
Abstract
Purpose
Soft tissue sarcomas are a heterogeneous group of rare tumours of mesenchymal origin. Evidence mapping is one of the most didactic and friendly approaches to organise and summarise the range of research activity in broad topic fields. The objective of this evidence mapping is to identify, describe and organise the current available evidence about therapeutic interventions on soft tissues sarcomas.
Methods
We followed the methodology of global evidence mapping. We performed a search of the PubMed, EMBASE, The Cochrane Library and Epistemonikos to identify systematic reviews (SRs) with or without meta-analyses published between 1990 and March 2016. Two independent literature reviewers assessed eligibility and extracted data. Methodological quality of the included systematic reviews was assessed using AMSTAR. We organised the results according to identified PICO questions and used tables and a bubble plot to display the results.
Results
The map is based on 24 SRs that met eligibility criteria and included 66 individual studies. Three-quarters were either observational or uncontrolled clinical trials. The quality of the included SRs was in general moderate or high. We identified 64 PICO questions from them. The corresponding results mostly favoured the intervention arm.
Conclusions
This evidence mapping was built on the basis of SRs, which mostly included non-experimental studies and were qualified by the AMSTAR tool as of moderate quality. The evidence mapping created from PICO questions is a useful approach to describe complex and huge clinical topics through graphical media and orientate further research to fulfil the existing gaps. However, it is important to delimitate the steps of the evidence mapping in a pre-established protocol.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
Soft tissues sarcomas (STS) are a group of rare tumours of mesenchymal origin, with an estimated incidence of 4.74 per 100,000 adults per year in Europe [1,2,3], whilst in children they represent 7–10% of all childhood cancers [4]. The research on STS poses some challenges due to the heterogeneity and rarity of the cases, a broad range of classification into the different subtypes and the tendency to pool sarcoma subtypes to show the outcomes [5]. In addition, access to summarised, comprehensive and updated information in this clinical field is limited.
Poor access to good research evidence is the most reported barrier to make well-informed clinical decisions [6, 7]. New, faster and emerging strategies have been launched to overcome those difficulties [8]. Evidence mapping is one of the most didactic and friendly approaches to organise and summarise the range of research results in very extensive areas, allowing to systematically characterise the evidence, identify gaps in knowledge and prioritise new research questions. This strategy can be the first approach to conduct a further systematic review or to provide a framework to inform policy development [9,10,11,12].
The goal of this evidence mapping is to identify, describe and organise the current available evidence about therapeutic interventions on sarcomas. Due to the vast diversity of sarcoma types, the results were split into two groups: gastrointestinal stromal tumour (GIST) and soft tissues sarcomas (STS). In a previous paper, we reported the results corresponding to GIST [13].
Methods
We carried out an evidence map according to the methodology of Global Evidence Mapping (GEM) [10] and adding some new components: an exhaustive search strategy and the assessment of methodological quality of the included systematic reviews (SRs). We divided the process into four stages, the two first stages have been described widely elsewhere [13].
-
1.
Setting the boundaries and context of the evidence map:
To frame our mapping project, we consulted the 2013 World Health Organization (WHO) classification [14] and the relevant clinical practise guidelines (CPG), combined with the consultation to an experienced oncologist in the field. We selected SRs that evaluated therapeutic interventions in patients diagnosed with STS, which included either experimental or non-experimental studies. We excluded studies focused on Kaposi sarcoma and/or Ewing’s tumours because of their unique biological characteristics and management [15, 16].
-
2.
Search and selection of systematic reviews:
We carried out a highly sensitive search strategy in PubMed, EMBASE, The Cochrane Library, and Epistemonikos databases from 1990 to November 2016. The detailed search strategies are listed in Online Resource 1.
-
3.
Data analysis:
We defined a data extraction tailored form to register the main characteristics and quality of the included SRs. We tested this form to ensure consistency among reviewers in a pilot study with 20% of the eligible SRs. Two independent literature reviewers extracted data (MB, NM). Discrepancies were solved by discussion with a third author (AL). We included all types of treatment regardless of whether it was being used or not in the current clinical practice. We collected data according to three levels:
-
(a)
General characteristics from SRs: authors, year of publication, type of SR (with or without meta-analysis), objective, search strategy design and number of included studies, type and number of patients included, and quality of the systematic review. The quality of included SR was evaluated by two independent reviewers (MB, NM) using the AMSTAR tool. Discrepancies were discussed and solved with a third author (AL). We obtained AMSTAR scores by summing one point for each item rated as “yes” and no points for items rated as “no”, “can´t answer” and “not applicable”, resulting in an overall score ranging from 0 to 11. SRs were grouped in three categories: 0–3 points (low quality), 4–7 points (moderate quality) and 8–11 points (high quality) [17].
