
Abstract
The function of phagocytic and antigen presenting cells is of crucial importance to sustain immune competence against infectious agents as well as malignancies. We here describe a reproducible procedure for the quantification of phagocytosis by leukocytes in whole blood. For this, a pH-sensitive green-fluorescent protein- (GFP) like dye (Eos-FP) is transfected into infectious microroganisms. After UV-irradiation, the transfected bacteria emit green (≈5160 nm) and red (≈581 nm) fluorescent light at 490 nm excitation. Since the red fluorescent light is sensitive to acidic pH, the phagocytosed bacteria stop emitting red fluorescent light as soon as the phagosomes fuse with lysosomes. The green fluorescence is maintained in the phagolysosome until pathogen degradation is completed. Fluorescence emission can be followed by flow cytometry with filter settings documenting fluorescence 1 (FL 1, FITC) and fluorescence 2 (FL 2, phycoerythrin, PE). Eos-FP transfected bacteria can also be traced within phagocytes using microscopical techniques. A standardized assay has been developed which is suitable for clinical studies by providing clinicians with syringes pre-filled with fixed and appropriately UV-irradiated Eos-FP E. coli (TruCulture™). After adding blood or body fluids to these containers and starting the incubation at 37°C, phagocytosis by granulocytes proceeds over time. Cultures can be terminated at a given time by lysing red blood cells followed by flow cytometry. A pilot study demonstrated that Eos-FP E. coli phagocytosis and digestion was up-regulated in the majority of patients with either severe sepsis or septic shock as compared to healthy donors (p < 0.0001 after o/n incubation). Following treatment with recombinant human granulocyte colony-stimulating factor (rhG-CSF) in selected patients with sepsis, phagolysosome fusion appeared to be accelerated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Polymorphonuclear neutrophils (PMN) play a pivotal role in the unspecific immune response (Smith 1994). One of the first steps in the elimination of microorganisms is phagocytosis by PMN. Patients with impaired neutrophil function are at increased risk of developing sepsis that progresses to septic shock and multiple organ failure (Martin et al. 1989; (Vincent et al. 1998) with its accompanied high mortality rate (40% to 60%) (Casey et al. 1993; Friedman et al. 1998). Diminished function of PMN, such as phagocytic activity of granulocytes, may contribute to reduced elimination of microorganisms. As a result, infection can go on, leading to severe sepsis or septic shock. The improved diagnosis of neutrophil dysfunction in neonates is a highly requested tool in modern medicine (Melvan et al. 2010).
Granulocyte colony-stimulating factor (G-CSF), a hematopoietic growth factor, which is up-regulated during bacterial infections (Omori et al. 1992), plays a central role in functional recruitment and activation of mature and immature neutrophils (Kawakami et al. 1990; Weiss et al. 1999). In order to maintain successful anti-infective defense, endogenous production of G-CSF is indispensable for reproduction and functional activation of neutrophils. Worse outcome has been reported in patients with bacterial infections and low endogenous serum concentrations of G-CSF (Chen et al. 1995). Patients who recover from the infection showed an immediate increase of endogenous G-CSF serum concentrations and leukocyte counts, followed by a decrease (Kragsbjerg et al. 1996; Tanaka et al. 1996). The beneficial application of supplementation with myeloid growth factors, GM-CSF and G-CSF, has been a matter of discussion for many years (Carr et al. 2003).
Phagocytosis is a process to inactivate pathogens and to sensitize the immune system for the generation of cytotoxic cells and specific antibodies against antigen specific helper T cells. A number of surface receptors are known to regulate activation of the phagocyte and its function, i. e. the uptake of antigens and intracellular degradation. These are chemokine- and Fc gamma-receptors (CD16, CD32, CD64), as well as intercellular adhesion molecule 1 (ICAM-1), integrins, CD11b, L-selectin, CD62-L and complement receptors (Seely et al. 2003). In severe sepsis associated with a high incidence of mortality (Casey et al. 1993; Friedman et al. 1998), a number of pathologies have been reported to cause anergy and death by nosocomial infections (Bone 1996). Amongst others, the Trojan horse theory may be put forward, suggesting that pathogens invade the organism and eventually are taken up and spread by phagocytes without being efficiently degraded. Therefore, pathogens may migrate to tissues sensitive for infections and cause lesions. Cytokines and growth factors play a major role in guiding the recruitment of neutrophil effectors to the periphery as well as to sites of infections. In this context, G-CSF has been demonstrated to play a major role (Furze and Rankin 2008).
