
Abstract
The aim of the study is to explore the association of obesity by body mass index (BMI) measurements with subjective health status (SHS), objective health status (OHS) and wellbeing status among older adults in England. The sample of 5640 participants (aged 50 years and over) are considered from the English Longitudinal Study of Ageing Wave 8 dataset. Multivariate logistic regression analysis is performed to explore the cross-sectional relationship of the study variables. The statistical analyses explored those overweight and obese older adults are progressively vulnerable to increasing odds of poor SHS, OHS and poor wellbeing in an adjusted model compared to their normal-weight counterparts. The outcome of the present study would enable policymakers and healthcare providers to have greater insight into the effects of socio-demographic and lifestyle factors and the effect of high BMI on older adults’ health and wellbeing.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obesity is a worldwide problem and is one of the biggest public health challenges today with increasing prevalence and incidence in both developed and developing countries (Bell et al., 2016). Compared to the rest of Europe, England has some of the worst figures. A report by the Department of Health and Social Care (UK Government, 2020) states that currently, in England, approximately 63% of adults have a high Body Mass Index (BMI) and half of them are obese. Since 2007, the adult obesity trend has accelerated faster than predicted (UK Government, 2020). It is estimated that by 2024, the number of obese adults in England will be between 26.6% and 33.9% (Public Health England, 2019).
Increasing life expectancy and obesity among older adults jointly lead to disability and dependencies. Moreover, ageing itself is a contributor to poor metabolic health, a decline in immune system function, reduction of lean body mass, alterations in body fat distribution and an increase in abdominal obesity (Jura & Kozak, 2016). For older women, abdominal obesity is more prevalent and nearly double the rate of general obesity, amounting to 73.8% of women aged 60 years and over (Lumsden & Hor, 2015). There is evidence that older adults’ subjective health appraisal may depend on various factors other than objective health (e.g., clinically diagnosed). A study on self-rated health vs objective health status (OHS) of elderly people (Araújo et al., 2018) revealed that 46.5% of participants marked their health as good, very good, or excellent despite their functional impairment. Djalalinia et al. (2015) have argued that there is a need to evaluate the influence that obesity has on various dimensions of health (for example, physical health and illness, mental health and wellbeing), particularly for older adults. Therefore, self-rated health appraisal, which reflects an individual’s physical and mental health is an important area of research and is used to measure an individual’s subjective health status (SHS) in many population surveys.
Furthermore, several studies found that a higher level of wellbeing is influential for older adults in reducing the risk of injury, disease, illness, and increased longevity, better immune functioning, and speedier recovery (Centres for Disease Control and Prevention, 2018). However, the ‘Obesity Care Pathway Toolkit’, developed by the National Obesity Forum (2005), 'Care pathway for the management of overweight and obesity’ by the National Health Service (NHS) (2006), National Institute for Health and Care Excellence (NICE) guidance on obesity (2014), 'Wandsworth Healthy Weight Care Pathway Toolkit' by Public Health Wandsworth Council (2018) and The 'Report of the working group into: Joined-up clinical pathways for obesity’ by a joint working group with representation from various health regulatory bodies of England (NHS England, 2014); sub-optimally addresses the areas under the care pathway for overweight and obese older adults for all aspects of their wellbeing related to their current health status to improve their quality-of-life. It is, therefore, essential to explore the association between current health status and wellbeing among older adults with obesity. In consideration of this, the current research poses the following question:
Is there any association between obesity with current health status and the wellbeing of older adults in England?
Background
In the United Kingdom, the prevalence of obesity is more visible among older adults, with approximately three-quarters of older adults aged between 65–74 years being classified as overweight or obese (Gulland, 2010). Some past studies have reported that high BMI may have a protective role in premature mortality in older adults (Janssen, 2007; Pischon et al., 2008). For example, a study on older adults by Han et al. (2011) found that high BMI, increased the absolute mortality risk up to the age of 75 years, with the association becoming weaker for older adults over 80 years of age. This phenomenon has been termed the 'obesity paradox' or ‘reverse epidemiology’ (Chapman, 2010; Hainer & Aldhoon-Hainerova, 2013). However, it is important to note that the idea of the obesity paradox does not consider the older adults’ health and wellbeing status concerning their BMI.
The evidence also shows that increased abdominal fat is linked to an increased risk of cardiovascular disease and type 2 diabetes (Lumsden & Hor, 2015). Therefore, obesity in older adults is an increasingly important public health concern as it is an increasing and major source of mortality, morbidity, and disability for the past 3–4 decades (Abdelaal et al, 2017). Systematic reviews and meta-analyses by Ofori-Asenso et al. (2019) aimed at the older adults (aged ≥ 65 years) in high-income countries explored that 2 in 5 and 1 in 8 older adults had ≥ 3 and ≥ 5 chronic medical conditions, respectively. There has also been an epidemiological transition, in most countries, as national disease burdens move to a greater or equal predominance of non-communicable diseases compared to communicable diseases (Arokiasamy & Selvamani, 2018). Older adults are therefore more prone to develop multiple chronic diseases, frequently described as 'multimorbidity', due to the biology of ageing and the shifting disease burden profile (Arokiasamy et al., 2015). An increase in longevity and obesity leads to an increase in chronic conditions, complex morbidities with more than two diseases, disability, and premature mortality in older adults, particularly in developed countries (Gallagher & Gates, 2006; Nam et al., 2012). A report by Office for National Statistics (ONS, 2013) stated that in Great Britain (England, Scotland, and Wales), 36% and 20% of adults reported having long-term conditions or disabilities or a limiting long-term condition or disability, that is more than one in three and one in five adults, respectively. It had also been found that people with chronic conditions, complex morbidities and impaired mobility who are also obese have lower wellbeing (Local Government Association, 2020). However, some studies explored that being overweight possibly be a protective factor concerning chronic diseases (Coqueiro et al., 2013; Pes et al., 2019), but the effect appears to be weakening for the elderly (Dixon et al., 2015).
