
Abstract
According to the published European public health policies, emphasis should be given on the identification of high-risk areas, in terms of both Cardiovascular Diseases (CVDs) incidence, as well as of its main clinical risk factors. Thus, we aimed to investigate: (a) the geographical variability of the sex and age-specific 10-year incidence of CVDs and its clinical risk factors in the Athens metropolitan area, the most urbanised city in Greece accounting for about 35% of the total Greek population, and (b) the spatial heterogeneity of the association between the main clinical risk factors and the 10-year CVD incidence at an aggregated level. Data regarding the 10-year CVD incidence (% of population in each municipality with any CVD after the 10-year period), as well as the prevalence of the risk factors (obesity, hypertension, diabetes mellitus, hypercholesterolaemia; expressed as % of population in each municipality) were provided by the ATTICA epidemiological study for 2020 individuals found during the 10-year follow-up with complete data for locality geocoding. Socio-economic, demographic, and environmental characteristics for each municipality of the Attica region, were obtained from official national and international databases. A local statistical modelling approach, namely the Geographically Weighted Regression, was implemented in order to investigate the associations at a local level and therefore give emphasis on the design of more effective public health programs, taking into account the special characteristics of each area. Hypercholesterolaemia was found to be the most prevalent clinical risk factor in the study area, while higher prevalence for all the risk factors were presented in areas of lower socioeconomic status (SES), where a significantly higher number of new CVD cases in the decade were detected as well. 10-year CVD incidence was also found to be significantly elevated in areas characterized by worse health status in terms of the risk factors’ prevalence, while the sex and age- specific CVD incidence rates were found to be differently affected by these factors. Interestingly, despite the fact that CVDs are acknowledged as a man’s disease, areas of higher (South & North) and moderate (East) SES were found to be characterized by higher CVD incidence rates in females, while in areas of lower SES (West), higher CVD incidence rates were found in males. In line with the current European policy, the identification of areas where the intensity of the studied associations is stronger, can be considered a crucial methodological aspect for the design and implementation of more effective CVD prevention programs at the community level.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
According to the World Health Organization (WHO), noncommunicable diseases (NCDs) cause approximately 41 million deaths annually, a figure which is aimed to be reduced by a third until 2030 according to the UN Sustainable Development Goals (2015). Cardiovascular diseases (CVDs), which account for the majority of the NCDs, are estimated to have caused 330 million years of life lost and another 35.6 million years lived with disability until today (GBD 2019 Demographics Collaborators, 2020; GBD 2019 Diseases and Injuries Collaborators, 2020), while in Europe, despite the decline in the CVDs- specific mortality rates observed during the past 30 years, still remain responsible for more than 64 million disability-adjusted life years (DALYs), (Timmis et al., 2018).
During the last decades, several investigators have extensively reported the modifiable risk factors of both CVD mortality and incidence at the individual level, the most important of which are the behavioral (diet, low physical activity, smoking, alcohol use) and the clinical risk factors (high systolic blood pressure, high total cholesterol, high fasting plasma glucose, and high body mass index (BMI)) (Timmis et al., 2018). However, the investigation of the spatial variability of the association between these risk factors and the CVD incidence, especially in the European region, is limited, despite the fact that such an investigation could provide great input for the design and implementation of effective public health programs aiming at reducing the CVD burden. The implementation of local statistical modelling approaches, such as the Geographically Weighted Regression (GWR), is considered a significant methodological approach for such aims, as the geographic variation in risk factors for CVDs is too complex to be captured by a single set of regression coefficients (Sarra & Nissi, 2016). Furthermore, as outlined in previous studies (Aturinde et al., 2021), in order to manage the effects of multiple risk factors on CVDs, public health policies should be informed of the areas where these effects are more pronounced, so as to design and implement area-specific interventions. Nevertheless, the study of such non- homogeneous spatial patterns between disease outcomes and a set of risk factors, could provide valuable and actionable tools for disease management (Alves et al., 2016; Feuillet et al., 2015).
Thus, based on the data from a large representative sample of the Greek population residing in the Athens metropolitan area, namely the prospective ATTICA epidemiological study, the main aim of the present work was to identify the spatial variability of the sex and age-specific 10-year CVD incidence in the most urbanised city of Greece, as well as, to examine the non- stationarity of the relationship between the most widely acknowledged clinical risk factors (obesity, hypertension, hypercholesterolemia and diabetes mellitus) and the 10-year CVD incidence at a local level, aiming at the identification of high-risk areas, which is going to have a significant contribution on the design and implementation of more effective CVD prevention programs at the community level.
Material and Methods
Design
The ATTICA study, being consisted of a large representative sample of the Greek population residing in the Athens metropolitan area, is a prospective, observational cohort investigation, that was initiated in 2001–2002 and included two follow- up examinations in 2006 and in 2011–2012, respectively (Panagiotakos et al., 2015; Panagiotakos et al., 2008; Pitsavos et al., 2003). The particular study constitutes one of the most important studies, both in Greece, as well as at an international level, as hitherto it has given great research insights in the field of chronic diseases and CVD epidemiology (Kouvari et al., 2020a, b, c, 2022; Panagiotakos et al., 2019).
Sample
The sampling procedure of the ATTICA epidemiological study was random, multistage (by city) and it was based on the age – sex distribution of the province of Attica provided by the National Statistical Service, according to the census of 2001. Only one participant per household was enrolled, while according to the study’s protocol all people living in institutions were excluded from the sampling. From May 2001 to December 2002, 4056 inhabitants from the above area were randomly selected and asked to participate into the study. Of them, a representative sample of 3042 apparently healthy volunteers residing in 40 municipalities of the Athens metropolitan area agreed to participate at baseline (2001–2002) (75% participation rate). It is noted that there were no significant differences between those who participated and those who did not fulfil the study’s inclusion criteria (Panagiotakos et al., 2015; Panagiotakos et al., 2008; Pitsavos et al., 2003). Of the enrolled participants, 1514 (49.8%) were men [mean age = 46 (Standard Deviation (SD) = 13) years old] and 1528 (50.2%) were women [mean age = 45 (SD = 14) years old]. During the 10-year follow-up conducted in 2012, 2020 of the 3042 initially enrolled participants were found (66% participation rate; no significant differences were observed as regards social and clinical characteristics between those who lost to follow up and the rest (Tsiampalis & Panagiotakos, 2020; Tsiampalis et al., 2021a)). For the aim of the present work, we used data from the 2020 participants found during the follow-up with complete data for locality geocoding in 40 different municipalities of the Athens Metropolitan area (i.e., physical address, municipality, and postcode); of them, 1014 (50.2%) were women [mean age = 45 (SD = 14) years old] and 1006 (49.8%) were men [mean age = 46 (SD = 13) years old]. Further details regarding the methods and the sampling procedure applied in the ATTICA study have been previously detailed (Pitsavos et al., 2003).
Bioethics
The ATTICA study was approved by the Bioethics Committee of Athens Medical School. The study was carried out in accordance with the Declaration of Wolinsky (2006) of the World Medical Association. All participants were informed about the study aims and procedures and provided written informed consent.