-
(b)
Assessment of the clinical questions within the SRs: we elaborated PICO questions (specifying its four key components: population, intervention, comparison and outcomes) based on SR objectives and eligibility criteria.
The PICOs were grouped into three main clinical scenarios: localised disease, advanced disease and specific STS subtypes (uterine, retroperitoneal sarcomas and other rare specific subtypes). We then retrieved details about the participants’ characteristics (e.g. adult population or children, type of sarcoma, localisation of tumours); the intervention and its referent when existing (e.g. type of intervention and its control group broadly categorised as chemotherapy, surgery, radiotherapy and others); characteristics of the intervention; and comparison; and the outcomes. For descriptive purposes, we also classified the conclusions reported by the authors of the included studies into five categories: “inconclusive”, “no effect”, “harmful”, “probably beneficial” and “beneficial” (see Table 1 for further detail of the criteria followed for this categorisation). This classification does not represent any formal evaluation of the interventions’ effectiveness.
-
(c)
Characteristics of other research questions addressed in the SRs, here considered as secondary PICOs: we defined as secondary those research questions that had all the elements of the PICO question, but the conclusions about the direction of the effect were barely described in the article. We extracted the same information described above for the main research question.
Based on the PICO format, we summarised the synthesizing findings for each included review in:
-
(a)
Table describing the characteristics of the included SRs, and another one with all identified PICOs (main and secondary).
-
(b)
Graphic display of the mapping based on bubble plots, where each bubble represents one SR. This graphic provides information in three dimensions: (1) in the x-axis, there is the rating of authors conclusions as “beneficial”, “probably beneficial”, “harmful”, “no effect” and “inconclusive” (they were further described in the data extraction section); (2) in the y-axis, the AMSTAR assessment is shown; and (3) we displayed the bubble size proportionally to the number of individual studies included in the SR. Each bubble is also a pie graph which represents with a black bold line the proportion of RCTs included in the respective SR.
Results
We retrieved 1791 records once duplicates were removed. In total, 143 articles were deemed potentially relevant by at least one reviewer and, therefore, the full text was obtained. A total of 41 citations fulfilled the eligibility criteria, of which 24 SRs referred to STS and the remaining 17 SRs to GIST. A flowchart is detailed in Fig. 1. The reasons for exclusion of the 102 reviews publications are detailed in Online resource 2.

Flow chart outlining the study selection process
Characteristics and quality of systematic reviews
Our final sample consisted of 24 SRs focusing on STS [15, 18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38], 8 of them included a meta-analysis [18, 21, 26, 30, 32, 33, 38]. All SRs were published between 2003 and 2016 which included studies carried out between 1973 and 2014. The search strategy was described in detail in only eight SRs [18, 21, 22, 27, 29, 31, 34, 38]. The SRs included a total of 279 primary studies, out of which 195 were observational studies (either prospective or retrospective), 41 were RCTs, 4 were non-randomised controlled trials and 39 were experimental non-controlled studies (mainly phase II trials). Nine SRs did not include any RCT [18, 22,23,24, 27, 29, 30, 35, 36], 1 was an empty review [27] and the remaining 15 included at least one [28, 29, 31,32,33,34, 37, 38]. The total number of patients analysed in the SRs ranged from 216 to 6467, all of them being adults.
According to the evaluated treatment, 13 SRs appraised chemotherapy therapies [15, 18, 21, 25,26,27, 30,31,32, 37,38,39]; 5 SRs evaluated radiotherapy interventions [19, 22, 23, 33, 36]; 2 SRs assessed surgical interventions [24, 34]; 1 SR assessed a combination of surgery (cytoreduction) plus intraperitoneal chemotherapy [28]; and finally 3 SRs assessed a therapy at the forefront named isolated limb perfusion (ILP) [20, 29, 35].
Thirteen SRs assessed interventions with a curative intention [19, 20, 22,23,24, 27, 29, 32,33,34,35,36, 40], whereas in the other 11 the interventions was palliative [15, 18, 21, 25, 26, 28, 30, 31, 37,38,39].
The most reported outcome was overall survival, where only 3 SRs did not report this outcome [24, 29, 35]; followed by response rate, which was informed in 13 SRs [15, 20, 21, 25,26,27, 29, 34,35,36,37,38,39]; progression-free survival and local or distant recurrence rate were described in nine reviews [19, 20, 22,23,24, 28, 32, 36, 40], whereas quality of life was appraised only in four SRs [15, 21, 27, 28]. Furthermore, 18 reviews [15, 18,19,20,21,22, 25,26,27,28,29,30,31, 35,36,37,38,39] informed about adverse events.
