
Abstract
This literature review explores the impact of COVID-19 upon the residential aged care (RAC) workforce during the coronavirus (COVID-19) pandemic, including the workforce from culturally and linguistically diverse (CALD) backgrounds. It also considers COVID-19 related interventions for the RAC workforce. The databases ProQuest, PubMed, Cumulated Index to Nursing and Allied Health Literature (CINAHL), Google Scholar and Cochrane Central were searched in April and May 2022. Twenty-six studies were identified which were related to the impact of COVID-19 on the RAC workforce, including four studies on the CALD workforce. Many studies highlighted the impact of COVID-19 upon workforce shortages, workplace demands, worker wellbeing, and intention to quit the profession. The importance of workplace communication and support strategies during the COVID-19 pandemic were also underlined. Issues pertinent to the CALD workforce included understanding dementia, vaccine hesitancy and the impact of aged care, migration and labour market policies on the workforce. Workforce factors, including poor working conditions (and lack of paid leave) had a significant impact upon COVID-19 morbidity and mortality. Conversely, responding to COVID-19 impacted workforce mental health. There is a need for workforce support policies and research which consider organisational communication, work-life balance, and specific training and support needs of workers from CALD backgrounds, who comprise a significant proportion of the aged care workforce in Australia and many other countries.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background and Rationale
Residents and staff of residential aged care facilities (RACF) are at elevated risk of acquiring and transmitting COVID-19 (Frazer et al., 2021), with contributing workforce factors including staff working across multiple facilities (Dykgraaf et al., 2021; Giri et al., 2021), the casualisation of the workforce and working conditions (e.g. low renumeration). The impact of COVID-19 upon the workforce (physically and psychologically) is an important consideration both for worker wellbeing and retention and the containment of the COVID-pandemic.
Studies on ‘lessons learnt’ for the containment of COVID-19 in nursing homes and other health care facilities, have had a strong focus on infection prevention and control (IPC) strategies (Gilbert, 2020; Johnston et al., 2021; Shrader et al., 2021). The workforce in this sector is an important resource for developing and implementing IPC strategies. There is a need to ensure RACF staff are adequately trained in IPC, paying particular attention to any training needs of workers from culturally and linguistically diverse (CALD) backgrounds.
Governmental and organisational factors such as the establishment of risk communication with strong community engagement strategies to ensure the successful and prompt sharing of information (including in relevant languages and with diverse communities) and listening to communities during a COVID-19 outbreak is important for outbreak containment (WHO, 2018). Cultural factors and practices may play a role in effective COVID-19 response strategies, and the CALD workforce within RACFs, given their significant cultural understanding and linguistic skills, could be harnessed to better support CALD residents and families.
In Australia, the RACF workforce is highly culturally and linguistically diverse, with 24% of the RAC workforce from CALD backgrounds (Australian Government, 2021). However, the cultural and linguistic diversity of aged care workers is often overlooked in policy formation. For example, the Australian Government’s Department of Health Aged Care Workforce Strategy (Aged Care Workforce Strategy Taskforce, 2018), fails to note the high proportion of migrants and those from CALD backgrounds in this workforce, and so does not address the implications this may have for the delivery of appropriate care (Adebayo et al., 2021), including pandemic preparedness and response.
This literature review sought to understand the experiences of RACF staff during COVID-19, with a particular focus on workers from culturally and linguistically diverse (CALD) backgrounds. Questions considered were:
-
How did the COVID-19 pandemic impact the RAC workforce?
-
What was the experience of the workforce from culturally and linguistically diverse (CALD) backgrounds working in RACFs during the COVID19 pandemic?
-
How did cultural understandings and factors impact upon responses to COVID-19 requirements for RACFs?
-
Were there specific organisational challenges during the COVID-19 pandemic for RAC organisations that had a high CALD workforce?
-
What are the key factors which enable optimal service delivery during an outbreak or pandemics which take into account the CALD aged care workforce?
Methodology
This literature review was undertaken as part of a broader systematic scoping review study that considered the impact of COVID-19 on the RAC sector (Authors, forthcoming) and people with cognitive impairment (Authors, forthcoming). This article focuses on the review articles and commentaries which made reference to the workforce in RACFs (including the CALD workforce) during the COVID-19 pandemic. This broader review followed guidance for conducting systematic scoping reviews.
The databases ProQuest, PubMed, Cumulated Index to Nursing and Allied Health Literature (CINAHL), Google Scholar and Cochrane Central were searched between 6 April and 9 May 2022 for review articles and original studies related to organisational challenges, sector (including workforce) impact and innovations related to COVID-19, and residents with cognitive impairment (concept areas 1–5 below). Additional Google Scholar searches related to interventions for residential care facility residents with cognitive impairment during the COVID-19 pandemic was undertaken on 9 May 2022 (concept areas 1, 2, 4 and 6 below). On 24 May 2022 an additional search was undertaken for papers which considered the workforce from CALD backgrounds (using concept areas 1, 2, 7 and 8 below). Inclusion criteria were 1) peer reviewed review articles that included reviews, original studies and commentary articles, 2) published between December 2019 and May 2022, 3) articles in English.
In mid-June, further searches sought grey and academic literature on international and national (Australian) policy documents (and websites), along with academic literature on the assessment of country level policies and guidelines (using concept areas 1, 2, 4 and 9 below), with a focus on Australian policies within the grey literature. In late August 2022, additional searches were conducted on service delivery guidelines in the RAC sector during COVID-19 (using concept areas 1, 2 and 10), with a focus on international and national (Australian) guidelines. Search terms for various concept areas are in Table 1 below.
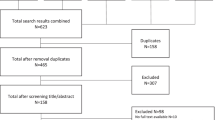
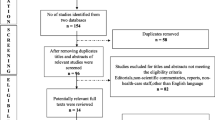
Following initial searches, titles of papers were screened and abstracts were read to conduct an initial assessment for eligibility, and articles downloaded into Endnote. Given the high volume of articles identified, the decision was made to focus upon review articles for ‘sector impact’ and review and individual studies that focused on residents with cognitive impairment for the resident impact/interventions, and all workforce (including CALD workforce) articles. Following a full read of articles, articles were transferred across of Endnote files and/or included or excluded based upon relevance to the study and bibliographies. A database was established for data extraction for the academic review, research and commentary articles, with information extracted including: author/title/year of publication, purpose of study, country of origin, setting, research design, methodology, search period, databases searched and type of papers included (for review articles), study population and sample size (if applicable), type of intervention, exposure and control (if applicable), measures, key findings (including statistical findings) and implications, and quality of study/review (considering the level of evidence in the National Health and Medical Research Council framework (NHMRC, 2009). The total number of full articles included in the broader review was 116 articles. A full explanation of the search methodology is outlined in an integrative literature review report (Battams & Martini, 2023). Table 2 below indicates the number of articles identified, screened, downloaded into the Endnote files, read and included in the review.