To address the question of neutrophil function in healthy donors as compared to patients with sepsis and septic shock, we set up a test which can be used to simultaneously study i)pathogen phagocytosis and ii) the degradation of the phagocytosed particle when entering the lysosomal compartment. For this, E. coli bacteria were transfected with a pH-sensitive dye, Eos-FP which had been cloned from a coral Lobophyllia hemprichii (Wiedenmann et al. 2004). After irradiating the transfected bacteria with UV-light of 400 nm, peptide cleavage in Eos-FP occurs and the transfected bacteria emit green as well as red fluorescent light upon excitation with 490 nm (Wiedenmann et al. 2004). Interestingly, the green fluorescence is quite stable whereas the red fluorescence is pH sensitive. For assay standardization, the UV-irradiated Eos-FP bacteria were fixed with paraformaldehyde, washed and the bacteria concentration was adjusted to the phagocytic capacity of granulocytes from healthy donors in 0.5 ml of whole blood. When whole blood was mixed with Eos-FP bacteria, the pathogens were taken up and eventually, phagosomes fused with lysosomes and the acidic pH resulted in the loss of the red fluorescent light, whereas the green fluorescent light emission was maintained as long as protein degradation was incomplete. Healthy donors were compared with sepsis patients. Individual sepsis patients were also tested before and after treatment with rhG-CSF (Neupogen®) (300 μg/24 h).
Methods
Eos-FP E. coli
A pH-sensitive green-fluorescent protein- (GFP) like dye (Eos-FP), cloned from a coral Lobophyllia hemprichii was transfected into E. coli K12. After growing the bacteria to a cell density of 1010 bacteria/ml, the fluorescent micro organisms were irradiated with a UV light source of 400-nm to induce peptide cleavage of a majority of Eos-FP molecules resulting in fluorescence emission from green (520 nm) to red (580 nm) at 490 nm excitation (Wiedenmann et al. 2004) (Patent 102006062398.3). The irradiated bacteria were then fixed with 3.5% paraformaldehyde (electron microscopical grade, http://www.emsdiasum.com) and washed in sterile phosphate buffered saline.
Assay development
The amount of 1 × 108 fluorescent bacteria per 2 ml of RPMI1640, 25 mM Hepes, 100U/ml sodium heparin were filled into TruCulture™ containers (EDI-GmbH, Reutlingen, Germany) designed to be filled with 0.5 ml of fresh heparinized (50 IU/ml) peripheral blood. The containers were stored at +4° for 1 week or at −20°C for several weeks in the dark until used.
For assay-performance, Eos-FP-TruCultures were thawed and adjusted to room temperature. Whole blood was added to the first tube, which was placed on ice after 1 min following gentle mixing. For other time points, the Eos-FP-TruCultures™ were mixed with 0.5 ml of whole blood, gently mixed and placed into an incubator (37°C) in an upright position. After 30 min, 60 min, 120 min and following overnight (o/n) incubation, the TruCultures™ were removed from the incubator and phagocytosis was terminated on ice. The supernatant was removed and sedimented blood was subjected to 5 ml of lysing buffer (BD-Biosciences) to remove red cells. Following 2 washes with PBS, the cell suspension was ready to be analyzed by flow cytometry. Non-specific adhesion of fluorescent bacteria were tested by analyzing blood samples mixed with Eos-FP bacteria for 1 min (Santos et al. 1995).
Fluorescence microscopy and flow cytometric analysis (FACS)
White blood cell populations were gated into lymphocytes (R1), monocytes and macrophages (R2) and neutrophils (R3) using forward and side scatter analysis in a FACScalibur (BD Biosciences). Supplementary Figure 1 shows, how granulocytes were gated by scatter analysis. The gated granulocyte population was identified by surface staining of CD45 and CD14. A larger set of monoclonal antibodies specifically binding to granulocytes (CD16, CD33), monocytes/macrophages (HLA-DR) and lymphocytes (CD2, CD19) was also used (data not shown). In order to distinguish surface-bound bacteria from those being engulfed by the phagocytes, we compared flow cytometric results of samples treated with and w/o methylene blue to quench the fluorescence of extracellular E. coli. We also performed short-term incubation of Eos-FP E. coli in whole blood (1 min) according to Santos and colleagues (Santos et al. 1995) Fluorescence of phagocytes with ingested bacteria was determined by documentation of green (fluorescence 1 (FITC channel), FL1) and red fluorescence (fluorescence 2 (PE channel), FL2). Results were recorded as the percentage of granulocytes emitting green plus red fluorescence after a defined culture period and as mean fluorescence intensity (MFI) related to the amount of ingested fluorescent pathogens (MFI are calculated by the following formula: \( \left[ {\hbox{percent positive cells}} \right] \times \left[ {\hbox{mean channel fluorescence}} \right] - \left[ {\hbox{percent positive cells in the negative control}} \right] \times \left[ {\hbox{mean channel of the negative control}} \right] \)). We also determined the ratio of green to red fluorescence as a measure of phagosome-lysosome fusion. For documentation of the results we used CellQuest software (BD Biosciences).