On the other hand, a Taiwan study by Chang et al. (2018) argued that overweight older adults had significantly better self-rated health scores and obese older adults had significantly better self-rated happiness scores than the normal-weight population. But there are studies that also established those obese older adults experience significant impairments in quality of life (QOL) because of their obesity, with a higher level of obesity-associated with greater impairments in QOL (Daviglus et al., 2003; Sach et al., 2006). However, that is not always true in terms of emotional wellbeing, especially in individuals who are obese without any chronic conditions (Doll et al., 2000). A longitudinal study by Shankar et al. (2014) evaluated that hedonic wellbeing (greater enjoyment in life) could be associated with an individual's poor health, and Steptoe et al. (2015) found that hedonic wellbeing could be declined progressively with the number of comorbidities. Approximately 79% of NHS admissions for obesity-related bariatric surgery for the age group of 35 and 64 years (NHS Digital, 2019) reflect the mental health status of these individuals. Amarya et al. (2014) argue that quality of life or wellbeing may be the most important goal of therapy in older adults. Several studies explored that SHS of older adults is not solely dependent on ageing or age-related health status and functional difficulty, and there is an existing discrepancy between subjective and objective indicators of health among older adults (Araújo et al., 2018; Cho et al., 2012).
However, there is a lack of published studies that could capture the effects of BMI on SHS, OHS and wellbeing of obese older adults compared to normal-weight older adults. In this study, we have examined the cross-sectional association between above-normal BMI in older adults aged 50 years and above and the perceived differences in their SHS, OHS and wellbeing.
Methods
Sample and Participants
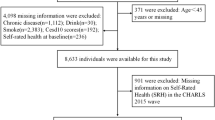
The English Longitudinal Study of Ageing (ELSA) is a panel survey of a representative cohort of English women and men aged fifty years and over living within the community (Institute for Fiscal Studies, 2018). It’s a distinctively made supply of knowledge on the health, social circumstances, wellbeing, and economic conditions of its participants. Details concerning the method and technical aspects of the survey and its methodology are revealed elsewhere (Bowling & Windsor, 2008; Pongiglione et al., 2017). This study has used the ELSA Wave eight survey dataset. The Wave eight survey was meted out between May 2016 and June 2017. It had a sample size of 8,445 participants. For this study, underweight respondents (BMI < 18.5 kg/m2) were removed from the analytic dataset to avoid selection bias. This is because several studies have found that physical or mental impairments, disabilities and morbidity can be causal health effects of poor nutrition among older adults (Sawada et al., 2021; Wei et al., 2018). Therefore, the present study only considered 5,640 participants.
All ELSA participants provided written and informed consent and all the ELSA waves have been approved by the National Research and Ethics Committee (London Multicentre Research Ethics Committee (MREC/01/2/91)). The ELSA participants are anonymised, and the anonymised data are freely accessible from the UK Data Service (UK Data Service, 2018).
Data Collection
Three methods of data collection were used for ELSA Wave 8: face-to-face interviews were conducted using computer-assisted personal interviewing (CAPI), self-completion questionnaires completed using pen and paper (PAPI) and an observation and examination visit by a nurse. Face-to-face interviews were undertaken by trained interviewers using laptop computers at the participant’s residential address to collect baseline demographic and physical and mental health status information for each participant (Slater et al., 2018).
Nurse home visits in Wave 8 involved collecting data for anthropometric measures and physical performance measures along with bio-measurements. However, in wave 8, the participant’s height was not measured, as part of the anthropometric measurements. Therefore, Wave 6 participant’s height data has been merged with the Wave 8 dataset to calculate the participant’s BMI. This was because the Wave 8 cohort group were the same as the Wave 6 cohort group.
Variables and Measurements
Subjective Health Status
To determine participant’s SHS, self-rated single item health was evaluated with a single question (“In general, would you say your health is…”) and asking the respondents to mark their health on a 5-point Likert scale, where positively structured responses were reversely scored (0–4) from excellent, very good, good, fair, and poor. However, for regression analysis in the present study, the above mentioned self-rated health status (SHS) has been dichotomised as 0–1 (fair/poor and excellent/very good/good respectively).
Objective Health Status
To determine OHS, 11 medically diagnosed morbidities are considered to be relevant from the literature (Araújo et al., 2018; Jehan et al., 2017). The previous studies (Barnett et al., 2012; Salisbury, 2013) suggest that a single disease approach is failed to evaluate the complexity of the problem correctly. Moreover, there is no international consensus on a list of chronic conditions for older adults to be used in research and surveillance (Li et al., 2016). These are high blood pressure, high cholesterol, angina, heart attack, stroke, other heart diseases, diabetes, cancer, dementia, arthritis, and osteoporosis. However, there are a few more diagnosed diseases in the ELSA dataset, but the number of respondents is very low for those to be included in the analysis. The definition of 'comorbidity' and 'multimorbidity' was adapted from past studies (Fortin et al., 2012; Pes et al., 2019). The former is defined as the co-occurrence of two clinically diagnosed disease conditions, and the latter is the co-occurrence of three or more clinically diagnosed disease conditions along with the primary disease or index disease. However, different researchers have defined comorbidity and multimorbidity in many ways, according to their study purpose. In the present study, the primary or index condition is a high level of BMI above what is defined as normal weight for a participant, and the aim is to explore the connection between excess weight with other clinically diagnosed conditions. A four-point scale was used to measure morbidities, where “no morbidity” was coded as 0, 1 for “single morbidity”, 2 for “comorbidity”, and 3 for “multimorbidity”.
Wellbeing
Wellbeing was measured as hedonic or psychological wellbeing. To evaluate the effect of positive weight gain on psychological wellbeing, a strongly validated scale that is Control autonomy self-realisation pleasure scale (CASP) has been used. The 19-items CASP-19 measuring instrument was included as part of the self-completion document. Participants were asked how frequently each of the statements (all the statements are jotted down in Table 1) in CASP-19 was applied to them on a 4-point Likert scale ranging from 0–3, where 0 represents often and 3 represents never. The statements are mostly negatively worded. Therefore, few positively worded statements coding has been changed to match with the rest of the statements coding, where 0 represents good quality of life and 3 represents poor quality of life. All the responses have been summed up to have a total score (range 0–57), with higher scores reflecting poor wellbeing.
Body Mass Index
To calculate BMI participants’ height was measured to the nearest millimetre by a portable stadiometer, asking them to stand upright without shoes. Weight was measured by using a portable electronic scale to the closest 0.1 kg. However, the portable electronic scale has a limit to weigh up to 130 kg, therefore, those participants’ weights were estimated. Participants were requested to take their shoes off and to wear only light clothing. Each informant’s BMI was calculated as weight in kilograms divided by height in meters squared. Participants’ weight was categorised according to the World Health Organisation (WHO) classification into three groups- normal (BMI ≥ 18.5 to < 25), overweight (BMI ≥ 25 to < 30) and obese (BMI ≥ 30). The BMI variable is coded progressively as 1 for “normal”, 2 for “overweight” and 3 for “obese”.
