
Abstract
Cancer is frequently caused by microRNAs, which control post-transcriptional levels of gene expression by binding to target mRNAs. MiR-29a-3p has recently been shown to play a twofold function in the majority of malignancies, including colorectal cancer (CRC), according to mounting evidence. Here, we not only briefly summarize such connection between miR-29a-3p and cancers, but aslo primarily evaluate the miR-29a-3p expression pattern, clinical applicability, and molecular mechanisms in CRC to provide a guide for future studies. This review established the diagnostic and prognostic value of miR-29a-3p abnormalty in a variety of clinical samples for CRC. Furthermore, current molecular mechanisms of miR-29a-3p for regulating cancerous biological processes such growth, invasion, metastasis, the epithelial-mesenchymal transformation process, and immunomodulation through its upstream regulatory factors and downstream targeted genes were briefly explored. More specifically, miR-29a-3p has been linked to a few medications that have been shown to have anticancer benefits. To sum up, miR-29a-3p is a promising biomarker and prospective therapeutic target for the diagnosis and prognosis of CRC, but further research is still needed to establish a theoretical basis for more practical applications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is the third most common cancer and the second most common cause of cancer worldwide [1]. Finding new biomarkers and medicines for early identification and efficient therapy is imperative due to the characteristics of CRC, which include strong concealment of clinical signs, a high degree of malignancy, and a dismal prognosis, particularly in the advanced stages [2, 3]. Thus, understanding the underlying mechanisms in the pathogenesis of CRC remains critical for developing new diagnostic or prognostic biomarkers and therapeutic approaches. As a heterogeneous disease, the carcinogenesis of CRC is a multifactorial and multistep process consisting of a sequential accumulation of environmental, genetic, and epigenetic factors [3]. MicroRNA dysregulation is an epigenetic alteration that has the potential to be a cancer-specific biomarker and a therapeutic target for CRC [4]. As a post-transcriptional regulator of gene expression, microRNAs are a class of highly conserved, endogenous, single-stranded, non-coding small RNAs composed of approximately 22 nucleotides [5]. Since these small RNA molecules are only expressed in certain types of cells and tissues, it has been shown that abnormal expression of miR-29a-3p plays a role in a number of pathophysiological processes, including liver fibrosis [6], cardiac remodelling [7], pulmonary vascular remodelling [8], fibro-inflammatory processes [9], neurodegenerative events [10]. More significantly, earlier studies have revealed the dual function of miR-29a-3p in a number of malignancies, particularly hepatocellular carcinoma (HCC) [45, 46]. Furthermore, on account of a growing body of studies, dysregulation of miR-29a-3p and increasing regulatory genes have been implicated in the tumorigenesis and development of various cancers via regulating tumor-related malignant biological and pathological processes such as proliferation, apoptosis, cell cycle, migration, invasion, angiogenesis, and epithelial-mesenchymal transformation (EMT) and so on. Of all the studies, most have reported that miR-29a-3p serves as a tumor suppressor; yet, existing evidence has also found it as an oncogene under certain circumstances. For example, miR-29a-3p was downregulated in head and neck squamous cell carcinoma [11], non-small cell lung cancer [109], and prostate cancer [12], but also upregulated in leukemia [13], and breast cancer [14]. Such miRNA has important clinical value for early diagnosis, targeted treatment, and improving the prognosis of various cancers [15]. In particular, in CRC, an increasing number of studies in vivo and in vitro experiments have demonstrated that miR-29a-3p dysregulation is positively or inversely correlated to the malignant biological processes through a multitude of regulatory mechanisms; however, the previous and the latest findings come to differ in such field. Correspondently, it’s necessary to sufficiently summarize the current findings of miR-29a-3p and its roles in diverse mechanisms, biological functions, and clinical value in CRC alone, and here we conducted a systematic review.
Characteristic of MiR-29a-3p
According to reports, the human genome contains roughly 2300 miRNAs, which control more than 60% of protein-coding genes and represent 2–4% of all expressed genes [16, 17]. Discovered firstly in human Hela cells in 2001 [18], the miR-29 family comprises four species with identical seed sequences and two genomic clusters. While miR-29b-2/c is found in the miR-29c cluster, miR-29a/b-1 is found in the miR-29a cluster. The mature sequences of miR-29b-1 and miR-29b-2 are identical and there exists the same seed sequence but only a nucleotide difference outside the seed sequence among miR-29a, miR-29b, and miR-29c. The miR-29a/b-1 cluster and the miR-29b-2/c cluster are encoded on different chromosomes in the human genome, respectively, at positions 7q32.3 and 1q32.2 [19] (Fig. 1). MiR-29a-3p biogenesis, like that of other miRNAs, begins in the nucleus and then moves to the cytoplasm. A mature miRNA duplex is formed from pri-miRNA and pre-miRNA after they are transcribed by RNA polymerase II and cleaved primarily by the RNase III enzymes Drosha and Dicer. MiR-29a-3p or 5p is selected from the 5′ or 3′ arm of the pre-miRNA with an imperfect stem-loop structure and then loaded onto Argonaut proteins to yield RNA-induced silencing complex (RISC), which can specifically bind to the perfect or imperfect complementary sites in the 3′untranslated region (3'UTR) of messenger RNAs, thus regulating downstream gene expression at the post-transcriptional level by degradation or translational repression of the target [5, 20] (Fig. 2). Although complex mechanisms may influence miRNA arm selection, 3p arm miRNAs are the most abundant in the miR-29 family in humans [21]. Accordingly, the majority of studies related to colorectal cancer focus on miR-29a-3p rather than miR-29a-5p as well. Despite being directly equivalent to miR-29a in previous studies,miR-29a-3p is now considered a more standardized naming for its highest expression abundance. It is worth noting that a single miRNA can target several target genes. In the meanwhile, one gene can also be regulated by multiple miRNAs. As a result, miR-29a-3p and the downstream genes that modulate its functions form a complex network.

Schematic illustration of the miR-29a-3p family members focusing on location (A) and sequence (B). Seed sequence at position 2–8 nt (red box) is important for pairing with target messenger RNAs in the miR-29-3p family. Tri-uracil instability sequence at position 9–11 nt (blue box) presents in miR-29b-3p and miR-29c-3p. Nuclear localization sequence at position 18–23 nt (purple box) only exists in miR-29b-3p. Abbreviation: nt, nucleotide

miR-29a-3p biogenesis. In the nucleus, RNA Polymerase II (Pol II) performs the initial transcription of miR-29a-3p to create a pri-miR-29a-3p transcript. Drosha, an RNase III enzyme, and DGCR8, a double-stranded RNA-binding protein, then convert the pri-miR-29a-3p transcript into pre-miR-29a-3p, an incomplete stem-loop RNA (64 nucleotides in length). Notably, pre-miR-29a-3p is exported into the cytoplasm by the RAN-GTP dependent transporter exportin 5, and processed by Dicer into miR-29a-3p duplex (a double-stranded miRNA of 22 nucleotides in length). The mature miR-29a-3p (a single-stranded miRNA of 22 nucleotides in length) is created once this dsRNA is unlocked. Mature miR-29a-3p binds to the 3'UTRs of mRNA targets and represses their production in two different ways after being integrated with Argonaute proteins into the RISC complex. This image was created using Figdraw. Available online: https://www.figdraw.com. pri-miR-29a-3p Primary miR-29a-3p, pre-miR-29a-3p precursor miR-29a-3p, DGCR8 The double-stranded RNA-binding protein, mRNA Messenger RNA, 3’UTRs 3’Untranslated regions, RISC MiRNA-induced silencing complex
MiR-29a-3p as a biomarker in CRC
MiR-29a-3p in tissues as a malignant marker
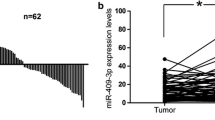
Until now, consistency and reproducibility of research have been major barriers to making miR-29a-3p in tissues a convincing potential malignant marker for CRC diagnosis and prognosis prediction (Table 1). Clearly, a substantial body of evidence has revealed that the differential expression of miR-29a-3p in CRC tissues was up-regulated when compared to adjacent normal tissues or healthy patients [22,23,24]. It is worth noting that the levels of miR-29a-3p were significantly higher in colorectal cancer tissues compared to normal tissues, but not in adenomas [25]. According to the TNM staging system, He et al. found that miR-29a-3p expression levels were lower in stage I CRC patients than in stage II and III [26]. Weissmann-Brenner et al. obtained comparable results and went on to conduct a ROC analysis. Up-regulated miR-29a-3p in tissues had a 94% positive predictive value and a 67% sensitivity for distinguishing CRC patients without recurrence. This work also found that miR-29a-3p levels in tissues were positively related to disease-free survival, and were confirmed as an independent prognostic factor for patients with II-stage CRC by multivariate analysis [27]. In addition, Krbal et al. proved that higher expressed miR-29a-3p was found in isolated colon cancer (CC) cells from clinical specimens compared with CC-derived lymph node metastatic cells [28].