Based on AMSTAR scores, the quality of the included SRs was moderate to high, as seen in Fig. 2. The major drawbacks were: not detailing the included and excluded studies, not declaring potential conflicts of interest, not evaluating the likelihood of publication bias and not assessing the risk of bias of individual studies. The characteristics of the included SRs are reported in Table 2.

AMSTAR scores of the included SRs
PICO questions identified in systematic reviews
We retrieved 51 PICO questions from the SRs about STS, whose main characteristics are detailed in Online resource 3. According to the STS clinical stage, the PICOS were classified to encompass the full spectrum of the disease, from initial stages to metastatic disease, in the following eight clinical scenarios:
-
1.
Patients with localised resectable STS (First line): Four SRs [19, 32, 33, 40] were identified with a total of 27 RCTs and 32 observational studies, which addressed three different therapeutic options within this scenario. Two SRs compared different regimens of adjuvant chemotherapy [32, 40] mainly based in doxorubicin or doxorubicin plus ifosfamide with surgery. Adjuvant chemotherapy was considered by the authors as “probably beneficial” in one SR and as “inconclusive” in another SR.
One SR compared adjuvant radiotherapy [33] with surgery and its authors qualified this intervention as “probably beneficial”. Another SR compared neoadjuvant radiotherapy [19] with surgery, and as stated in the conclusion, the authors considered this intervention as “probably beneficial”. Evidence mapping is detailed in Fig. 3.
Fig. 3 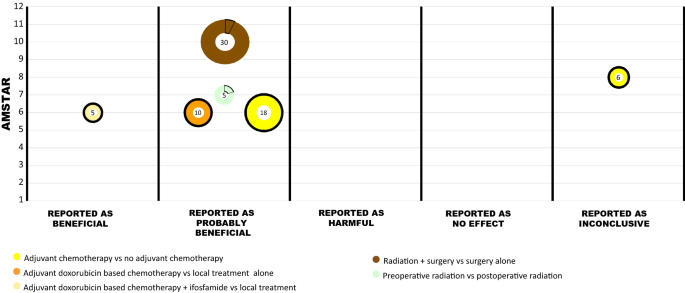
Evidence mapping of the therapeutic interventions for patients with localisable resectable STS (first line)
-
2.
Patients with locally advanced unresectable and/or metastatic STS (First Line): Six SRs [18, 21, 30, 31, 37, 38] included a total of 17 RCTs, 19 non-controlled trials and 5 observational studies, addressing mainly two therapeutic options in this scenario. Two SRs compared chemotherapy of doxorubicin-based combination versus doxorubicin alone. In general, the combined schemes were considered by authors as “harmful”, “no effect” and “inconclusive” depending on the different regimens assessed. Evidence mapping is detailed in Fig. 4.
Fig. 4 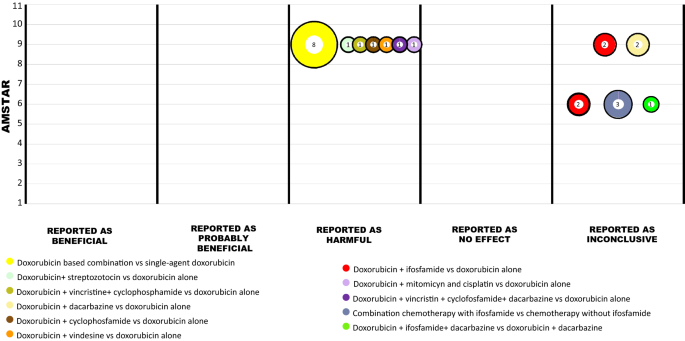
Evidence mapping of the therapeutic interventions for patients with locally advanced unresectable and/or metastatic STS (first line)


Four SRs [18, 30, 31, 37] compared dose-intensive chemotherapy by autologous bone marrow support, stem cell transplantation or growth factor with standard-dose chemotherapy. Two of them in patients diagnosed of rhabdomyosarcoma [18, 30]. In general, the results were stated by the authors as “harmful” and “inconclusive”. Evidence mapping is detailed in Fig. 5.

Evidence mapping of the therapeutic interventions for patients with locally advance STS
-
3.
Patients with unresectable, locally advanced STS of the extremities: Three SRs [20, 29, 35] evaluated the use of hyperthermic isolated limb perfusion (ILP) in these patients. In total, 4 RCTs were included, 9 non-controlled trials, and 38 observational studies. In general, the authors considered the results as “probably beneficial” and “inconclusive”. Evidence mapping is detailed in Fig. 5.
-
4.
