection motivation theory. Journal of Applied Social Psychology, 30(1), 106–143.
Rogers, R. W. (1983). Cognitive and physiological processes in fear appeals and attitude change: A revised theory of protection motivation. In J. T. Cacioppo & R. E. Perry (Eds.), Social psychophysiology: A source book (pp. 153–176). New York: Guildford Press.
Ruiter, R. A. C., Abraham, C., & Kok, G. (2001). Scary warnings and rational precautions: A review of the psychology of fear appeals. Psychology & Health, 16, 613–630.
Ruiter, R. A. C., Verplanken, B., Kok, G., & Werrij, M. Q. (2003). The role of coping appraisal in reactions to fear appeals: Do we need threat information? Journal of Health Psychology, 8, 465–474.
Sabzmakan, L., Ghasemi, M., Asghari Jafarabadi, M., Kamalikhah, T., & Chaleshgar, K. M. (2018). Factors associated with tobacco use among Iranian adolescents: An application of protection motivation theory. Substance Use & Misuse, 53(9), 1511–1518.
Schwarzer, R., & Fuchs, R. (1996). Self-efficacy and health behaviors. In M. Conner & P. Norman (Eds.), Predicting health behavior: Research andpr-nctice with social cognition models (pp. 163–196). Buckingham: Open University Press.
Seyde, E., Taal, E., & Wiegman, O. (1990). Risk-appraisal, outcome and self-efficacy expectancies: Cognitive factors in preventive behaviour related to cancer. Psychology & Health, 4(2), 99–109.
Stainback, R. D., & Rogers, R. W. (1983). Identifying effective components of alcohol abuse prevention programs: Effects of fear appeals, message style, and source expertise. International Journal of the Addictions, 18(3), 393–405.
Taheri-Kharameh, Z., Bashirian, S., Heidarimoghadam, R., Poorolajal, J., Barati, M., & Rásky, É. (2020). Predictors of fall protective behaviors among Iranian community-dwelling older adults: An application of the protection motivation theory. Clinical Interventions in Aging, 15, 123–129.
Thrul, J., Stemmler, M., Bühler, A., & Kuntsche, E. (2013). Adolescents' protection motivation and smoking behaviour. Health Education Research, 28(4), 683–691.
Webb, T. L., Sniehotta, F. F., & Michie, S. (2010a). Using theories of behaviour change to inform interventions for addictive behaviours. Addiction., 105(11), 1879–1892.
Webb, T. L., Sniehotta, F. F., & Michie, S. (2010b). Using theories of behavior change to inform interventions for addictive behaviours. Addiction, 105, 1879–1892.
Xu, Y., & Chen, X. (2016). Protection motivation theory and cigarette smoking among vocational high school students in China: A cusp catastrophe modeling analysis. Glob Health Res Policy., 1, 3.
Yan, Y., Jacques-Tiura, A. J., Chen, X., Xie, N., Chen, J., Yang, N., Gong, J., & MacDonell, K. K. (2014). Application of the protection motivation theory in predicting cigarette smoking among adolescents in China. Addictive Behaviors, 39(1), 181–188.
Yang, G. H., Li, Q., Wang, C. X., et al. (2010). Findings from 2010 Global Adult Tobacco Survey: Implementation, of MPOWER Policy in China. Biomed Environ Sci, 23(6), 422–429.
Funding
This study was supported by Peking University.
Author information
Authors and Affiliations
Contributions
HX L wrote the first draft. CC managed the study. All the authors have approved the final paper for submission.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
This study was approved by the Peking University. Verbal informed consent was obtained from all the participants.
Consent for Publication
Not applicable.
Competing Interests
On behalf of all the authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lin, Hx., Chang, C. Factors associated with the quitting intention among Chinese adults: Application of protection motivation theory. Curr Psychol 42, 1083–1091 (2023). https://doi.org/10.1007/s12144-021-01500-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-021-01500-5