Results
There were 26 review and original research articles identified where a main focus was the impact of COVID-19 on the RAC sector workforce, including four which considered the workforce from CALD backgrounds. This includes two systematic reviews (Frazer et al., 2021; Gray et al., 2021), one scoping review (Adebayo et al., 2020), one commentary article (Gaur et al., 2022), eleven cross sectional or cohort studies (Krzyzaniak et al., 2021; Brydon et al., 2022; Harrington et al., 2020); Xu et al., 2020; Werner & Coe, 2021; Pförtner et al., 2021; Senczyszyn et al., 2020; Tomaszewska et al,. 2022; Niznik et al., 2022; Cimarolli et al., 2022), eight qualitative studies (Fisher et al., 2021; Scheffler et al., 2022; White et al., 2021; Sarabia-Cobo et al., 2021; Hoedl et al., 2022; Yau et al., 2021; Kuhlmann et al., 2020; Hung et al., 2022) and three intervention studies which were non-randomised or quasi-experimental studies (Feifer et al., 2021; Lingum et al., 2021; Nakanishi et al., 2021). Three studies were from Australia, eleven studies were from the United States of America (USA), two were from Canada, nine from Europe, and one from Japan. Just two studies in this review were on nursing home assistants only (Niznik et al., 2022; Scheffler et al., 2022), whilst another considered nursing home assistants and other staff (Fisher et al., 2021). Below, articles associated with key themes on the impact of COVID-19 on the RAC workforce are firstly discussed before considering those which explored the impact of COVID-19 on the workforce from CALD backgrounds.
Overall Impact of the COVID-19 Pandemic Upon the RAC Workforce
A number of articles considered the overall impact of the COVID-19 pandemic on the RACF workforce.. These emphasised the psychological burden for RACF staff during the COVID-19 pandemic, high workload and staff shortages, the association between COVID-19 and number of staff at facilities, challenges of changing regulations and inconsistent messaging, and work-life balance issues. Positive elements reported included increased collegiality, resilience and professional commitment.
Frazer et al.’s (2021) systematic review focused on measures implemented in LTC facilities to reduce transmission of COVID-19. The review found that there was no pattern between COVID-19 prevention strategies adopted and the prevalence of COVID-19 infection. The size and number of outbreaks were associated with factors such as: size of the facility (higher number of beds), availability of staff (higher numbers of staff preferable), numbers of staff working across multiple facilities, the for-profit status of facilities and access to paid sick leave (Frazer et al., 2021).
Gray et al. (2021)’s systematic review sought to examine the experiences of RACF staff during the pandemic, and found that staff anxiety, distress and Post Traumatic Stress Disorder (PTSD) was common and associated with fear of contagion and transmitting COVID-19. These were associated with conditions such as difficulties obtaining and using appropriate PPE, inconsistent government and organisational guidelines, high workload and staff shortages, social pressure, ongoing contact with death and suffering and the unpredictable environment. Groups more vulnerable to mental health concerns included shift workers, females (Riello et al., 2020, in Gray et al., 2021), Black, Asian, Minority and Ethnic (BAME) staff, nurses and younger staff (Greene et al., 2021, in Gray et al., 2021). Positive factors arising from the COVID-19 pandemic included: increased team working skills and co-operation across residents, staff and family groups (White et al., 2021, in Gray et al., 2021) and the establishment of peer support networks (Spilsbury et al., 2021, in Gray et al., 2021). The review recommended providing access to a psychologist for staff, peer support and supervisor support, virtual support groups, providing staff recognition, ensuring consistent guidelines and effective organisational communication, and taking a bio-psycho-social perspective to supporting staff in RACFs (Gray et al., 2021) (see Table 3).
White et al. (2021) conducted an online survey with staff (n = 152) in US nursing homes, and discovered seven key themes: constraints on access to PPE and testing resources; burdensome and contradictory regulations and guidance across levels of government; staff concerns for their own health and that of their family; concern for residents related to both COVID-19 and social distancing requirements; staff burnout related to staff shortages, increased workload and new responsibilities; teamwork, communication and flexibility; and public blame and lack of support and recognition for nursing home staff. White et al. (2021) highlighted the potential long-term effects of the physical, mental and emotional burden experienced by nursing home staff during the pandemic.
Two smaller qualitative studies from the US also highlighted staff mental health issues (Fisher et al., 2021; Scheffler et al., 2022). Fisher et al. (2021) sought to explore factors that influenced the wellbeing of staff (n = 14) working in long term care (LTC) in New York City and found that they consistently reported stress, anxiety and trauma during the spring 2020 COVID-19 surge, along with home-work life balance stressors and workplace stressors. Recommendations included increased staff bonuses and incentives, extra protection for staff, provision of childcare, increasing staff numbers, providing more sick leave, and providing counselling support. Scheffler et al.’s (2022) study of nursing home assistants (n = 9) in the US during the COVID-19 found changing and challenging regulations and requirements, the need for more training on issues such as PPE usage, mixed perceptions of the nursing home assistant role, feelings of isolation and psychological stress. Recommendations included providing consistent messages across nursing home facilities, local communities and the media to support nursing assistants, promoting their emotional wellbeing and develop a mutually supportive learning community. Scheffler et al.’s (2022) noted that nursing assistants’ participation in training was limited due to reduced staffing levels associated with COVID-19, and called for leadership commitment to upskilling, and more recognition and support for nursing assistants.
A Canadian qualitative study with a small number of participants (n = 30) (Hung et al., 2022) considered the experiences, challenges and needs of long term care (LTC) staff during COVID-19. Four main themes were identified: staff feeling proud of their resilience in working in the profession during the challenging times of COVID-19 and having passion for their role; staff feeling anxious about contracting and spreading COVID-19 and residents’ declining mental health; growing closer to residents and other staff members during the pandemic; and, the helpfulness of vaccines in controlling the pandemic. The study concludes by emphasising the need for policy and structural support to develop the resilience, mental health and wellbeing of staff.
Krzyzaniak et al.’s Australian study (2021) similarly found a high proportion of those working in RACFs (63%) reported that they had suffered work related stress during COVID-19, but just over half (53%) had been offered mental health support from their organisation. Additionally, although 28% were concerned about the continuing impact of the pandemic upon their mental health. Many respondents (43%) reported unfair or abusive treatment by family and friends of residents. Fifty-one percent reported a very high workload and 31% reported a high workload since COVID-19. A higher proportion of those working in private for profit and not for profit/charitable facilities reported a very high workload (p < 0.05) compared to those working in government facilities. Qualitative responses revealed workload increase, burnout, anxiety, insomnia, depression, grief, emotional stress, family issues and fatigue. Support from colleagues, and training, debriefing and frequent meetings were factors identified as being helpful at this time.