In contrast to the clinical finding above, a couple of studies have indicated lower expression of miR-29a-3p could lead to poorer tumor progression. For example, Wang et al. demonstrated that the expression of miR-29a-3p in tissues was inversely related to TNM staging and lymph node metastasis of CRC [29]. Additionally, there was no statistical significance among miR-29a-3p expression and other clinical parameters, including differentiation and distant metastasis. Furthermore, Kuo et al. showed that CRC patients with early recurrence had lower miR-29a-3p expression levels than those without early recurrence, and in return lower miR-29a-3p levels were positively associated with shorter one-year survival rates [30]. Taken together, the expression pattern of miR-29a-3p in CRC is still debatable, despite the fact that it may be a marker of malignancy in CRC with some clinical relevance. The disagreement is probably given rise to the small sample size, criteria for inclusion and exclusion, individual characterization, analytical procedures, and so on.
Circulating MiR-29a-3p as a biomarker
Emerging evidence elucidated that miR-29a-3p can act as potential non-invasive diagnostic biomarkers in CRC; they are measurable in various body fluids such as serum, plasma, and exosome in sera, but among those were only a few studies as follows focusing on precancerous lesions and early-staged CRC to prevent CRC, which are curable and then function to reduce high morbidity and mortality of CRC (Table 2). In the serum samples, using two phases for screening and validation, Yamada et al. made a comparison of miR-29a-3p levels between the patients with precancerous lesions in colorectal tissues and health controls. This study found that the group of precancerous lesions expressed much higher levels of serum miR-29a-3p with an AUC of roughly 0.74 and the subgroup of advanced neoplasia (AN) was almost the same. Furthermore, this work found that serum miR-29a-3p levels were inversely related to the size of colorectal lesions. Last but not at least, in terms of combined biomarkers in the peripheral blood, the AUC values for the combination of the serum miR-21, miR-29a-3p, and miR-125b in discriminating precancerous lesions and AN patients from healthy controls were approximately 0.83 and 0.76, respectively [31]. Later, Uratani et al. used small samples and reported that serum miR-29a-3p alone had a higher AUC of 0.85 for advanced adenomas, although the AUC of 0.68 was lower for all adenomatous polyps. Additionally, the miR-29a-3p levels in exosomes did not show a favorable diagnostic lower at all [32]. Furthermore, Marcuello et al. found that the diagnostic value of the other serum miRNAs panel showed an improvement in differentiating advanced adenomas (AA) from healthy controls. The combination of six miRNAs (miR-19a-3p, miR-19b-3p, miR-335-5p, miR-29a-3p, miR-15b-5p, miR-18a-5p) yielded a higher AUC of 0.80 with 81% sensitivity, and 63% specificity [33]. In the plasma samples, Huang et al. came to a similar conclusion and reported that the high levels of miR-29a-3p alone could be used to discriminate AA from healthy controls with an AUC of 0.77, with 62% sensitivity and 85% specificity. Additionally, combined with miR-92a could enhance the sensitivity up to 73% [34]. However, another case–control study in Spain reported that the statistical significance of elevated plasma miR-29a-3p levels in AA wasn’t found [35]. Therefore, the robustness remains unclear for different circulating samples in diagnosing AA, and much more samples in different countries and specimen sources are needed to be validated.
As for CRC diagnosis, circulating miR-29a-3p is so stable that it acts as a promising non-invasive biomarker while colonoscopy as the gold standard is invasive, troublesome, and relatively expensive, and the widely used stool/blood-based tests are of low diagnostic power [36, 37]. At first, Huang et al. studied the miR-29a-3p levels for CRC screening and detection. Based on the plasma specimens, they found that compared with healthy controls, miR-29a-3p levels were highly expressed in the CRC group in China [34], and later, a study carried out a study in Spain came to the same conclusion [35]. In addition, Huang et al. also evaluated the diagnostic value of miR-29a-3p alone for CRC with an AUC of 0.84, 69% sensitivity, and 89% specificity. Furthermore, combined with miR-92a showed improvement in the diagnostic value for CRC with an AUC of 0.88, a sensitivity of 83%, and a specificity of 85%. However, there was no statistical significance between plasma miR-29a-3p level and TNM staging, tumor location, and other clinical parameters [34]. Different from the specimens in plasma, Yamada et al. reported that miR-29a-3p levels in sera were higher in CRC patients than in controls, but no significant difference was found, which was inconsistent with the previous and subsequent studies [31]. In the last five years, both miR-29a-3p alone and a combination of other miRNAs in sera have shown considerable diagnostic values. Liu et al. demonstrated that serum miR-29a-3p level was significantly higher in CRC patients than in healthy controls and showed a higher AUC of 0.88 with 69% sensitivity and 95% specificity, compared with the AUC of 0.808 and 0.705, respectively, for serum CEA and CA19-9. This work further found the optimal combination of miRNAs in serum for CRC well-diagnosis and finally reported that high levels of the 4-miRNAs panel (miR-21, miR-29a-3p, miR-92a, miR-125b) for discriminating CRC yielded the highest diagnostic value with an AUC value of 0.95, a sensitivity of 85% and a specificity of 99% than any miRNAs reported ever before [38]. Concerning Marcuello M's research, whether a serum 6-miRNAs panel was alone or in combination with hemoglobin concentration in feces, their diagnostic values for CRC in diagnosing CRC were inferior to the previous result [33]. Above all, although there seems to be a lack of consistency in different circulating samples and the diagnostic values were discrete, miR-29a-3p is a promising biomarker for CRC and further studies are worthwhile.
Notably, El-Daly et al. constructed a murine model of colitis-related CRC to initially access the dynamic changing in the expression level of miR-29a-3p during the stepwise carcinogenesis process and the consistency of miR-29a-3p level in serum and corresponding tissue samples. Noteworthy, higher miR-29a-3p levels were found in the advanced stage of carcinogenesis and yielded higher diagnostic values for early colon lesions than serum CEA and CA-19-9. Furthermore, this work confirmed that serum miR-29a-3p may derive from tissue for its consistency in the diagnostic power during the carcinogenesis process. However, only vivo experiments in the mouse model could limit the clinical application of the above results, and further clinical correlations are still needed to be done [39].
Although not much, some studies were performed to evaluate the circulating miR-29a-3p levels to predict the progress and prognosis of CRC. In general, higher circulating miR-29a-3p levels showed a higher risk of malignant progression and poor prognosis. For example, Zhou et al. revealed that upregulation of miR-29a-3p in sera could predict the liver metastasis of CRC with a high AUC of 0.85, 66% sensitivity, and 84% specificity. Further combination with serum COX-2 and matrix metallopeptidase 2(MMP2) show higher diagnostic values of AUC = 0.90, 72% sensitivity, and 95% specificity [40]. Yuan et al. found that a high preoperative miR-29a-3p level in plasma could predict relapse of CRC within 3 years with an AUC of 0.70 while dynamic postoperative plasma miR-29a-3p levels did not correlate with CRC recurrence [41]. Interestingly, to access and analyze the non-vesicular to extracellular vesicles miR-29a-3p expression ratio in serum for the first time, Shiosaki et al. enrolled a cohort of CRC patients from different races from Japan and Hawaii. However, they found that compared with healthy controls, such ratio was higher in both the early-staged (stage I, II) and advanced (stage III, IV) CRC patients, and the AUC for diagnosis of CRC was 0.70. Additionally, the levels of miR-29a-3p only in extracellular vesicles showed a stepwise reduction during the progression of CRC stages, which could explain the corresponding increased ratio [42].
