
Abstract
Objective
To evaluate the pediatric residents’ cardiopulmonary resuscitation (CPR) skills, and their improvements after recorded video feedbacks.
Methods
Pediatric residents from a university hospital were enrolled. The authors surveyed the level of pediatric resuscitation skill confidence by a questionnaire. Eight psychomotor skills were evaluated individually, including airway, bag-mask ventilation, pulse check, prompt starting and technique of chest compression, high quality CPR, tracheal intubation, intraosseous, and defibrillation. The mock code skills were also evaluated as a team using a high-fidelity mannequin simulator. All the participants attended a concise Pediatric Advanced Life Support (PALS) lecture, and received video-recorded feedback for one hour. They were re-evaluated 6 wk later in the same manner.
Results
Thirty-eight residents were enrolled. All the participants had a moderate to high level of confidence in their CPR skills. Over 50 % of participants had passed psychomotor skills, except the bag-mask ventilation and intraosseous skills. There was poor correlation between their confidence and passing the psychomotor skills test. After course feedback, the percentage of high quality CPR skill in the second course test was significantly improved (46 % to 92 %, p = 0.008).
Conclusions
The pediatric resuscitation course should still remain in the pediatric resident curriculum and should be re-evaluated frequently. Video-recorded feedback on the pitfalls during individual CPR skills and mock code case scenarios could improve short-term psychomotor CPR skills and lead to higher quality CPR performance.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
A cardiopulmonary resuscitation course is highly recommended for all medical healthcare providers, especially for the medical trainees. The American Heart Association (AHA) recommends the Pediatric Advanced Life Support (PALS) course in the US Pediatric Residency Training Programs [1]. Pediatric residents are the first frontiers to perform cardiopulmonary resuscitation (CPR) in pediatric patients with in-hospital cardiac arrest. A previous study demonstrated that pediatric residents have inadequate experience of real instances of pediatric cardiopulmonary arrests [2]. A study evaluating pediatric residents in a tertiary care center using a high-fidelity mannequin simulator program demonstrated that pediatric residents delay starting chest compression according to the AHA’s standard [3]. Therefore, the PALS course is crucial in Pediatric Residency Training Program. Advanced resuscitation courses consist of both cognitive knowledge and psychomotor skills. A prior study measured the resuscitation knowledge and performance in the two groups of pediatric residents and showed more pediatric residents in the intervention group passing basic or advanced airway skills [4]. Studies have shown that PALS courses improve knowledge [5, 6], and enhance pediatric residents’ cognitive knowledge but have variable effects on psychomotor skills [7, 8]. A few studies have shown improvement of the psychomotor skill of pediatric residents before and immediately after completing a PALS course [9, 10]. In 2010, the AHA implemented new PALS guidelines [11]. Several new training methods have been implemented to improve the confidence, knowledge, competency, or psychomotor skills, including e-learning, screen-based simulation, and video-assisted real time simulation. However, one training method could enhance only some skills [10, 12, 13]. The authors’ institute provides a two-day PALS course for new residents, which includes lectures, skill stations, core case simulation, and mega code stations. However, the authors believe that practice and learning from errors could possibly increase both knowledge and psychomotor skills. To the best of authors’ knowledge, no study has previously evaluated pediatric residents’ psychomotor skills through a PALS course combined with teaching, and video recording pitfalls feedback. This study was aimed to evaluate the resuscitation skills of pediatric residents and their performances as team concept in the simulated case scenario mock code, and their improvements after recorded video feedback for their pitfalls.
Material and Methods
The study was performed at Ramathibodi Hospital, a tertiary care academic center. It is a regional referral center for pediatric subspecialty care in Thailand. There are a 10-bed tertiary non-cardiac PICU and a 11-bed intermediate ward. Also there are approximately 5000 annual pediatric admissions; 70,000 outpatient visits; and 600 PICU admissions. Pediatric residents were invited to participate. At the time of study, there were 45 pediatric trainees which included 15 of first-year (PG1), 15 of second-year (PG2), and 15 of third-year (PG3) pediatric residents. All participants attended a two-day PALS course. This study was approved by the Institutional Review Board (IRB) of authors’ center and all participants provided their written consents.