Standard fluorescence microcopy with an upright microscope (Zeiss) using with an excitation filter 450–490 nm, FT510 and LP 520 nm, 63× oil immersion objective was applied. A confocal laser scanning microscope (Zeiss LSM501 meta, 63× objective) was used for spectral light emission analysis and z-stack analysis (0.5 μm/section, LSM 501 meta™ software (Zeiss.de) for localization of intra- vs. extracellular bacteria. In selected experiments cultured macrophages were applied for improved spatial resolution in the cytoplasm. IBIDI™ μ-slides (Ibidi.de) were used throughout.
Patients
Seventeen patients with severe sepsis (n = 5) and septic shock (n = 12) admitted at the Intensive Care Unit (ICU), Dept. Anaesthesiology, University Hospital Ulm were included in this pilot study (Table 1). Sepsis, was defined by the 1992 American College of Chest Physicians / Society of Critical Care Medicine (ACCP/SCCM) consensus conference definitions (American 1992). Severe sepsis was defined as sepsis plus organ dysfunction. As recommended (Vincent et al. 1998), in the present study, applying the 1992 sepsis definitions, organ failure was regarded to be present if patients had lactic acidosis or oliguria, or reached greater than two points in one organ system (lung, coagulation, liver, kidney) using the SOFA (Sepsis-related Organ Failure Assessment) score. Septic shock was defined as sepsis plus shock. Shock was defined as hypotension despite adequate volume resuscitation, a systolic blood pressure of ≤90 mmHg, or the need for vasopressors to keep blood pressure greater than 90 mmHg. Stages of sepsis and the SOFA score were monitored on a daily basis to assess the severity of illness. In a pilot study approved by the local ethics committee, aimed at the evaluation of immune function in patients under intensive care treatment, the function to ingest Eos-FP bacteria was analyzed by comparing n = 17 patients with severe sepsis or septic shock with 28 healthy donors without current infection. Table 1 summarizes the patients’ characteristics.
Statistics
Comparisons among values for all groups were performed with an analysis of variance (ANOVA). The phagocytosis (uptake of fluorescent bacteria) and digestion (decline of red fluorescence emission of ingested Eos-FP E. coli) bacteria in healthy volunteers and in patients with severe sepsis were compared by describing. The Mann-Whitney U-test was applied to compare phagocytosis and digestion of Eos-FP E. coli data between healthy volunteers and patients with sepsis. A p-value of less than 0.05 was considered significant.
Results
Fluorescence emission of Eos-FP-transfected E. coli by confocal laser scanning microscopy
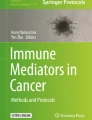
Isolated granulocytes were with fixed and UV-irradiated Eos-FP-transfected E. coli in medium containing 5% human serum for different periods of time. Phagocytes were washed once and microscopy was performed on 15well µ-slides (Ibidi™). When using standard fluorescence microscopy and excitation with 450–490 nm fluorescent light and a FT 510 nm and LP 520 nm filter combination, non-digested Eos-FP bacteria appear in an orange color and phagocytosed Eos-FP emitted only green fluorescent light (Fig. 1). Confocal scanning microscopy and spectral analysis of the emitted light was used to study the fluorescence emission of isolated bacteria labeled as a region of interest (ROI). According to the information given in Fig. 1b, c, undigested Eos-FP E. coli emit green (515 nm) and red (575 nm) fluorescent light (ROI2 and 3, Fig. b, c), whereas Eos-FP bacteria that has entered the lysosomal compartment lack red fluorescent light emission (ROI4, Fig. 1b, c). The peak height of light emission is directly related to fluorescence intensity. Following proteolytic degradation ingested Eos-FP bacteria eventually completely lose fluorescence (data not shown in Fig. 1).