Selected Covariates
The socio-demographic factors used are age, gender, marital status, education, and the socio-economic factor used is employment status. The behavioural or lifestyle factors used are the amount of smoking and drinking alcohol. Several past studies on older adults have found good agreement when using the variables mentioned above as the risk factors for health, wellbeing, and social care outcomes (Jackson et al., 2019; Pongiglione et al., 2017). Ethnicity is not considered as one of the covariates for this study, as the study sample was not a representative sample of non-white respondents. The number of ‘white’ participants was 6,746 (94.6%) whereas the number of non-white respondents was 387 (5.4%). Age variable has been progressively valued as, 0 for 50–60, 1 for 61–70, 2 for 71–80 and 3 for 81 + years of the age cohort. Please see other coding and measurements in Table 1.
Data Analysis
A descriptive statistical analysis is initially performed with the help of the SPSS V.25.0 software package summarising the impact of obesity on SHS and OHS of older adults. The data are subsequently stratified according to respondents’ demographics. To conclude the hypothesis with 95% confidence, the generated p-value of the χ2 statistics should be less than 0.05 (p < 0.05) to be considered statistically significant.
Multivariate models are used to predict whether an increased level than normal BMI is associated with older adults’ SHS, OHS and wellbeing. Unadjusted and adjusted ORs with corresponding 95% CI are calculated to determine the participant’s SHS and wellbeing. Multinomial logistic regression is applied to predict the connection between obesity and the three categories of OHS measures with no morbidity as a reference group.
Results
Participant Characteristics
All selected characteristics of the participants are presented in Table 1. The mean age of the respondents was 68 years, out of which 32.7% of the participants were obese. Compared to the normal-weight participants, there were 9.8% and 0.5% more obese and overweight participants, respectively, in the working dataset. The study population comprised more females than males (50.5% vs 49.5%), with most of them being married (65.4%), having at least one co-resident (76%), and currently not smoking (53.4%) and retired or unemployed (68.5%). About half of the participants (49.7%) consumed alcohol frequently or daily. Out of 5640 participants, only 1111 (19.7%) participants were either continuing their education during data collection or leaving their formal education at 19-year age or over. About three quarter (73.1%) of participants left their formal education between 15–18-year of age. Most older adults marked their subjective health status (SHS) as good (32.1%) and very good (29%) than poor (8.5%). However, 18.9% of participants marked their health status fair than excellent (11.5%). In the Wave 8 ELSA dataset more participants had single morbidity (30.7%), and very few participants reported having no morbidity (1.5%). More participants reported having comorbidities than multimorbidity (22.3% vs 16%).
Results from the Chi-square (χ2) statistical analysis (Table 2 and Table 3) reveals that high BMI is statistically significant with an individual's SHS and OHS (χ2 (2) = 82.73, p < 0.05; and χ2 (2) = 26.89, p < 0.05, respectively). Except for an individual's gender and smoking status, all other socio-demographic, behavioural and socio-economic covariates are strongly associated (p < 0.01) with respondents’ both SHS and OHS. Although participant’s sex is not significantly associated with their SHS (χ2 (1) = 4.46, p > 0.05), however, strongly associated with their OHS (χ2 (1) = 15.23, p < 0.05). In contrast, an individual's smoking status is strongly associated with their SHS (χ2 (1) = 60.11, p < 0.05), but not strongly connected with their OHS (χ2 (1) = 3.19, p > 0.05).
Examining the Differences in SHS Risk Between the BMIs Groups
The unadjusted binary logistical regression analysis (Table 4) shows the independent effect of BMI, that compared to normal-weight individuals, the chance of having better SHS is strongly reduced for obese participants by 27% (OR: 0.73, 95% CI: 0.63–0.84, p < 0.01). However, the effect is found to be insignificant for overweight participants and the odds of having good SHS were reduced by 12% for them (OR: 0.88, 95% CI: 0.75–1.03, p > 0.05).
The adjusted model (Table 4) shows that compared to normal-weight individuals, the chance of having better SHS is significantly reduced for both their obese and overweight counterparts by 36% and 27%, respectively (OR: 0.64, 95% CI: 0.52–0.80, p < 0.01; OR: 0.73, 95% CI: 0.58–0.91, p < 0.05, respectively) while the other variables are held constant. On the other hand, compared to the 50–60-year age group, increasing age significantly increased the chance of having better SHS by 65%, 53% and 45% for those of their 61–70's, 71–80's and 81 + years, respectively. Compared to females, the odds of having better SHS are insignificantly reduced by 13% for those males and compared to retired or unemployed individuals, the odds of having better SHS are significantly increased by 256% for those in employment. Moreover, compared to the married and non-smokers respondents, being unmarried/single/divorced/widowed and current smokers strongly reduced the odds of having better SHS of 29% and 52%, respectively. At the same time, compared to the none or rare alcohol drinkers, the odds of having better SHS significantly increased by 80% for their frequent or daily drinker counterparts. Finally, compared to the individuals with no education or minimum education (/ ≤ 14 years), having the highest education (≥ 19 years/ not yet finished) and finishing education between 15–18 years significantly increased the odds of having better SHS by 301% and 95%, respectively.