Setting
The study area was the Athens metropolitan area, which is the capital city of Greece including 58 municipalities, which are organized in 7 regional units. Athens is the most urbanised city in Greece, with 3,828,434 population (2011 census), accounting for about 35% of the country’s total population. For the scope of the present work, the analysis was restricted to 40 municipalities of the metropolitan area of Athens, with a population of 3,338,131, due to the available data for geocoding of the 2020 ATTICA study participants. Based on their socio- economic characteristics, the remaining 40 municipalities were reformed in the following five sectors, so as to be characterized by common socioeconomic status (SES): North sector- the highest SES (Ns; 10 municipalities–487,762 population), South sector- high SES (Ss; 7 municipalities–435,188 population), East sector-moderate SES (Es; 7 municipalities–404,261 population), West sector- low SES (Ws; 11 municipalities–809,258 population) and Central sector- mixed SES (Cs; 5 municipalities–1,201,662 population).
Data Sources
Socio- Economic and Demographic Characteristics
Socio-economic and demographic characteristics for the population in the study area, were provided by the Hellenic Statistical Authority and the General Secretariat for Information Systems of the Greek Ministry of Economy and Finance. In particular, the socio-economic indicators which were used in the present work were, the average annual income (in thousand euros), the unemployment rate (%), the illiterate population (% of population that has not completed primary school – International Standard Classification of Education (ISCED) level 0 (United Nations Educational Scientific and Cultural Organization Institute for Statistics, 2012)) and the immigrant population (%), while the female population (%), the mean population’s age (in years) and the married population (%) were the population’s demographic characteristics which were used in the present work.
Environmental Characteristics
Environmental characteristics for the study area were provided by the Urban Atlas (Prastacos et al., 2011) which is a joint initiative of the European Commission Directorate-General for Regional and Urban Policy and the Directorate-General for Enterprise and Industry. Specifically, the land coverage by green urban areas and sports facilities (% of the municipalities’ extent) were drawn from the previously mentioned sources, as the focus of the present work was to adjust the results for the built environment’s characteristics, since the lifestyle characteristics were provided by the ATTICA epidemiological study, in contrast to the study of Tabb et al., 2020.
Lifestyle Characteristics
Dietary Assessment- Level of Adherence to Mediterranean Diet
The level of adherence to the Mediterranean diet was estimated by an 11-item diet index, the MedDietScore (range: 0–55) (Panagiotakos et al., 2006), which was applied to all the participants of the ATTICA study. This scale consists of 11 items estimating the frequency with which individuals consume several foods, which are either close to the Mediterranean diet (e.g., fruits, vegetables, non-refined cereals, and products), or away (e.g., meat and meat products). Higher values of this scale indicate adherence to the traditional Mediterranean diet, while lower values indicate adherence to the “Westernized” diet. The median MedDietScore value was used as a cut-off point, based on which, participants scoring≤26 were classified as having unhealthy dietary habits, in terms of a low level of adherence to the Mediterranean diet. For the aims of the present work, the percent (%) of people with low adherence to the Mediterranean diet at the municipality level was used, as the sample of the ATTICA study was representative of the population residing in each municipality.
Physical Activity Status
Participants’ physical activity status was evaluated through the validated short Greek version (9 items) of the “International Physical Activity Questionnaire” (IPAQ). According to the reported physical activities, participants were classified into four categories: inactive, low (i.e., <150 metabolic equivalent - MET-minutes/week), moderate (150–300 MET-minutes/week) and Healthy Engaged Physically Active - HEPA (>300 MET-minutes/week) (Papathanasiou et al., 2009). For the purposes of the present work participants were further classified into two main categories, inactive (sedentary) and physically active; the % of people with sedentary lifestyle at the municipality level was used, as the sample of the ATTICA study was representative of the population residing in each municipality.
Smoking Habits
Participants’ smoking habits were evaluated through pack-years of smoking (a pack year was defined as twenty cigarettes smoked daily for one year.). Current smokers were defined as those who reported smoking at least one cigarette or any type of tobacco per day at the time of the interview, while former smokers were defined as those who previously smoked but had quitted within the previous year before enrolment.
Finally, based on the participants’ smoking habits and physical activity status, participants were further classified into two main categories, as those having a healthier lifestyle (non- smokers and physically active) and those having an unhealthier lifestyle (current/ former smokers, or physically inactive) in terms of smoking habits and physical activity status. The % of those having an unhealthy lifestyle at the municipality level was used, as the sample of the ATTICA study was representative of the population residing in each municipality.
Clinical Characteristics
Assessment of clinical characteristics in the ATTICA study’s participants (obesity, hypertension, hypercholesterolemia, and diabetes mellitus) was performed according to established physical examination procedures and pharmaceutical treatment.
Obesity
Height and weight were measured to the nearest 0.5 cm and 100 g respectively. BMI was then calculated and based on the WHO cut-off points (WHO, 2000), obesity was defined as BMI greater than 29.9 kg/m2. The % of those classified as obese at the municipality level was used, as the sample of the ATTICA study was representative of the population residing in each municipality.
Hypertension
Arterial blood pressure was measured and participants whose average blood pressure levels were ≥ 140/90 mmHg or were under antihypertensive medication were classified as having hypertension. The % of those classified as hypertensive at the municipality level was used, as the sample of the ATTICA study was representative of the population residing in each municipality.
Hypercholesterolaemia
Total serum cholesterol was measured using a chromatographic enzymic method in a Technicon automatic analyser RA-1000 and hypercholesterolemia was defined as total cholesterol levels greater than 200 mg/dl or the use of lipid-lowering agents. The % of those diagnosed with hypercholesterolaemia at the municipality level was used, as the sample of the ATTICA study was representative of the population residing in each municipality.
Diabetes Mellitus
Blood glucose levels (mg/dl) were measured with a Beckman Glucose Analyzer and diabetes mellitus (type 2) was defined according to the American Diabetes Association diagnostic criteria (i.e. blood glucose levels >125 mg/dl classified participants as having diabetes). The % of those diagnosed with diabetes mellitus at the municipality level was used, as the sample of the ATTICA study was representative of the population residing in each municipality.
Clinical Endpoint- 10-Year CVD Incidence
The endpoint studied in the present work was the development of a first fatal or non-fatal CVD event during the 10-year follow-up, which was defined as the development of: myocardial infarction, or angina pectoris, or other identified forms of ischemia (WHO-ICD coding 410–414.9, 427.2, 427.6), or heart failure of different types and chronic arrhythmias (WHO-ICD coding 400.0–404.9, 427.0–427.5, 427.9-) or the development of stroke (WHO-ICD coding 430–438). The sex and age-specific 10-year CVD incidence (%) at the municipality level was used for the scope of the present analysis, as the sample of the ATTICA study was representative of the population residing in each municipality.
Data Analysis
Geographical Analysis
A spatial database was created in Geographic Information Systems (GIS) including all the aforementioned data and the spatial layers of the administrative units. Geocoding of ATTICA study participants’ characteristics was based on their residential address by attributing each observation to the district in which the participants were residing, and the aggregation was performed by summing up the observations per district to calculate the total number of people with each characteristic in each spatial unit. For mapping purposes, point features were used in the GIS system, and the spatial features’ construction was based on the vector data model. A series of GIS-supported procedures were implemented to geocode and aggregate all data by spatial unit. Choropleth maps were created to visualize the spatial distribution of all indicators, by using the quantile classification method, as the specific method generates comparable classification solutions which is considered to be extremely useful when there is need to make comparisons across maps, like in an atlas.