Fluorescence imaging of phagocytes after 3 h Eos-FP phagocytosis. Standard immune fluorescence microscopy using excitation filter 450–490 nm, FT510 and LP 520 nm , 63× oil immersion microscopy and Ibidi μ-slides. The distally located bacteria have just been phagocytozed and emit green and red fluorescent light (appearing orange in color). The phagocytosed bacteria entering the lysosomal compartment are partially degraded and emit only green fluorescent light (a). Confocal scanning microscopical image (Zeiss 510 Meta spectral analysis, 63× oil immersion objective), and spectral analysis of individual regions of interest (ROI) are labeled as colored crosses (region of interest, ROI2: green, ROI3: blue, ROI4: yellow). The phagocytes’ nuclei appear dark and are encircled by a dotted line. Bacteria appear turquoise in color (b). Spectral analysis of ROI2 (green) reveals two peaks of emitted fluorescent light at ≈515 nm and at ≈575–580 nm. ROI3 (blue) shows the same peaks of fluorescent light at 515 nm and 580 nm, however, the 580 nm peak is less intense. ROI4 (yellow) shows fluorescence emission at 515 nm, only (c)
Detection of phagocytosis of Eos-FP labeled E. coli using flow cytometry
When testing whole blood samples of several individuals at a time, flow cytometry is a suitable method to quantify Eos-FP E. coli phagocytosis and subsequent degradation in the lysosomal compartment. For this procedure, the amount of bacteria has been adjusted to complete uptake and digestion by polymorph nuclear cells in 0.5 ml of whole blood (diluted in 2.0 ml of serum-free culture medium) and a defined incubation time of less than 24 h. Representative dot blots and gating strategies to identify lymphocytes, granulocytes and lymphocytes are shown in Fig. 2a. Figure 2b demonstrates a representative example of whole blood flow cytometric analysis after various incubation times. After one minute, the granulocyte population lacks any fluorescence, indicating that there was no non-specific adhesion of Eos-FP E. coli to the granulocyte fraction. After 30 min, about 50% of the granulocyte fraction emit green (FL 1) as well as red (FL 2) fluorescent light due to phagocytosis of Eos-FP E. coli. After 60 min and 120 min of incubation, the relative amount of red fluorescence is gradually declining. After o/n incubation, almost 100% of granulocytes lack red fluorescence but green fluorescence remains. Almost all granulocytes appear in the lower right quadrant of the dot plot (Fig. 2b). The specificity of gating is demonstrated by the distinct expression of the leukocyte common antigen CD45 as well as CD14 (supplementary Figure 1A, B) using FITC and phycoerythrin- (PE-) labeled monoclonal antibodies. CD45 density is characteristically lower on granulocytes as compared to eosinophiles and monocytes, respectively. In selected experiments performed with sepsis patients, the granulocytes’ expression of the following myloid differentiation antigens has been performed: CD11b (integrin), CD16 (FcR typeII), CD64 (FcRtypeI), CD62L, CD33 (myeloid antigen) as well as HLA-DR (data not shown, (Woehrle et al. 2008)). After a series of healthy donors’ blood samples (n = 28) had been tested, fresh blood of 17 patients with severe sepsis or septic shock was subjected to Eos-FP E. coli phagocytosis.

Fluorescence of granulocytes gated from whole blood phagocytosis assays with Eos-FP E. coli. Scatter analysis (forward scatter, FSC: x-axis, and side scatter, SSC: y-axis) of Eos-FP E. coli whole blood culture terminated after 1 min (control), 30 min, 60 min, 120 min and o/n (A). Fluorescence 1 (FL 1, green, x-axis); fluorescence 2 (FL 2, red, y-axis) of granulocytes after 1 min, 30 min, 60 min, 120 min, and o/n of whole blood with Eos-FP E. coli. (B) Percent positive granulocytes emitting green plus red fluorescence are given in the upper right quadrant and granulocytes emitting green fluorescence only are given in the lower right quadrant
Phagocytosis of Eos-FP labeled E. coli in patients with sepsis
As summarized in Fig. 3, the fluorescence emission of granulocytes phagocytosing Eos-FP E. coli increases with the time of incubation. It is more suitable to monitor the stable green fluorescence emission, given as mean fluorescence intensity (MFI). There is higher phagocytic activity in sepsis patients as compared with healthy donors. The difference reaches significance after 120 min (p < 0.05) and after o/n incubation (p < 0.001).

Total fluorescence detected in granulocytes of healthy donors and sepsis patients after different incubation times with Eos-FP transfected bacteria. Green fluorescence emission (given as mean fluorescence intensity (MFI on the y-axis) was detected in granulocytes of healthy donors and sepsis patients after different times of incubation with Eos-FP transfected bacteria (x-axis). Significant differences between groups are indicated by an asterix* above the scatter plots
Phagosome-lysosome fusion kinetics of Eos-FP E. coli in patients with sepsis
Figure 4 demonstrates that granulocytes of patients with sepsis show a faster loss of red fluorescence emission due to phagosome-lysosome fusion events. The red fluorescence of Eos-FP is highly sensitive to acidic pH. Thus the earlier the decline of the red fluorescence is observed, the more efficient or the more rapid is the phagosome-lysosome fusion process. This effect can be quantified by calculating the ratio of the mean fluorescence intensity of the green fluorescence divided by the mean fluorescence intensity of the red fluorescence. The differences between healthy donors and patients with sepsis were significant at all time points (p < 0.001) (Fig. 4).