A third reported difficulties in estimating and ordering appropriate quantities of PPE, with staff from private for profit and government owned RACFs more likely to feel they had received a sufficient amount of PPE compared to those from not for profit/charitable facilities (p < 0.05). Over half (63%) felt they had sufficient access to COVID-19 testing resources, with those from government operated RACFs more satisfied with their access to tests (p < 0.05). Most respondents (92%) felt that they had received sufficient information on dealing with suspected COVID-19 cases, but fewer (66%) felt that their facilities had received clear instructions from official bodies about testing for COVID-19. The majority (87%) thought that relevant health care authorities were able to be easily contacted for further information when required and that they had received instruction on how to use PPE (90%), and the type (95%) and quantity of PPE needed (84%). Qualitative responses revealed difficulties in accessing COVID-19 information or receiving conflicting information, and there was a perceived lack of clear messaging from government on appropriate protocols (Krzyzaniak et al., 2021).
Another Australian study considered the prevalence of pandemic related distress within the RACF sector and contributing factors, as perceived by senior care staff (Brydon et al., 2022). Survey respondents estimated that around 36% of staff were anxious, 27% had poor mental health, 27% had lower morale, and 20% had increased depression as a result of the COVID-19 pandemic, associated with concerns about transmitting COVID-19 in the RACF and watching news media on COVID-19 outbreaks. There was also increased personal leave (24%) and workplace conflict (18%). The survey was supported by qualitative data on the mental health difficulties of residents and staff (Brydon et al., 2022).
A Spanish qualitative study with a small number of participants (n = 24) (Sarabia-Cobo et al., 2021) involved interviews with nurses across four countries, with three main themes identified: fear of the pandemic and uncertainty about strategies adopted; a sense of duty and professional commitment as well as social stigma towards nursing homes and the profession; and emotional exhaustion associated with anxiety, depression and emotional burnout. Sarabia-Cobo et al. (2021) argue that nurses require a continuum of psychological support (from prevention to treatment) at different levels (organisational to individual care to team support). Proposed areas for future research include; evaluating the impact of COVID-19 on the mental health of nurses in the longer term and research on interventions to prevent and manage emotional exhaustion and burnout (Sarabia-Cobo et al., 2021).
An Austrian qualitative study with nursing home staff (n = 18) on burdens arising from COVID-19 and their consequences (Hoedl et al., 2022) found the following themes: staff workload increases associated with COVID-19 infection prevention and control and attending to residents and families; changed working conditions that were psychologically and physically challenging and associated with fear, stress and uncertainty; staff restricting their social activities due to fears about contracting and transmitting COVID-19; and staff supporting each other. Nurses also reported that visiting restrictions had led to the decline of residents’ emotional state and an increase in loneliness. Hoedl et al. (2022) call for pandemic recommendations that enhance resident’s psychological and social wellbeing and their physical wellbeing, and measures to support staff and residents, such as individually tailored programs to decrease psychological stress and fear.
The Role of Institutional Factors and Non Workplace Factors Upon Staff Mental Health
Two Polish studies highlighted the role of institutional support and demands outside of the workplace upon the mental health of RACF staff. Senczyszyn et al. (2020) set out to assess psychological consequences of responding to COVID-19 among Polish LTC facility staff, using the General Health Questionnaire (GHQ-28). The study underscored the importance of institutional factors including access to PPE, workplace safety guidelines and availability of psychological support to the mental health of nursing home staff. Staff who had access to PPE had lower scores on social dysfunction and having well-developed workplace safety guidelines were related to lower anxiety and insomnia. Beliefs that there were staff shortages during the pandemic was related to a higher GHQ-28 total score. Staff in facilities that had access to a psychologist at the workplace had lower GHQ-28 scores than staff in facilities that did not.
In another Polish study, Tomaszewska et al. (2022) considered the impact of the COVID-19 pandemic on psychosocial burden and job satisfaction amongst LTC nurses in Poland. The study found less work-related stress than was expected, with higher mean psychosocial risk/psychosocial hazards in the workplace associated with lower job satisfaction. This study also highlighted non workplace factors upon job satisfaction, including having a higher number of people and higher number of children in the household. These associations were attributed to concerns about risk of COVID-19 transmission to the home environment.
Effect of Employer Communication, Job Stressors, Intention to Quit and Resignation
Two studies considered the association between job stressors and intention to quit the profession or resignation (Cimarolli et al., 2022; Pförtner et al., 2021)). In a US study with a large sample (n = 1730), Cimarolli et al. (2022) investigated if the quality of employer communication and staff preparedness to care for residents with COVID-19 could mediate the effects of COVID-19 related stressors on nursing home employees and their decision to resign. Staff who had resigned had significantly lower scores on perceived quality of employer communication regarding how to care for residents during COVID-19 (p = 0.02), and how to protect yourself and your family (p = 0.02), and perceived level of preparedness (p = 0.00) for COVID-19. There was no significant direct association between COVID-19 related stressors and worker resignation, however there was a significant positive indirect effect of such stressors on resignation. Better quality of organisational communication was significantly associated with higher preparedness, and higher preparedness was significantly associated with reduced likelihood of resignation. Cimarolli et al. (2022) conclude that high quality organisational communication is important to both care for residents with COVID-19 and to retain nursing home staff.
In a German study (n = 532), Pförtner et al. (2021) sought to determine if the demands of COVID-19 would increase the intention of LTC managers to quit the profession. The percentage of those who said they intended to quit the profession ‘often/very often’ rose from 12.8% (n = 68/532) to 20.3% (n = 61/301) across two survey periods during the COVID-19 pandemic (P = 0.004). The perceived level of pandemic related demands also increased significantly (p = 0.004), along with levels of general demands (P ≤ 0.001). Results of multivariate logistic regression analysis indicated an association between intention to quit the profession and ratings on pandemic-specific demands (OR = 1.034; CI = 1.011–2.057, P = 0.003) and general demands (OR = 1.023; CI = 1.001–1.045, P = 0.042) (Pförtner et al., 2021).
Relationship Between COVID-19, Staffing Levels and Location of Facility
Three US studies considered the relationship between COVID-19 and staffing levels (Harrington et al., 2020; Werner & Coe, 2021; Xu et al., 2020), whilst a fourth considered staffing levels and facility location (Yang et al., 2021). Harrington et al. (2020) found that higher rates of COVID-19 were associated with total nurse and Registered Nurse (RN) staffing levels, health practice deficiencies (e.g., infection control violations) and total number of beds. If RN staffing was less than 0.75 h per resident day the odds ratio (OR) of residents having COVID-19 was 2.086 (95% CI: 1.318, 3.301] (B = 0.735, p < 0.001). Notably, almost 80% of Californian nursing homes did not meet the recommended staffing levels for RNs and 55% did not meet the minimum recommended total nursing standard.
Xu et al. (2020) considered factors associated with shortages of nursing home staff during the COVID-19 pandemic. Of the nursing homes, 15.9% reported shortages of licensed nursing staff, 18.4% reported shortages of nurse aides, 2.5% shortages of clinical staff and 9.8% shortages of other staff. There were significant associations between nursing home staff shortages and residents having COVID-19. Shortage in licensed nurses and in nurse aids were more likely in nursing homes having residents with COVID-19 and those that had any staff with COVID-19.