Global Statistical Modelling
Descriptive characteristics are presented as mean (SD) values, both for the total sample of the municipalities, as well as, separately according to the sector in which they belong. Beta- coefficients (β) and their corresponding 95% Confidence Intervals were evaluated through univariable and multivariable linear regression analysis, which was used to investigate the significant predictors of higher sex and age-specific 10-year CVD incidence. The final multivariable model and the determination of the predictors was based on the minimization of the corrected Akaike’s Information Criterion (AICc). In particular, the final multivariable models for each clinical risk factor (obesity, hypertension, hypercholesterolaemia and diabetes mellitus) were adjusted for demographic, socioeconomic, environmental and lifestyle characteristics of the residential area (% Female population, Mean population’s age in years, % Married population, % Unemployment rate, % Illiterate population, % Land coverage by green urban areas, % Land coverage by sports facilities, % Unhealthy lifestyle, and % Unhealthy dietary habits).
Local Statistical Modelling
The spatial variation of the relationships identified through the global modelling, were investigated by the univariable and the multivariable Geographically Weighted Linear Regression analysis (GWR). The adaptive Gaussian kernel function was employed for the estimation of bandwidth in the GWR models, while the optimal number of nearest neighbours was determined by minimizing the corrected Akaike’s Information Criterion (AICc), which was also used for determining the final GWR model and for comparing the GWR model with the global model. As for the final multivariable GWR models regarding the relationship of each clinical risk factor with the 10-year incidence of cardiovascular diseases, the following equations were used:
-
(1)
Model 1- Effect of obesity on 10-year CVD incidence
$$\textrm{CVD}\ \textrm{incidencei}={\textrm{b}}_0\left({\textrm{u}}_{\textrm{i}}\right)+{\textrm{b}}_1\ \left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Prevalence}\ \textrm{of}\ \textrm{obesity},\%\right)+{\textrm{b}}_2\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Female}\ \textrm{population},\%\right)+{\textrm{b}}_3\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Mean}\ {\textrm{population}}^{'}\textrm{s}\ \textrm{age},\textrm{years}\right)+{\textrm{b}}_4\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Married}\ \textrm{population},\%\right)+{\textrm{b}}_5\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unemployment}\ \textrm{rate},\%\right)+{\textrm{b}}_6\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Illiterate}\ \textrm{population},\%\right)+{\textrm{b}}_7\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Land}\ \textrm{coverage}\ \textrm{by}\ \textrm{green}\ \textrm{urban}\ \textrm{areas},\%\right)+{\textrm{b}}_8\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Land}\ \textrm{coverage}\ \textrm{by}\ \textrm{s}\textrm{ports}\ \textrm{facilities},\%\right)+{\textrm{b}}_9\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unhealthy}\ \textrm{lifestyle},\%\right)+{\textrm{b}}_{10}\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unhealthy}\ \textrm{dietary}\ \textrm{habits},\%\right)$$ -
(2)
Model 2- Effect of hypertension on 10-year CVD incidence:
$$\textrm{CVD}\ \textrm{incidencei}={\textrm{b}}_0\left({\textrm{u}}_{\textrm{i}}\right)+{\textrm{b}}_1\ \left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Prevalence}\ \textrm{of}\ \textrm{hypertension},\%\right)+{\textrm{b}}_2\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Female}\ \textrm{population},\%\right)+{\textrm{b}}_3\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Mean}\ {\textrm{population}}^{'}\textrm{s}\ \textrm{age},\textrm{years}\right)+{\textrm{b}}_4\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Married}\ \textrm{population},\%\right)+{\textrm{b}}_5\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unemployment}\ \textrm{rate},\%\right)+{\textrm{b}}_6\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Illiterate}\ \textrm{population},\%\right)+{\textrm{b}}_7\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Land}\ \textrm{coverage}\ \textrm{by}\ \textrm{green}\ \textrm{urban}\ \textrm{areas},\%\right)+{\textrm{b}}_8\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Land}\ \textrm{coverage}\ \textrm{by}\ \textrm{s}\textrm{ports}\ \textrm{facilities},\%\right)+{\textrm{b}}_9\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unhealthy}\ \textrm{lifestyle},\%\right)+{\textrm{b}}_{10}\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unhealthy}\ \textrm{dietary}\ \textrm{habits},\%\right)$$ -
(3)
Model 3- Effect of hypercholesterolaemia on 10-year CVD incidence:
$$\textrm{CVD}\ \textrm{incidencei}={\textrm{b}}_0\left({\textrm{u}}_{\textrm{i}}\right)+{\textrm{b}}_1\ \left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Prevalence}\ \textrm{of}\ \textrm{hypercholesterolaemia},\%\right)+{\textrm{b}}_2\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Female}\ \textrm{population},\%\right)+{\textrm{b}}_3\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Mean}\ {\textrm{population}}^{'}\textrm{s}\ \textrm{age},\textrm{years}\right)+{\textrm{b}}_4\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Married}\ \textrm{population},\%\right)+{\textrm{b}}_5\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unemployment}\ \textrm{rate},\%\right)+{\textrm{b}}_6\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Illiterate}\ \textrm{population},\%\right)+{\textrm{b}}_7\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Land}\ \textrm{coverage}\ \textrm{by}\ \textrm{green}\ \textrm{urban}\ \textrm{areas},\%\right)+{\textrm{b}}_8\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Land}\ \textrm{coverage}\ \textrm{by}\ \textrm{s}\textrm{ports}\ \textrm{facilities},\%\right)+{\textrm{b}}_9\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unhealthy}\ \textrm{lifestyle},\%\right)+{\textrm{b}}_{10}\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unhealthy}\ \textrm{dietary}\ \textrm{habits},\%\right)$$ -
(4)
Model 4- Effect of diabetes mellitus on 10-year CVD incidence:
$$\textrm{CVD}\ \textrm{incidencei}={\textrm{b}}_0\left({\textrm{u}}_{\textrm{i}}\right)+{\textrm{b}}_1\ \left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Prevalence}\ \textrm{of}\ \textrm{diabetes}\ \textrm{mellitus},\%\right)+{\textrm{b}}_2\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Female}\ \textrm{population},\%\right)+{\textrm{b}}_3\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Mean}\ {\textrm{population}}^{'}\textrm{s}\ \textrm{age},\textrm{years}\right)+{\textrm{b}}_4\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Married}\ \textrm{population},\%\right)+{\textrm{b}}_5\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unemployment}\ \textrm{rate},\%\right)+{\textrm{b}}_6\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Illiterate}\ \textrm{population},\%\right)+{\textrm{b}}_7\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Land}\ \textrm{coverage}\ \textrm{by}\ \textrm{green}\ \textrm{urban}\ \textrm{areas},\%\right)+{\textrm{b}}_8\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Land}\ \textrm{coverage}\ \textrm{by}\ \textrm{s}\textrm{ports}\ \textrm{facilities},\%\right)+{\textrm{b}}_9\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unhealthy}\ \textrm{lifestyle},\%\right)+{\textrm{b}}_{10}\left({\textrm{u}}_{\textrm{i}}\right)\ast \left(\textrm{Unhealthy}\ \textrm{dietary}\ \textrm{habits},\%\right)$$
where ui = {uxi, uyi} the geographical location with (uxi, uyi) denoting the two-dimensional co-ordinates of municipalities’ centroids. It is noted that the multivariable GWR models were also applied to estimate the spatial variation of the relationship of the risk factors with the sex and age- stratified 10-year CVD incidence.