All the participants completed the questionnaire, rating their level of confidence with pediatric resuscitation skills on a scale of 1 (not at all confident) to 10 (extremely confident), the number of CPR courses attended, the number of CPRs performed in real situations, as well as the number of intubations performed, intraosseous line (IO) placements, and defibrillations.
The following model of the CPR training was created:
-
1.
The evaluation test (the first course test): All participants were grouped into teams; each team composed of 3 pediatric residents (mixing of PG1, PG2, PG3) and each team was allowed 30 min for evaluation test (Fig. 1).
-
1.1)
Each individual resident was rotated for each individual test (5-min interval of each station) and was evaluated on his/her performances on 8 psychomotor skills at 3 stations, composed of Station A: performing basic life support (BLS) for testing skills consisting of:
Fig. 1 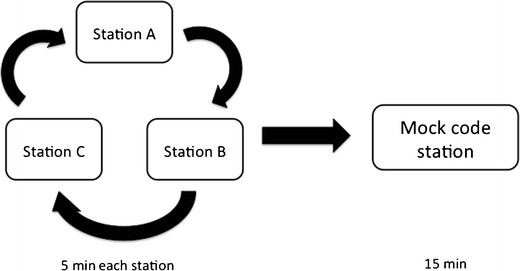
Diagram showing the rotation of the evaluation test
-
1) opening and maintaining of airway, 2) adequate ventilation by bag-mask ventilation, 3) pulse check within 10 s, 4) technique of chest compression, and 5) high quality CPR (push hard, push fast, full chest recoil); Station B: for testing skills including 6) tracheal intubation and 7) intraosseous (IO) skills, and Station C: for testing 8) defibrillation skill. These 8 skill tests used a Laerdal infant mannequin with inflatable lungs®, a mannequin head with an intubatable airway, a mannequin with an artificial tibia for IO placement or a mannequin with an electrocardiography display (Zoll M series®). All these 3 stations had single certified-PALS instructor in each station to evaluate and score these skill tests with direct feedback on residents’ performances at the end of each test.
-
-
1.2)
All the 3 residents who were grouped as one team performed together at the mock code station (Station D) for 15 min. There was one nurse who assisted airway and breathing with Ambu-bag® on the command of the team leader but did not give any advice on patient management. The Laerdal SimMan® human mannequin simulator was used for the mock code station. Each team was asked to evaluate a case scenario: A 6-y-old boy with severe pneumonia, intubated and connected with a ventilator support in the pediatric intensive care unit, developed sudden cyanosis. The script included a standardized progression depending on resident’s actions and was based on the 2010 AHA-PALS guidelines. The mock code station had a similar scenario for every group. Data were collected on seven tasks which composed of 1) rapid assessment using the mnemonic DOPE (displacement of tube, obstruction of tube, pneumothorax, and equipment failure) for mechanically ventilated patients who deteriorates, 2) high quality CPR, 3) recognition of ventricular arrhythmias, 4) proper defibrillation, 5) minimal interruption of chest compression, 6) correct medication used, and 7) discovery of reversible causes. Each task had clearly defined criteria with agreement by the study group. Video recording was done during performance in the mock code station in all the groups. Performance was scored independently by two certified-PALS instructors using standardized checklist scoring as pass or fail. After completing the mock code station, participants received direct feedback on their performances by these two instructors.
-
1.1)

-
2.
One week later, participants attended a one hour course, composed of common pitfalls of their performances, and scenario video indicating their common pitfalls during case scenario.
-
3.
Six weeks later, the second course test was conducted in the same manner as the first course test with the same observers, except that the mock code skill station scenario was different from the first course test but similar checklist, participants’ team, and two independent observers were used.
