
Abstract
In patients undergoing open-heart surgery, abnormalities in thyroid hormone levels have been observed even in the absence of primary thyroid disease. These abnormal changes in thyroid hormone level and function have been found to be sufficient to affect myocardial performance and postoperative recovery. In the intensive care unit, postoperatively, it has been found that features such as low cardiac output, left ventricular dysfunction and prolonged ventilator support were associated with hypothyroidism. We reviewed the available literature on the effect of thyroid hormone supplementation in paediatric patients undergoing open-heart surgery under cardiopulmonary bypass and concluded that children after complex congenital cardiac surgery are at risk of developing a clinically significant hypothyroid state in the early postoperative period. In the literature where the effects of supplementation of thyroxine were studied, beneficial effects were observed in terms of reduced mechanical ventilation time, reduced inotropic support and intensive care unit stay, rapid achievement of negative fluid balance and early recovery. Supplementation with thyroid hormones enables a smoother postoperative recovery and is beneficial. The total duration of this therapy is, however, unclear.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Thyroid hormones are known to be the key regulators of metabolism. Thyroxine (T4) and triiodothyronine (T3) are both produced by the thyroid gland. T4 is the main product and is converted in the periphery by deiodination to T3 which is the main biologically active thyroid hormone. During hyperthyroidism, a high cardiac output state exists secondary to increased heart rate and contractility along with a reduction in systemic vascular resistance and reciprocal effects are observed during hypothyroidism. We therefore reviewed the available literature on the effect of thyroid hormone supplementation in paediatric patients undergoing open-heart surgery for congenital heart defects and elucidate some pertinent observations.
Review method
We performed an exhaustive PubMed interface and Google database search in the time frame between January 1996 and October 2013 for all papers that addressed the issue of thyroid hormones in post-cardiotomy paediatric patients in the English literature. The reference lists of each publication were searched. Papers discussing this issue in adults or patients undergoing non-cardiac surgery were excluded. We specifically aimed to address if the thyroid hormone supplementation has the potential to improve myocardial performance in the form of optimal heart rate, systolic blood pressure, cardiac output, less inotropic support, less intensive care unit (ICU) stay and hospital stay. Sixteen papers were found using the reported search. Out of these, seven papers provided the best evidence to form this review (Table 1).
Effects of thyroid hormones
Children with hypothyroidism may present with dyspnea, pedal oedema and pleural effusions suggestive of heart failure. These symptoms can be explained due to decreased heart rate, reduced ventricular filling and decrease in myocardial contractility. These children are also at increased risk of ventricular arrhythmias due to prolonged cardiac action potential. Supplementation with thyroid hormones can lead to reversal of these cardiovascular symptoms [1–3]. On the other hand, tachycardia and rhythm disturbances are the most common cardiac manifestations noticed in children with hyperthyroidism. Supranormal cardiac output noticed in these patients can be related to the increase in heart rate, left ventricular contractility and reduction in systemic vascular resistance.
Precipitous decline in circulating concentrations of T3, T4 and thyroid-stimulating hormone (TSH) occurs during severe physiological stress conditions like cardiac surgery. Euthyroid sick syndrome is an adaptive response to keep to a minimum metabolic demand during the stress of cardiac surgery and has also been referred to as the non-thyroidal illness syndrome (NTIS) [4, 5]. These reductions were previously attributed to the haemodilution following the institution of cardiopulmonary bypass (CPB). However, recent studies have revealed similar reductions in thyroid hormone levels in patients who underwent cardiac surgery without utilizing CPB support. This implies that NTIS during cardiac surgery is a non-specific stress response and CPB is not the only contributing factor to its occurrence [2, 3, 6]. This NTIS does require thyroid hormone replacement therapy in view of the presence of transient hypothyroidism. Reduction in concentrations of free T3 (fT3) in hospitalized patients has been demonstrated to be predictive of mortality [7]. Suppression of thyroid function after cardiac surgery although transient is well documented. However, the need for therapeutic intervention is not yet strongly recommended [8]. The use of thyroxine is hypothesized to improve the postoperative course of children suffering from cardiac failure following open-heart surgery. It has been documented earlier that thyroid hormone concentrations fall in the immediate postoperative period [9]. Triiodothyronine is hypothesized to improve the cardiac performance by nuclear binding or extranuclear binding [10]. Acute inotropic effects of triiodothyronine are achieved without oxygen wasting and without an increase of protein catabolism. It also potentiates the cardiovascular effects of catecholamines administered after cardiac surgery [11].