Finally, choropleth maps were created to visualize the spatial variability of the β-coefficients, based on the multivariable modelling approach. ArcGIS version 10.2 software was used for the creation of the spatial database, STATA version 14 was used for the spatial mapping and the global statistical modelling, while R version 3.6.1 and the R package GWmodel version 2.1–3 (Gollini et al., 2015) were used for the local statistical modelling.
Results
As presented in Table 1, in the decade approximately 13,000 new CVD cases per 100,000 population were presented in the study area, with the number of new CVD cases being higher in women (16,400 cases/ 100,000 population) compared to men (9000 cases/ 100,000 population), and in people aged ≥55 years old (36,300 cases/ 100,000 population) when compared to their younger counterparts (≤45 years old: 4300 cases/ 100,000 population; 46–54 years old: 17,600 cases/ 100,000 population). Hypercholesterolaemia was found to be the most prevalent clinical risk factor in the study area (38.7%), followed by hypertension (28.1%), obesity (17.7%) and diabetes mellitus (5.4%), while as for the population’s lifestyle, approximately three out of four and almost half of those residing in the study area were characterized as having an unhealthy lifestyle and unhealthy dietary habits, respectively. Furthermore, as it can be observed in Figs. 1 and 2, higher 10-year CVD incidence was detected in areas characterized by lower SES, for both sexes and all age groups, where higher prevalence of all the risk factors was presented as well, while it is also worth noting the fact that the number of new CVD cases in the decade presented in the West sector (lowest SES) was at least 2 times higher when compared to the North sector (highest SES) in all sex and age strata.

Spatial variability of the sex and age- specific 10-year incidence of cardiovascular diseases for the population residing in the Athens metropolitan area; ATTICA epidemiological study, Greece (2002–2012). Notes: CVD = cardiovascular diseases; 10-year CVD incidence was defined the development of a first fatal or non-fatal CVD event during the 10-year follow-up, and more specifically as the development of: Myocardial infarction, or angina pectoris, or other identified forms of ischemia (WHO-ICD coding 410–414.9, 427.2, 427.6), or heart failure of different types and chronic arrhythmias (WHO-ICD coding 400.0–404.9, 427.0–427.5, 427.9-) or the development of stroke (WHO-ICD coding 430–438); north sector- the highest SES (ns; 10 municipalities–487,762 population), south sector- high SES (Ss; 7 municipalities–435,188 population), east sector-moderate SES (Es; 7 municipalities–404,261 population), west sector- low SES (Ws; 11 municipalities–809,258 population) and central sector- mixed SES (Cs; 5 municipalities–1,201,662 population)




Spatial variability of the (a) socio-economic, (b) environmental, (c) lifestyle and (d) clinical characteristics for the population residing in the Athens metropolitan area; ATTICA epidemiological study, Greece (2002–2012). Notes: Illiterate population was determined as the % of population that has not completed primary school – International standard classification of education (ISCED) level 0; adherence to the Mediterranean diet was measured via the MedDietScore scale (score: 0–55) in the participants of the ATTICA epidemiological study and those scoring≤26 in the MedDietScore scale (median score), were classified as having unhealthy dietary habits; level of physical activity was measured in METS- minutes via the IPAQ questionnaire in the participants of the ATTICA epidemiological study; healthy lifestyle = non- smokers and physically active participants, unhealthy lifestyle = either smokers, or physically inactive participants; obesity was defined as BMI greater than 29.9 kg/m2; participants whose average blood pressure levels were ≥ 140/90 mmHg or were under antihypertensive medication were classified as having hypertension; hypercholesterolemia was defined as total cholesterol levels greater than 200 mg/dl or the use of lipid-lowering agents; diabetes mellitus (type 2) was defined according to the American Diabetes Association diagnostic criteria (i.e. blood glucose levels >125 mg/dl classified participants as having diabetes); north sector- the highest SES (ns; 10 municipalities–487,762 population), south sector- high SES (Ss; 7 municipalities–435,188 population), east sector-moderate SES (Es; 7 municipalities–404,261 population), west sector- low SES (Ws; 11 municipalities–809,258 population) and central sector- mixed SES (Cs; 5 municipalities–1,201,662 population)
Based on the results from the multivariable ordinary least squares regression analysis (Table 2), after taking into account the demographic, socioeconomic, environmental and lifestyle profile of each area’s residents, the 10-year CVD incidence rate was found to be significantly higher in areas characterized by higher prevalence of all the clinical risk factors (all p-values<0.05). More specifically, in the total population, areas with 10% higher prevalence of diabetes mellitus (β-coefficient = 1.26, 95% CI = 0.78, 1.71; per 1% increment), obesity (β-coefficient = 0.42, 95% CI = 0.08, 0.76; per 1% increment), hypertension (β-coefficient = 0.36, 95% CI = 0.02, 0.70; per 1% increment) and hypercholesterolaemia (β-coefficient = 0.27, 95% CI = 0.04, 0.51; per 1% increment), were characterized by 12.6%, 4.2%, 3.6% and 2.7% higher CVD incidence rate, respectively. As for the sex and age- specific CVD incidence rates, they were found to be differently affected by these characteristics. In particular, 10-year CVD incidence in women was significantly affected by all the risk factors except for the hypertension (β-coefficient = 0.27, 95% CI = −0.07, 0.60), while male-specific CVD incidence was only affected by the prevalence of diabetes mellitus in the area. It is also worth noting the fact, that the effect of diabetes mellitus was found to be significantly higher on male- specific CVD incidence rate, as areas characterized by 10% higher prevalence of diabetes mellitus, were characterized by approximately 2.5 times higher male- specific CVD incidence rate (16.2%; β-coefficient = 1.62, 95% CI = 0.81, 2.42; per 1% increment), than female specific (6.7%; β-coefficient = 0.67, 95% CI = 0.12, 1.23; per 1% increment). In addition, in areas characterized by higher prevalence of obesity, hypertension and diabetes mellitus a significantly higher number of new CVD cases was detected among people aged less than 45 years old, while in the same areas higher 10-year CVD incidence was presented among people aged 46–54 years old, as well, with the associations although being of borderline significance (p-values<0.10). Moreover, it should be noted that despite the fact that both the “≤45 years” specific CVD incidence rate, and the “≥55 years” specific CVD incidence rate were mainly affected by the prevalence of diabetes mellitus in the area (R2 = 18% and 8%, respectively), the most contributing factor to the “46–54 years” specific CVD incidence rate seemed to be the prevalence of obesity (R2 = 8.4%).