Examining the Differences in OHS Risk Between the BMIs Groups
Table 5 evaluates that compared to normal-weight individuals, the risk of having single morbidity, comorbidity and multimorbidity than no morbidity is significantly increased for obese participants by 165%, 304% and 342%, respectively when the model is controlled for other variables. At the same time, although the risk of having single morbidity and comorbidity is not significant for overweight, strongly increased the hazard of having multimorbidity at a 5% level. Surprisingly, compared to the 50–60-year age group, increasing age reduced the risk of having single morbidity than having no morbidity by 39%, 44% and 16% for those their 61–70's, 71–80's and 81 + years, respectively. However, compared to the 50–60-year age group, the risk of comorbidity than no morbidity increased for the oldest old (aged 81 + years) by 10%. Although the hazard of having comorbidity reduced for those of 61–70's and 71–80 years by 43% and 36%, respectively to their 50–60 years counterparts, as well as the effects of age, are insignificant in predicting comorbidity when the model is controlled for BMI and other variables. Nevertheless, compared to the 50–60-year age group, the hazard of multimorbidity than no morbidity increased with age by 115%, 220% and 414% for individuals of 61–70, 71–80 and 81 + year age groups, respectively. The oldest-old strongly predicts the risk of multimorbidity at a 5% level, but other age groups are insignificant. On the other hand, compared to females, married, and being retired or unemployed, the odds of having single morbidity, comorbidity and multimorbidity than having no morbidity were reduced for those of males, unmarried/single/divorced/widowed and in employment, respectively. Where an individual's gender and employment status significantly predict the risk of comorbidity and multimorbidity, but marital status is insignificant at a 5% level. Nevertheless, compared to the current non-smokers the hazard of having single morbidity, comorbidity and multimorbidity than no morbidity is significantly increased by 548%, 475% and 602%, respectively for their current smokers’ counterparts. However, although compared to the none or rare alcohol drinkers the hazard of having single morbidity and comorbidity insignificantly increased by 28% and 1% respectively, the odds of having multimorbidity than having no morbidity is reduced by 8% for frequently or daily alcohol drinkers. Furthermore, compared to the individuals with no education or minimum education (never/ ≤ 14 years), those with higher education insignificantly reduced the risk of single morbidity, comorbidity and multimorbidity for both finishing education between 15–18 years and having the highest education (≥ 19 years/ not yet finished).
Examining the Differences in Wellbeing Between the BMIs Groups
Table 6 shows that an individual's poor wellbeing increases with an individual's increasing degree of BMI, irrespectively the model is controlled for other predictors or not. Compared to the normal weight individuals, on average every 1 kg/m2 increase in BMI for overweight and obese participants, we expect an increased risk of poor wellbeing of 0.22 units and 0.98 units respectively (B: 0.22, 95% CI: -0.7328 to 1.18, p > 0.05, and B: 0.98, 95% CI: 0.08 to 1.89, p < 0.05, respectively), when the model is adjusted for BMI and other variables. The risk of having poor wellbeing is significantly higher for an obese individual, but the risk is insignificant for overweight individuals. Paradoxically, increasing age strongly reduced the risk of having poor wellbeing. Compared to the 50–60-year age group, every 1-year increase of age in average for the participants of 61–70 and 71–80-year age groups, we expect a reduced risk of poor wellbeing of 3.76 units and 3.93 units, respectively, while the other variables are held constant. The average risk of poor wellbeing was significantly lower by 3.26 units for the oldest old (aged 81 + years) adults (B: -3.26, 95% CI: -4.81 to -1.72, p < 0.01). In addition, compared to females, males insignificantly reduced the average risk of poor wellbeing by 0.07 units and compared to married individuals and non-smokers, the hazard of poor wellbeing is significantly higher by 1.51 units and 1.28 units for those who are unmarried/single/divorced/widowed and current smokers, respectively. Moreover, compared to never or rare alcohol drinkers and retired or unemployed participants, the average risk of poor wellbeing is strongly reduced by 1.00 units and 1.30 units for their frequent or daily drinkers and employed counterparts, respectively. Nevertheless, being highly educated insignificantly increased the risk of an individual's poor wellbeing compared to individuals with no education or minimum education (never/≤ 14 years). Furthermore, individuals with excellent/very good/good SHS significantly reduced the hazard of poor wellbeing by 7.73 units compared to those who reported their SHS as fair or poor. At the same time, it is not surprising that the hazard of poor wellbeing is insignificantly higher by 0.15 units and 0.63 units for individuals with comorbidity and multimorbidity, respectively.
Discussion
The statistical analyses explored those older adults (aged 50 years and over) who were overweight and obese were progressively vulnerable to increasing odds of poor subjective and objective health status and poor wellbeing in an adjusted model compared to their normal-weight counterparts. In addition, obesity by BMI classification strongly predicted the participant’s SHS, complex morbidities and poor wellbeing. On the other hand, compared to the 50–60 years age group, increasing age increased the odds of multimorbidity and only for the oldest old, increased the odds of comorbidity, whereas increasing age reduced the odds of single morbidity in an adjusted model. Surprisingly, increasing age reduced the odds of poor SHS and poor wellbeing among older adults. In addition, participants who were female, unmarried/single/widowed/divorced, low level of education, retired/unemployed and current smokers were progressively vulnerable to increased odds of complex morbidities. Whereas participants who were male, unmarried/single/widowed/divorced, low level of education, were retired/unemployed and current smokers were progressively vulnerable to increasing odds of poor SHS and poor wellbeing. Moreover, although the increasing frequency of alcohol increased the odds of single morbidity and comorbidity, it reduced the odds of multimorbidity, poor SHS and poor wellbeing among older adults. Finally, although older adults’ good SHS significantly reduced the odds of poor wellbeing, the effect of objective health status (except single morbidity) concerning comorbidity and multimorbidity; however, were insignificant.
The findings from the exploratory data analysis (Table 2 and Table 3) are consistent with previous studies, see for example- López-García et al., 2003; Giuli et al., 2014, where the percentage of SHS rating as fair/poor are significantly higher for obese older adults than that of their overweight and normal-weight counterparts. The findings can be explained by the fact that, for obese older adults, lack of physical activities leads to depression and social isolation or discrimination, resulting in poor self-esteem and body image distortions (Abdelaal et al., 2017; Trull et al., 2012). In addition, it is noted that about one quarter (22.7%) of respondents have multimorbidity. The findings are in line with other UK estimates of multimorbidity that ranged from 23% (Barnett et al., 2012) to 58% (Macleod et al., 2004).
The outcomes displayed in Table 4 are in line with an English Longitudinal Study conducted by Hulman et al. (2019) that finds high risk of poor SHS is associated with the advancement of BMI in old age. However, the study evaluates that poor SHS for the older participants (aged ≤ 60 years < 75 years) is related to only the development of BMI, whereas, for the elderly (aged ≥75 years), it is due to the decline of BMI. Another cross-sectional study by Araújo et al. (2018) revealed that most of the oldest-old participants with severe to moderate dependence had a reasonable to excellent SHS. This can be explained by survival bias theory, as obese individuals are at greater risk of dying early. Therefore, only selectively healthy individuals could survive into old age (Kuk et al., 2009; Ng et al., 2017).