Werner and Coe (2021) examined nursing home staffing levels in the US during the first nine months of 2020, compared with the same period in 2019. Whilst there was a decline in nursing home staff hours during the period studied, there was also a decline in average nursing home residents. When the resident decline was considered, nursing home staff hours remained steady or increased slightly (with increases concentrated in areas where COVID-19 rates were highest). The study concludes by advocating for widespread access to COVID-19 testing for staff, hazard pay, safe transportation, expanded paid sick leave and developing strategies for the safe return of families to nursing homes (Werner & Coe, 2021).
In a large US study, location of nursing homes was found to be associated with staffing shortages, however rural nursing homes were less likely to have residents with COVID-19 or residents dying from COVID-19, even though they were more likely to have experienced staff shortages during the COVID-19 pandemic (Yang et al., 2021).
Best Practices and Recommended Strategies for Improvement
Two articles focused upon best practices for the workplace during COVID-19 (Gaur et al., 2022; Yau et al., 2021). Gaur et al.’s (2022) US commentary article discusses principles of safety and the need to better integrate them into nursing homes and the regulatory environment. Gaur et al. (2022) also identified positive practices associated with the COVID-19 pandemic, including recognising the high-risk nature of nursing homes and collaboration across ranks, disciplines and levels of government. The Centers for Medicare and Medicaid Services (CMS) dedicated resources to address safety concerns, suspending the regular survey process and focusing on infection prevention and control. There were also blanket waivers for telemedicine, relaxing training and certification requirements for nurse aides and allowing physicians to delegate more tasks to nurse practitioners, clinical nurse specialists and physician assistants. States implemented strike teams in partnership with the National Guard to provide personnel, technical expertise and material assistance to nursing homes including staffing, testing assistance, vaccine clinics, PPE and administration of monoclonal antibodies.
Yau et al.’s (2021) small Canadian study identified critical factors for outbreak management related to the workforce which included: external support and assistance (e.g. infection prevention and control support and rapid onsite assessments); staff training and education (inhouse training and education by external infection prevention and control teams); workplace culture, organisational leadership and management (staff commitment to providing care, leaders as role models); coordination and communication (having an explicit and effective communications strategy and regular communication with stakeholders); and working to maintain or increase staffing levels. Key recommendations were: maintain a high level of vigilance for COVID-19 at LTC facilities; provide regular, ongoing and comprehensive infection prevention and control training and education; and, develop formal mechanisms for communication and coordination during the pandemic.
Education and Training for Staff During the Pandemic
Two studies considered the efficacy of online training for staff in LTC facilities, one of which focused on preparation for dealing with residents with COVID-19 (Lingum et al., 2021), and the other on the efficacy of a training program for staff working with residents with neuropsychiatric symptoms of dementia (Nakanishi et al., 2021). Lingum et al.’s (2021) Canadian study set out to determine whether a virtual education program (Project ECHO) was effective in providing just-in-time learning and best practices to support LTC teams and residents during the pandemic. The training consisted of one-hour sessions across 12 weeks with 252 registered for the training, mainly nurses and nurse practitioners (43.8%). The study assessed health professionals’ confidence and comfort with working with residents who were at risk of, suspected of or confirmed as having COVID-19. Overall, confidence and comfort in working with residents who were at risk, confirmed, or suspected of having COVID-19 increased after participating in the training sessions (effect sizes all ≥ 0.7, p < 0.001) (Lingum et al., 2021).
Nakanishi et al.’s (2021) Japanese study sought to evaluate the feasibility and efficacy of an e-learning course for staff in combination with a web-based tool to address neuropsychiatric symptoms of dementia. The e-learning on dementia behaviour analysis and support enhancement (DEMBASE) course was delivered three times to professional caregivers during a period of six months (July to December 2020) online and face to face. The training involved an interdisciplinary meeting to evaluate neuropsychiatric symptoms and specify unmet needs using a checklist and, establishing and implementing an action plan, using the Neuropsychiatric Inventory (NPI) via a web-based tool. Professional caregivers who completed the web-based course were less likely to implement follow up evaluations (p = < 0.001) than those that attended the face-to-face training.. The level of NPI symptoms was significantly reduced for both experimental and control groups at follow up (no significant differences between NPI scores between groups). Nakanishi et al. (2021) claim that this showed the efficacy of the e-learning training course in reducing neuropsychiatric symptoms.
CALD Workforce
Four articles were identified on the COVID-19 pandemic and the CALD workforce, including one scoping review (Adebayo et al., 2020) and three individual studies (Feifer et al., 2021; Kuhlmann et al., 2020; Niznik et al., 2022). Adebayo et al (2020) considered dementia care experiences in the migrant aged care workforce. Some studies suggested there may be a limited understanding of dementia amongst some groups of migrant aged care workers. For example, one Swedish study included participants reporting that there was no definitive description of dementia in Middle Eastern culture, and that dementia care was considered a family responsibility (Antelius & Plejert 2016, in Adebayo et al., 2020). Several factors were identified for the retention of staff from CALD backgrounds, including: availability of organisational support and resources; professional development opportunities; reciprocity and mutual respect between migrant care workers, care recipients and co-workers; and good working conditions (e.g., renumeration and working hours). Barriers to retention of CALD workers identified included discrimination and racism faced as a care worker (from other workers and care-recipients) and lack of understanding of workplace culture among workers from CALD backgrounds. It was found that communication difficulties may arise between migrant care workers and residents or co-workers/employers, related to language skills. Conversely, having a shared native language between the migrant care worker and care-recipient could increase wellbeing among residents. Conversely, migrant care workers could be favoured by employers due to their work ethic, loyalty and willingness to work a range of shifts. In one study, cultural norms including respect for elders influenced perceptions that they were better care workers. Workers from CALD backgrounds are also more likely to develop relationships that extended beyond the care setting. However, high workload and low staff-patient ratios could impact relationships between care workers and care recipients. Adebayo et al. (2020) conclude by highlighting the need for: dementia training for all staff; resources for support and education; orientation programs; access to language support services; providing information on health care resources; training on workplace culture; and cultural competence training for staff members working with migrant workers.