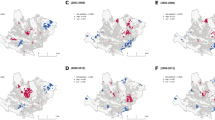
According to the GWR analysis the spatial heterogeneity and the non-stationarity of the studied associations were revealed (Fig. 3). It is noted here that the local statistical models’ AICc values (Obesity: 493, Hypertension: 502, Hypercholesterolemia: 497 and Diabetes mellitus: 620) were lower than the global’ s (Obesity: 1089, Hypertension: 1205, Hypercholesterolemia: 925 and Diabetes mellitus: 1103), indicating the better quality of GWR models in all cases. Specifically, as regards the total population and the females, all the risk factors seemed to have the weakest positive effect on the 10-year CVD incidence in areas of the highest SES (Ns). On the contrary, the greatest effect of diabetes mellitus, hypercholesterolaemia and obesity on the 10-year CVD incidence among males was presented in areas of the Ss and the Es. Besides, the greatest effect of the prevalence of diabetes mellitus, hypertension, and obesity on the 10-year CVD incidence among younger people (≤ 45 years old) was presented in areas of the Ws, which also found to be true for the effect of diabetes mellitus and hypertension on the 10-year CVD incidence among people older than 46 years old. Finally, the greatest effect of the prevalence of obesity and hypercholesterolaemia on the number of new CVD cases in the decade among people aged more than 46 years old was presented in areas of the highest SES. It is also noted that after the exclusion of extreme values in risk factors’ prevalence, the estimated coefficients did not change substantially. The results for the GWR models are presented in more detail in the Supplementary Table 1.




Spatial variability of the effect of the prevalence of (a) diabetes mellitus, (b) hypercholesterolaemia, (c) hypertension and (d) obesity on the sex and age- specific 10-year CVD incidence for the population residing in the Athens metropolitan area; ATTICA epidemiological study, Greece (2002–2012). Notes: Results are based on the multivariable geographically weighted regression analysis. CVD = cardiovascular diseases; 10-year CVD incidence was defined the development of a first fatal or non-fatal CVD event during the 10-year follow-up, and more specifically as the development of: Myocardial infarction, or angina pectoris, or other identified forms of ischemia (WHO-ICD coding 410–414.9, 427.2, 427.6), or heart failure of different types and chronic arrhythmias (WHO-ICD coding 400.0–404.9, 427.0–427.5, 427.9-) or the development of stroke (WHO-ICD coding 430–438); obesity was defined as BMI greater than 29.9 kg/m2; participants whose average blood pressure levels were ≥ 140/90 mmHg or were under antihypertensive medication were classified as having hypertension; hypercholesterolemia was defined as total cholesterol levels greater than 200 mg/dl or the use of lipid-lowering agents; diabetes mellitus (type 2) was defined according to the American Diabetes Association diagnostic criteria (i.e. blood glucose levels >125 mg/dl classified participants as having diabetes); north sector- the highest SES (ns; 10 municipalities–487,762 population), south sector- high SES (Ss; 7 municipalities–435,188 population), east sector-moderate SES (Es; 7 municipalities–404,261 population), west sector- low SES (Ws; 11 municipalities–809,258 population) and central sector- mixed SES (Cs; 5 municipalities–1,201,662 population)
Discussion
The present work aimed at identifying the geographical variability of the sex and age-specific 10-year CVD incidence and its clinical risk factors in the metropolitan area of Athens, as well as at investigating the spatial heterogeneity and the non-stationarity of the association between the risk factors and the number of new CVD cases in the decade at the community level. Data analyses revealed that hypercholesterolaemia was the most prevalent risk factor in the study area, while higher prevalence rates for all the risk factors were presented in areas of lower SES, where a significantly higher number of new CVD cases in the decade were detected as well. 10-year CVD incidence was also found to be significantly elevated in areas characterized by worse health status in terms of the risk factors’ prevalence, while the sex and age- specific CVD incidence rates were found to be differently affected by these factors.
The inverse association found between the area’s SES and the population’ health, in terms of the higher prevalence of all the clinical risk factors, as well as the higher 10-year CVD incidence, has been well documented in previous research works (Stringhini et al., 2017; Psaltopoulou et al., 2017), with only a small number of them although having been conducted at the area level (Faka et al., 2018, 2019, 2020). In developed countries, there is a growing body of evidence, suggesting the harmful effect of several SES indicators, such as education and household income or expenditures, on serum lipid levels (Backholer et al., 2017), obesity (Dinsa et al., 2012) and hypertension (Leng et al., 2015), both in men and women, as the low-SES population is known to have unhealthier lifestyle behaviours (e.g. cigarette smoking and alcohol consumption) (Leng et al., 2015), poorer dietary habits (Tsiampalis et al., 2020), health status (Tsiampalis et al., 2021b) and quality of life. Besides, several epidemiological studies conducted at the individual level, have already confirmed the inverse association between diabetes mellitus and SES (Espelt et al., 2011), while regional deprivation, which is often used as a proxy for individual SES, has been reported to have an independent negative impact both on the incidence and the prevalence of diabetes mellitus (Maier et al., 2013). Likewise, many investigators have previously reported that lower educational level, which is often used as a proxy for broader social disadvantage, is directly connected with higher CVD incidence and mortality (Mackenbach et al., 2000), as it lessens the individuals’ ability to obtain effective healthcare by lowering their awareness regarding the importance of seeking timely care (Rosengren et al., 2009; Matheus et al., 2013).
Interestingly, despite the fact that CVDs are being widely acknowledged as a man’s disease, areas of higher (South & North) and moderate (East) SES were found to be characterized by higher CVD incidence rates in females. These findings come to support all the research initiatives and campaigns made for raising the awareness (Suero-Abreu et al., 2020), both concerning the sex differences in CVD, as well as the importance of CVD in the female population (Peters et al., 2019; Kouvari et al., 2019, 2020a, b, c). Besides, the women’s global health agenda, containing several policies and practices which address the sex equality in CVD prevention, has recently been reformulated to address more accurately the CVD prevention, diagnosis, and treatment. In accordance with these initiatives, as underscored by Kouvari et al. (2020a, b, c), a multidimensional approach is needed for the generation of evidence- based decisions, which will incorporate both sex, as well as gender- specific guidelines for improving the CVD prevention, management, and rehabilitation procedures.
Our findings regarding the association of the risk factors with the 10-year CVD incidence at the municipality level, are in full concordance with previous studies having demonstrated the negative impact of all the risk factors on the individuals’ CVD risk. Diabetes mellitus, which was found to have the greatest contribution on the increase of the 10-year CVD incidence in the study area, is widely acknowledged to be directly connected with the overexpression of many cytokines by adipose tissue (Chait et al., 2005; Félix-Redondo et al., 2013), having a detrimental effect on blood vessels and leading to the development of cardiomyopathy and myocardial infraction (Chait et al., 2005). In addition, several investigators have previously reported that obese individuals are more likely to develop cardiovascular diseases and other health problems when compared to their normal-weight counterparts (Prospective Studies Collaboration et al., 2009; Schneider et al., 2010). Furthermore, the harmful effect of hypertension and hypercholesterolaemia on CVD incidence and mortality have long been recognized by several epidemiological studies, showing that hypertension increases the individuals’ CVD risk for at least two times, while increased level of serum cholesterol increases the risk of premature death from coronary heart disease (Neaton & Wentworth, 1992).