Patients with locally advanced STS after failure of prior anthracyclines and ifosfamide (Second line): Two SRs [15, 39] included 7 RCTs, 3 non-controlled trials and 94 observational studies addressing four different therapeutic options in this scenario. One SR compared pazopanib versus placebo, and the authors considered pazopanib as “probably beneficial”. Gemcitabine plus dacarbazine was compared with dacarbazine alone in one SR, in which the authors considered combination as “inconclusive”. Trabectedin was compared with standard treatment in another SR, and the conclusion was stated as “inconclusive”. In this same SR, two different doses of trabectedin (1.5 mg three times per week versus 0.58 weekly) were compared. The authors considered that the use of higher doses of trabectedin as “probably beneficial”. Evidence mapping is detailed in Fig. 5.
-
5.
Patients with endometrial stromal sarcoma localised: One SR [34] including one RCT, one non-controlled trial and 84 observational studies evaluated three different therapeutic options in this population. The addition of lymphadenectomy to hysterectomy with salpingectomy, as well as ovarian sparing was qualified as “no effect” by the authors. Adjuvant radiotherapy was compared to surgery; this intervention was considered as “probably beneficial”. Evidence mapping is detailed Fig. 6.
-
6.
Patients with advanced, recurrent or metastatic uterine sarcomas: Three SRs [25, 26, 34], including four RCTs, 25 non-controlled trials and 84 observational studies addressed mainly two therapeutic options in this scenario. Combination chemotherapy was compared with a single chemotherapy agent in two SRs [25, 26]. Combination chemotherapy was considered as “no effect”, “inconclusive” and “probably beneficial”, depending on the subtype of uterine sarcoma and the different regimens used. Adjuvant hormonal therapy was compared with surgery in one SR, where adjuvant hormonal therapy was qualified as “probably beneficial”. Evidence mapping is detailed in Fig. 6.
Fig. 6 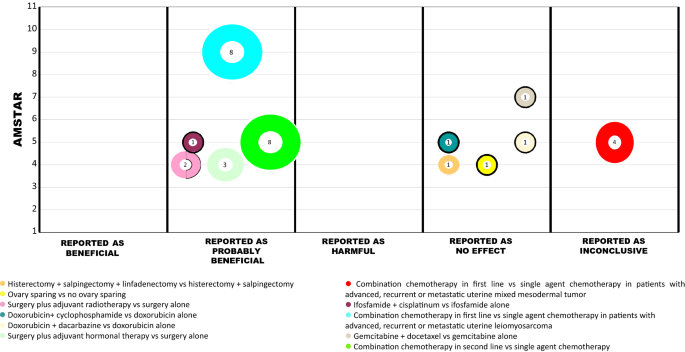
Evidence mapping of the therapeutic interventions for patients with uterine sarcomas
-
7.
Patients with retroperitoneal sarcoma: Two SRs [22, 36] evaluated different combinations of radiotherapy. In total, two non-controlled trials and 33 observational studies were included. The results were evaluated by the authors and considered as “probably beneficial” and “no effect” depending on different regimens assessed. Evidence mapping is detailed in Fig. 7.
Fig. 7 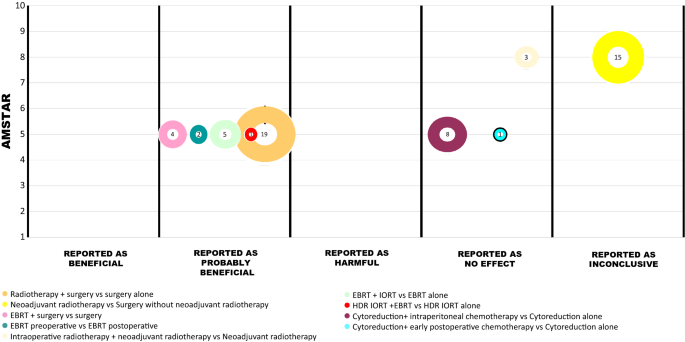
Evidence mapping of the therapeutic interventions for patients with retroperitoneal sarcomas and peritoneal sarcomatosis
-
8.
Special entities: Two comparisons were evaluated in patients with radiation-associated angiosarcoma within one SR [23]. Surgery plus radiotherapy was considered as “probably beneficial” compared with surgery alone, and surgery plus chemotherapy was considered as “no effect” compared with surgery alone.


In patients with dermatofibrosarcoma protuberans Mohs, micrographic surgery was considered as “probably beneficial” compared with wide local excision in one SR [24]. Finally, in patients diagnosed with peritoneal sarcomatosis the addition to intraperitoneal chemotherapy to cytoreduction was considered as “no effect” in one SR [28].
Discussion
Currently, there are several options to perform rapid systematic reviews to assess the effects of interventions among which are: rapid reviews, scoping review, evidence mapping, etc. The decision about the type to use should be selected depending on the topic, time for conduction and resources. In contrast, evidence mapping is a new methodological systematic approach whose purpose is to identify gaps in the existing knowledge and prioritise further research in very broad fields by displaying it in a friendly format. [9]. Its potential advantages include summarizing and displaying large quantity of information in an efficient and friendly way.