Fecal and salivary MiR-29a-3p as a biomarker
Although these sample types seem to be more non-invasive and easier to get than blood, there indeed exists controversy in the expression of miR-29a-3p in between saliva and feces among the limited literature that has been published (Table 2). Rapado-González et al. have proven that salivary miR-29a-3p levels were significantly higher in CRC patients than in healthy controls, and yielded an AUC value of 0.63 to differentiate CRC from normality. Furthermore, a 5-miRNAs panel (miR-186-5p, miR-29a-3p, miR-29c-3p, miR-766-3p, miR-491-5p) yielded a higher AUC value of 0.75, with a sensitivity of 70%, compared with a sensitivity of 45% for serum CEA. Notably, this 5-miRNAs panel combined with serum CEA could enhance a higher sensitivity up to 89%. In terms of demographic and clinicopathological characteristics in CRC patients, the salivary miR-29a-3p levels were only significantly higher in males than in women, however, no significant association was found between salivary miR-29a-3p levels and other parameters. Additionally, the study also confirmed that these salivary 5-miRNAs panel levels are independent prognostic factors for progression-free survival in patients with IV CRC by univariate and multivariate cox regression analysis [43].
Contrary to Rapado-González ‘s findings, Zhu et al. showed that compared with healthy controls, fecal miR-29a-3p was abnormally downregulated in stool samples of CRC patients with an AUC of 0.78, 85% sensitivity, and 61% specificity, which surpassed the partial diagnostic values of miR-223 (AUC: 0.744, 60% sensitivity), and miR-224 (AUC: 0.745, 75% sensitivity). Different from all the above studies, a significant association was found between fecal miR-29a-3p level and location of CRC, that is, colon cancer expressed a lower level of miR-29a-3p than rectal cancer [44]. In conclusion, samples were not enough to clarify the contradiction in miR-29a-3p dysregulation and clinical values in different sources of samples in CRC. What’s more, multicenter researches, unified methodology, and calculation methods are also further needed.
The mechanisms of MiR-29a-3p in cancers
As was already ascertained, miR-29a-3p regulates a variety of malignancies due to its dual expression patterns. The underlying molecular mechanism and functional role of miR-29a-3p, which functions as a frequently downregulated tumor suppressor or occasionally an oncogene in a variety of cancers through various upstream genes and target genes, have been the subject of an increasing number of studies over the past three years. Consistently, given the information that is now available, a sufficient summary of miR-29a-3p’s dual roles in HCC was provided last year [45]. Therefore, Table 3 details the most current discoveries about the roles and mechanisms of miR-29a-3p and its validated gene in cancer. In particular, considering the preceding review [46], we partially concentrate on the research connecting miR-29a-3p and competing endogenous RNAs in malignancies, which may, to some extent, enhance the activity of miR-29a-3p alone but has previously been constrained.
MiR-29a-3p functions as a tumor suppressor by preventing cell proliferation, invasion, migration, cell cycle, EMT process, angiogenesis, drug resistance, and enhancing apoptosis in various cancers. This is achieved by binding to the 3′UTR of validated target genes of all types. Numerous oncogenes targeted by miR-29a-3p were experimentally confirmed to be down-regulated in terms of inhibiting tumor growth, including DPP4 [47], KDM5B1 [48], AKT2 [49], SPAPCD2 [50], MDM2 [51], PDGF [52], and others. The direct targets of miR-29a-3p, such as the associated genes collagens (COL) [54,55,55], STAT3 [56], VEGF [57], LOX [58], LOXL2 [59], ROBO1 [60], mostly affected the tumor microenvironment, which was the site of angiogenesis, EMT process, and metastasis. In addition, miR-29a-3p-targeted genes C1QTNF [61], LTβR [62], and OTUB2 [63] that are involved in immunomodulation in malignancies were also confirmed to contribute to tumor growth and progression. With regard to cervical cancer (CC) [64, 65] and endometrial cancer (EC) [66], numerous pieces of evidence revealed that miR-29a-3p played a detrimental role in the growth of tumors by targeting epigenetic modifiers such DNMT1, DNMT3A, and DNMT3B. The cytokine signaling 1 (SOCS1) gene was consistently directly demethylated by these epigenetic modifiers, which in turn controlled the NF-kB signaling pathway in both the CC and EC [65, 66].
More recent studies have shown that miR-29a-3p expression levels are negatively regulated by competing endogenous RNAs, such as long non-coding RNAs (lncRNA) and circular RNAs (circRNA), through the miR-sponging process. For instance, by competitively sponging miR-29a-3p, lncRNA HOXA-AS3, lncRNA LIFR-AS1, lncRNA NR2F1-AS1, and circ29 have a promotive function in the carcinogenesis of gastric cancer [62, 53, 57, 67]. Importantly, Li et al. identified one of them, circ29, as a miR-29a-3p sponge that supported tumor angiogenesis [57]. In addition to being recognized as one of the ceRNAs in HCC [45], lncRNA TUG1 was also recognized as a potential anti-cancer factor due to its direct inhibition of miR-29a-3p production in cholangiocarcinoma. Furthermore, lncRNA H19 sponged and downregulated miR-29a-3p in both acute myeloid leukemia (AML) and osteosarcoma, which prevented cell death and enhanced cell proliferation, migration, and invasion [68, 69]. Interestingly, in prostate cancer (PC), Kong et al. proved that circFOXO3 exerted a tumor-promoting role in inhibiting the capacity of cell apoptosis and cell cycle arrest via directly down-regulating miR-29a-3p, and then up-regulating SLC25A15 [12]. Inversely, according to Yang et al., although circFOXO3 overexpression was observed in renal cell carcinoma (RCC), it served as an inhibitor in vitro by directly sponging miR-29a-3p, which increased NK cell cytotoxicity toward RCC cells. On the other hand, miR-29a-3p overexpression weakened this immunomodulation process [70].
Several pieces of evidence have shown that miR-29a-3p works as an oncogene in many different types of malignancies, including RCC, oral squamous cell carcinoma (OSCC), ovarian cancer (OC), breast cancer, and ameloblastoma, in contrast to the tumor-suppressive role that has been discussed in cancers. As previously reported, circFOXO3 demonstrated the opposite impact through tumor immunomodulation and tumorigenicity in several malignancies. In this regard, it was established that circFOXO3 directly binds to and inversely modulatesmiR-29a-3p. In the tumor immune microenvironment, miR-29a-3p acted to attenuate the NK cell cytotoxicity towards RCC cells augmented by circFOXO3, which made it a tumor-promoter [70]. Furthermore, Lu et al. indicated that tumor-associated macrophages (TAMs)-derived miR-29a-3p in exosome could foster OC cell proliferation in vitro [90]. Mechanistically, miR-29a-3p functioned as a tumor-promoting factor by downregulating the FOXO3-AKT/GSK3β axis and subsequently suppressing the expression of PD-L1, which was a known target molecule for anti-tumor immunotherapy, to shield OC cells from immune escape. Additionally, Cai et al. showed thatmiR-29a-3p was strongly expressed in the tissues of OSCC and encouraged M2 subtype macrophage polarization in the form of OSCC-derived exosomes produced by OSCC, which increased cell proliferation, invasion in vitro, and tumor growth in vivo. The mechanism was that miR-29a-3p bound to SOCS1 and further up-regulated transcriptional activator 6 (STAT6) in macrophages [71]. Liu et al. found that miR-29a-3p levels in tissues were higher than normal in ameloblastoma. Additional research showed that miR-29a-3p directly targets the β-catenin interacting protein 1 (CTNNBIP1), which negatively regulated the activity of the Wnt/-βcatenin pathway and facilitates cell migration and invasion [72]. Sikder et al. discovered PC4, a transcriptional coactivator, as a target of miR-29a-3p in breast cancer, which led to tumor growth both in vitro and in vivo. In the same year, Wu et al. found that the overexpression of miR-29a-3p in breast cancer cells facilitated both in vitro and in vivo migration and invasion by binding to SUV420H2, a histone methyltransferase that preferentially trimethylates Lys-20 of histone H4 (H4K20). H4K20 trimethylation was further modulated by connective tissue growth factor (CTGF) and growth response protein-1 (EGR1), which are involved in the EMT process [73].