CALD Workforce and COVID-19 Vaccine Hesitancy and Interventions
Two US studies considered vaccine hesitancy and people from CALD backgrounds (Niznik et al., 2022; Feifer et al., 2021). In a small US study, Niznik et al. (2022) researched the perceptions of COVID-19 vaccines amongst healthcare assistants, 53.5% of which were working in nursing homes. Health care assistants reported low confidence in COVID-19 vaccines and a lower proportion of black survey respondents (compared to white) believed that the vaccines had been adequately tested for safety and effectiveness amongst people of colour. This finding was attributed to less actual testing of vaccines among racial minorities, less trust in government and structural racism. Where organisational leadership was rated as poor, survey respondents were more likely to believe that vaccines were less effective at preventing people from being sick and that vaccines had not been adequately tested for safety and effectiveness, especially among people of colour. Feifer et al. (2021) considered racial disparities in vaccine acceptance amongst RACF staff pre and post an intervention which involved a vaccine education campaign and establishment of a Diversity, Equity and Inclusion Committee whose representatives attended information sessions to help facilitate culturally sensitive discussions with multilingual Doctors. The study indicated the effectiveness of the intervention as there were significant improvements in the likelihood of being vaccinated for black employees and Hispanic employees, compared with white, across two survey periods.
The CALD Workforce and Labour and Migration Policies
Kuhlmann et al. (2020) sought to explore the situation of migrant carers in long-term care in European Union Member states, and the impact of disruptions caused by the COVID-19 pandemic. Long term care, labour migration and migrant carer policies were considered across Austria, Italy, Germany, Poland and Romania, and discussions were held at an expert meeting at the European Public Health (EPH) conference in Marseilles. The study found that most care is provided at home unpaid or by personal carers, however there was scarce data on care being provided at home and the number of migrant carers within countries. The provision of universal health care was not commensurate with access to LTC, and all countries and areas of LTC faced shortages of professional carers and nurses. The migration policies researched indicated that mobility flows of migrant carers were determined by government actions. Two policy recommendations were made: include LTC migrant professional care workers in public health and workforce research and develop European health workforce governance mechanisms which connect health system needs, health labour markets and individual migrant professional carers.
Discussion
There were common themes on the impact of COVID-19 on the workforce across studies, including high workload and workforce shortages, mental health impacts, collegiality and support felt by colleagues, and changing guidelines of governments. Frontline workers in RACFs experienced significant demands, changes to the nature of work undertaken and additional work as a result of COVID-19. The importance of institutional factors was also highlighted, including the relationship between working conditions (and use of agency staff) and COVID-19, provision of PPE and testing, good organisational communication and engagement strategies (i.e. especially for CALD workers) and effective leadership.
Many larger scale studies identified in this review were US cross-sectional studies which considered the association between COVID-19 and RACF staffing shortages. A range of studies have highlighted that workforce factors such as staffing levels, secure employment conditions and paid sick leave are important for infection prevention and control and ultimately reducing COVID-19 morbidity and mortality (Dykgraaf et al., 2021; Fisher et al., 2021; Frazer, et al., 2021; Rios et al., 2020; Werner & Coe, 2021). We found few studies that considered government policies and organisational factors that could assist in reducing stressors and retaining workers in RACFs, with only one European study examining the impact of aged care, migrant and labour market policies on the migrant carer workforce.
Where there was a focus at the organisational level, studies emphasised the importance of leadership and good organisational communication, training and support in infection prevention and control, good working conditions, and access to psychological support/counselling for staff during the COVID-19 pandemic. Given the high proportion of workers from CALD backgrounds, culturally tailored communication and engagement strategies and support should be considered in response to COVID-19.
Professional Roles
Few studies highlighted the relative impact of the COVID-19 pandemic upon different professional roles within the RAC sector. In Krzyzaniak et al.’s Australian study (2021), a higher proportion of registered nurses had experienced work-related stress related to COVID-19 when compared to other care assistants, and this may be related to the noted shortage of RN staff in Australian nursing homes. Gray et al.’s (2021) systematic review also found that nurses were more vulnerable to the mental health impact of COVID-19. However, Scheffler et al.’s (2022) US study on the experiences of nursing home assistants also found feelings of isolation and psychological stress amongst this group.
Retention, Knowledge and Support of the CALD Workforce
Despite the high number of staff from CALD backgrounds in RACFs, few studies considered the experience of these workers during the COVID-19 pandemic, whilst a scoping review that commenced prior to the pandemic focused on migrant carers’ dementia care experiences (Adebayo et al., 2020). Adebayo’s (2020) recommendation that policy responses must consider training and support needs of CALD workers, including the provision of specific training on dementia, is an important consideration during the COVID-19 pandemic, due to the high morbidity and mortality associated with COVID-19 for people with cognitive impairment including dementia (Azarpazhooh et al., 2020; Brown et al., 2020; Hardan et al., 2021; Keng et al., 2020; Numbers & Brodaty, 2021; Thomas, 2021; Zhang et al., 2021). The importance of face-to-face training for dementia, highlighted by Nakanishi et al.’s study (2021) may be more salient for migrant aged care workers, whilst tailored training programs (with language support) may also be required.
Other studies in this review suggested that workforce retention is associated with stressors associated with work-life balance and informal caring responsibilities (Cimarolli et al., 2022; Fisher et al., 2021; Tomaszewska et al., 2022). Many workers are likely to be involved in intergenerational caring roles, especially those from CALD backgrounds. The development of IPC and communication strategies for COVID-19 would ideally include an understanding of the work, social and family networks and responsibilities of staff and visitors in RACFs, along with the cultural diversity of the residents. Another area for future research is the relative impact of improved working conditions (and work-life balance) on CALD worker retention, career progression and COVID-19. Notably, the workforce from CALD backgrounds in the RAC sector in Australia is predominantly lower paid personal care workers (72% of CALD workers), as well as nurses (24%) and allied health professionals (Australian Government, 2021). According to the findings of Scheffler et al. (2022) care workers may require extra support to feel less isolated and reduce psychological stress.
Australian Government Policy
Due to workforce shortages and demand associated with the COVID-19 pandemic, the Australian government relaxed visa restrictions for those working in aged care. The Changes to Working Rules for People on Temporary Visas allowed an increase in the hours that international students working in aged care and nursing were permitted to work during the COVID-19 pandemic (Menzies Centre for Health Governance, 2021). Other Australian government measures included enabling workers whose visa was expiring, and who were unable to leave the country, to apply for a COVID-19 Pandemic event Temporary Activity Visa to stay up to 12 months if working in a critical sector, which included aged care (Menzies Centre for Health Governance, 2021). The Australian Government also established the CALD Communities COVID-19 Health Advisory Group, where the focus appeared to be strategies aimed at increasing vaccination rates in CALD communities, rather than strategies to support, train and maintain the aged care workforce from CALD backgrounds. There is scope for future research to consider the impact of these policies.
As the Australian government introduced mandatory vaccination for the aged care workforce, with agencies required to keep records on vaccination status and report to the government, the issue of vaccine hesitancy identified in US studies was less salient for Australia. The Australian Government also introduced an allowance for COVID-19, known as the Pandemic Leave Disaster Payment, for those who could not earn income during to self-isolation or quarantine associated with COVID-19, or needing to care for someone in self isolation or quarantine (Australian Government, 2022). This may have prevented the problems reported elsewhere regarding an association between absence of RACF staff paid sick leave and COVID-19 rates (Frazer et al., 2021).