Despite the fact that the association of CVD incidence with all these clinical risk factors has been widely examined and acknowledged by several research teams at the individual- level, the present investigation has a strong added- value for the relevant literature, due to the implementation of the local statistical modelling approach. In particular, the specific approach is considered to be crucial when modelling the epidemiology of CVDs, as spatial data tend to be dependent on each other (Pfeiffer et al., 2008), while in addition to this, disease data tend to be also geographically heterogeneous (Anselin, 2010). Since the design and implementation of intervention programmes for tackling the burden of both CVDs and all of these clinical risk factors at the whole population level may be very costly (Santos et al., 2020), recognizing specific areas of a country where these associations are more pronounced, leads to the adaptation of more effective preventive programmes at the local extent (Abuya et al., 2010). Besides, the identification by GWR of how these risk factors and their relationship with CVD incidence vary spatially, can offer crucial insights to both hospital decision making, as well as to healthcare resource allocation, as it can lead to the best possible spatial distribution of the healthcare facilities and services (Gao et al., 2021; Pan et al., 2018).
Strengths and Limitations
To the best of our knowledge, this is one of the very first studies investigating the geographical variability of the sex and age-specific 10-year CVD incidence and its risk factors, at an aggregated municipal-level, in a highly urbanised area in Europe. One of the most significant strengths of the present work is the wide range of ages of the CVD free participants included in the baseline examination and tested for developing CVD during the decade, which is considered to be of crucial importance when addressing pathobiological hypotheses concerning primary CVD prevention. Another strength of the present work is the implementation of a local statistical modelling approach via the linear GWR analysis, which can provide useful insights to policymakers and decision makers, for both designing effective prevention programmes at a local level, as well as for efficiently distributing the available healthcare resources and services in areas where the studied relationships are stronger. In particular, by recognizing the specific areas where the CVD incidence rate is higher, as well as where its association with the clinical and other risk factors is more pronounced, more effective and less costly prevention programmes can be designed and implemented, focusing on the specific needs of each area’s population. However, the conclusions should be considered under some existing limitations, such as the fact that the lifestyle and the clinical risk factors data were aggregated at the municipality level by assuming a uniform distribution, yet it should be noted that this aggregation was permitted due to the fact that the ATTICA study sample was representative of the population residing in the Athens metropolitan area. Another potential limitation of the present work is the fact that the analysis was restricted to 40 out of 58 municipalities of the Attica region, yet the studied sample is representative of the whole population residing in the Athens metropolitan area. Finally, as far as the generalizability of the present findings is concerned, since the Athens metropolitan area is the most urbanised city in Greece, their generalizability could be done for areas in other European countries with similar characteristics.
Conclusions
In conclusion, the identification of areas where the intensity of the studied associations between the risk factors and the sex and age- specific 10-year CVD incidence is stronger, can be considered a crucial methodological aspect for the design and implementation of more effective CVD prevention programs at the community level, tailored made to specific needs of men and women, separately, as well as of different age groups, as by targeting the high-risk groups and areas a widespread reduction of CVD risk can be achieved.
Data Availability
The data are available upon request. For expression of interest, please contact Prof. Demosthenes Panagiotakos (dbpanag@hua.gr).
Code Availability
None applicable.
References
Abuya, T., Amin, A., Molyneux, S., Akhwale, W., Marsh, V., & Gilson, L. (2010). Importance of strategic management in the implementation of private medicine retailer programmes: Case studies from three districts in Kenya. BMC Health Services Research, 10(Suppl 1), S7.
Alves, A. T., Nobre, F. F., & Waller, L. A. (2016). Exploring spatial patterns in the associations between local AIDS incidence and socioeconomic and demographic variables in the state of Rio de Janeiro, Brazil. Spatial and Spatio-temporal Epidemiology, 17, 85–93.
Anselin, L. (2010). Thirty years of spatial econometrics. Papers in Regional Science, 89, 3–25.
Aturinde, A., Farnaghi, M., Pilesjö, P., Sundquist, K., & Mansourian, A. (2021). Spatial analysis of ambient air pollution and cardiovascular disease (CVD) hospitalization across Sweden. GeoHealth, 5(5), e2020GH000323. https://doi.org/10.1029/2020GH000323
Backholer, K., Peters, S. A. E., Bots, S. H., Peeters, A., Huxley, R. R., & Woodward, M. (2017). Sex differences in the relationship between socioeconomic status and cardiovascular disease: A systematic review and meta-analysis. Journal of Epidemiology and Community Health, 71(6), 550–557. https://doi.org/10.1136/jech-2016-207890
Chait, A., Han, C. Y., Oram, J. F., & Heinecke, J. W. (2005). Lipoprotein-associated inflammatory proteins: Markers or mediators of cardiovascular disease. Journal of Lipid Research, 46(3), 389–403.
Dinsa, G. D., Goryakin, Y., Fumagalli, E., & Suhrcke, M. (2012). Obesity and socioeconomic status in developing countries: A systematic review. Obesity Reviews, 13(11), 1067–1079. https://doi.org/10.1111/j.1467-789X.2012.01017.x
Espelt, A., Arriola, L., Borrell, C., Larrañaga, I., Sandín, M., & Escolar-Pujolar, A. (2011). Socioeconomic position and type 2 diabetes mellitus in Europe 1999-2009: A panorama of inequalities. Current Diabetes Reviews, 7(3), 148–158. https://doi.org/10.2174/157339911795843131
Faka, A., Chalkias, C., Montano, D., et al. (2018). Association of Socio-Environmental Determinants with diabetes prevalence in the Athens metropolitan area, Greece: A spatial analysis. The Review of Diabetic Studies, 14(4), 381–389. https://doi.org/10.1900/RDS.2017.14.381
Faka, A., Chalkias, C., Georgousopoulou, E. N., Tripitsidis, A., Pitsavos, C., & Panagiotakos, D. B. (2019). Identifying determinants of obesity in Athens, Greece through global and local statistical models. Spat Spatiotemporal Epidemiol., 29, 31–41. https://doi.org/10.1016/j.sste.2019.02.002
Faka, A., Chalkias, C., Magriplis, E., et al. (2020). The influence of socio-environmental determinants on hypertension. A spatial analysis in Athens metropolitan area, Greece. Journal of Preventive Medicine and Hygiene, 61(1), E76–E84. Published 2020 Apr 2. https://doi.org/10.15167/2421-4248/jpmh2020.61.1.988
Félix-Redondo, F.J., Grau, M., Baena-Díez, J.M., et al. (2013). Prevalence of obesity and associated cardiovascular risk: The DARIOS study. BMC Public Health, 13, 542. Published 2013 Jun 5. https://doi.org/10.1186/1471-2458-13-542
Feuillet, T., Charreire, H., Menai, M., Salze, P., Simon, C., Dugas, J., et al. (2015). Spatial heterogeneity of the relationships between environmental characteristics and active commuting: Towards a locally varying social ecological model. International Journal of Health Geographics, 14(1), 1–14.
GA U. (2015). Transforming our world: the 2030 Agenda for Sustainable Development. Division for Sustainable Development Goals.
Gao, F., Guhl, M., Boukebous, B., & Deguen, S. (2021). Efficiency of fine scale and spatial regression in modelling associations between healthcare service spatial accessibility and their utilization. International Journal of Health Geographics, 20(1), 1–19.