As a part of an evidence mapping project about sarcomas, we identified, described and organised the current available evidence about soft tissue sarcomas. In a previous paper, we reported the evidence mapping on gastrointestinal stromal tumours (GIST) [13], and now we focus on soft tissue sarcomas. We found 24 SRs including 279 individual studies. Same as described in the evidence maps for GIST, the majority of studies retrieved for STS (85%) were also non-randomised controlled trials (observational studies, or non-controlled, or non-randomised clinical trials), and in all but one the control group was placebo. For this reason, the evidence base in this area is weak, as non-experimental designs include information about treatment effects which may probably be biased or unreliable [41]. For instance, although some clinical practice guidelines (CPGs) recommend the combination of doxorubicin and ifosfamide as the most effective first-line chemotherapy for patients with locally advanced unresectable and/or metastatic STS [42], the authors of two SRs report this option as “inconclusive”. Likewise, one recent randomised controlled trial published did not observe any effect on overall survival and its use would only be justified if the specific therapeutic goal is tumour shrinkage [43].
Furthermore, CPGs recommend pazopanib as second-line chemotherapy in patients with advanced STS after failure of prior anthracyclines and ifosfamide [4, 44, 45]. However, the unique SR that addresses this issue reported this intervention as “probably beneficial” based on a single RCT where the control group was placebo [15].
According to our results, the majority of SRs addressed palliative treatments and only four SRs included quality of life as an outcome [15, 21, 27, 28], meanly because the majority of primary studies did not measure this outcome. Due to the fact that palliative care seeks the prevention and relief of suffering derived from pain and other physical problems, which in turn may positively affect quality of life, it is outstanding that most studies do not include this outcome to provide a comprehensive perspective of treatment effect. On the other hand, this outcome is essential to distinguish between treatments which have an effect on symptoms, but not necessarily equal impact over quality of life. Therefore, it should be measured in all studies conducted in sarcomas patients [46].
Our evidence maps used a new format to display the results graphically in order to facilitate the understanding and interpretation of them and make them user friendly. However, it should be noted that some graphs (bobble plots) included treatments that are not currently used, or are used only in specific clinical settings. For instance, it was the case for the bubble plot number two (different schemes of doxorubicin in patients with locally advanced unresectable and/or metastatic STS were plotted). In consequence, this graphic format itself does not inform about the best treatment option, but allows us to display the history of treatment along time. Hence, clinical experience is needed to identify the clinical utility and implications of it.
The overall quality of SRs applying the AMSTAR criteria was moderate to high. Nervertheless, as we detected in the GIST mapping, there are some domains that are less frequently reported: the reporting of excluded studies (only 4 studies out of 24 did it), the methods used to combine the findings of studies (7 out 24 did it), and the assessment of publication bias (3 out 24 did it).
Strengths
Although several methodologies have been proposed, we selected the one widely used and incorporated new components to make the tool more useful.
Although the evidence mapping methodology does not usually describe the type and quality of included studies, our mapping provided this type of information, which will eventually facilitate stakeholders to take a decision of the most suitable design in future research and identify the quality of the evidence in which clinical decisions are based.
We used the PICO format to organise the available information and describe the results applied to more specific scenarios according to current clinical practice. We believed that this approach is appropriate in clinical settings as it gives a better understanding and clarity to the description of the results. However, it is essential to define the PICOs from the beginning of the project, that is, since the protocol was designed. We also considered essential to include an expert on the topic and a methodologist as well, to improve and include the relevant perspectives in the analysis, presentation of results, discussion and conclusions.
The results of evidence mapping should ideally be displayed graphically, to synthesise the information in a friendly format. We considered that according to the amount the information is available it is important to define what type of specific graphic format is more illustrative. In fields where a huge amount of information is available, the bubble plots are a good option.
Limitations
As in the mapping of GIST we faced some limitations. Firstly, our SRs search was done in 2016, but their respective study searches were conducted in 2014 or earlier. Therefore, we have not detected other studies that may publish but are not included in the systematic reviews. Nevertheless, we are confident that these limitations would not substantially modify our results bearing in mind that the aim is to identify the gaps in the knowledge instead of supporting clinical decisions. In relation to this point, we considered that is important to establish what is the best type of study design to do the evidence maps (randomised controlled trial and/or observational studies), taking into account the subject of study, the time to do the mapping, and the objective of mapping the evidence (define the research gap to propose a research question or to conduct a SR). Secondly, as aforementioned in the GIST mapping, a drawback of this methodology is that it solely organises and describes the evidence as reported by the respective authors. Hence, some results could be described as beneficial even if they are based on non-experimental studies or low quality evidence. For this reason, this is not an appropriate tool for making clinical decision in health care.