Table 5 shows that obesity among older adults is significantly associated with single morbidity, comorbidity and multimorbidity, while the model is adjusted for other lifestyle and socio-demographic factors. The outcome is consistent with several past studies (Dhalwani et al., 2016; Li et al., 2016). Dhalwani et al. (2016) that found although obesity is not significantly associated with multimorbidity independently, the overall risk of multimorbidity is increased more with the combined presence of certain unhealthy lifestyle factors than the quantity, which is in line with the present study. A cross-sectional US study by Pantalone et al. (2017) explored that high BMI is associated with a high prevalence of comorbidity, although, the study participants were ≥ 20 years old. Another single-centre study by Pes et al. (2019) found that moderately overweight with a BMI range of 27.5–29.9 kg/m2 can be a protective factor for particularly older males concerning comorbidity, whereas the present study evaluated that the risk of having single morbidity and comorbidity for overweight older adults is insignificant. Besides, the findings are supported by Booth et al. (2014) that found the prevalence of multimorbidity significantly increased with age in each overweight and obese category by BMI classification. The findings are also consistent with a past longitudinal English population study by Singer et al. (2019) that found increasing age increased the probability of having multimorbidity. Nevertheless, in older adults, the relation between BMI and chronic diseases is complex, and the effect of BMI seems attenuated, which can be explained by the ‘obesity paradox’ (Dixon et al., 2015; Leal Neto et al., 2016) and perhaps a few combinations of medically diagnosed diseases are more hazardous than others (Hernández et al., 2019).
On the other hand, the findings that evaluated participants who are male reduced the risk of multimorbidity than females are in line with a prospective English population study by Dhalwani et al. (2016). A study on older Irish adults by Hernández et al. (2019) explored the gender variations according to the prevalence of various clusters of comorbid conditions and found females had a high probability of suffering from osteoporosis, and arthritis. The study also found that obesity and arthritis were the highest prevalence of comorbidity in the male participants. However, the study evaluated those female cohorts might have a more complex set of highly occurring coexisting conditions than males. The outcome regarding the association of OHS with smoking and alcohol drinking is agreed by a recent longitudinal study (Singer et al., 2019) that found the odds of having multimorbidity reduced by the increasing frequency of alcohol consumption. Another study by Dhalwani et al. (2016) did not find a significant association between the risk of multimorbidity and frequent alcohol consumption among the older English population. However, the study evaluated that obesity and smoking, if combined with excess alcohol consumption, lack of physical activity, and inadequate fruit/vegetable intake, could have the strongest association with multimorbidity incidence. The study found that few combinations of lifestyle factors could be more hazardous than others in the increasing risk of multimorbidity.
On the other hand, the result that is displayed in Table 6 is in line with a cross-sectional US study that used primary data and evaluated those overweight and obese patients who had a substantially lower health-related quality of life, and the effect was reduced when combined with age, sex, smoking and comorbidity (Katz et al., 2000). However, the paradoxical outcome between increasing age for an older adult and reduced risk of poor wellbeing is in line with an English study by Deaton (2008), using data from a proceeding survey of over 160 countries that explored the U-shaped association between age and wellbeing, where 45–54 years age group had the worst wellbeing. Although, they did not explore the combined effect of obesity and other lifestyle factors on individuals' increasing age and wellbeing.
There are a few limitations of our study. Firstly, height was not measured in the same data collection wave as weight, other lifestyle, health, and social care factors, hence it could introduce measurement bias, as participants may have changed their height status since older adult's height can reduce due to age-associated spinal shortening (Han et al., 2011). several past studies have found good agreement on health outcomes using height coefficients from the ELSA dataset as height is measured in every alternative Wave in ELSA (Copley et al., 2017; Jackson et al., 2015). Secondly, although BMI is a well-known measure of obesity, there is evidence that the measure of central obesity may be more important in determining health outcomes (Zaninotto et al., 2010). Moreover, different studies use different cut-points of BMI to determine obesity. Thirdly, ELSA used self-reported medical diagnosis of chronic disease and participants with cognitive impairment had to have a proxy interview. However, for objective assessment of medically diagnosed diseases, the participants had to be engaged with the health care system and that could have resulted in under-reporting, particularly for the participants, who were not eligible to have free medical care (Hernández et al., 2019). Moreover, no measures were put on whether discrepancies between wellbeing and subjective and objective indicators of health among older adults and how these may be culturally influenced because the ELSA survey data is an English population survey only. Finally, the cross-sectional study is per se a limitation. This study design does not explore a deeper understanding of patients’ experiences living with physical health conditions over the period. As a result, causation could not be inferred.
However, the strength of the study is using a large English prospective cohort data set and therefore, our findings are generalisable to the English population. Moreover, ELSA used standardised data collection methods and all data collection tools are validated, for example, the CASP-19 scale.
Conclusion
The outcome of the present study would enable policymakers and healthcare providers to have greater insight into the effects of socio-demographic and lifestyle factors and the effect of high BMI on older adults’ health and wellbeing. Further research is required to investigate the severity of chronic conditions in overweight and obese older adults’ and identify the combination of chronic diseases that are more hazardous.
References
Abdelaal, M., le Roux, C. W., & Docherty, N. G. (2017). Morbidity and mortality associated with obesity. Annals of translational medicine, 5(7), 161. https://doi.org/10.21037/atm.2017.03.107
Amarya, S., Singh, K., & Sabharwal, M. (2014). ‘Health consequences of obesity in the elderly’, Journal of Clinical Gerontology and Geriatrics, 5(3), p. 63–67. Available at: https://www.sciencedirect.com/science/article/pii/S2210833514000070 (Accessed: 29 April 2018).
Araújo, L., Teixeira, L., Ribeiro, O., & Paúl, C. (2018). Objective vs Subjective Health in Very Advanced Ages: Looking for Discordance in Centenarians. Frontiers in Medicine, 5, 189. https://doi.org/10.3389/fmed.2018.00189
Arokiasamy, P., & Selvamani, Y. (2018). Age, socio-economic patterns and regional variations in grip strength among older adults (50+) in India: Evidence from WHO’s Study on Global Ageing and Adult Health. Archives of Gerontology and Geriatrics, 76, 100–105. https://doi.org/10.1016/j.archger.2018.02.007
Arokiasamy, P., Uttamacharya., & Jain, K. (2015). ‘Multi-morbidity, functional limitations, and self-rated health among older adults in India: cross-sectional analysis of LASI pilot survey, 2010’. Sage Open, 5(1). https://doi.org/10.1177/2158244015571640.