Phagosome-lysosome fusion after Eos-FP E. coli phagocytosis of sepsis patients as compared to healthy donors. Ratios of green to red fluorescence (y-axis) indicate phagosome-lysosome fusion and acidic pH after Eos-FP E. coli phagocytosis. The medians of all incubation time points (x-axis) analyzed are different between sepsis patients and healthy donors. Significant differences between groups are indicated by an asterix* above the scatter plots
Phagosome-lysosome fusion kinetics of Eos-FP E. coli in patients with sepsis treated with recombinant human granulocyte colony-stimulating factor (rhG-CSF, Neupogen®)
Patients who did not up-regulate their leukocytes during sepsis (Weiss et al. 2003) were treated with 300 μg of recombinant human granulocyte-colony stimulating factor G-CSF (Neupogen®) per 24 h. Eos-FP phagocytosis demonstrates that and digestion analysis was performed before and after treatment. All our patients suffered from bacterial sepsis when examined in our study, their peripheral granulocyte population was often increased and a significant proportion of them displayed an immature phenotype. Exogenous growth factors may improve immune function against infectious agents. We investigated whether treatment rhG-CSF (300 μg infused in 24 h) would result in improved phagocytosis and lysosomal degradation of Eos-FP E. coli. Figure 5 demonstrates that G-CSF up-regulated phagocytosis in sepsis patients. In 4 out of 5 patients’ samples, o/n incubation resulted in less fluorescence emission after G-CSF treatment as compared to pre-treatment values. These results indicate that G-CSF also stimulated the degradation of phagocytosed bacteria including the Eoos-FP dye (Fig. 5a). The phagosome-lysosome function indicated by the loss of the pH-sensitive red fluorescent light emission was also up-regulated by G-CSF. There was one exception after o/n incubation, when post G-CSF isolates had a higher green/red ratio as compared to the pre-treatment value (Fig. 5b). In this small patient population, there was no correlation with death (red symbols) or survival of patients during their stay on intensive care (ICU).

Phagocytosis and phagosome-lysosome fusion in sepsis patients before and after treatment with rhG-CSF (a). Phagocytosis is quantified by MFI (y-axis) after different time points (x-axis). MFI are in part higher when tested after G-CSF treatment up to 120 min. However, after o/n incubation all but one post-GSF specimen display less fluorescence than pre-G-CSF specimen (a). Phagosome-lysosome fusion is upregulated in all but one patient’s granulocytes post G-CSF treatment up to 120 min. Following o/n incubation, one isolate shows a delay in phagosome-lysosome fusion events (b). Red symbols are from patients who died during their stay on ICU
Discussion
The present investigation demonstrates that fluorescent dyes may be applied to simultaneously quantify phagocytosis and phagosome-lysosome fusion events in whole blood isolates. The present study extends currently available phagocytosis assays using FITC-labeled bacteria (Burow and Valet 1987; Rothe et al. 1992; Rothe and Valet 1988; Gille et al. 2009). These experimental set-ups are also similar to a previous study, when GFP transfected E. coli were applied (Bicker et al. 2008). In our procedure, we used fixed E. coli transfected with a novel GFP-like protein named Eos-FP. The irradiation of Eos-FP with UV light genereates a partially degraded molecule with pH-sensitive red fluorescent emission properties (Wiedenmann et al. 2004; Wiedenmann and Nienhaus 2006). Therefore, Eos-FP transfected E. coli are suitable i) to quantify phagocytic granulocytes (percent fluorescent granulocytes), ii) to quantify the amount of ingested bacteria (MFI, green fluorescence), and iii) to determine phagolysosome fusion (green-to-red ratio).
To establish this phagocytosis and digestion assay, we applied E. coli K12 for convenience but other pathogenic bacteria of interest can similarly used. Using confocal scanning microscopy and spectral analysis, individual bacteria can be located within or outside of the phagocyte. CLSM combined with computed imaging analysis enables us to observe these structures three-dimensionally in routinely processed light microscopic specimens (White et al. 1987). Confocal imaging reduces interference from out-of-focus structures and optical slices of 0.25 μm were applied for image analysis. Intracellular bacteria show various grades of reduced red fluorescent light but non-phagocytozed bacteria emitted the same intensity of green (518 nm) as well as red (581 nm) fluorescence upon excitation at 490 nm (Fig. 1). When using standard immune fluorescence, the non-digested bacteria appear orange in color and locate to the outer rim of the phagocyte. The fluorescent bacteria in the inner part of the phagocyte are only green fluorescent and many are also structurally degraded (Fig. 1a).