Conclusions
This evidence mapping was built on the basis of SRs, which mostly included non-experimental studies and were qualified by the AMSTAR tool as of moderate quality. The evidence mapping created from PICO questions is a useful approach to describe complex and huge clinical topics through graphical media and orientate further research to fulfil the existing gaps. However, is important to delimitate the steps of the evidence mapping in a pre-established protocol.
Abbreviations
- AMSTAR:
-
Assessing the methodological quality of systematic reviews
- GEM:
-
Global Evidence Mapping Initiative
- GIST:
-
Gastrointestinal stromal tumours
- PICO:
-
Population, intervention, comparison, outcome
- RCT:
-
Randomised controlled trial
- SRs:
-
Systematic reviews
- WHO:
-
World Health Organization
References
Ducimetiere F, Lurkin A, Ranchere-Vince D, Decouvelaere AV, Peoc’h M, Istier L, et al. Incidence of sarcoma histotypes and molecular subtypes in a prospective epidemiological study with central pathology review and molecular testing. PLoS ONE. 2011;6(8):e20294 (Epub 2011/08/10).
Stiller CA, Trama A, Serraino D, Rossi S, Navarro C, Chirlaque MD, et al. Descriptive epidemiology of sarcomas in Europe: report from the RARECARE project. Eur J Cancer. 2013;49(3):684–95 (Epub 2012/10/20).
Gatta G, van der Zwan JM, Casali PG, Siesling S, Dei Tos AP, Kunkler I, et al. Rare cancers are not so rare: the rare cancer burden in Europe. Eur J Cancer. 2011;47(17):2493–511 Epub 2011/10/29.
Dangoor A, Seddon B, Gerrand C, Grimer R, Whelan J, Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res. 2016;6:20 (Epub 2016/11/29).
Thomas DM, Ballinger ML. Etiologic, environmental and inherited risk factors in sarcomas. J Surg Oncol. 2015;111(5):490–5 Epub 2014/10/23.
Ganann R, Ciliska D, Thomas H. Expediting systematic reviews: methods and implications of rapid reviews. Implement Sci IS. 2010;5:56 Epub 2010/07/21.
Lawani MA, Valera B, Fortier-Brochu E, Legare F, Carmichael PH, Cote L, et al. Five shared decision-making tools in 5 months: use of rapid reviews to develop decision boxes for seniors living with dementia and their caregivers. Syst Rev. 2017;6(1):56 (Epub 2017/03/17).
Haby MM, Chapman E, Clark R, Barreto J, Reveiz L, Lavis JN. What are the best methodologies for rapid reviews of the research evidence for evidence-informed decision making in health policy and practice: a rapid review. Health Res Policy Syst. 2016;14(1):83 (Epub 2016/11/26).
Miake-Lye IM, Hempel S, Shanman R, Shekelle PG. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst Rev. 2016;5:28 Epub 2016/02/13.
Bragge P, Clavisi O, Turner T, Tavender E, Collie A, Gruen RL. The global evidence mapping initiative: scoping research in broad topic areas. BMC Med Res Methodol. 2011;11:92 Epub 2011/06/21.
Jaramillo A, Welch VA, Ueffing E, Gruen RL, Bragge P, Lyddiatt A, et al. Prevention and self-management interventions are top priorities for osteoarthritis systematic reviews. J Clin Epidemiol. 2013;66(5):503-10e4 (Epub 2012/09/22).
Clavisi O, Bragge P, Tavender E, Turner T, Gruen RL. Effective stakeholder participation in setting research priorities using a global evidence mapping approach. J Clin Epidemiol. 2013;66(5):496-e2–502-e2 (Epub 2012/07/24).
Ballesteros M, Montero N, López-Pousa A, Urrutia G, Solá I, Rada G, Pardo-Hernandez H, Bonfil X. Evidence mapping based on systematic reviews of therapeutic interventions for gastrointestinal stromal tumors (GIST). MC Med Res Methodol. 2017;17(1):135
Chan KH, Chan CW, Chow WH, Kwan WK, Kong CK, Mak KF, et al. Gastrointestinal stromal tumors in a cohort of Chinese patients in Hong Kong. World J Gastroenterol WJG. 2006;12(14):2223–8 Epub 2006/04/13.
Sharma S, Takyar S, Manson SC, Powell S, Penel N. Efficacy and safety of pharmacological interventions in second-or later-line treatment of patients with advanced soft tissue sarcoma: a systematic review. BMC Cancer. 2013;13:385 Epub 2013/08/14.
Brierley JD, Gospodarowicz MK, Wittekind C, editors. The TNM classification of malignant tumours. 8th ed. New York: Wiley; 2017.
Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10 (Epub 2007/02/17).