Barnett, K., Mercer, S. W., Norbury, M., Watt, G., Wyke, S., & Guthrie, B. (2012). Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. The Lancet, 380(9836), 37–43. https://doi.org/10.1016/S0140-6736(12)60240-2
Bell, S. P., Patel, N., Patel, N., Sonani, R., et al. (2016). Care of Older Adults. Journal of Geriatric Cardiology, 13(1), 1–7. https://doi.org/10.11909/j.issn.1671-5411.2016.01.019
Booth, H. P., Prevost, A. T., & Gulliford, M. C. (2014). Impact of body mass index on prevalence of multimorbidity in primary care: Cohort study. Family Practice, 31(1), 38–43. https://doi.org/10.1093/fampra/cmt061
Bowling, A., & Windsor, J. (2008). The effects of question order and response-choice on self-rated health status in the English Longitudinal Study of Ageing (ELSA). Journal of Epidemiology & Community Health, 62(1), 81–85. https://doi.org/10.1136/jech.2006.058214
Centres for Disease Control and Prevention (CDC) (2018). Health-Related Quality-of-life (HRQOL): Well-being concepts. Available at: https://www.cdc.gov/hrqol/wellbeing.htm (Accessed 29 February 2019).
Chang, H. T., Hsu, N. W., Chen, H. C., Tsao, H. M., Lo, S. S., & Chou, P. (2018). Associations between Body Mass Index and Subjective Health Outcomes among Older Adults: Findings from the Yilan Study, Taiwan. International Journal of Environmental Research and Public Health, 15(12), 2645. https://doi.org/10.3390/ijerph15122645
Chapman, I. M. (2010). Obesity paradox during aging. Interdisciplinary Topics in Gerontology, 37, 20–36. https://doi.org/10.1159/000319992
Cho, J., Martin, P., & Poon, L. W. (2012). The Older They Are, the Less Successful They Become? Findings from the Georgia Centenarian Study. Journal of Aging Research, 2012, 1–8. https://doi.org/10.1155/2012/695854
Copley, V.R., Cavill, N., Wolstenholme, J., Fordham, R., & Rutter, H. (2017). ‘Estimating the variation in need for community-based social care by body mass index in England and associated cost: population-based cross-sectional study’. BioMed Central Public Health, 17(1). https://doi.org/10.1186/s12889-017-4665-1.
Coqueiro, R.S., Santos, G.A.F., Borges, L.J., Sousa, T.F., Fernandes, M.H., & Barbosa, A.R. (2013). ‘Anthropometric indicators of obesity and hyperglycaemia in Brazilian older people.’ Journal of Diabetes Nursing, 17(9), pp. 351–355. Available at: https://www.diabetesonthenet.com/download/resource/. (Accessed: 12 July 2020).
Daviglus, M. L., Liu, K., Yan, L. L., Pirzada, A., Garside, D. B., Schiffer, L., Dyer, A. R., Greenland, P., & Stamler, J. (2003). Body Mass Index in Middle Age and Health-Related Quality of Life in Older Age. Archives of Internal Medicine, 163(20), 2448–2455. https://doi.org/10.1001/archinte.163.20.2448
Deaton, A. (2008). Income, health, and well-being around the world: Evidence from the Gallup World Poll. The Journal of Economic Perspectives: A Journal of the American Economic Association, 22(2), 53–72. https://doi.org/10.1257/jep.22.2.53
Dhalwani, N.N., Zaccardi, F., O’Donovan, G., Carter, P., Hamer, M., Yates, T., Davies, M., & Khunti, K. (2016). ‘Association Between Lifestyle Factors and the Incidence of Multimorbidity in an Older English Population.’ The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. glw146. https://doi.org/10.1093/gerona/glw146.
Dixon, J. B., Egger, G. J., Finkelstein, E. A., Kral, J. G., & Lambert, G. W. (2015). Obesity paradox’ misunderstands the biology of optimal weight throughout the life cycle. International Journal of Obesity (2005), 39(1), 82–84. https://doi.org/10.1038/ijo.2014.59
Djalalinia, S., Qorbani, M., Peykari, N., & Kelishadi, R. (2015). Health impacts of obesity. Pakistan Journal of Medical Sciences, 31(1), 239–242. https://doi.org/10.12669/pjms.311.7033
Doll, H. A., Petersen, S. E., & Stewart-Brown, S. L. (2000). ‘Obesity and physical and emotional wellbeing: Associations between body mass index, chronic illness, and the physical and mental components of the SF-36 questionnaire’. Obesity Research, 8(2), pp.160–170. Available at: https://www.ncbi.nlm.nih.gov/pubmed/10757202 (Accessed: 5 February 2019).
Fortin, M., Stewart, M., Poitras, M.-E., Almirall, J., & Maddocks, H. (2012). A Systematic Review of Prevalence Studies on Multimorbidity: Toward a More Uniform Methodology. The Annals of Family Medicine, 10(2), 142–151. https://doi.org/10.1370/afm.1337
Gallagher, C.S and Gates, J. (2006) ‘Obesity: changing the face of geriatric care’, Ostomy Wound Manage, 52 (10), pp. 36–38. Available at: https://www.ncbi.nlm.nih.gov/pubmed/17041253 (Accessed: 7 April 2018).
Giuli, C., Papa, R., Bevilacqua, R., Felici, E., Gagliardi, C., Marcellini, F., Boscaro, M., et al. (2014). Correlates of perceived health related quality of life in obese, overweight and normal weight older adults: An observational study. BioMed Central Public Health, 14(1), 35. https://doi.org/10.1186/1471-2458-14-35
GOV. UK (2020) Adult obesity: patterns and trends. Available at: https://www.gov.uk/government/publications/adult-obesity-patterns-and-trends. (Accessed: 10 January 2021).
Gulland, A. (2010). ‘Obesity among over 65s in UK reflects “lifetime of gaining weight.”’ British Medical Journal, 341. https://doi.org/10.1136/bmj.c3585.
Hainer, V., & Aldhoon-Hainerova, I. (2013). Obesity Paradox Does Exist. Diabetes Care, 36(2), S276–S281. https://doi.org/10.2337/dcS13-2023
Han, T. S., Tajar, A., & Lean, M. E. J. (2011). Obesity and weight management in the elderly. British Medical Bulletin, 97, 169–196. https://doi.org/10.1093/bmb/ldr002
Hernández, B., Reilly, R.B., & Kenny, R.A. (2019). ‘Investigation of multimorbidity and prevalent disease combinations in older Irish adults using network analysis and association rules.’ Scientific Reports, 9(1). https://doi.org/10.1038/s41598-019-51135-7.