The mechanism of MiR-29a-3p in CRC
MiR-29a-3p as an oncogene
Despite the considerable clinical studies described above showing that CRC clinical samples express abnormally high levels of miR-29a-3p, there has been little research on the mechanism underlying miR-29a-3p’s role as an oncogene in CRC (Fig. 3). Mechanistically, miR-29a-3p promoted invasion, metastasis, and drug resistance in CRC by directly targeting KLF4 and PTEN. The normal gastrointestinal tract has been shown to express KLF4, a transcription factor with zinc finger structure and a member of the KLF family. The normal gastrointestinal tract has been shown to express KLF4, a transcription factor with zinc finger structure and a member of the KLF family [110]. KLF4 was abnormally down-regulated in colorectal adenoma and CRC, respectively, and was involved in the development of CRC, according to earlier investigations [93, 94]. According to research by Tang et al., overexpressed miR-29a-3p increased invasion and metastasis as well as the EMT process in vitro by directly binding to KLF4 at both the mRNA and protein levels. It also affected the expression of MMP2 and E-cadherin. On the other side, the promotive role of miR-29a-3p in CRC could be reversed by the restoration of KLF expression. Additionally, in vivo experiments using a mouse model of CRC treated with miR-29a-3p revealed a dramatically reduced level of KLF4 expression in the liver-metastatic nodules. As previously noted, miR-29a-3p was expressed at higher levels in CRC tissues than in healthy controls, which increased the risk of metastasis and decreased overall survival in CRC patients [24]. In terms of chemotherapeutic resistance, paclitaxel-resistant SW480 cells had greater levels of miR-29a-3p than did non-resistant SW480 cells, and miR-29a-3p was linked to acquired paclitaxel resistance via inhibiting the PTEN/PI3K/AKT pathway. Additional in vitro studies supported the finding that transfection of the miR-29a-3p inhibitor had an inhibitory effect on cell growth and caused apoptosis in CRC via increasing PTEN expression [95]. Regarding radiotherapy resistance, both malignant and normal cells, such as human intestinal epithelial crypt cell (HIEC), HT29, HCT116, and DLD-1 cells, showed increased miR-29a-3p levels following radiation treatment. Interestingly, it's noted that the molecular mechanism of radiation resistance caused by miR-29a-3p overexpression was the same as that reported above by LL et al. [96].
MiR-29a-3p as a tumor suppressor
A few other mechanistic studies have demonstrated that miR-29a-3p acts as a tumor suppressor and inhibits the growth, invasion, and metastasis of CRC cells through a number of target genes, in contrast to the aforementioned clinical or experimental studies that discovered the cancer-promoting effects of miR-29a-3p (Fig. 3). Zheng et al. provided evidence that miR-29a-3p expression was abnormally down-regulated in CRC tissues and related CRC cell lines, including DLD-1, RKO, SW480, and HCT116 cells. Additionally, miR-29a-3p overexpression reduced the growth of cancer cells, prevented the progression of the cell cycle into the G0/G1 phase, and brought about apoptosis. More in vitro analysis confirmed that RPS15A was a direct target of miR-29a-3p. Overexpression of RPS15A, a ribosomal protein involved in ribosomal assembly and translation, had the opposite impact of miR-29a-3p’s anti-CRC by partially down-regulating the expression of p21 and Bcl-2 and up-regulating the expression of CDK4, cyclin D1, and Bax [97]. Additionally, Disheveled family member DVL3 plays a carcinogenic role in many tumors by acting as a receptor and downstream target of cytoplasmic scaffold proteins through the activation of Wnt and NOTCH signaling pathways [98]. In a more recent study, Zheng et al. asserted that miR-29a-3p inhibited the expression of DVL3 at the mRNA and protein levels in HT29 and HT-116 cells, functioning to prevent cell growth and metastasis and reduce apoptosis. Furthermore, in CRC tissues and paired neighboring normal tissues, an inverse connection was detected between miR-29a-3p and DVL3 protein levels. Additionally, it was shown that the long non-coding RNA TTTY15 acts as a negative upstream regulator of miR-29a-3p [99]. It is well known that CDC42BP, a member of the serine protein kinase family, promotes tumor invasion and migration via modulating actin [100]. In vitro research by He et al. revealed that miR-29a-3p overexpression inhibited cell invasion and migration in CRC. Up-regulation of cytoskeletal regulatory genes such as CDC42BP, IQGAP2, and SSH1 was detected at the mRNA and protein expression levels following the suppression of miR-29a-3p. Knockdown of CDC42BP in vitro partially abrogated the anti-CRC effect generated by miR-29a-3p, and this target was predicted as a downstream target of miR-29a-3p by public databases; nevertheless, the binding link between these two genes lacked further experimental verification [26]. Besides, in a mouse model of a malignant colonic tumor generated by TGF-β, Huang et al. discovered that the expression levels of miR-29a-3p and its anticipated target genes DNMT3A/3B were considerably down-regulated. However, a related experiment to confirm the interaction between DNMT3A/3B and miR-29a-3p was omitted. In addition, it appeared that miR-29a-3p and DNA methyltransferases formed a negative feedback loop. The levels of miR-29a-3p were partially re-expressed under treatment with a DNMT inhibitor, though they remained lower than the normal controls [101]. Similarly, Gerovska et al. have developed a mouse model of CRC liver metastasis and found that miR-29a-3p expression was significantly reduced in the liver tumor microenvironment cells compared to the healthy controls. Microarray analysis suggested a link between histone modification and DNA methylation [102]. Besides that, APOBEC3G, one of the metastasis-related genes, was also shown by Ding et al. to facilitate cell invasion and metastasis in colon cancer cells using an orthotopic animal model of CRC. Regarding the mechanism, they confirmed in vitro using PCR array that APOBEC3G reduced miR-29a-3p levels, leading to elevated expression of matrix metalloproteinase 2(MMP2) [103].
Lnc TTTY and two oncogenes, MYC and APOBEGC3G could inhibit miR-29a-3p. miR-29a-3p directly targeted RPS15A, MMP2, DVL3, CDC42BP, DNMT3A/3B, and PTEN to impede malignant biological processes. However, miR-29a-3p boosted malignant biological processes by binding to KLF4, IFN-γ, and PTEN. Additionally, only Wnt/β-catenin and PI3K/AKT signaling pathways are verified in CRC. Consequently, miR-29a-3p could promote or suppress the malignant biological functions in CRC, such as cell proliferation, apoptosis, invasion, metastasis, tumor growth, and therapeutic resistance. This figure was created with Figdraw. Available online: https://www.figdraw.com. (The red lines emitted indicate carcinogenic factors and the blue ones indicate suppressive factors.)

miR-29a-3p-related downstream and upstream genes and biological functions in CRC
Mir-29a-3p-based therapy for CRC
MiR-29a-3p in chemoradiotherapy resistance
Based on the results of the available experimental research, aberrant expression of miR-29a-3p can either increase or decrease resistance to radiation and chemotherapy by inhibiting the tumor suppressor PTEN (Fig. 3). For chemotherapy resistance, higher amounts of miR-29a-3p were discovered in paclitaxel-resistant SW480 cells than in SW480 cells, according to research by LL et al. This indirectly activates the PI3K/AKT signaling pathway by binding to PTEN 3'UTR. MiR-29a-3p inhibitor in vitro enhanced PTEN expression to reduce CRC cell proliferation and induce apoptosis [95]. In contrast to this observation, Shi X et al. showed that miR-29a-3p overexpression in CRC cells played a detrimental impact in doxorubicin (DOX) resistance by directly binding to PTEN and reducing PTEN expression. In particular, HT29/DOX doxorubicin-resistant cancer cells expressed less miR-29a-3p than HT2 cells did. MiR-29a-3p mimic transfection further decreased DOX resistance. In addition, membrane transporter P-glycoprotein expression was found to be suppressed in a pathway downstream of PTEN [104]. Wang et al. found that miR-29a-3p mimics boosted irradiation resistance in HIEC, a normal human intestinal epithelial crypt cell line, while the inhibitors sensitized drug-resistant CRC cell lines. As was reported earlier in drug resistance, an attractive mechanism was that miR-29a-3p served as a suppressor of PTEN [96].