Admiraal R, van der Paardt M, Kobes J, Kremer LC, Bisogno G, Merks JH. High-dose chemotherapy for children and young adults with stage IV rhabdomyosarcoma. Cochrane Database Syst Rev. 2010;12:CD006669 (Epub 2010/12/15).
Al-Absi E, Farrokhyar F, Sharma R, Whelan K, Corbett T, Patel M, et al. A systematic review and meta-analysis of oncologic outcomes of pre- versus postoperative radiation in localized resectable soft-tissue sarcoma. Ann Surg Oncol. 2010;17(5):1367–74 Epub 2010/03/11.
Bhangu A, Broom L, Nepogodiev D, Gourevitch D, Desai A. Outcomes of isolated limb perfusion in the treatment of extremity soft tissue sarcoma: a systematic review. Eur J Surg Oncol. 2013;39(4):311–9 Epub 2013/01/29.
Bramwell VH, Anderson D, Charette ML. Doxorubicin-based chemotherapy for the palliative treatment of adult patients with locally advanced or metastatic soft tissue sarcoma. Cochrane Database Syst Rev. 2003;3:CD003293 (Epub 2003/08/15).
Cheng H, Miura JT, Lalehzari M, Rajeev R, Donahue AE, Bedi M, et al. Neoadjuvant radiotherapy for retroperitoneal sarcoma: a systematic review. J Surg Oncol. 2016;113(6):628–34 Epub 2016/03/19.
Depla AL, Scharloo-Karels CH, de Jong MA, Oldenborg S, Kolff MW, Oei SB, et al. Treatment and prognostic factors of radiation-associated angiosarcoma (RAAS) after primary breast cancer: a systematic review. Eur J Cancer. 2014;50(10):1779–88 Epub 2014/04/16.
Foroozan M, Sei JF, Amini M, Beauchet A, Saiag P. Efficacy of Mohs micrographic surgery for the treatment of dermatofibrosarcoma protuberans: systematic review. Arch Dermatol. 2012;148(9):1055–63 (Epub 2012/09/19).
Gupta AA, Yao X, Verma S, Mackay H, Hopkins L. Systematic chemotherapy for inoperable, locally advanced, recurrent, or metastatic uterine leiomyosarcoma: a systematic review. Clin Oncol (R Coll Radiol). 2013;25(6):346–55 Epub 2013/01/09.
Kanjeekal S, Chambers A, Fung MF, Verma S. Systemic therapy for advanced uterine sarcoma: a systematic review of the literature. Gynecol Oncol. 2005;97(2):624–37 Epub 2005/05/03.
Mulder RL, Paulides M, Langer T, Kremer LC, van Dalen EC. Cyclophosphamide versus ifosfamide for paediatric and young adult bone and soft tissue sarcoma patients. Cochrane Database Syst Rev. 2015;9:CD006300 (Epub 2015/10/01).
Munene G, Mack LA, Temple WJ. Systematic review on the efficacy of multimodal treatment of sarcomatosis with cytoreduction and intraperitoneal chemotherapy. Ann Surg Oncol. 2011;18(1):207–13 Epub 2010/08/11.
Noorda EM, Vrouenraets BC, Nieweg OE, Van Coevorden F, Kroon BB. Isolated limb perfusion: what is the evidence for its use? Ann Surg Oncol. 2004;11(9):837–45 (Epub 2004/08/18).
Peinemann F, Kroger N, Bartel C, Grouven U, Pittler M, Erttmann R, et al. High-dose chemotherapy followed by autologous stem cell transplantation for metastatic rhabdomyosarcoma—a systematic review. PLoS ONE. 2011;6(2):e17127 (Epub 2011/03/05).
Peinemann F, Labeit AM. Autologous haematopoietic stem cell transplantation following high-dose chemotherapy for non-rhabdomyosarcoma soft tissue sarcomas: a Cochrane systematic review. BMJ Open. 2014;4(7):e005033 (Epub 2014/08/01).
Pervaiz N, Colterjohn N, Farrokhyar F, Tozer R, Figueredo A, Ghert M. A systematic meta-analysis of randomized controlled trials of adjuvant chemotherapy for localized resectable soft-tissue sarcoma. Cancer. 2008;113(3):573–81 (Epub 2008/06/04).
Qu X, Lubitz CC, Rickard J, Bergeron SG, Wasif N. A meta-analysis of the association between radiation therapy and survival for surgically resected soft-tissue sarcoma. Am J Clin Oncol. 2016;41:348–56 (Epub 2016/02/18).
Rauh-Hain JA, del Carmen MG. Endometrial stromal sarcoma: a systematic review. Obstet Gynecol. 2013;122(3):676–83 (Epub 2013/08/08).