One factor not considered within the workforce studies identified is how the reduction in volunteering impacted the RACF sector, and particularly those from CALD backgrounds (residents and staff). The 2020 Aged Care Workforce Census showed that in Australia, COVID-19 significantly impacted volunteering in the aged care workforce, with volunteering levels being half of what they were in 2016 (Australian Government, 2021). In 2019, the Australian government produced a guide for aged care providers to support older CALD people who were residents in aged care, and in 2020, the Australian National Ageing Research Institute produced a volunteers resource kit to assist in challenges encountered by older people from CALD backgrounds who are older volunteers. However, there is more scope to research how restricting volunteers in the aged care sector impacted the workforce and residents within the RAC sector during COVID-19, and the lasting impact these restrictions have had on the workforce and residents.
Recommendations from the ‘COVID-19 and Aged Care’ report associated with the Australian Royal Commission into Aged Care included the adequate provision of resourcing for staffing RACFs, including to deal with external visitors to enable more social engagement and the appointment of independent infection prevention and control officers (Australian Government, 2020). The Australian Association of Gerontology advocated for minimum staffing levels, holistic, multi-disciplinary care with needs assessments being done by interdisciplinary teams, and workforce planning (Australian Association of Gerontology, 2020). Improved training (through supervision, mentoring/student placements and professional development opportunities), renumeration and conditions for staff were also advocated for (Australian Association of Gerontology, 2020).
The Australian Government has recently passed new aged care legislation in response to the Royal Commission into Aged Care Quality and Safety; the Aged Care and Other Legislation Amendment (Royal Commission Response No. 1 and Response No. 2) Act 2021. Amongst reforms, there will be a new system for calculating aged care basic subsidies, new governance responsibilities for the sector, restrictive practices are to be used as a ‘last resort,’ a code of conduct will be implemented, a registered nurse at RACFs on site at all times, and a star-rating systems is to be introduced. Notably, a review by Konetzka et al. (2021) found no relationship between the externally rated quality of nursing home facilities (5-star ratings) in the US and COVID-19 outcomes.
Limitations
Limitations of this review include that it was part of a broader systematic scoping review which did not assess the quality of individual research studies. The quality of studies included in this review varied, and many studies were small qualitative studies with small numbers of participants. There were only two systematic reviews included. Twenty-two of the twenty-six articles included in this review were from the United States (13) and Europe (9), with only six papers from other countries and regions.
Conclusion
This review highlighted the impact of COVID-19 upon the RACF workforce, where a high proportion of workers are from CALD backgrounds. Impacts were related to staffing shortages and high workloads, increased workplace stressors and work-life balance issues, associated with mental health concerns, staff resignation and intention to quit the profession. The review highlighted the need to support all RACF workers, via pandemic preparedness and response training, and particularly CALD workers (for example, face to face training on responding to people with cognitive impairment who have COVID-19), and the need to provide mental health support for all staff. Australian government policies have focused upon increasing vaccination rates amongst the CALD community and boosting the aged care sector workforce. More recently, new legislation has been passed which will require new governance arrangements for the aged care sector, minimum funding for the sector, a code of conduct and using restrictive practices as a ‘last resort.’ There remains scope to improve the identification of training needs and support of the RAC workforce, including from CALD backgrounds, and to provide mental health support, to retain the workforce and facilitate worker and resident wellbeing.
Data Availability
Data is available from the Brightwater Research Centre, Brightwater Care Group.
References
Adebayo, B., Nichols, P., Albrecht, M. A., Brijnath, B., & Heslop, K. (2021). Investigating the impacts of acculturation stress on migrant care workers in australian residential aged care facilities. Journal of Transcultural Nursing, 32(4), 389–398. https://doi.org/10.1177/1043659620947810
Adebayo, B., Nichols, P., Heslop, K., & Brijnath, B. (2020). A scoping review of dementia care experiences in migrant aged care workforce. The Gerontologist, 60(2), e105–e116. https://doi.org/10.1093/geront/gnz027
Aged Care Workforce Strategy Taskforce. (2018). A matter of care: Australia’s aged care workforce strategy: report of the Aged Care Workforce Strategy Taskforce. Canberra: Australian Government.
Antelius, E., & Plejert, C. (2016). Ethnoculturally-profiled care: Dementia caregiving targeted towards Middle Eastern immigrants living in Sweden. Anthropology & Aging, 37, 9–26. https://doi.org/10.5195/aa.2016.107
Australian Association of Gerontology. (2020). AAG Position Paper: Aged are workforce, funding and governance. Retrieved July 1, 2022, from https://www.aag.asn.au/news-publications/policy-papers/aag-position-paper-aged-care-workforce-funding-and-governance
Australian Government. (2020). Royal commission into aged care quality and safety (September 2020): Aged care and COVID-19: a special report. Canberra, Australia: Australian Government.
Australian Government. (2021). 2020 Aged care workforce census report. Canberra, Australia: Australian Government. Retrieved July 1, 2022, from https://www.health.gov.au/resources/publications/2020-aged-care-workforce-census
Australian Government. (2022). Pandemic leave disaster payment. Retrieved July 1, 2022 from https://www.servicesaustralia.gov.au/pandemic-leave-disaster-payment?context=60352
Azarpazhooh, M. R., Amiri, A., Morovatdar, N., Steinwender, S., Rezaei Ardani, A., Yassi, N., Biller, J., Stranges, S., Belasi, M. T., Neya, S. K., Khorram, B., Andalibi, M. S. S., Arsang-Jang, S., Mokhber, N., & Di Napoli, M. (2020). Correlations between COVID-19 and burden of dementia: An ecological study and review of literature. Journal of the Neurological Sciences, 416, 117013. https://doi.org/10.1016/j.jns.2020.117013
Battams, S., & Martini, A. (2023). The impact of the COVID-19 pandemic on people with cognitive impairment residing in aged care facilities: An integrative review. INQUIRY: The Journal of Health Care Organization, Provision, and Financing, 60, 00469580231160898. https://doi.org/10.1177/00469580231160898