Hulman, A., Ibsen, D.B., Laursen, A.S.D., & Dahm, C.C. (2019). ‘Body mass index trajectories preceding first report of poor self-rated health: A longitudinal case-control analysis of the English Longitudinal Study of Ageing’. PLoS One, 14(2). Available at: https://doi.org/10.1371/journal.pone.0212862.
Institute for Fiscal Studies (2018). Data. Economic and Social Research Council. Available at: https://www.ifs.org.uk/research-data (Accessed: 2 May 2018).
Jackson, S. E., Beeken, R. J., & Wardle, J. (2015). Obesity, perceived weight discrimination, and psychological well-being in older adults in England. Obesity, 23(5), 1105–1111. https://doi.org/10.1002/oby.21052
Jackson, S. E., Williams, K., Beeken, R. J., & Steptoe, A. (2019). Changes in Health and Wellbeing in the Years Leading up to a Cancer Diagnosis: A Prospective Cohort Study. Cancer Prevention Research, 12(2), 79–88. https://doi.org/10.1158/1940-6207.CAPR-18-0277
Janssen, I. (2007). Morbidity and mortality risk associated with an overweight BMI in older men and women. Obesity, 15(7), 1827–1840. https://doi.org/10.1038/oby.2007.217
Jehan, S., Auguste, E., Pandi-Perumal, S. R., Kalinowski, J., Myers, A. K., Zizi, F., Rajanna, M. G., Jean-Louis, G., & McFarlane, S. I. (2017). ‘Depression, Obstructive Sleep Apnea and Psychosocial Health.’ Sleep medicine and disorders: international journal, 1(3), pp. 00012. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5836734/. (Accessed: 2 July 2020).
Jura, M., & Kozak, L.P. (2016). Obesity and related consequences to ageing. American Aging Association. 38(23). https://doi.org/10.1007/s11357-016-9884-3.
Katz, D. A., McHorney, C. A., & Atkinson, R. L. (2000). Impact of obesity on health-related quality of life in patients with chronic illness. Journal of General Internal Medicine, 15(11), 789–796. https://doi.org/10.1046/j.1525-1497.2000.90906.x
Kuk, J. L., Saunders, T. J., Davidson, L. E., & Ross, R. (2009). Age-related changes in total and regional fat distribution. Ageing Research Reviews, 8(4), 339–348. https://doi.org/10.1016/j.arr.2009.06.001
Leal Neto, J. D. S., Barbosa, A. R., & Meneghini, V. (2016). Diseases and chronic health conditions, multimorbidity and body mass index in older adults. Brazilian Journal of Kin Anthropometry and Human Performance, 18(5), 509–519. https://doi.org/10.5007/1980-0037.2016v18n5p509
Li, J., Green, M., Kearns, B., Holding, E., Smith, C., Haywood, A., Cooper, C., Strong, M., & Relton, C. (2016). Patterns of multimorbidity and their association with health outcomes within Yorkshire, England: baseline results from the Yorkshire Health Study. BioMed Central Public Health, 16(1). https://doi.org/10.1186/s12889-016-3335-z.
Local Government Association (2020). Social care and obesity. Available at: https://local.gov.uk/publications/social-care-and-obesity (Accessed: 20 February 2021).
López-García, E., Banegas Banegas, J. R., Gutiérrez-Fisac, J. L., Gzaciani Pérez-Regadera, A., Díez- Gañán, L., & Rodríguez-Artalejo, F. (2003). Relation between body weight and health-related quality of life among the elderly in Spain. International Journal of Obesity, 27(6), 701–709. https://doi.org/10.1038/sj.ijo.0802275
Lumsden, M. A., & Hor, K. (2015). Impact of obesity on the health of women in midlife. Royal College of Obstetrician & Gynaecologist, 17(3), 201–208. https://doi.org/10.1111/tog.12199
Macleod, U., Mitchell, E., Black, M., & Spence, G. (2004). Comorbidity and socio-economic deprivation: An observational study of the prevalence of comorbidity in general practice. European Journal of General Practice, 10(1), 24–26. https://doi.org/10.3109/13814780409094223
Nam, S., Kuo, Y. F., Markides, K. S., & Al Snih, S. (2012). Waist circumference (WC), body mass index (BMI), and disability among older adults in Latin American and the Caribbean (LAC). Archives of Gerontology and Geriatrics, 55(2), e40–e47. https://doi.org/10.1016/j.archger.2012.04.006
National Health Service (NHS) (2006). Care pathway for the management of overweight and obesity. Available at: http://www.htmc.co.uk/resource/data/htmc1/docs/Care%20pathway%20for%20the%20management%20of%20overweight%20and%20obesity.pdf (Accessed: 14 May 2019).
National Health Service (NHS) England (2014). Report of the working group into: Joined up clinical pathways for obesity. Available at: https://www.england.nhs.uk/wp-content/uploads/2014/03/owg-join-clinc-path.pdf (Accessed: 25 March 2019).
National Health Service (NHS) Digital (2019). Statistics on Obesity, Physical Activity and Diet, England, 2019: Obesity related hospital admissions for bariatric surgery. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-obesity-physical-activity-and-diet/statistics-on-obesity-physical-activity-and-diet-england-2019/part-1-obesity-related-hospital-admissions#obesity-related-hospital-admissions-for-bariatric-surgery (Accessed: 12 January 2022).
National Institute for Health and Care Excellence (NICE) (2014). Obesity: Identification, assessment and management. Available at: https://www.nice.org.uk/guidance/cg189 (Accessed: 18 January 2019).
National Obesity Forum (2005). Obesity Care Pathway Toolkit. Available at: http://www.nationalobesityforum.org.uk/images/stories/care-pathway-toolkit/Toolkit_supporting_obesity_care_pathway_annexes_1_to_9__Feb_07_2006.pdf (Accessed: 18 April 2018).
Ng, T.P., Jin, A., Chow, K.Y., Feng, L., Nyunt, M.S.Z., & Yap, K.B. (2017). Age-dependent relationships between body mass index and mortality: Singapore longitudinal ageing study. PloS One, 12(7). https://doi.org/10.1371/journal.pone.0180818.
Office for National Statistics (ONS) (2013). Adult Health in Great Britain. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandlifeexpectancies/compendium/opinionsandlifestylesurvey/2015-0319/adulthealthingreatbritain2013. (Accessed: 6 March 2019).