Trabulsi NH, Patakfalvi L, Nassif MO, Turcotte RE, Nichols A, Meguerditchian AN. Hyperthermic isolated limb perfusion for extremity soft tissue sarcomas: systematic review of clinical efficacy and quality assessment of reported trials. J Surg Oncol. 2012;106(8):921–8 Epub 2012/07/19.
Van De Voorde L, Delrue L, van Eijkeren M, De Meerleer G. Radiotherapy and surgery—an indispensable duo in the treatment of retroperitoneal sarcoma. Cancer. 2011;117(19):4355–64 (Epub 2011/03/30).
Verma S, Younus J, Haynes AE, Stys-Norman D, Blackstein M. Dose-intensive chemotherapy with growth factor or autologous bone marrow or stem-cell transplant support in first-line treatment of advanced or metastatic adult soft tissue sarcoma: a clinical practice guideline. Curr Oncol (Toronto, Ont). 2008;15(2):80–4 Epub 2008/05/06.
Verma S, Younus J, Stys-Norman D, Haynes AE, Blackstein M. Meta-analysis of ifosfamide-based combination chemotherapy in advanced soft tissue sarcoma. Cancer Treat Rev. 2008;34(4):339–47 Epub 2008/03/04.
(CAMUH) CdAdMdUH. Trabectedin (Yondelis) in the treatment of soft tissue sarcomas. Trabectedina (Yondelis) en el tractament de sarcomes de teixits tous. Catalunya: Catalan Agency for Health Information, Assessment and Quality (CAHIAQ-formerly CAHTA);2010.
Ma XWBJ, Xilin B, Jiang RB, He ZS. Chemotherapy versus non-chemotherapy in the treatment of soft tissue sarcoma: a systematic review. Chin J Evid Based Med. 2010;10(5):618–24.
Helmchen H. Ethical issues in naturalistic versus controlled trials. Dialog Clin Neurosci. 2011;13(2):173–82 (Epub 2011/08/17).
Lopez-Pousa A, Martin Broto J, Martinez Trufero J, Sevilla I, Valverde C, Alvarez R, et al. SEOM clinical guideline of management of soft-tissue sarcoma (2016). Clin Transl Oncol. 2016;18(12):1213–20 Epub 2016/12/03.
Judson I, Verweij J, Gelderblom H, Hartmann JT, Schoffski P, Blay JY, et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: a randomised controlled phase 3 trial. Lancet Oncol. 2014;15(4):415–23 Epub 2014/03/13.
von Mehren M, Randall RL, Benjamin RS, Boles S, Bui MM, Casper ES, et al. Soft tissue sarcoma, version 2.2014. J Natl Compr Cancer Netw JNCCN. 2014;12(4):473–83 (Epub 2014/04/11).
ESMO/European Sarcoma Network Working Group. Soft tissue and visceral sarcomas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(Suppl 3):iii102–12 (Epub 2014/09/12).
Guzman Sabogal YR, Pla Vidal J, Sanchez Pedraza R, Ortuno Sanchez-Pedreno F, Gomez Guevara MC. Health-related quality of life in stroke patients questionnaire, short version (HRQOLISP-40): validation for its use in Colombia. BMC Neurol. 2016;16(1):246 (Epub 2016/11/30).
Acknowledgements
The authors would like to acknowledge Montse Leon for their assistance with the edition of this paper. Also to the Iberoamerican Cochrane Centre to support this study as part of Mónica Ballesteros' PhD thesis in the Universitat Autònoma de Barcelona.
Funding
This work was supported by a grant by the Grupo Español de Sarcomas (GEIS) (8a Beca GEIS José Ma Buesa de Ayuda a la Investigación en Sarcomas-Convocatoria 2014). The initiative and sole responsibility for this research lies entirely and exclusively with the authors who have acted with complete independence from the funder.
Author information
Authors and Affiliations
Contributions
Conceived the study: XB, GU, MB, NM. Designed the study: MB, NM, XB, GU, IS, HP. Analysed the data: MB, NM, ALP. Wrote the first draft of the manuscript: MB, NM. Contributed to the writing of the manuscript: MB, NM, IS, XB, GU, GR. Approved the final manuscript and conclusions: MB, NM, ALP, GU, GR, IS, HP, XB.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
Not applicable.
Informed consent
None.
Availability of data and material
The datasets generated and/or analysed during the current study are available in the figshare repository: https://www.figshare.com/s/9a304798a6f8d31346fb. https://www.figshare.com/s/a9fbd04d4b898decee63.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Ballesteros, M., Montero, N., López-Pousa, A. et al. Evidence mapping based on systematic reviews of therapeutic interventions for soft tissue sarcomas. Clin Transl Oncol 21, 1398–1412 (2019). https://doi.org/10.1007/s12094-019-02069-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-019-02069-z