For radiotherapy resistance, Wang et al. proved that miR-29a-3p mimics increased the resistance to radiation in HIEC, the normal human intestinal epithelial crypt cell line, while the miR-29a-3p inhibitor could sensitize drug-resistant CRC cell lines. Interestingly, the underlying mechanism was that miR-29a-3p acted as a suppressor of PTEN as mentioned previously in drug resistance [108]. Taken together, despite the limited number of investigations, we noted that miR-29a-3p-targeted molecular therapy combined with radiotherapy and/or chemotherapy has the potential role to restore the treatment response and further improve the prognosis in advanced CRC patients with poor survival. Further studies should be conducted to find out more underlying mechanisms.
MiR-29a-3p-based drugs
Mounting data suggests that anticancer drugs can halt the formation and progression of CRC by controlling the dysregulation of miR-29a-3p (Fig. 3). In order to counteract colonic carcinogenesis brought on by TGF-β, Huang et al. found that the molecular mechanisms of Chinese herbal medicines, including berberine and evodiamine, were associated with the overexpression of epigenetic factors, particularly miR-29a-3p and its target genes DNMT3A/3B [101]. Additionally, the natural food additive inositol hexaphosphate (IP6) is recognized to have anti-CRC properties. Through using microarray analysis, Kapral et al. revealed that its anticancer mechanism is also connected to a notable decline in miR-29a-3p in vitro experiments [105]. According to Kim et al., Astaxanthin (ATX) inhibited the ability of CRC to invade and spread through the down-regulation of MCY and further inactivation of the miR-29a-3p/MMP2 and miR-200a/ZEB1 axis. MCY is an oncogenic transcription factor and interacts adversely with miR-29a-3p in PC and AML [59, 86]. Kim et al. found that MCY suppressed miR-29a-3p and miR-200a expression in CRC. As a result, the anti-metastasis impact of ATX was mediated by MCY inhibition, followed by the restoration of miR-29a-3p and miR-200a expression. Additionally, they indicated that miR-29a-3p inhibited MMP2 production, which hampered the EMT process in vitro. As an aside, approximately 55% of individuals with metastatic CRC had KRAS mutations [106]. Therefore, Parakrama et al. examined the molecular characteristics of patients with KRAS mutant CRC following reovirus treatment for the first time based on the anticancer activity of reovirus. Reovirus therapy for KAS-mutated metastatic CRC resulted in considerably decreased miR-29a-3p expression in peripheral blood mononuclear cells and exosomes compared to standard chemotherapy and anti-VEGF treatment with FOLFIRI and bevacizumab. Functionally, miR-29a-3p upregulated the production of IFN-γ, which in turn activated CD8 + T cells and triggered their cytotoxic potential [107]. Consequently, down-regulation of miR-29a-3p was recognized as a measure of reovirus therapeutic response. Taken together, more investigations on the link between miR-29a-3p and immune regulation in CRC are promising to help physicians make a better decision for customized therapy options.
Conclusion and prospect
Notably, miR-29a-3p aberrant expression in CRC may serve as a diagnostic and prognostic biomarker. Furthermore, miR-29a-3p expression in serum, exocrine, saliva, and feces will have a wider clinical utility as a non-invasive biomarker for co-detection. However, the question of whether miR-29a-3p is an oncogene or a tumor suppressor gene, and if miR-29a-3p differs in different CRC conditions, remains unresolved. Given the evidence for miR-29a-3p in CRC, the biological processes of proliferation, invasion, metastasis, the EMT process are closely related; however, further in-depth research into the complex regulatory mechanisms and functions of this miRNA is still required, both in vivo and in vitro. We observe that miR-29a-3p in the tumor immune microenvironment mostly serves a pro-cancer role in other cancers, which needs to be further investigated in CRC. This is based on the more extensive regulation mechanisms of miR-29a-3p in different other malignancies. Further investigation of additional ceRNAs that target miR-29a-3p will further provide light on CRC biology. Last but not least, miR-29a-3p has also been linked to the efficacy of some well-known medications and the responsiveness of current anticancer therapies, demonstrating its enormous potential as a therapeutic target for CRC. In conclusion, miR-29a-3p is a prospective marker for molecular targeting or therapeutic responsiveness as part of a customized and precise treatment approach for CRC patients. It is not just a viable candidate marker for diagnosis and prognosis. Most significantly, future relevant preclinical studies and clinical trials still need to be conducted in order to achieve the transfer from miR-29a-3p research to clinical application.
References
Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Przeglad Gastroenterol. 2019;14:89–103.
Kamel F, Eltarhoni K, Nisar P, Soloviev M. Colorectal cancer diagnosis: the obstacles we face in determining a non-invasive test and current advances in biomarker detection. Cancers. 2022;14:1889.
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer Lancet Lond Engl. 2019;394:1467–80.
Mollaei H, Safaralizadeh R, Rostami Z. MicroRNA replacement therapy in cancer. J Cell Physiol. 2019;234:12369–84.
Li C, Wang N, Rao P, Wang L, Lu D, Sun L. Role of the microRNA-29 family in myocardial fibrosis. J Physiol Biochem. 2021;77:365–76.
Matsumoto Y, Itami S, Kuroda M, Yoshizato K, Kawada N, Murakami Y. MiR-29a assists in preventing the activation of human stellate cells and promotes recovery from liver fibrosis in mice. Mol Ther. 2016;24:1848–59.
Mayoral-González I, Calderón-Sánchez EM, Galeano-Otero I, Martín-Bórnez M, Gutiérrez-Carretero E, Fernández-Velasco M, et al. Cardiac protection induced by urocortin-2 enables the regulation of apoptosis and fibrosis after ischemia and reperfusion involving miR-29a modulation. Mol Ther -Nucleic Acids. 2022;27:838–53.
Chouvarine P, Geldner J, Giagnorio R, Legchenko E, Bertram H, Hansmann G. Trans-right-ventricle and transpulmonary microrna gradients in human pulmonary arterial hypertension. Pediatr Crit Care Med J Soc Crit Care Med World Fed Pediatr Intensive Crit Care Soc. 2020;21:340–9.
Dey S, Udari LM, RiveraHernandez P, Kwon JJ, Willis B, Easler JJ, et al. Loss of miR-29a/b1 promotes inflammation and fibrosis in acute pancreatitis. JCI Insight. 2021;6: e149539.
Barbagallo C, Mostile G, Baglieri G, Giunta F, Luca A, Raciti L, et al. Specific signatures of serum miRNAs as potential biomarkers to discriminate clinically similar neurodegenerative and vascular-related diseases. Cell Mol Neurobiol. 2020;40:531–46.
Koshizuka K, Kikkawa N, Hanazawa T, Yamada Y, Okato A, Arai T, et al. Inhibition of integrin β1-mediated oncogenic signalling by the antitumor microRNA-29 family in head and neck squamous cell carcinoma. Oncotarget. 2018;9:3663–76.
Kong Z, Wan X, Lu Y, Zhang Y, Huang Y, Xu Y, et al. Circular RNA circFOXO3 promotes prostate cancer progression through sponging miR-29a-3p. J Cell Mol Med. 2020;24:799–813.
Raeisi F, Mahmoudi E, Dehghani-Samani M, Hosseini SSE, Ghahfarrokhi AM, Arshi A, et al. Differential expression profile of miR-27b, miR-29a, and miR-155 in chronic lymphocytic leukemia and breast cancer patients. Mol Ther Oncolytics. 2020;16:230–7.
Wu Y, Shi W, Tang T, Wang Y, Yin X, Chen Y, et al. miR-29a contributes to breast cancer cells epithelial–mesenchymal transition, migration, and invasion via down-regulating histone H4K20 trimethylation through directly targeting SUV420H2. Cell Death Dis. 2019;10:176.
Alizadeh M, Safarzadeh A, Beyranvand F, Ahmadpour F, Hajiasgharzadeh K, Baghbanzadeh A, et al. The potential role of miR-29 in health and cancer diagnosis, prognosis, and therapy. J Cell Physiol. 2019;234:19280–97.
Catalanotto C, Cogoni C, Zardo G. MicroRNA in control of gene expression: an overview of nuclear functions. Int J Mol Sci. 2016;17:E1712.