The unique dual emission wavelengths of Eos-FP make this dye suitable to be used by flow cytometry for quantification. The green fluorescence intensity (FL 1) correlates with the amount of phagocytozed pathogens; beyond that, the selective green to red fluorescence (FL 1 to FL 2 ratio) indicates phagosome-lysosome fusion. A quantitative loss of green fluorescence indicates proteolytic degradation of the ingested bacteria including the Eos-FP dye. According to the standards established here, we observed only in G-CSF-treated patients that full degradation of the phagocytosed bacteria occurred at the latest time point of o/n incubation (Fig. 5). The cell populations present in cell mixtures can be either identified by scatter analysis or stained by surface markers using fluorescence-labeled antibodies labeled which do not interfere with the emission spectrum of Eos-FP. The aim of the current study was the investigation of granulocyte-specific phagocytosis and digestion. Gating was done by scatter analysis and confirmation of CD45 and CD14 expression density (Canonico et al. 2004) in every blood sample tested by Eos-FP phagocytosis. In initial experiments, gating strategies were additionally evaluated by staining for other granulocyte-specific surface antigens such as CD13, CD15, CD16, CD64, CD32 (data not shown). Our Eos-FP phagocytosis and digestion assay uses fixed and fully dispersed bacteria which can be either stored at 4°C in the dark or in a frozen state using pre-filled syringes designed as TruCulture™. Thus the assay is unique in being able to perform patients’ studies in different centers and to fuse the analysis into larger cohort studies. The effects of various medications on the function of phagocytes can be monitored as exemplified by rhG-CSF application in the present study. In the future, the Eos-FP construct may be further valid for testing the effect mediated by other bacterial products which may or may not influence the formation of the phagolysosome (Hines et al. 1999; Gorvel and Moreno 2002; Makino et al. 2007). Importantly, the intracellular processing of pathogens is related to the activation of the immune system as much as the inflammatory response as such. Sustained immunity against a pathogen is accomplished by uptake, degradation, and processing and antigen presentation, leading to the sensitization of T- and B-cell immunity. The generation of protein-derived peptides preferentially occurs in professional antigen presenting cells and the machinery of proteasome-guided degradation. However, DNA-vaccines have proven that our understanding of intracellular trafficking as well as the chemistry of degradation is still incomplete. A more detailed analysis of GFP-derived proteins which can be used as tags to follow trafficking processes in an antigen presenting cell may help to address open questions (Nienhaus and Wiedenmann 2009).
Results presented here confirm the previous notion that granulocytes of patients with sepsis have an increased functional capacity (Rothe et al. 1992) and are also less apoptotic (Weiss et al. 2003; Marshall et al. 2007). The inhibition of phagocytosis is a result of a number of growth factors produced in the inflammatory environment. Figure 5 summarizes that not all patients respond with increased phagocytosis, but almost all patients’ granulocytes showed up-regulated phagolysosome fusion after rhG-CSF infusion.
In the present study, the usefulness of Eos-FP E. coli to study processes which occur in the lysosomal compartment in human cells has been demonstrated. None of our patients suffering from either severe sepsis or septic shock had a profound deficiency to ingest and degrade Eos-FP E. coli. On the contrary, the majority of patients were far more active in both, the amount of pathogen uptake (Fig. 3) as well as its degradation as demonstrated by phagolysosome fusion, corresponding to a higher and faster increase of the green-to-red ratio (Fig. 4). Altogether, the current results demonstrate that a deficiency of granulocytes to ingest and degrade bacteria is not responsible for dissemination of pathogens through the body that contribute to deterioration during sepsis. Moreover, the present study shows that the here applied whole blood Eos-FP E. coli phagocytosis is valid to substantiate the effects of growth factor treatment in septic patients. Along these lines we found that in vivo application of rhG-CSF stimulated not only phagocytosis but also enhanced the velocity of the phagosome-lysosome fusion process accompanied by degradation of the ingested pathogen in 3 of 5 sepsis patients.