GBD 2019 Demographics Collaborators. (2020). Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet, 396(10258), 1160–1203. https://doi.org/10.1016/S0140-6736(20)30977-6
GBD 2019 Diseases and Injuries Collaborators. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the global burden of disease study 2019. Lancet, 396(10258), 1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
Gollini, I., Lu, B., Charlton, M., Brunsdon, C., & Harris, P. (2015). GWmodel: An R package for exploring spatial heterogeneity using geographically weighted models. Journal of Statistical Software, 63(17), 1–50.
Kouvari, M., Panagiotakos, D. B., Chrysohoou, C., Georgousopoulou, E., Notara, V., Tousoulis, D., Pitsavos, C., & Investigators, A. G. S. (2019). Gender-specific, lifestyle-related factors and 10-year cardiovascular disease risk; the ATTICA and GREECS cohort studies. Current Vascular Pharmacology, 17(4), 401–410. https://doi.org/10.2174/1570161116666180608121720
Kouvari, M., Panagiotakos, D. B., Chrysohoou, C., Yannakoulia, M., Georgousopoulou, E. N., Tousoulis, D., Pitsavos, C., & ATTICA study Investigators. (2020a). Dietary vitamin D intake, cardiovascular disease and cardiometabolic risk factors: A sex-based analysis from the ATTICA cohort study. Journal of Human Nutrition and Dietetics : The Official Journal of the British Dietetic Association, 33(5), 708–717. https://doi.org/10.1111/jhn.12748
Kouvari, M., Panagiotakos, D. B., Chrysohoou, C., Notara, V., Georgousopoulou, E., Tousoulis, D., Pitsavos, C., & ATTICA & GREECS Studies Investigators. (2020b). Sex-discrete role of depressive symptomatology on 10-year first and recurrent cardiovascular disease incidence: Results from ATTICA and GREECS prospective studies. Hellenic journal of cardiology : HJC = Hellenike kardiologike epitheorese, 61(5), 321–328. https://doi.org/10.1016/j.hjc.2019.10.017
Kouvari, M., Souliotis, K., Yannakoulia, M., & Panagiotakos, D. B. (2020c). Cardiovascular diseases in women: Policies and practices around the globe to achieve gender equity in cardiac health. Risk management and healthcare policy, 13, 2079–2094. https://doi.org/10.2147/RMHP.S264672
Kouvari, M., Tsiampalis, T., Chrysohoou, C., Georgousopoulou, E., Skoumas, J., Mantzoros, C. S., Pitsavos, C. S., & Panagiotakos, D. B. (2022). Quality of plant-based diets in relation to 10-year cardiovascular disease risk: The ATTICA cohort study. European Journal of Nutrition, 61(5), 2639–2649. https://doi.org/10.1007/s00394-022-02831-0
Leng, B., Jin, Y., Li, G., Chen, L., & Jin, N. (2015). Socioeconomic status and hypertension: A meta-analysis. Journal of Hypertension, 33(2), 221–229. https://doi.org/10.1097/HJH.0000000000000428
Mackenbach, J. P., Cavelaars, A. E., Kunst, A. E., & Groenhof, F. (2000). Socioeconomic inequalities in cardiovascular disease mortality; an international study. European Heart Journal, 21(14), 1141–1151. https://doi.org/10.1053/euhj.1999.1990
Maier, W., Holle, R., Hunger, M., et al. (2013). The impact of regional deprivation and individual socio-economic status on the prevalence of type 2 diabetes in Germany. A pooled analysis of five population-based studies. Diabetic Medicine, 30(3), e78–e86. https://doi.org/10.1111/dme.12062
Matheus, A. S., Tannus, L. R., Cobas, R. A., Palma, C. C., Negrato, C. A., & Gomes, M. B. (2013). Impact of diabetes on cardiovascular disease: An update. International Journal of Hypertension, 2013, 653789. https://doi.org/10.1155/2013/653789
Neaton, J. D., & Wentworth, D. (1992). Serum cholesterol, blood pressure, cigarette smoking, and death from coronary heart disease. Overall findings and differences by age for 316,099 white men. Multiple risk factor intervention trial research group. Archives of Internal Medicine, 152(1), 56–64.
Pan, X., Kwan, M. P., Yang, L., Zhou, S., Zuo, Z., & Wan, B. (2018). Evaluating the accessibility of healthcare facilities using an integrated catchment area approach. International Journal of Environmental Research and Public Health, 15(9), 2051.
Panagiotakos, D. B., Pitsavos, C., & Stefanadis, C. (2006). Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutrition, Metabolism, and Cardiovascular Diseases, 16(8), 559–568. https://doi.org/10.1016/j.numecd.2005.08.006
Panagiotakos, D. B., Pitsavos, C., Chrysohoou, C., Skoumas, I., Stefanadis, C., & ATTICA Study. (2008). Five-year incidence of cardiovascular disease and its predictors in Greece: The ATTICA study. Vascular Medicine, 13(2), 113–121. https://doi.org/10.1177/1358863x07087731
Panagiotakos, D. B., Georgousopoulou, E. N., Pitsavos, C., et al. (2015). Ten-year (2002-2012) cardiovascular disease incidence and all-cause mortality, in urban Greek population: The ATTICA study. International Journal of Cardiology, 180, 178–184. https://doi.org/10.1016/j.ijcard.2014.11.206
Panagiotakos, D. B., Kouli, G. M., Magriplis, E., Kyrou, I., Georgousopoulou, E. N., Chrysohoou, C., Tsigos, C., Tousoulis, D., & Pitsavos, C. (2019). Beer, wine consumption, and 10-year CVD incidence: The ATTICA study. European Journal of Clinical Nutrition, 73(7), 1015–1023. https://doi.org/10.1038/s41430-018-0296-6
Papathanasiou, G., Georgoudis, G., Papandreou, M., et al. (2009). Reliability measures of the short international physical activity questionnaire (IPAQ) in Greek young adults. Hellenic Journal of Cardiology, 50(4), 283–294.
Peters, S. A., Muntner, P., & Woodward, M. (2019). Sex differences in the prevalence of, and trends in, cardiovascular risk factors, treatment, and control in the United States, 2001 to 2016. Circulation, 139(8), 1025–1035.
Pfeiffer, D. U., Robinson, T. D., Stevenson, M., Stevens, K. B., Rogers, D. J., & Clements, A. C. A. (2008). Spatial analysis in epidemiology. Oxford University Press.
Pitsavos, C., Panagiotakos, D.B., Chrysohoou, C., Stefanadis, C. (2003). Epidemiology of cardiovascular risk factors in Greece: Aims, design and baseline characteristics of the ATTICA study. BMC Public Health, 3, 32. Published 2003 Oct 20. https://doi.org/10.1186/1471-2458-3-32
Prastacos, P., Chrysoulakis, N., Kochilakis, G. (2011). Urban Atlas, land use modelling and spatial metric techniques. Proceedings of the 51st European Congress of the Regional Science Association International; Barcelona, Spain; 30 August–2 September 2011.