Alles J, Fehlmann T, Fischer U, Backes C, Galata V, Minet M, et al. An estimate of the total number of true human miRNAs. Nucleic Acids Res. 2019;47:3353–64.
Lagos-Quintana M, Rauhut R, Lendeckel W, Tuschl T. Identification of novel genes coding for small expressed RNAs. Science. 2001;294:853–8.
Kwon JJ, Factora TD, Dey S, Kota J. A systematic review of miR-29 in Cancer. Mol Ther-Oncolytics. 2019;12:173–94.
O’Brien J, Hayder H, Zayed Y, Peng C. Overview of MicroRNA biogenesis, mechanisms of actions, and circulation. Front Endocrinol. 2018;9:402.
Warnement CM, Cismowski MJ, Rogers LK. Optimizing miR-29 measurements in biobanked, heparinized samples. Life Sci. 2019;238: 116894.
Kara M, Yumrutas O, Ozcan O, Celik OI, Bozgeyik E, Bozgeyik I, et al. Differential expressions of cancer-associated genes and their regulatory miRNAs in colorectal carcinoma. Gene Amsterdam: Elsevier Science Bv. 2015;567:81–6.
Brunet Vega A, Pericay C, Moya I, Ferrer A, Dotor E, Pisa A, et al. microRNA expression profile in stage III colorectal cancer: circulating miR-18a and miR-29a as promising biomarkers. Oncol Rep. 2013;30:320–6.
Tang W, Zhu Y, Gao J, Fu J, Liu C, Liu Y, et al. MicroRNA-29a promotes colorectal cancer metastasis by regulating matrix metalloproteinase 2 and E-cadherin via KLF4. Br J Cancer. 2014;110:450–8.
Uratani R, Toiyama Y, Kitajima T, Kawamura M, Hiro J, Kobayashi M, et al. Diagnostic potential of cell-free and exosomal micrornas in the identification of patients with high-risk colorectal adenomas. PLoS ONE. 2016;11:e0160722.
He PY, Yip WK, Chai BL, Jabar MF, Dusa N, Mohtarrudin N, et al. Inhibition of cell migration and invasion by miR-29a-3p in a colorectal cancer cell line through suppression of CDC42BPA mRNA expression. Oncol Rep. 2017;38:3554–66.
Weissmann-Brenner A, Kushnir M, Yanai GL, Aharonov R, Gibori H, Purim O, et al. Tumor microRNA-29a expression and the risk of recurrence in stage II colon cancer. Int J Oncol. 2012;40:2097–103.
Krbal L, Hanusova V, Soukup J, John S, Matouskova P, Ryska A. Contribution of in vitro comparison of colorectal carcinoma cells from primary and metastatic lesions to elucidation of mechanisms of tumor progression and response to anticancer therapy. Tumor Biol London: Sage Publications Ltd. 2016;37:9565–78.
Wang J, Chen X, Xie C, Sun M, Chenrui Hu, Zhang Z, et al. MicroRNA miR-29a inhibits colon cancer progression by downregulating B7–H3 expression: potential molecular targets for colon cancer therapy. Mol Biotechnol. 2021;63:849–61.
Kuo T-Y, Hsi E, Yang I-P, Tsai P-C, Wang J-Y, Juo S-HH. Computational analysis of mRNA expression profiles identifies microrna-29a/c as predictor of colorectal cancer early recurrence. PLoS ONE. 2012;7:e31587.
Yamada A, Horimatsu T, Okugawa Y, Nishida N, Honjo H, Ida H, et al. Serum miR-21, miR-29a, and miR-125b Are Promising Biomarkers for the Early Detection of Colorectal Neoplasia. Clin Cancer Res Philadelphia Amer Assoc Cancer Res. 2015;21:4234–42.
Uratani R, Toiyama Y, Kitajima T, Kawamura M, Hiro J, Kobayashi M, et al. Diagnostic potential of cell-free and exosomal microRNAs in the identification of patients with high-risk colorectal adenomas. PLoS ONE. 2016;11: e0160722.
Marcuello M, Duran-Sanchon S, Moreno L, Jose Lozano J, Bujanda L, Castells A, et al. Analysis of A 6-mirna signature in serum from colorectal cancer screening participants as non-invasive biomarkers for advanced adenoma and colorectal cancer detection. Cancers Basel Mdpi. 2019;11:1542.
Huang Z, Huang D, Ni S, Peng Z, Sheng W, Xiang Du. Plasma microRNAs are promising novel biomarkers for early detection of colorectal cancer. Int J Cancer Hoboken Wiley. 2010;127:118–26.
Giráldez MD, Lozano JJ, Ramírez G, Hijona E, Bujanda L, Castells A, et al. Circulating micrornas as biomarkers of colorectal cancer: results from a genome-wide profiling and validation study. Clin Gastroenterol Hepatol. 2013;11:681-688.e3.
Chan SCH, Liang JQ. Advances in tests for colorectal cancer screening and diagnosis. Expert Rev Mol Diagn Oslo Taylor Francis As. 2022;22:449–60.
To KK, Tong CW, Wu M, Cho WC. MicroRNAs in the prognosis and therapy of colorectal cancer: from bench to bedside. World J Gastroenterol. 2018;24:2949–73.
Liu H-N, Liu T-T, Wu H, Chen Y-J, Tseng Y-J, Yao C, et al. Serum microRNA signatures and metabolomics have high diagnostic value in colorectal cancer using two novel methods. Cancer Sci Hoboken Wiley. 2018;109:1185–94.
El-Daly SM, Morsy SM, Medhat D, El-Bana MA, Latif YA, Omara EA, et al. The diagnostic efficacy of circulating miRNAs in monitoring the early development of colitis-induced colorectal cancer. J Cell Biochem. 2019;120:16668–80.
Zhou D-J, Yuan H. Diagnostic value of serum miR-29a, COX-2 and MMP2 in patients with liver metastases from colorectal cancer. Chinese Journal of General Practice. 2017;15:1944–7.
Yuan Z, Baker K, Redman MW, Wang L, Adams SV, Ming Yu, et al. Dynamic plasma microRNAs are biomarkers for prognosis and early detection of recurrence in colorectal cancer. Br J CANCER. 2017;117:1202–10.
Shiosaki J, Tiirikainen M, Peplowska K, Shaeffer D, Machida M, Sakamoto K, et al. Serum micro-RNA identifies early stage colorectal cancer in a multi-ethnic population. Asian Pac J Cancer Prev APJCP. 2020;21:3019–26.
Rapado-Gonzalez O, Majem B, Alvarez-Castro A, Diaz-Pena R, Abalo A, Suarez-Cabrera L, et al. A novel saliva-based miRNA signature for colorectal cancer diagnosis. J Clin Med Basel Mdpi. 2019;8:2029.
Zhu Y, Xu A, Li J, Fu J, Wang G, Yang Y, et al. Fecal miR-29a and miR-224 as the noninvasive biomarkers for colorectal cancer. Cancer Biomark Amst Ios Press. 2016;16:259–64.
Yang Y-L, Chang Y-H, Li C-J, Huang Y-H, Tsai M-C, Chu P-Y, et al. New insights into the role of miR-29a in hepatocellular carcinoma: implications in mechanisms and theragnostics. J Pers Med. 2021;11:219.
Wang J-Y, Zhang Q, Wang D-D, Yan W, Sha H-H, Zhao J-H, et al. MiR-29a: a potential therapeutic target and promising biomarker in tumors. 2018. Biosci Rep. https://doi.org/10.1042/BSR20171265.
Wang Y, Han J, Lv Y, Zhang G. miR-29a inhibits proliferation, invasion, and migration of papillary thyroid cancer by targeting DPP4. Onco Targets Ther. 2019;12:4225–33.
Zhao L-F, Qi F-Y, Zhang J-G, Pang J-R, Ren H-M, Shen D-D, et al. Identification of the upstream regulators of KDM5B in gastric cancer. Life Sci Neth. 2022;298:120458.
Zhao J, Liu X, Lin J, Jiang M, Xu F, Zhang C, et al. AKT2 identified as a potential target of mir-29a-3p via microRNA profiling of patients with high proliferation lacrimal gland adenoid cystic carcinoma. Exp Eye Res Engl. 2022;219:109067.