These results may contribute in clarifying the current discussion of the Trojan horse hypothesis to explain pathogen transmission throughout the body of a sepsis patient (Kim 2008). However, live bacteria have to be tested in the Eos-FP E. coli phagocytosis assay as well. As demonstrated before, the uptake and degradation of living pathogens is intrinsically different from that of dead organisms and the ratio of pathogens to phagocytes influences the fate of the neutrophils to either enter apoptosis or die by necrosis (Matsuda et al. 1999). All these questions can be addressed by application-dependent modifications of the currently described assay protocol.
References
American (1992) College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Committee: American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 20:864–874
Bicker H, Hoflich C, Wolk K, Vogt K, Volk HD, Sabat R (2008) A simple assay to measure phagocytosis of live bacteria. Clin Chem 54:911–915
Bone R (1996) Sir Isaac Newton, sepsis, SIRS, and CARS. Crit Care Med 24:1125–1128
Burow S, Valet G (1987) Flow-cytometric characterization of stimulation, free radical formation, peroxidase activity and phagocytosis of human granulocytes with 2, 7-dichlorofluorescein (DCF). Eur J Cell Biol 43:128–133
Canonico B, Zamai L, Burattini S, Granger V, Mannello F, Gobbi P, Felici C, Falcieri E, Reilly JT, Barnett D, Papa S (2004) Evaluation of leukocyte stabilisation in TransFix-treated blood samples by flow cytometry and transmission electron microscopy. J Immunol Methods 295:67–78
Carr R, Modi N, Dore C (2003) G-CSF and GM-CSF for treating or preventing neonatal infections. Cochrane Database Syst Rev:CD003066
Casey LC, Balk RA, Bone RC (1993) Plasma cytokine and endotoxin levels correlate with survival in patients with the sepsis syndrome. Ann Intern Med 119:771–778
Chen YM, Whang-Peng J, Chern CH, Kuo BIT, Wang SY, Perng RP (1995) The prognostic value of serum cytokine levels in patients with acute infections. Chin Med J (Taipei) 56:75–79
Friedman G, Silva E, Vincent JL (1998) Has the mortality of septic shock changed with time. Crit Care Med 26:2078–2086
Furze RC, Rankin SM (2008) Neutrophil mobilization and clearance in the bone marrow. Immunology 125:281–288
Gille C, Leiber A, Mundle I, Spring B, Abele H, Spellerberg B, Hartmann H, Poets Ch F, Orlikowsky TW (2009) Phagocytosis and postphagocytic reaction of cord blood and adult blood monocyte after infection with green fluorescent protein-labeled Escherichia coli and group B Streptococci. Cytometry B Clin Cytom 76B:271–284
Gorvel JP, Moreno E (2002) Brucella intracellular life: from invasion to intracellular replication. Vet Microbiol 90:281–297
Hines ME 2nd, Baldwin CA, Styer EL, Hullinger GA, Cole JR Jr (1999) Effects of macrophage inhibitory factor-A3 (MIF-A3) on cytokine secretion and phagolysosome fusion in murine macrophages. Vet Microbiol 65:47–60
Kawakami M, Tsutsumi H, Kumakawa T, Abe H, Hirai M, Kurosawa S, Mori M, Fukushima M (1990) Levels of serum granulocyte colony-stimulating factor in patients with infections. Blood 76:1962–1964
Kim KS (2008) Mechanisms of microbial traversal of the blood-brain barrier. Nat Rev Microbiol 6:625–634
Kragsbjerg P, Holmberg H, Vikerfors T (1996) Dynamics of blood cytokine concentrations in patients with bacteremic infections. Scand J Infect Dis 28:391–398
Makino M, Maeda Y, Fukutomi Y, Mukai T (2007) Contribution of GM-CSF on the enhancement of the T cell-stimulating activity of macrophages. Microbes Infect 9:70–77
Marshall JC, Malam Z, Jia S (2007) Modulating neutrophil apoptosis. Novartis Found Symp 280:53–66, discussion 67–72, 160–164
Martin MA, Pfaller MA, Wenzel RP (1989) Coagulase-negative staphylococcal bacteremia. Mortality and hospital stay. Ann Intern Med 110:9–16
Matsuda T, Saito H, Inoue T, Fukatsu K, Lin MT, Han I, Furukawa S, Ikeda S, Muto T (1999) Ratio of bacteria to polymorphonuclear neutrophils (PMNs) determines PMN fate. Shock 12:365–372
Melvan JN, Bagby GJ, Welsh DA, Nelson S, Zhang P (2010) Neonatal sepsis and neutrophil insufficiencies. Int Rev Immunol 29:315–348
Nienhaus GU, Wiedenmann J (2009) Structure, dynamics and optical properties of fluorescent proteins: perspectives for marker development. Chemphyschem 10:1369–1379