Results of supplementation
Most of the published literature support thyroid hormone supplementation in the early postoperative period following congenital cardiac surgery.
Bettendorf et al. [1] studied 132 children with a median age of 2 days to 16 years (90 children were below 6 years, 48 patients were below 1 year of age) undergoing open-heart surgery and assessed plasma thyroid-stimulating hormone (TSH), thyroxine (T4), free thyroxine (fT4), triiodothyronine (T3) and thyroglobulin (Tg). Preoperative plasma thyroid hormone concentrations and urinary iodine excretion were compared with the maximal postoperative change and with the maximal change during recovery thereafter. They found a significantly low plasma concentration of these hormones, starting from day 1 with minimum levels on day 2 when patients did not receive dopamine and on day 3 when they received dopamine. They showed that this transient secondary hypothyroidism, particularly when T3 concentration was less than 0.6 nmol/l (n = 52), was associated with prolonged mechanical ventilation, more inotropic support and ICU stay. Urinary iodine excretion increased by 370 % after CPB and peaked at 1 day postoperatively. Subsequently, urinary iodine excretion decreased but was still elevated 5 days after surgery. A weak negative correlation was found between maximal postoperative urinary iodine excretion and lowest postoperative plasma concentrations of T3. These changes occurred irrespective of patient’s age, gender and cardiac malformations. This is the first study in paediatric age group that provided evidence that thyroid dysfunction may affect the early postoperative period and change the overall outcome.
Chowdhury et al. [12] evaluated 28 patients (age 1 to 18 years), undergoing cardiac surgery, where serum total T3 level was less than 40 ng/dl (or <60 ng/dl in newborns) on postoperative days 0–2). Out of these, 14 patients were randomized to T3 treatment and 14 patients were controls. They found that T3 levels decreased in all patients with a maximum fall at 24 to 48 h but did not find a significant relation between T3 levels and postoperative outcome (ionotropic score and therapeutic interventional scoring system (TISS)), but when compared with neonates (age <1 month), this TISS score and inotropic score were significantly less in patients who were treated with T3 infusion. The duration of mechanical ventilation and hospital stay was shorter in neonates who were treated with T3.
Portman et al. [13] performed a randomized multicenter randomized trial in patients (<2 years) with perimembranous ventricular septal defect and tetralogy of Fallot and divided them into two groups: one received T3 (before CPB initiation and second dose after clamp release) and another did not receive any T3. They observed an increase in heart rate and peak pressure-rate product in patients who received T3, while the control group did not show any increase in heart rate, systolic and diastolic blood pressure and peak pressure-rate product. They suggested that because cross-clamp time was relatively short in these special group of patients (ventricular septal defect and tetralogy of Fallot), further study is needed to define the haemodynamic impact of T3 repletion.
Bettendorf et al. [9] performed a randomized double-blind placebo-controlled trial in 40 patients (age 2 days to 10 years) dividing them into two groups: one received the T3 supplementation in the postoperative period and one received placebo. Primary measures were the thyroid hormone concentrations and the echocardiographic variables of left ventricular function. Secondary measures were the intervention scoring system, the postoperative inotropic support with catecholamines and diuretics, the postoperative need for mechanical ventilation and oxygen supplementation, and the time spent in the hospital. In both groups, plasma triiodothyronine concentrations were greatly decreased after surgery and rose after T3 infusion in the treatment group. Plasma concentrations of thyrotropin were equally suppressed in all patients after cardiac surgery. The mean therapeutic intervention score was equally raised in the triiodothyronine and placebo groups just after surgery. An important finding of the study was that systolic cardiac function (measured by echocardiography) and cardiac index were improved in most patients who received T3. They concluded that treatment with T3 improves the myocardial function and reduces the need of postoperative intensive care.