Statistical analysis was performed using the R, version 2.8.1 (www.R-project.org), and SPSS, version 16 (SPSS Inc. Chicago Illinois), statistical software packages. Descriptive analyses were performed for baseline characteristics and pretest questionnaires. Parametric continuous variables were described as median and range. Categorical variables were expressed as number of patients and percentage. Comparisons between the groups were analyzed with Pearson’s chi-square test for categorical variables and with the Mann-Whitney U statistic test for nonparametric continuous variables. Paired samples t-test was used to compare pre- and post-test pass-fail score differences. Cohen’s Kappa test was used to assess inter-observer agreement for mock code station, and was calculated by constructing 2 × 2 tables for pre- and post-test. The interpretation of kappa values was based on Landis and Koch’s [14] guidelines, which recommends values between 0 and 0.20 represent poor agreement, 0.21–0.40 represent fair agreement, 0.41–0.60 represent moderate agreement, 0.61–0.80 represent good agreement, and 0.81–1.00 represent very good agreement. A p < 0.05 was considered statistically significant.
Results
Overall, 38 of 45 (79 %) pediatric residents [15 (PG1), 12 (PG2), and 11 (PG3)] completed all the 4 skill stations of first and second course tests respectively. The median age of participants was 28 y and 34 were females.
According to the questionnaire survey, all the participants had performed cardiopulmonary resuscitation in the past year. Most CPRs occurred in the pediatric intensive care unit. All the participants had performed intubation in real patients at least once, but only 15 of 38 (39 %) had performed this skill more than 5 times. Interestingly, most PG1 and PG2 had never performed IO placement (93 % and 75 % respectively) and defibrillation (93 % and 75 % respectively) whereas most PG3 (91 %) had performed these procedures (91 % and 73 % respectively). All the participants had moderate to high level of confidence of their CPR skills before the first course test (Table 1).
Of the 8 psychomotor skills, more than 50 % of participants passed these skills which included the opening and maintaining of airway (61 %), prompt starting and technique of chest compression (71 %), and tracheal intubation (68 %) (Fig. 2). Only 29 % of the participants passed the bag-mask ventilation and IO placement skill in the first course test. When the psychomotor skill and the confidence in CPR skills were compared by a questionnaire survey, there were poor correlations between the confidence and psychomotor skills including the technique of chest compression, defibrillation, and intraosseous line placement, (r2 = 0.399, 0.497, and 0.427 respectively).

Bar graph showing percentage of pediatric residents (n = 38) passing each of 8 psychomotor cardiopulmonary resuscitation skill tests as compared between the first and second courses tests
Importantly, most individual skills including opening and maintaining airway, bag-mask ventilation, pulse check, defibrillation, and IO skills statistically significantly improved after course feedback (p < 0.05) (Fig. 2). However, only 66 % and 68 % of participants passed IO and high quality CPR, respectively after course feedback (Fig. 2). Subgroup analysis demonstrated that 53 %, 75 %, and 82 % of PG1, PG2, and PG3 passed the high quality CPR test after course feedback, respectively.
For mock code skill station (Table 2), there was a good inter-observer agreement between 2 independent observers in all 8 task assessments (kappa =0.701, 95%CI 0.572–0.830). Most teams passed the categories: correct medication (100 %), recognition of ventricular fibrillation (92 %), proper defibrillation (92 %), resuming of chest compression after defibrillation (85 %) whereas only 69 % passed finding of reversible causes, only 46 % passed rapid assessment and high quality CPR.
After course feedback, the second course test demonstrated that the percentage of team passing the high quality CPR concept (push hard, push fast, and full chest recoil) increased from 46 % to 92 %, p = 0.008 whereas the percentages of team passing rapid assessment and finding reversible causes showed no significant improvement.