Prospective Studies Collaboration, Whitlock, G., Lewington, S., et al. (2009). Body-mass index and cause-specific mortality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet, 373(9669), 1083–1096. https://doi.org/10.1016/S0140-6736(09)60318-4
Psaltopoulou, T., Hatzis, G., Papageorgiou, N., Androulakis, E., Briasoulis, A., & Tousoulis, D. (2017). Socioeconomic status and risk factors for cardiovascular disease: Impact of dietary mediators. Hellenic Journal of Cardiology, 58(1), 32–42. https://doi.org/10.1016/j.hjc.2017.01.022
Rosengren, A., Subramanian, S. V., Islam, S., et al. (2009). Education and risk for acute myocardial infarction in 52 high, middle and low-income countries: INTERHEART case-control study. Heart, 95(24), 2014–2022. https://doi.org/10.1136/hrt.2009.182436
Santos, J. V., Vandenberghe, D., Lobo, M., & Freitas, A. (2020). Cost of cardiovascular disease prevention: Towards economic evaluations in prevention programs. Annals of translational medicine, 8(7), 512. https://doi.org/10.21037/atm.2020.01.20
Sarra, A. L., & Nissi, E. (2016). Geographically weighted regression analysis of cardiovascular diseases: Evidence from Canada health data. In Topics on methodological and applied statistical inference (pp. 191–203). Springer.
Schneider, H. J., Friedrich, N., Klotsche, J., et al. (2010). The predictive value of different measures of obesity for incident cardiovascular events and mortality. The Journal of Clinical Endocrinology and Metabolism, 95(4), 1777–1785. https://doi.org/10.1210/jc.2009-1584
Stringhini, S., Carmeli, C., Jokela, M., et al. (2017). Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: A multicohort study and meta-analysis of 1·7 million men and women [published correction appears in Lancet. 2017 Mar 25;389(10075):1194] [published correction appears in Lancet. 2017 Mar 25;389(10075):1194]. Lancet, 389(10075), 1229–1237. https://doi.org/10.1016/S0140-6736(16)32380-7
Suero-Abreu, G. A., Barajas-Ochoa, A., Perez-Peralta, A., Rojas, E., & Berkowitz, R. (2020). Assessment of the effect of the go red for women campaign on search engine queries for cardiovascular disease in women. Cardiology research, 11(5), 348–352. https://doi.org/10.14740/cr1107
Tabb, L. P., McClure, L. A., Ortiz, A., Melly, S., Jones, M. R., Kershaw, K. N., & Roux, A. V. D. (2020). Assessing the spatial heterogeneity in black-white differences in optimal cardiovascular health and the impact of individual-and neighborhood-level risk factors: The multi-ethnic study of atherosclerosis (MESA). Spatial and spatio-temporal epidemiology., 33, 100332.
Timmis, A., Townsend, N., Gale, C., et al. (2018). European Society of Cardiology: Cardiovascular disease statistics 2017. European Heart Journal, 39(7), 508–579. https://doi.org/10.1093/eurheartj/ehx628
Tsiampalis, T., Panagiotakos, D. B. (2020). Missing-data analysis: Socio- demographic, clinical and lifestyle determinants of low response rate on self- reported psychological and nutrition related multi- item instruments in the context of the ATTICA epidemiological study. BMC Medical Research Methodology, 20(1), 148. Published 2020 Jun 8. https://doi.org/10.1186/s12874-020-01038-3
Tsiampalis, T., Faka, A., Kouvari, M., et al. (2020). The impact of socioeconomic and environmental determinants on Mediterranean diet adherence: A municipal-level spatial analysis in Athens metropolitan area, Greece [published online ahead of print, 2020 Jul 12]. International Journal of Food Sciences and Nutrition, 1–12. https://doi.org/10.1080/09637486.2020.1791057
Tsiampalis, T., Vassou, C., Psaltopoulou, T., & Panagiotakos, D. B. (2021a). Socio-demographic, clinical and lifestyle determinants of low response rate on a self-reported psychological multi-item instrument assessing the adults’ hostility and its direction: ATTICA epidemiological study (2002-2012). International Journal of Statistics in Medical Research, 10, 1–9.
Tsiampalis, T., Faka, A., Kouvari, M., Psaltopoulou, T., Pitsavos, C., Chalkias, C. & Panagiotakos, D.B. (2021b). Geographical variability of sex-specific, health related determinants of quality of life in Athens metropolitan area: A spatial analysis in the context of the ATTICA epidemiological study. Applied Spatial Analysis and Policy, 1–21.
United Nations Educational Scientific and Cultural Organization Institute for Statistics (2012). International Standard Classification of Education ISCED 2011.
Wolinsky, H. (2006). The battle of Helsinki: Two troublesome paragraphs in the declaration of Helsinki are causing a furore over medical research ethics. EMBO reports, 7(7), 670–672. https://doi.org/10.1038/sj.embor.7400743
World Health Organization. (2000). Obesity: Preventing and managing the global epidemic.
Acknowledgements
The authors would like to thank the ATTICA study group of investigators: Christina Chrysohoou, Yannis Skoumas, Natasa Katinioti, Labros Papadimitriou, Constantina Masoura, Spiros Vellas, Yannis Lentzas, Manolis Kambaxis, Konstanitna Paliou, Vassiliki Metaxa, Ekavi Georgousopoulou, Agathi Ntzouvani, Dimitris Mpougatas, Nikolaos Skourlis, Christina Papanikolaou, Aikaterini Kalogeropoulou, Evangelia Pitaraki, Alexandros Laskaris, Mihail Hatzigeorgiou, Athanasios Grekas, and Eleni Kokkou for assistance in the initial physical examination and/or the follow-up evaluation; Efi Tsetsekou for her assistance in psychological evaluation and follow-up evaluation, as well as the laboratory team: Carmen Vassiliadou and George Dedousis (genetic analysis), Marina Toutouza-Giotsa, Constantina Tselika and Sia Poulopoulou (biochemical analysis) and Maria Toutouza for the database management. We would also like to thank all the individuals participated in the ATTICA study.
Funding
Open access funding provided by HEAL-Link Greece. The ATTICA study is supported by research grants from the Hellenic Cardiology Society [HCS2002] and the Hellenic Atherosclerosis Society [HAS2003].
Author information
Authors and Affiliations
Contributions
TT wrote the manuscript (interpretation of the results and discussion) and performed the statistical analysis. AF, TP, CC and CP contributed to the interpretation of the results and discussion. DBP and CP were responsible for the study’s design and implementation and critically reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics Approval
ATTICA study was approved by the Bioethics Committee of Athens Medical School. The study was carried out in accordance with the Declaration of Wolinsky (2006) of the World Medical Association.
Consent to Participate
All participants were informed about the study aims and procedures and provided written informed consent.
Consent for Publication
Non applicable.
Conflicts of Interest/Competing Interests
All authors declare no conflicts of interest related to this research work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tsiampalis, T., Faka, A., Psaltopoulou, T. et al. The Spatial Variability of the Sex and Age- Specific 10-Year Incidence of Cardiovascular Diseases and its Clinical Risk Factors in Athens Metropolitan Area: a Local Statistical Modelling Approach in the Context of the ATTICA Epidemiological Study. Appl. Spatial Analysis 16, 939–965 (2023). https://doi.org/10.1007/s12061-023-09508-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12061-023-09508-z