Yang Z, Ding H, Pan Z, Li H, Ding J, Chen Q. YY1-inudced activation of lncRNA DUXAP8 promotes proliferation and suppresses apoptosis of triple negative breast cancer cells through upregulating SAPCD2. Cancer Biol Ther. 2021;22:216–24.
Chen Q, Wang W, Chen S, Chen X, Lin Y. miR-29a sensitizes the response of glioma cells to temozolomide by modulating the P53/MDM2 feedback loop. Cell Mol Biol Lett. 2021;26:21.
Yang Y, Dodbele S, Park T, Glass R, Bhat K, Sulman EP, et al. MicroRNA-29a inhibits glioblastoma stem cells and tumor growth by regulating the PDGF pathway. J Neurooncol United States. 2019;145:23–34.
Pan H, Ding Y, Jiang Y, Wang X, Rao J, Zhang X, et al. LncRNA LIFR-AS1 promotes proliferation and invasion of gastric cancer cell via miR-29a-3p/COL1A2 axis. Cancer Cell Int. 2021;21:7.
An Q, Liu T, Wang M-Y, Yang Y-J, Zhang Z-D, Lin Z-J, et al. circKRT7-miR-29a-3p-COL1A1 axis promotes ovarian cancer cell progression. Onco Targets Ther. 2020;13:8963–76.
Zhao B, Song X, Guan H. CircACAP2 promotes breast cancer proliferation and metastasis by targeting miR-29a/b-3p-COL5A1 axis. Life Sci Neth. 2020;244:117179.
Liu Y-B, Wang Y, Zhang M-D, Yue W, Sun C-N. MicroRNA-29a functions as a tumor suppressor through targeting STAT3 in laryngeal squamous cell carcinoma. Exp Mol Pathol Neth. 2020;116:104521.
Li S, Li J, Zhang H, Zhang Y, Wang X, Yang H, et al. Gastric cancer derived exosomes mediate the delivery of circRNA to promote angiogenesis by targeting miR-29a/VEGF axis in endothelial cells. Biochem Biophys Res Commun United States. 2021;560:37–44.
Yang Y-L, Tsai M-C, Chang Y-H, Wang C-C, Chu P-Y, Lin H-Y, et al. MIR29A impedes metastatic behaviors in hepatocellular carcinoma via targeting LOX, LOXL2, and VEGFA. Int J Mol Sci. 2021;22:6001.
Dey S, Kwon JJ, Liu S, Hodge GA, Taleb S, Zimmers TA, et al. miR-29a is repressed by MYC in pancreatic cancer and its restoration drives tumor-suppressive effects via downregulation of LOXL2. Mol Cancer Res. 2020;18:311–23.
Zhang Z, Guo X, Guo X, Yu R, Qian M, Wang S, et al. MicroRNA-29a-3p delivery via exosomes derived from engineered human mesenchymal stem cells exerts tumour suppressive effects by inhibiting migration and vasculogenic mimicry in glioma. Aging-Us. 2021;13:5055–68.
Lin G, Lin L, Lin H, Xu Y, Chen W, Liu Y, et al. C1QTNF6 regulated by miR-29a-3p promotes proliferation and migration in stage I lung adenocarcinoma. BMC Pulm Med. 2022;22:285.
Qu F, Zhu B, Hu Y-L, Mao Q-S, Feng Y. LncRNA HOXA-AS3 promotes gastric cancer progression by regulating miR-29a-3p/LTβR and activating NF-κB signaling. Cancer Cell Int. 2021;21:118.
Ma Y, Sun Y. miR-29a-3p inhibits growth, proliferation, and invasion of papillary thyroid carcinoma by suppressing NF-κB signaling via direct targeting of OTUB2. Cancer Manag Res. 2019;11:13–23.
Wang A, Xu Q, Sha R, Bao T, Xi X, Guo G. MicroRNA-29a inhibits cell proliferation and arrests cell cycle by modulating p16 methylation in cervical cancer. Oncol Lett. 2021;21:272.
Gong Y, Wan J-H, Zou W, Lian G-Y, Qin J-L, Wang Q-M. MiR-29a inhibits invasion and metastasis of cervical cancer via modulating methylation of tumor suppressor SOCS1. Future Oncol England. 2019;15:1729–44.
Gong H-L, Tao Y, Mao X-Z, Song D-Y, You D, Ni J-D. MicroRNA-29a suppresses the invasion and migration of osteosarcoma cells by regulating the SOCS1/NF-κB signalling pathway through negatively targeting DNMT3B. Int J Mol Med. 2019;44:1219–32.
Li D, Xu M, Wang Z, Huang P, Huang C, Chen Z, et al. The EMT-induced lncRNA NR2F1-AS1 positively modulates NR2F1 expression and drives gastric cancer via miR-29a-3p/VAMP7 axis. Cell Death Dis. 2022;13:84.
Zhao T-T, Liu X. LncRNA-H19 inhibits apoptosis of acute myeloid leukemia cells via targeting miR-29a-3p. Eur Rev Med Pharmacol Sci Italy. 2019;23:224–31.
Jin H, Wang H, Jin X, Wang W. Long non-coding RNA H19 regulates LASP1 expression in osteosarcoma by competitively binding to miR-29a-3p. Oncol Rep. 2021;46:207.
Yang F, Chen Y, Luo L, Nong S, Li T. circFOXO3 induced by KLF16 modulates clear cell renal cell carcinoma growth and natural killer cell cytotoxic activity through sponging miR-29a-3p and miR-122-5p. Dis Markers. 2022;2022:6062236.
Cai J, Qiao B, Gao N, Lin N, He W. Oral squamous cell carcinoma-derived exosomes promote M2 subtype macrophage polarization mediated by exosome-enclosed miR-29a-3p. Am J Physiol-Cell Physiol United States. 2019;316:C731–40.
Liu S, Liu D, Liu J, Liu J, Zhong M. miR-29a-3p promotes migration and invasion in ameloblastoma via Wnt/β-catenin signaling by targeting catenin beta interacting protein 1. Head Neck United States. 2021;43:3911–21.
Wu Y, Shi W, Tang T, Wang Y, Yin X, Chen Y, et al. miR-29a contributes to breast cancer cells epithelial-mesenchymal transition, migration, and invasion via down-regulating histone H4K20 trimethylation through directly targeting SUV420H2. Cell Death Dis. 2019;10:176.
Liu T, Wang W, Xu Y-C, Li Z-W, Zhou J. Long noncoding RNA NEAT1 functions as an oncogene in human laryngocarcinoma by targeting miR-29a-3p. Eur Rev Med Pharmacol Sci Italy. 2019;23:6234–41.
Chen Z-F, Wang Y, Sun L-L, Ding S-Y, Jinag H. LncRNA SNHG20 enhances the progression of oral squamous cell carcinoma by regulating the miR-29a/DIXDC1/Wnt regulatory axis. Eur Rev Med Pharmacol Sci Italy. 2020;24:5436–45.
Huang Y-H, Lian W-S, Wang F-S, Wang P-W, Lin H-Y, Tsai M-C, et al. MiR-29a Curbs hepatocellular carcinoma incidence via targeting of HIF-1α and ANGPT2. Int J Mol Sci. 2022;23:1636.
Hao WY, Guo LW, Luo J, Shao GL, Zheng JP. LncRNA TUG1 promotes growth and metastasis of cholangiocarcinoma cells by inhibiting miR-29a. Cancer Manag Res. 2020;12:11103–11.
Chen X, Zhu H, Ye W, Cui Y, Chen M. MicroRNA-29a enhances cisplatin sensitivity in non-small cell lung cancer through the regulation of REV3L. Mol Med Rep. 2019;19:831–40.
Wang J, Huang K, Shi L, Zhang Q, Zhang S. CircPVT1 Promoted the progression of breast cancer by regulating MiR-29a-3p-mediated AGR2-HIF-1α pathway. Cancer Manag Res. 2020;12:11477–90.
Zhang F, Luo B-H, Wu Q-H, Li Q-L, Yang K-D. LncRNA HCG18 upregulates TRAF4/TRAF5 to facilitate proliferation, migration and EMT of epithelial ovarian cancer by targeting miR-29a/b. Mol Med. 2022;28:2.