Brown, E. E., Kumar, S., Rajji, T. K., Pollock, B. G., & Mulsant, B. H. (2020). Anticipating and mitigating the impact of the COVID-19 pandemic on alzheimer’s disease and related dementias. American Journal of Geriatric Psychiatry, 28(7), 712–721. https://doi.org/10.1016/j.jagp.2020.04.010
Brydon, A., Bhar, S., Doyle, C., Batchelor, F., Lovelock, H., Almond, H., & Wuthrich, V. (2022). National survey on the impact of COVID-19 on the mental health of australian residential aged care residents and staff. Clinical Gerontology, 45(1), 58–70. https://doi.org/10.1080/07317115.2021.1985671
Cimarolli, V. R., Bryant, N. S., Falzarano, F., & Stone, R. (2022). Job resignation in nursing homes during the COVID-19 pandemic: The role of quality of employer communication. Journal of Applied Gerontology, 41(1), 12–21. https://doi.org/10.1177/07334648211040509
Dykgraaf, S. H., Matenge, S., Desborough, J., Sturgiss, E., Dut, G., Roberts, L., McMillan, A., & Kidd, M. (2021). Protecting nursing homes and long-term care facilities from COVID-19: A rapid review of international evidence. Journal of the American Medical Directors Association, 22(10), 1969–1988. https://doi.org/10.1016/j.jamda.2021.07.027
Feifer, R. A., Bethea, L., & White, E. M. (2021). Racial disparities in COVID-19 vaccine acceptance: Building trust to protect nursing home staff and residents. Journal of the Americal Medical Directors Association, 22(9), 1853-1855.e1851. https://doi.org/10.1016/j.jamda.2021.07.006
Fisher, E., Cárdenas, L., Kieffer, E., & Larson, E. (2021). Reflections from the “Forgotten Front Line”: A qualitative study of factors affecting wellbeing among long-term care workers in New York City during the COVID-19 pandemic. Geriatric Nursing, 42(6), 1408–1414. https://doi.org/10.1016/j.gerinurse.2021.09.002
Frazer, K., Mitchell, L., Stokes, D., Lacey, E., Crowley, E., & Kelleher, C. C. (2021). A rapid systematic review of measures to protect older people in long-term care facilities from COVID-19. British Medical Journal Open, 11(10), e047012. https://doi.org/10.1136/bmjopen-2020-047012
Gaur, S., Kumar, R., Gillespie, S. M., & Jump, R. L. P. (2022). Integrating principles of safety culture and just culture into nursing homes: lessons from the pandemic. Journal of the Americal Medical Directors Association, 23(2), 241–246. https://doi.org/10.1016/j.jamda.2021.12.017
Gilbert, G. L. (2020). COVID-19 in a Sydney nursing home: A case study and lessons learnt. Medical Journal of Australia, 213(9), 393-396.e391. https://doi.org/10.5694/mja2.50817
Giri, S., Chenn, L. M., & Romero-Ortuno, R. (2021). Nursing homes during the COVID-19 pandemic: A scoping review of challenges and responses. European Geriatric Medicine, 12(6), 1127–1136. https://doi.org/10.1007/s41999-021-00531-2
Gray, K. L., Birtles, H., Reichelt, K., & James, I. A. (2021). The experiences of care home staff during the COVID-19 pandemic: A systematic review. Aging and Mental Health, 1–10. https://doi.org/10.1080/13607863.2021.2013433
Greene, T., Harju-Seppänen, J., Adeniji, M., Steel, C., Grey, N., Brewin, C. R., Bloomfield, M. A., & Billings, J. (2021). Predictors and rates of PTSD, depression and anxiety in UK frontline health and social care workers during COVID-19. European Journal of Psychotraumatology, 12(1), 1882781. https://doi.org/10.1101/2020.10.21.20216804
Hardan, L., Filtchev, D., Kassem, R., Rim, B., Lukomska-Szymanska, M., Tarhini, H., Salloum-Yared, F., Mancino, D., Kharouf, N., & Haikel, Y. (2021). COVID-19 and Alzheimer’s Disease: A Literature Review. Medicina, 57(11), 1159. https://doi.org/10.3390/medicina57111159
Harrington, C., Ross, L., Chapman, S., Halifax, E., Spurlock, B., & Bakerjian, D. (2020). Nurse staffing and coronavirus infections in california nursing homes. Policy Politics and Nursing Practice, 21(3), 174–186. https://doi.org/10.1177/1527154420938707
Hoedl, M., Thonhofer, N., & Schoberer, D. (2022). COVID-19 pandemic: Burdens on and consequences for nursing home staff. Journal of Advanced Nursing. https://doi.org/10.1111/jan.15193
Hung, L., Yang, S. C., Guo, E., Sakamoto, M., Mann, J., Dunn, S., & Horne, N. (2022). Staff experience of a Canadian long-term care home during a COVID-19 outbreak: A qualitative study. BMC Nursing, 21(1), 45. https://doi.org/10.1186/s12912-022-00823-3
Johnston, F. H., Anderson, T., Harlock, M., Castree, N., Parry, L., Marfori, T., McPherson, M., Veitch, M., Smith, K. J., & Stephens, N. (2021). Lessons learnt from the first large outbreak of COVID-19 in health-care settings in Tasmania. Australia. Western Pacific Surveillance Response J, 12(4), 1–7. https://doi.org/10.5365/wpsar.2021.12.4.884
Keng, A., Brown, E. E., Rostas, A., Rajji, T. K., Pollock, B. G., Mulsant, B. H., & Kumar, S. (2020). Effectively caring for individuals with behavioral and psychological symptoms of dementia during the COVID-19 Pandemic. Frontiers in Psychiatry, 11, 573367. https://doi.org/10.3389/fpsyt.2020.573367
Konetzka, R. T., White, E. M., Pralea, A., Grabowski, D. C., & Mor, V. (2021). A systematic review of long-term care facility characteristics associated with COVID-19 outcomes. Journal of the American Geriatric Society, 69(10), 2766–2777. https://doi.org/10.1111/jgs.17434
Krzyzaniak, N., Scott A, Bakhit M, Bryant A, Taylor M, & C., D. M. (2021). Impact of the COVID-19 pandemic on the Australian residential aged care facility (RACF) workforce. Australian Journal of Advanced Nursing. 2021 Aug. 26.
Kuhlmann, E., Falkenbach, M., Klasa, K., Pavolini, E., & Ungureanu, M. I. (2020). Migrant carers in Europe in times of COVID-19: a call to action for European health workforce governance and a public health approach. European Journal of Public Health, 30(Supplement_4), iv22–iv27. https://doi.org/10.1093/eurpub/ckaa126
Lingum, N. R., Sokoloff, L. G., Meyer, R. M., Gingrich, S., Sodums, D. J., Santiago, A. T., Feldman, S., Guy, S., Moser, A., Shaikh, S., Grief, C. J., & Conn, D. K. (2021). Building long-term care staff capacity during COVID-19 through just-in-time learning: evaluation of a modified ECHO model. Journal of the Americal Medical Directors Association, 22(2), 238-244.e231. https://doi.org/10.1016/j.jamda.2020.10.039
Menzies Centre for Health Governance. (2021). Australian COVID-19 policy responses: A health equity report card. Retried July 1, 2022, from https://regnet.anu.edu.au/node/8438
Nakanishi, M., Yamasaki, S., Endo, K., Niimura, J., Ziylan, C., Bakker, T. J. E., Granvik, E., Nagga, K., & Nishida, A. (2021). e-learning and web-based tools for psychosocial interventions addressing neuropsychiatric symptoms of dementia during the COVID-19 pandemic in Tokyo, Japan: Quasi-experimental study. JMIR Medical Education, 7(4), e30652. https://doi.org/10.2196/30652
National Health and Medical Research Council. (NHMRC). (2009). NHMRC levels of evidence and grades for recommendations for developers of guidelines. Canberra: National Health and Medical Research Council.