Carrel et al. [14] studied seven patients (age <1 year), with complex congenital heart disease, who had severe low cardiac output in the postoperative period characterized by mean arterial pressure <40 mmHg, central venous pressure >18 mmHg, urine output <1 ml/kg, base excess >−10, high inotropic support (including milrinone) and nitric oxide ventilation. Before T3 supplementation, the level of T3 was <60 ng/dl in neonates and <40 mg/dl in infants. All these patients received a bolus dose of T3 followed by continuous infusion for the next 24–48 h. Although two patients did not survive, remaining five recovered fully. These results showed the impact of T3 supplementation in such complex congenital cardiac diseases after surgery.
Mackie et al. [15], in their double-blind, randomized placebo-controlled trial of 42 patients who underwent surgery for complex congenital cardiac lesions, showed results of T3 supplementation. Primary end points were composite clinical outcome score, derived through consensus by experts in paediatric cardiac intensive care; (a) time until negative fluid balance first achieved, (b) time until sternal closure and (c) time until first extubation; and cardiac index. Secondary end points included serum lactate level at 12, 24 and 48 h; serious adverse events; and inotropic score. Total and free T3 levels were significantly higher in the T3 supplement group. They showed favourable composite clinical outcome scores in the early postoperative period as a rapid achievement of a negative fluid balance. They also observed a shorter ICU stay and hospital stay, but these were not significant. They concluded that T3 supplementation is safe and resulted in more rapid achievement of negative fluid balance and early recovery.
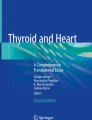
Talwar et al. [16] studied 100 consecutive patients (age 15.9 ± 14.6 months) who underwent open-heart surgery for congenital cardiac lesions and found a significant inverse relationship of total T4 with inotropic score and duration of mechanical ventilation. They assessed the free T4, total T4 (TT4), free T3, total T3 and TSH at baseline and at 1, 24, 48 and 72 h of cardiac surgery and found a significant fall (29.1 % for FT4, 32.1 % for TT4, 77 % for TSH, 46 % for FT3 and 45 % for T3; P < 0.0001) in thyroid hormones. Patient who survived had a high total T4 level compared to non-survivors. When the area under the curve (AUC) for postoperative TT4 was compared between survivors (n = 87) and non-survivors (n = 12), a significantly larger AUC was seen in survivors (492.81 ± 158.6; confidence interval (CI) = 459.01–526.60) than non-survivors (360.75 ± 179.6; CI = 246.59–474.9; P = 0.0125; Fig. 1). AUC TT4 was significantly larger in those who had an uneventful postoperative course in comparison with those who had postoperative complications (516.48 ± 18.6 vs. 394.78 ± 29.9, P = 0.001). AUC TT4 showed a significant inverse correlation with inotropic score (r 2 = −0.06, P = 0.014; Fig. 2) and a borderline inverse correlation with duration of mechanical ventilation (r 2 = −0.03, P = 0.08; Fig. 3).

Area under the curve for TT4 between survivors and non-survivors. The length of the whiskers refers to 1.5 times the width of the inter-quartile range from the median (reproduced with permission from [16])

Area under the curve of TT4 is co-related with the inotropic score (reproduced with permission from [16])

Area under the curve of TT4 is co-related with duration of mechanical ventilation (in hours) (reproduced with permission from [16])
A detailed analysis of the above studies, however, does not shed any light on the optimal dosage, duration and route of administration of the thyroid hormones, and current research including that of the authors is directed in this area. In the Western countries, injectable preparations of T3 are used; however, this is not available in India. At the authors’ institution, a double-blind randomized trial using oral thyroxine preparations in the postoperative period while the patient is in the ICU is in progress and results are expected soon.