Chen Y, Zhang W, Yan L, Zheng P, Li J. miR-29a-3p directly targets Smad nuclear interacting protein 1 and inhibits the migration and proliferation of cervical cancer HeLa cells. PeerJ. 2020;8: e10148.
Nan P, Niu Y, Wang X, Li Q. MiR-29a function as tumor suppressor in cervical cancer by targeting SIRT1 and predict patient prognosis. OncoTargets Ther. 2019;12:6917–25.
Geng A, Luo L, Ren F, Zhang L, Zhou H, Gao X. miR-29a-3p inhibits endometrial cancer cell proliferation, migration and invasion by targeting VEGFA/CD C42/PAK1. BMC Cancer. 2021;21:843.
Li L-M, Hao S-J, Ni M, Jin S, Tian Y-Q. DUXAP8 promotes the proliferation and migration of ovarian cancer cells via down-regulating microRNA-29a-3p expression. Eur Rev Med Pharmacol Sci Italy. 2021;25:1837–44.
Li T, Sun X, Chen L. Exosome circ_0044516 promotes prostate cancer cell proliferation and metastasis as a potential biomarker. J Cell Biochem United States. 2020;121:2118–26.
Wang C, Li L, Li M, Wang W, Liu Y, Wang S. Silencing long non-coding RNA XIST suppresses drug resistance in acute myeloid leukemia through down-regulation of MYC by elevating microRNA-29a expression. Mol Med. 2020;26:114.
Qi S, Xu L, Han Y, Chen H, Cheng A. miR-29a-3p mitigates the development of osteosarcoma through modulating IGF1 mediated PI3k/Akt/FOXO3 pathway by activating autophagy. Cell Cycle. 2022;21:1980–95.
Zhang H, Yu Y, Wang J, Han Y, Ren T, Huang Y, et al. Macrophages-derived exosomal lncRNA LIFR-AS1 promotes osteosarcoma cell progression via miR-29a/NFIA axis. Cancer Cell Int. 2021;21:192.
Wang Y, Zhang L, Pang Y, Song L, Shang H, Li Z, et al. MicroRNA-29 family inhibits rhabdomyosarcoma formation and progression by regulating GEFT function. Am J Transl Res. 2020;12:1136–54.
Lu L, Ling W, Ruan Z. TAM-derived extracellular vesicles containing microRNA-29a-3p explain the deterioration of ovarian cancer. Mol Ther-Nucleic Acids. 2021;25:468–82.
Sikder S, Kumari S, Kumar M, Sen S, Singhal NB, Chellappan S, et al. Chromatin protein PC4 is downregulated in breast cancer to promote disease progression: Implications of miR-29a. Oncotarget. 2019;10:6855–69.
Chen XM, Johns DC, Geiman DE, Marban E, Dang DT, Hamlin G, et al. Kruppel-like factor 4 (Gut-enriched Kruppe-llike factor) inhibits cell proliferation by blocking G(1)/S progression of the cell cycle. J Biol Chem Bethesda Amer Soc Biochem Mol Biol Inc. 2001;276:30423–8.
Zhao WD, Hisamuddin IM, Nandan MO, Babbin BA, Lamb NE, Yang VW. Identification of Kruppel-like factor 4 as a potential tumor suppressor gene in colorectal cancer. Oncogene Lon Nat Publish Group. 2004;23:395–402.
Ma Y, Lin Wu, Liu X, Yuqiao Xu, Shi W, Liang Ye, et al. KLF4 inhibits colorectal cancer cell proliferation dependent on NDRG2 signaling. Oncol Rep Athens: Spandidos Publ Ltd. 2017;38:975–84.
Yuan L-L, Li L, Liu J-N, Mei J, Lei C-J. Down-regulation of miR-29a facilitates apoptosis of colorectal carcinoma cell SW480 and suppresses its Paclitaxel resistance. Eur Rev Med Pharmacol Sci. 2018;22:5499–507.
Wang J, Xu J, Fu J, Yuan D, Guo F, Zhou C, et al. MiR-29a regulates radiosensitivity in human intestinal cells by targeting PTEN gene. Radiat Res Lawrence Radiat Res Soc. 2016;186:292–301.
Zheng Z, Cui H, Wang Y, Yao W. Downregulation of RPS15A by miR-29a-3p attenuates cell proliferation in colorectal carcinoma. Biosci Biotechnol Biochem Abingdon: Taylor Francis Ltd. 2019;83:2057–64.
Zhao Q, Zhuang K, Han K, Tang H, Wang Y, Si W, et al. Silencing DVL3 defeats MTX resistance and attenuates sternness via notch signaling pathway in colorectal cancer. Pathol Res Pract. 2020;216:152964.
Zheng X-Y, Cao M-Z, Ba Y, Li Y-F, Ye J-L. LncRNA testis-specific transcript, Y-linked 15 (TTTY15) promotes proliferation, migration and invasion of colorectal cancer cells via regulating miR-29a-3p/DVL3 axis. Cancer Biomark Sect Dis Markers. 2021;31:1–11.
East MP, Asquith CRM. CDC42BPA/MRCKα: a kinase target for brain, ovarian and skin cancers. Nat Rev Drug Discov. 2021;20:167–167.
Huang C, Liu H, Gong X-L, Li-Yun Wu, Wen B. Effect of evodiamine and berberine on the interaction between DNMTs and target microRNAs during malignant transformation of the colon by TGF-β1. Oncol Rep. 2017;37:1637–45.
Gerovska D, Garcia-Gallastegi P, Crende O, Marquez J, Larrinaga G, Unzurrunzaga M, et al. GeromiRs are downregulated in the tumor microenvironment during colon cancer colonization of the liver in a murine metastasis model. Int J Mol Sci Basel Mdpi. 2021;22:4819.
Ding Q, Chang C-J, Xie X, Xia W, Yang J-Y, Wang S-C, et al. APOBEC3G promotes liver metastasis in an orthotopic mouse model of colorectal cancer and predicts human hepatic metastasis. J Clin Invest. 2011;121:4526–36.
Shi X, Valizadeh A, Mir SM, Asemi Z, Karimian A, Majidina M, et al. miRNA-29a reverses P-glycoprotein-mediated drug resistance and inhibits proliferation via up -regulation of PTEN in colon cancer cells. Eur J Pharmacol Amst Elsevier. 2020;880:173138.
Kapral M, Wawszczyk J, Węglarz L. Regulation of microrna-155 and Its related genes expression by inositol hexaphosphate in colon cancer cells. Molecules. 2019;24:4153.
Kim H-Y, Kim Y-M, Hong S. Astaxanthin suppresses the metastasis of colon cancer by inhibiting the MYC-mediated downregulation of microRNA-29a-3p and microRNA-200a. Sci Rep Lond Nat Publ Group. 2019;9:9457.
Parakrama R, Fogel E, Chandy C, Augustine T, Coffey M, Tesfa L, et al. Immune characterization of metastatic colorectal cancer patients post reovirus administration. Bmc Cancer Lond Bmc. 2020;20:569.
Wang J, Xu J, Fu J, Yuan D, Guo F, Zhou C, et al. MiR-29a Regulates Radiosensitivity in Human Intestinal Cells by Targeting PTEN Gene. Radiat Res. Lawrence: Radiation Research Soc; 2016;186:292–301.
Chen B, Wang J, Wang J, Wang H, Gu X, Tang L, et al. A regulatory circuitry comprising TP53, miR-29 family, and SETDB1 in non-small cell lung cancer. Biosci Rep. 2018;38:BSR20180678.
Xinming, Chen David C, Johns Deborah E, Geiman Eduardo, Marban Duyen T, Dang Gina, Hamlin Ronggai, Sun Vincent W, Yang. Krüppel-like Factor 4 (Gut-enriched Krüppel-like Factor) Inhibits Cell Proliferation by Blocking G1/S Progression of the Cell Cycle. Journal of Biological Chemistry. 2001;276(32):30423–30428:S0021925820897555. https://doi.org/10.1074/jbc.M101194200.
Funding
This study wasn’t funded by any project.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study's conception and design.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent to publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mo, WY., Cao, SQ. MiR-29a-3p: a potential biomarker and therapeutic target in colorectal cancer. Clin Transl Oncol 25, 563–577 (2023). https://doi.org/10.1007/s12094-022-02978-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-022-02978-6