
Abstract
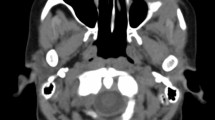
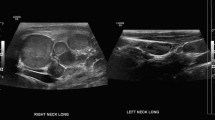
Rosai Dorfman disease or sinus histiocytosis is a rare, idiopathic, benign and self-limiting histiocytic proliferative disorder, usually seen in younger patients. It most commonly involves the cervical lymph nodes, with a predominant infiltration of sinusoidal histiocytes and classically presents with massive cervical lymhadenopathy. Extranodal disease occurs in about 43% of cases and produces different signs and symptoms depending upon its location. We report a case of this disorder in 22-year-old male with initial isolated involvement of bilateral nasal cavity and paranasal sinuses with subsequent involvement of cervical lymph nodes and skin. The clinical presentation, histologic characterstics, radiographic findings and treatment of the disease are discussed.
Similar content being viewed by others

References
Rosai J, Dorfman RF (1969) Sinus histiocytosis with massive lymphadepathy: a newly recognized benign clinicopathologic entity. Arch Pathol 87:63–70
Wenig BM, Abbondnzo SL, Childer EL et al (1993) Extranodal sinus histiocytosis with massive lymphadenopathy (Rosai Dorfman disease) of the head and neck. Hum Pathol 24:483–492
Annesi G, Gianneti A (1996) Purely cutaneous Rosai Dorfman disease. Br J Dermatol 134:749–753
Goodnight JW, Wang MB, Secarz JA et al (1996) Extranodal Rosai Dorfman disease of head neck. Laryngoscope 106: 253–256
Peter KKM, Michael TCF, Leung CY et al (1999) Nasal manifestation of extranodal Rosai-Dorfman disease-diagnosis and management. J. Laryngol Otol 113:275–280
Gregor RT, Ninnin D (1994) Rosai Dorfman disease of the paranasal sinuses. J Laryngol Otol 108:152–155
Foucar E, Rosai J, Dorfman RF (1979) The ophthalmologic manifestations of sinus histiocytosis with massive lymphadenopathy. Am J Ophthalmol 87:354–367
Foucar E, Rosai J, Dorfman RF (1978) Sinus histiocytosis with massive lymphadenopathy: Ear, nose and throat manifestations. Arch Otolaryngol Head Neck Surg 104: 687–693
Green I, Dorfman RF, Rosai J (1997) Breast involvement by extranodal Rosai-Dorfman disease: report of seven cases. Am. J. Surg Pathol 21:664–668
Resnick DK, John BL, Lovely TJ (1996) Rosai Dorfman disease presenting with multiple orbital and intracranial masses. Acta Neuropathologica 91:554–557
Paulli M, Rosso R, Kindl S, et al (1992) Immunophenotypic characterization of the cell infiltrate in five cases of sinus histiocytosis with massive lymphadenopathy (Rosai Dorfman disease). Hum Pathol 23:647–654
Sacchi S, Artusi T, Torelli U et al (1992) Sinus histiocytosis with massive lymphadenopathy. Leuk Lymphoma 23: 647–654
Wright DH, Richards DB (1981) Sinus histiocytosis with massive lymphadenopathy (Rosai Dorfman disease): Report of a case with widespread nodal and extranodal dissemination. Histopathology 5(6):697–709
Eisen RN, Backley PJ, Howard DJ (1990) Immunophenotypic characterization of sinus histiocytosis with massive lymphadenopathy(Rosai-Dorfman disease). Semin Diagn Pathol 7:74–82
McAlister WH, Herman T, Dehner LP (1990) Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease). Pediatr Radiol 20:425–432
Komp DM (1990) The treatment of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease). Semin Diagn Pathol 7:83–86
Jabali Y, Smrcka V, Pradna J (2005) Rosai-Dorfman disease: successful long-term results by combination chemotherapy with prednisone, 6-mercaptopurine, methotrexate, and vinblastine: a case report. Int J Surg Pathol 13:285–9
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Parida, P.K., Panda, N.K., sharma, A. et al. Varied manifestations of Rosai-Dorfman disease and its management — a case report and review of literature. Indian J Otolaryngol Head Neck S 60, 365–368 (2008). https://doi.org/10.1007/s12070-008-0117-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-008-0117-7
Key messages
- Our case demonstrated
- isolated involvement of nose and paranasal sinuses with subsequent involvement of lymph nodes and skin
- Most of the time
- the disease process undergoes spontaneous remission indicating that conservative
- expectant management is sufficient in most patients
- but more aggressive treatment may be necessary in selected cases