Conclusion
Children after complex congenital cardiac surgery are at a specific risk of developing a clinically significant hypothyroid state in the early postoperative period. Supplementation with thyroid hormones enables smoother postoperative recovery and is beneficial. The total duration of this therapy is, however, unclear.
References
Bettendorf M, Schmidt KG, Tiefenbacher U, Grulich-Henn J, Heinrich UE, Schönberg DK. Transient secondary hypothyroidism in children after cardiac surgery. Pediatr Res. 1997;41:375–9.
Faber J, Petersen L, Wiinberg N, Schifter S, Mehlsen J. Hemodynamic changes after levothyroxine treatment in subclinical hypothyroidism. Thyroid. 2002;12:319–24.
Velissaris T, Tang AT, Wood PJ, Hett DA, Ohri SK. Thyroid function during coronary surgery with and without cardiopulmonary bypass. Eur J Cardiothorac Surg. 2009;36:148–54.
De Groot LJ. Dangerous dogmas in medicine: the nonthyroidal illness syndrome. J Clin Endocrinol Metab. 1999;84:151–64.
Chopra IJ. Euthyroid sick syndrome: is it a misnomer? J Clin Endocrinol Metab. 1997;82:329–34.
Osman F, Gammage MD, Franklyn JA. Hyperthyroidism and cardiovascular morbidity and mortality. Thyroid. 2002;12:483–7.
Iglesias P, Munoz A, Prado F, et al. Alterations in thyroid function tests in aged hospitalized patients: prevalence, aetiology and clinical outcome. Clin Endocrinol (Oxf). 2009;70:961–7.
Utiger RD. Altered thyroid function in nonthyroidal illness and surgery: to treat or not to treat? N Engl J Med. 1995;333:1562–63.
Bettendorf M, Schmidt KG, Grulich-Henn J, Ulmer HE, Heinrich UE. Tri-iodothyronine treatment in children after cardiac surgery: a double-blind, randomised, placebo-controlled study. Lancet. 2000;356:529–34.
Klein I. Thyroid hormone and the cardiovascular system. Am J Med. 1990;88:631–37.
Bilezikian JP, Loeb JN. The influence of hyperthyroidism and hypothyroidism on alpha- and beta-adrenergic receptor systems and adrenergic responsiveness. Endocr Rev. 1983;4:378–88.
Chowdhury D, Ojamaa K, Parnell VA, McMahon C, Sison CP, Klein I. A prospective randomized clinical study of thyroid hormone treatment after operations for complex congenital heart disease. J Thorac Cardiovasc Surg. 2001;122:1023–5.
Portman MA, Fearneyhough C, Karl TR, et al. The Triiodothyronine for Infants and Children Undergoing Cardiopulmonary Bypass (TRICC) study: design and rationale. Am Heart J. 2004;148:393–8.
Carrel T, Eckstein F, Englberger L, Mury R, Mohacsi P. Thyronin treatment in adult and pediatric heart surgery: clinical experience and review of the literature. Eur J Heart Fail. 2002;4:577–82.
Mackie AS, Booth KL, Newburger JW, et al. A randomized, double-blind, placebo-controlled pilot trial of triiodothyronine in neonatal heart surgery. J Thorac Cardiovasc Surg. 2005;130:810–6.
Talwar S, Khadgawat R, Sandeep JA, et al. Cardiopulmonary bypass and serum thyroid hormone profile in pediatric patients with congenital heart disease. Congenit Heart Dis. 2012;7:433–40.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that they have no conflict of interest and do not receive any research grants from any company, have not received a speaker honorarium from any company, do not own any stock in any company and are not members of a committee.
Funding
The study did not receive any funding.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Talwar, S., Kumar, M.V., Choudhary, S.K. et al. Thyroid hormone supplementation following open-heart surgery in children. Indian J Thorac Cardiovasc Surg 32, 17–22 (2016). https://doi.org/10.1007/s12055-015-0411-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12055-015-0411-4