Ofori-Asenso, R., Chin, K. L., Curtis, A. J., Zomer, E., Zoungas, S., & Liew, D. (2019). Recent Patterns of Multimorbidity Among Older Adults in High-Income Countries. Population Health Management, 22(2), 127–137. https://doi.org/10.1089/pop.2018.0069
Pantalone, K. M., Hobbs, T. M., Chagin, K. M., Kong, S. X., Wells, B. J., Kattan, M. W., Bouchard, J., Sakurada, B., Milinovich, A., Weng, W., Bauman, J., et al. (2017). Prevalence and recognition of obesity and its associated comorbidities: Cross-sectional analysis of electronic health record data from a large US integrated health system. British Medical Journal Open, 7(11), e017583. https://doi.org/10.1136/bmjopen-2017-017583
Pes, G. M., Licheri, G., Soro, S., Longo, N. P., Salis, R., Tomassini, G., Niolu, C., Errigo, A., & Dore, M. P. (2019). Overweight: A Protective Factor against Comorbidity in the Elderly. International Journal of Environmental Research and Public Health, 16(19), 3656. https://doi.org/10.3390/ijerph16193656
Pischon, T., Boeing, H., Hoffmann, K., Bergmann, M., Schulze, M. B., et al. (2008). General and abdominal adiposity and risk of death in Europe. The New England Journal of Medicine, 359(20), 2105–2120. https://doi.org/10.1056/NEJMoa0801891
Pongiglione, B., Ploubidis, G. B., & De Stavola, B. L. (2017). Levels of disability in the older population of England: Comparing binary and ordinal classifications. Disability and Health Journal, 10(4), 509–517. https://doi.org/10.1016/j.dhjo.2017.01.005
Public Health Wandsworth Council (2018). Wandsworth healthy weight care pathway toolkit’ by public health Wandsworth council. Available at: https://search3.openobjects.com/mediamanager/wandsworth/fsd/docs/healthy_weight_toolkit.pdf (Accessed: 26 May 2019).
Public Health England (PHE) (2019). Guidance: Adult obesity: applying All Our Health. Available at: https://www.gov.uk/government/publications/adult-obesity-applying-all-our-health/adult-obesity-applying-all-our-health. (Accessed: 17 September 2020)#
Sach, T. H., Barton, G. R., Doherty, M., Muir, K. R., Jenkinson, C., & Avery, A. J. (2006). The relationship between body mass index and health-related quality of life: comparing the EQ-5D, EuroQol VAS and SF-6D. International Journal of Obesity, 31(1), 189–196. https://doi.org/10.1038/sj.ijo.0803365
Salisbury, C. (2013). Multimorbidity: Redesigning health care for people who use it. The Lancet, 380(9836), 7–9. https://doi.org/10.1016/S0140-6736(12)60482-6
Sawada, M., Kubota, N., Sekine, R., Yakabe, M., Kojima, T., Umeda-Kameyama, Y., Usami, S., Akishita, M., & Ogawa, S. (2021). Sex-related differences in the effects of nutritional status and body composition on functional disability in the elderly. PLoS ONE, 16(2), e0246276. https://doi.org/10.1371/journal.pone.0246276
Shankar, A., Rafnsson, S. B., & Steptoe, A. (2014). Longitudinal associations between social connections and subjective wellbeing in the English Longitudinal Study of Ageing. Psychology & Health, 30(6), 686–698. https://doi.org/10.1080/08870446.2014.979823
Singer, L., Green, M., Rowe, F., Ben-Shlomo, Y., & Morrissey, K. (2019). ‘Social determinants of multimorbidity and multiple functional limitations among the ageing population of England’, 2002–2015. SSM - Population Health, 8, 100413. https://doi.org/10.1016/j.ssmph.2019.100413
Slater, N., Rowley, C., Venables, R.H., White, S., & Frisher, M. (2018). Evaluating associations between metabolic health, obesity and depressive symptoms: a prospective analysis of data from the English Longitudinal Study of Ageing (ELSA) with a 2 year follow up. British Medical Journal Open, 8(12). https://doi.org/10.1136/bmjopen-2018-025394.
Steptoe, A., Deaton, A., & Stone, A. A. (2015). Subjective wellbeing, health, and ageing. The Lancet, 385(9968), 640–648. https://doi.org/10.1016/S0140-6736(13)61489-0
Trull, T. J., Vergés, A., Wood, P. K., Jahng, S., & Sher, K. J. (2012). The structure of Diagnostic and Statistical Manual of Mental Disorders (4th edition, text revision) personality disorder symptoms in a large national sample. Personality Disorders, 3(4), 355–369. https://doi.org/10.1037/a0027766
UK data Service (UKDS) (2018). English Longitudinal Study of Ageing: Waves 0–7, 1998–2015. Available at: https://discover.ukdataservice.ac.uk/catalogue/?sn=5050&type=Data%20catalogue (Accessed: 11 April 2018).
Wei, K., Nyunt, M.-S.-Z., Gao, Q., Wee, S.-L., Yap, K.-B., & Ng, T.-P. (2018). Association of Frailty and Malnutrition with Long-term Functional and Mortality Outcomes Among Community-Dwelling Older Adults. The Journal of the American Medical Association Network Open, 1(3). https://doi.org/10.1001/jamanetworkopen.2018.0650.
Zaninotto, P., Pierce, M., Breeze, E., de Oliveira, C., & Kumari, M. (2010). BMI and waist circumference as predictors of well-being in older adults: Findings from the English Longitudinal Study of Ageing. Obesity, 18(10), 1981–1987. https://doi.org/10.1038/oby.2009.497
Acknowledgements
I would like to express my deepest appreciation to my supervisor Professor Hafiz T.A. Khan, who believed in my abilities and dedication and motivated me to take up challenges, guided me through difficult periods, and offered constructive criticism during my study and beyond. I would also like to thank my co-supervisor, Dr Salim Vohra.
I am grateful to the University of West London PhD Studentship that assisted me to focus entirely on maximising my research productivity. I express my sincere and earnest thankfulness to the College of Nursing, Midwifery and Healthcare, the committee members, and the admin staff of the Graduate School of the University of West London.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Declarations of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ghosh, G., Khan, H.T.A. & Vohra, S. Differentials in Health and Wellbeing in Older Adults with Obesity in England: A Cross-Sectional Analysis Using the English Longitudinal Study of Ageing. Population Ageing 16, 819–847 (2023). https://doi.org/10.1007/s12062-022-09386-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12062-022-09386-2