Discussion
The incidence of in-hospital pediatric cardiac arrest is low but the overall mortality rate is still high [15, 16]. Successful CPR relies on several factors, including the causes of cardiac arrest, the duration of initial resuscitation, and the experience of health care providers [17, 18]. PALS course is mandatory for health care providers especially during the pediatric training program. Evidence demonstrates substantial retention loss within 1 y after successful completion of the PALS course [19]. Prior studies have shown that the knowledge could be retained longer than the psychomotor skills [20]. Other studies have shown that repeated exposure or feedback improve competency in communication, professional, or criteria-based tasks [21, 22]. Regular update on pediatric resuscitation is necessary for pediatric residency training [23]. The index study demonstrated that pediatric residents had moderate to high level of confidences in the CPR questionnaire survey of pediatric residents. However, more than 50 % of pediatric residents failed the psychomotor skills in the first course test. This is consistent with a previous study which demonstrated that resuscitation experience without feedback increases confidence but does not increase competence [24]. The index study also demonstrated that several months after a two-day PALS course, 60 % of pediatric residents passed only two of eight CPR skills including tracheal intubation and technique of chest compression. This clearly demonstrates that a two-day PALS course at the beginning of the pediatric residency-training program is inadequate. After course feedback using concise direct feedback, and video recording for the pitfalls, most psychomotor skills could be improved. However, less than 75 % of pediatric residents passed IO skill test after this feedback. As IO placement is one of the most important procedures in fluid and medication management of pediatric resuscitation, the authors recommend adding IO workshop training in the pediatric residents’ curriculum and this skill should be re-evaluated periodically to ascertain that all pediatric residents could perform IO placement in real situation. In the same direction as individual CPR skills, the high quality CPR in the mock code station after course feedback got significantly improved. The 2015 AHA guidelines for cardiopulmonary resuscitation still emphasize on high quality CPR [25]. From the index study, the authors recommend the use of training model including individual CPR skill tests, mock code scenario test, concise lecture on PALS, direct feedback, and video feedback of the pitfalls in addition to standard PALS course. The rapid assessment and finding of reversible causes should be emphasized during feedback. There are many limitations; first, according to the inherence to a non-randomized control and cross-sectional survey, the possibility of memory recall bias from the first course performance skewed the results toward better second course performance. Nevertheless, as the duration between the pre- and post-test was 6 wk and the case scenario was changed in the post-test mock code station, this bias might have been reduced. Second, the checklists used to measure psychomotor and mock code skills have not been validated prior to this study. However, these checklists were adapted according to PALS guidelines by the consensus of 4 PALS certified instructors. Furthermore, the observers used the same instructions in the pre- and post-test checklists. Finally, this model of CPR training can not be generalized to other institutions since it has been evaluated only in a single program at a tertiary university hospital and only included a small number of pediatric residents. However, this method of resuscitation education can improve the procedural skills in pediatric residency training. Further follow up on rate of successful real CPR would be the ultimate outcome measurement.
Conclusions
The confidence of pediatric residents on their CPR skills did not correlate with their psychomotor CPR skills. The pediatric resuscitation course should still remain in the pediatric resident curriculum and should be re-evaluated frequently. PALS course alone, before starting the pediatric residency training program might not be adequate for maintaining CPR skills during the training. Video recording feedbacks on the pitfalls during individual CPR skills and mock code case scenario can improve short-term psychomotor CPR skills, leading to high quality CPRs.
References
Halamek LP, Kaegi DM. Who's teaching neonatal resuscitation to housestaff? Results of a national survey. Pediatrics. 2001;107:249–55.
Hunt EA, Patel S, Vera K, Shaffner DH, Pronovost PJ. Survey of pediatric resident experiences with resuscitation training and attendance at actual cardiopulmonary arrests. Pediatr Crit Care Med. 2009;10:96–105.
Hunt EA, Vera K, Diener-West M, et al. Delays and errors in cardiopulmonary resuscitation and defibrillation by pediatric residents during simulated cardiopulmonary arrests. Resuscitation. 2009;80:819–25.
Nadel FM, Lavelle JM, Fein JA, Giardino AP, Decker JM, Durbin DR. Teaching resuscitation to pediatric residents: the effects of an intervention. Arch Pediatr Adolesc Med. 2000;154:1049–54.
Waisman Y, Amir L, Mimouni M. Does the pediatric advanced life support course improve knowledge of pediatric resuscitation? Pediatr Emerg Care. 2002;18:168–70.
Soltani AE, Khan ZH, Arbabi S, Hossini B, Nahvi H, Agamohammadi A. Evaluation of pediatric CPR course on knowledge of pediatric residents–before and after ACLS course. Middle East J Anesthesiol. 2009;20:89–92.