Omori F, Okamura S, Shimoda K, Otsuka T, Harada M, Niho Y (1992) Levels of human serum granulocyte colony-stimulating factor and granulocyte-macrophage colony-stimulating factor under pathological conditions. Biotherapy 4:147–153
Rothe G, Valet G (1988) Phagocytosis, intracellular pH, and cell volume in the multifunctional analysis of granulocytes by flow cytometry. Cytometry 9:316–324
Rothe G, Klingel S, Assfalg-Machleidt I, Machleidt W, Zirkelbach C, Banati RB, Mangel WF, Valet G (1992) Flow cytometric analysis of protease activities in vital cells. Biol Chem Hoppe Seyler 373:547–554
Santos JL, Montes MJ, Gutierrez F, Ruiz C (1995) Evaluation of phagocytic capacity with a modified flow cytometry technique. Immunol Lett 45:1–4
Seely AJ, Pascual JL, Christou NV (2003) Science review: cell membrane expression (connectivity) regulates neutrophil delivery, function and clearance. Crit Care 7:291–307
Smith J (1994) Neutrophils, host defense, and inflammation: a double-edged sword. J Leuko Biol 56:672–686
Tanaka H, Ishikawa K, Nishino M, Shimazu T, Yoshioka T (1996) Changes in granulocyte colony-stimulating factor concentration in patients with trauma and sepsis. J Trauma 40:718–726
Vincent JL, de Mendonca A, Cantraine F, Moreno R, Takala J, Suter PM, Sprung CL, Colardyn F, Blecher S (1998) Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit Care Med 26:1793–1800
Weiss M, Moldawer LL, Schneider EM (1999) Granulocyte colony-stimulating factor to prevent the progression of systemic non-responsiveness in SIRS and sepsis. Blood 93:425–439
Weiss M, Elsharkawi M, Welt K, Schneider EM (2003) Transient leukocytosis, granulocyte colony-stimulating factor plasma concentrations, and apoptosis determined by binding of annexin V by peripheral leukocytes in patients with severe sepsis. Ann N Y Acad Sci 1010:742–747
White JG, Amos WB, Fordham M (1987) An evaluation of confocal versus conventional imaging of biological structures by fluorescence light microscopy. J Cell Biol 105:41–48
Wiedenmann J, Nienhaus GU (2006) Live-cell imaging with EosFP and other photoactivatable marker proteins of the GFP family. Expert Rev Proteomics 3:361–374
Wiedenmann J, Ivanchenko S, Oswald F, Schmitt F, Rocker C, Salih A, Spindler KD, Nienhaus GU (2004) EosFP, a fluorescent marker protein with UV-inducible green-to-red fluorescence conversion. Proc Natl Acad Sci U S A 101:15905–15910
Woehrle T, Du W, Goetz A, Hsu HY, Joos TO, Weiss M, Bauer U, Brueckner UB, Schneider EM (2008) Pathogen specific cytokine release reveals an effect of TLR2 Arg753Gln during Candida sepsis in humans. Cytokine 41:322–329
Acknowledgements
We thank Joerg Wiedenmann for preparing Eos-FP E. coli. This work was in part supported by the Histiocytosis Association of America.
Competing interests statement
No competing interests to be disclosed by any of the authors. LS performed the experiments as a part of his doctoral thesis in medicine, MH-L and MW contributed patients and wrote the ms. HH performed assays and assay analysis. EMS designed the study, developed the assay, performed the analysis and wrote the ms.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Figure 1
Strategy to gate granulocytes in whole blood samples by scatter analysis. The specificity of gating leukocyte subpopulations in whole blood by scatter analysis (A) has been proven by the distinct expression of the leukocyte common antigen CD45 as well as CD14 (B) using FITC and phycoerythrin- (PE-) labeled monoclonal antibodies. CD45 density is characteristically lower on granulocytes as compared to eosinophiles and monocytes. In selected experiments performed with sepsis patients, the granulocytes’ expression of the following myloid differentiation antigens has been performed: CD11b (integrin), CD16 (FcR typeII), CD64 (FcRtypeI), CD62L, CD33 (myeloid antigen) as well as HLA-DR. Lymphocytes were identified by CD2 and CD19 (as described previously, (Woehrle et al. 2008)). (PPT 265 kb)
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Schreiner, L., Huber-Lang, M., Weiss, M.E. et al. Phagocytosis and digestion of pH-sensitive fluorescent dye (Eos-FP) transfected E. coli in whole blood assays from patients with severe sepsis and septic shock. J. Cell Commun. Signal. 5, 135–144 (2011). https://doi.org/10.1007/s12079-010-0112-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12079-010-0112-0