Niznik, J. D., Harrison, J., White, E. M., Syme, M., Hanson, L. C., Kelley, C. J., Porter, L., & Berry, S. D. (2022). Perceptions of COVID-19 vaccines among healthcare assistants: A national survey. Journal of the American Geriatrics Society, 70(1), 8–18. https://doi.org/10.1111/jgs.17437
Numbers, K., & Brodaty, H. (2021). The effects of the COVID-19 pandemic on people with dementia. Nature Reviews. Neurology, 17(2), 69–70. https://doi.org/10.1038/s41582-020-00450-z
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., & Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 2021(372), n71. https://doi.org/10.1136/bmj.n71
Pförtner, T. K., Pfaff, H., & Hower, K. I. (2021). Will the demands by the covid-19 pandemic increase the intent to quit the profession of long-term care managers? A repeated cross-sectional study in Germany. Journal of Public Health (oxf), 43(3), e431–e434. https://doi.org/10.1093/pubmed/fdab081
Riello, M., Purgato, M., Bove, C., MacTaggart, D., & Rusconi, E. (2020). Prevalence of post-traumatic symptomatology and anxiety among residential nursing and care home workers following the first COVID-19 outbreak in Northern Italy. Royal Society Open Science, 7(9), 200880. https://doi.org/10.1098/rsos.200880
Rios, P., Radhakrishnan, A., Williams, C., Ramkissoon, N., Pham, B., Cormack, G. V., Grossman, M. R., Muller, M. P., Straus, S. E., & Tricco, A. C. (2020). Preventing the transmission of COVID-19 and other coronaviruses in older adults aged 60 years and above living in long-term care: A rapid review. Systematic Reviews, 9(1), 218. https://doi.org/10.1186/s13643-020-01486-4
Sarabia-Cobo, C., Pérez, V., de Lorena, P., Hermosilla-Grijalbo, C., Sáenz-Jalón, M., Fernández-Rodríguez, A., & Alconero-Camarero, A. R. (2021). Experiences of geriatric nurses in nursing home settings across four countries in the face of the COVID-19 pandemic. Journal of Advanced Nurings, 77(2), 869–878. https://doi.org/10.1111/jan.14626
Scheffler, B., Petruccelli, K., Baughman, A. W., Yurkofsky, M., Lipsitz, L. A., & Lau-Ng, R. (2022). Fighting the COVID-19 nursing home crisis: The untold story of the nursing assistants. Journal of the American Geriatrics Society, 70(2), 379–383. https://doi.org/10.1111/jgs.17515
Senczyszyn, A., Lion, K. M., Szcześniak, D., Trypka, E., Mazurek, J., Ciułkowicz, M., Mackowiak, M., Duda-Sikula, M., Wallner, R., & Rymaszewska, J. (2020). Mental health impact of SARS-COV-2 pandemic on long-term care facility personnel in Poland. Journal of the Americal Medical Directors Association, 21(11), 1576–1577. https://doi.org/10.1016/j.jamda.2020.09.020
Shrader, C. D., Assadzandi, S., Pilkerton, C. S., & Ashcraft, A. M. (2021). Responding to a COVID-19 Outbreak at a long-term care facility. Journal of Applied Gerontology, 40(1), 14–17. https://doi.org/10.1177/0733464820959163
Spilsbury, K., Devi, R., Griffiths, A., Akrill, C., Astle, A., Goodman, C., Gordon, A., Hanratty, B., Hodkinson, P., Marshall, F., Meyer, J., & Thompson, C. (2021). Seeking answers for care homes during the COVID-19 pandemic (COVID SEARCH). Age and Ageing, 50(2), 335–340. https://doi.org/10.1093/ageing/afaa201
Thomas, R. E. (2021). Reducing Morbidity and Mortality Rates from COVID-19, Influenza and pneumococcal illness in nursing homes and long-term care facilities by Vaccination and comprehensive infection control interventions. Geriatrics, 6(2), 48. https://doi.org/10.3390/geriatrics6020048
Tomaszewska, K., Majchrowicz, B., & Delong, M. (2022). Impact of SARS-CoV-2 Pandemic on psychosocial burden and job satisfaction of long-term care nurses in Poland. International Journal of Environmental Research and Public Health, 19(6), 3555. https://doi.org/10.3390/ijerph19063555
Werner, R. M., & Coe, N. B. (2021). Nursing home staffing levels did not change significantly during COVID-19. Health Affairs (millwood), 40(5), 795–801. https://doi.org/10.1377/hlthaff.2020.02351
White, E. M., Wetle, T. F., Reddy, A., & Baier, R. R. (2021). Front-line nursing home staff experiences during the COVID-19 pandemic. Journal of the American Medical Directors Association, 22(1), 199–203. https://doi.org/10.1016/j.jamda.2020.11.022
WHO. (2018). Communicating risk in public health emergencies. World Health Organization.
Xu, H., Intrator, O., & Bowblis, J. R. (2020). Shortages of staff in nursing homes during the COVID-19 pandemic: What are the driving factors? Journal of the American Medical Directors Association, 21(10), 1371–1377. https://doi.org/10.1016/j.jamda.2020.08.002
Yang, B. K., Carter, M. W., & Nelson, H. W. (2021). Trends in COVID-19 cases, deaths, and staffing shortages in US nursing homes by rural and urban status. Geriatric Nursing, 42(6), 1356–1361. https://doi.org/10.1016/j.gerinurse.2021.08.016
Yau, B., Vijh, R., Prairie, J., McKee, G., & Schwandt, M. (2021). Lived experiences of frontline workers and leaders during COVID-19 outbreaks in long-term care: A qualitative study. American Journal of Infection Control, 49(8), 978–984. https://doi.org/10.1016/j.ajic.2021.03.006
Zhang, X.-M., Jiao, J., Cao, J., Xiao-Peng, H., Chen, Z., Xin-Juan, W., & Xiao-Hua, X. (2021). Frailty as a predictor of mortality among patients with COVID-19: A systematic review and meta-analysis. BMC Geriatrics, 21, 1–11. https://doi.org/10.1186/s12877-021-02138-5
Acknowledgements
Funder: Lotterywest. Study partners—Brightwater Care Group, Bethanie, Amana Living, Baptist Care, and Juniper.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions LotteryWest.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interests
All authors declare no conflict of interest.
Informed Consent
None.
Ethical Treatment of Experimental Subjects (Animals and Humans)
No experimental treatment was conducted on either human or animal subjects in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Battams, S., Martini, A. Impact of COVID-19 on the Residential Aged Care Workforce, and Workers From Culturally and Linguistically Diverse Backgrounds: A Rapid Literature Review. Ageing Int (2024). https://doi.org/10.1007/s12126-023-09546-5
Accepted:
Published:
DOI: https://doi.org/10.1007/s12126-023-09546-5