White JR, Shugerman R, Brownlee C, Quan L. Performance of advanced resuscitation skills by pediatric housestaff. Arch Pediatr Adolesc Med. 1998;152:1232–5.
Nadel FM, Lavelle JM, Fein JA, Giardino AP, Decker JM, Durbin DR. Assessing pediatric senior residents' training in resuscitation: fund of knowledge, technical skills, and perception of confidence. Pediatr Emerg Care. 2000;16:73–6.
Quan L, Shugerman RP, Kunkel NC, Brownlee CJ. Evaluation of resuscitation skills in new residents before and after pediatric advanced life support course. Pediatrics. 2001;108:E110.
Biese KJ, Moro-Sutherland D, Furberg RD, et al. Using screen-based simulation to improve performance during pediatric resuscitation. Acad Emerg Med. 2009;16:S71–5.
Kleinman ME, Chameides L, Schexnayder SM, et al. Part 14: pediatric advanced life support: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122:S876–908.
Coolen EH, Draaisma JM, Hogeveen M, Antonius TA, Lommen CM, Loeffen JL. Effectiveness of high fidelity video-assisted real-time simulation: a comparison of three training methods for acute pediatric emergencies. Int J Pediatr. 2012;2012:709569.
O'Leary FM. Pediatric resuscitation training: is e-learning the answer? A before and after pilot study. J Paediatr Child Health. 2012;48:529–33.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–74.
Hickey RW, Cohen DM, Strausbaugh S, Dietrich AM. Pediatric patients requiring CPR in the prehospital setting. Ann Emerg Med. 1995;25:495–501.
Berg MD, Schexnayder SM, Chameides L, et al. Pediatric basic life support: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Pediatrics. 2010;126:e1345–60.
Kuisma M, Suominen P, Korpela R. Paediatric out-of-hospital cardiac arrests epidemiology and outcome. Resuscitation. 1995;30:141–50.
Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. J Am Med Assoc. 2006;295:50–7.
Wolfram RW, Warren CM, Doyle CR, Kerns R, Frye S. Retention of pediatric advanced life support (PALS) course concepts. J Emerg Med. 2003;25:475–9.
Patel J, Posencheg M, Ades A. Proficiency and retention of neonatal resuscitation skills by pediatric residents. Pediatrics. 2012;130:515–21.
Hodder RV, Rivington RN, Calcutt LE, Hart IR. The effectiveness of immediate feedback during the objective structured clinical examination. Med Educ. 1989;23:184–8.
Derstine PL. Implementing goals for non-cognitive outcomes within a basic science course. Acad Med. 2002;77:931–2.
Ahmed M, Pai B, Reynolds T. Retention of knowledge of the pediatric life support guidelines. J Coll Physicians Surg Pak. 2012;22:194–5.
Marteau TM, Wynne G, Kaye W, Evans TR. Resuscitation: experience without feedback increases confidence but not skill. BMJ. 1990;300:849–50.
de Caen AR, Berg MD, Chameides L, et al. Part 12: pediatric advanced life support: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S526–42.
Acknowledgments
The authors would like to acknowledge CPR training center, Faculty of Medicine Ramathibodi Hospital, Ploypan Insub, and Anchalee Leejakpai for their contributions in preparation of all the mannequins and equipments used in the skill stations; Duangrudee Wattanasirichaigoon (program director of Pediatric Residency Training Program) for allowing them to perform this study with Pediatric residents.
Contributions
NA: Design of the study, carried out data collection, data analysis and a major part of the writing. JV: Design of the study, and carried out data collection. TK: Data collection. HK: Data collection. AK: Design of the study, carried out data collection, data analysis and was responsible for major critical revisions of the manuscript. He will act as guarantor for the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Source of Funding
None.
Conflict of Interest
None.
Rights and permissions
About this article

Cite this article
Anantasit, N., Vaewpanich, J., Kuptanon, T. et al. Improvement of Skills in Cardiopulmonary Resuscitation of Pediatric Residents by Recorded Video Feedbacks. Indian J Pediatr 83, 1242–1247 (2016). https://doi.org/10.1007/s12098-016-2133-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-016-2133-z