
Abstract
Background
A newly emerging approach “caudal to cranial” with complete mesenteric excision (CME) has recently been proposed for right colectomy in patients with right colon cancer. To date, only a few studies about this approach have appeared. Our study aims to investigate the safety and efficacy of this new technique.
Methods
A systematic review of the literature was conducted to evaluate the evidence regarding short- and long-term outcomes after the caudal-to-cranial approach (CCA). Methodological Index for Non-Randomized Studies was used to evaluate methodological quality. The risk of bias was assessed using Robvis tool. Meta-analyses have been conducted for the outcomes of studies comparing CCA with other techniques.
Results
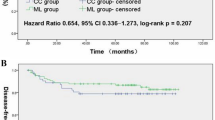
We found six studies from 2017 to 2021 with a total of 594 patients. The postoperative complications and oncological outcomes were acceptable. Two studies comparing CCA to medial-to-lateral approach were included in the meta-analysis. No differences were found between the techniques regarding to operative time, length of hospital stay, overall morbidity, and number of lymph nodes.
Conclusion
Although the interpretation of our findings may be restrained by methodological limitations, risk of bias, and the absence of well-designed randomized controlled trials, CCA with CME in right-sided colon cancer may be a feasible and safe procedure.





Similar content being viewed by others


Data Availability
The data that support the findings of this study are available from the corresponding author, [MM], upon reasonable request.
References
Zou L-N, Lu X-Q, Wan J. Techniques and feasibility of the caudal-to-cranial approach for laparoscopic right colectomy with complete mesenteric excision. Dis Colon Rectum. 2017;60(4):e23–4.
Li H, He Y, Lin Z, Xiong W, Diao D, Wang W, et al. Laparoscopic caudal-to-cranial approach for radical lymph node dissection in right hemicolectomy. Langenbecks Arch Surg. 2016;401(5):741–6.
Ding J, Liao G-q, Xia Y, Zhang Z-M, Pan Y, Liu S, et al. Medial versus lateral approach in laparoscopic colorectal resection: a systematic review and meta-analysis. World J Surg. 2013;37(4):863–72.
Zou L, Xiong W, Li H, He Y, Diao D, Zheng Y, et al. Efficacy analysis of laparoscopic radical right hemicolectomy using caudal-to-cranial approach. Zhonghua wei chang wai ke za zhi= Chin J Gastrointes Surg. 2015;18(11):1124–7.
Wang Y, Zhang C, Zhang D, Fu Z, Sun Y. Clinical outcome of laparoscopic complete mesocolic excision in the treatment of right colon cancer. World J Surg Oncol. 2017;15(1):174.
Petz W, Ribero D, Bertani E, Borin S, Formisano G, Esposito S, et al. Suprapubic approach for robotic complete mesocolic excision in right colectomy: oncologic safety and short-term outcomes of an original technique. Eur J Surg Oncol. 2017;43(11):2060–6.
Miyo M, Takemasa I, Ishihara H, Hata T, Mizushima T, Ohno Y, et al. Long-term outcomes of single-site laparoscopic colectomy with complete mesocolic excision for colon cancer: comparison with conventional multiport laparoscopic colectomy using propensity score matching. Dis Colon Rectum. 2017;60(7):664–73.
Killeen S, Mannion M, Devaney A, Winter D. Complete mesocolic resection and extended lymphadenectomy for colon cancer: a systematic review. Colorectal Dis. 2014;16(8):577–94.
Chaouch MA, Dougaz MW, Bouasker I, Jerraya H, Ghariani W, Khalfallah M, et al. Laparoscopic versus open complete mesocolon excision in right colon cancer: a systematic review and meta-analysis. World J Surg. 2019;43(12):3179–90.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions: John Wiley & Sons; 2019.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–6.
McGuinness L, Higgins J. Risk-of-bias VISualization (robvis): an R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods. 2021;12(1):55–61.
Zou L, Xiong W, Li H, He Y, Diao D, Zheng Y, et al. [Efficacy analysis of laparoscopic radical right hemicolectomy using caudal-to-cranial approach]. Zhonghua wei chang wai ke za zhi = Chin J Gastrointes Surg. 2015;18(11):1124–7.
Chen Q, Shuai X, Chen L. Safety and feasibility of the combined medial and caudal approach in laparoscopic D3 lymphadenectomy plus complete mesocolic excision for right hemicolectomy in the treatment of right hemicolon cancer complicated with incomplete ileus. Zhonghua Wei Chang Wai ke za Zhi = Chinese J Gastrointest Surg. 2018;21(9):1039–44.
Spinoglio G, Petz W, Borin S, Piccioli AN, Bertani E. Robotic right colectomy with complete mesocolic excision and indocyanine green guidance. Minerva Chir. 2019;74(2):165–9.
Zou L, Xiong W, Mo D, He Y, Li H, Tan P, et al. Laparoscopic radical extended right hemicolectomy using a caudal-to-cranial approach. Ann Surg Oncol. 2016;23(8):2562–3.
Schulte am Esch J, Iosivan S-I, Steinfurth F, Mahdi A, Förster C, Wilkens L, et al. A standardized suprapubic bottom-to-up approach in robotic right colectomy: technical and oncological advances for complete mesocolic excision (CME). BMC Surgery. 2019;19(1):72.
Yi X, Li H, Lu X, Wan J, Diao D. “Caudal-to-cranial” plus “artery first” technique with beyond D3 lymph node dissection on the right midline of the superior mesenteric artery for the treatment of right colon cancer: is it more in line with the principle of oncology? Surgical Endoscopy. 2019:1–12.
Tokuhara K, Yoshida T, Matsui Y, Yoshioka K, Sekimoto M. Laparoscopy-assisted right hemicolectomy with the bottom-to-up approach for right-side colon cancer. Indian J Surg. 2021;83(5):1178–84.
Ksantini R, Bedoui H, Ayadi S, Fterich F, Makni A, Bouchiba N, et al. Laparoscopic ileocecal resection for Crohn’s disease. Tunis Med. 2007;85(5):376–9.
Chebbi F, Ayadi MS, Rhaiem R, Daghfous A, Makni A, Rebaϊ W, et al. Laparoscopic ileo-cecal resection: the total retro-mesenteric approach. Surg Endosc. 2015;29(1):245–51.
Feng B, Ling T-L, Lu A-G, Wang M-L, Ma J-J, Li J-W, et al. Completely medial versus hybrid medial approach for laparoscopic complete mesocolic excision in right hemicolon cancer. Surg Endosc. 2014;28(2):477–83.
Rotholtz NA, Bun ME, Tessio M, Lencinas SM, Laporte M, Aued ML, et al. Laparoscopic colectomy: medial versus lateral approach. Surg Laparosc Endosc Percutan Tech. 2009;19(1):43–7.
Yan J, Ying M, Zhou D, Chen X, Chen L, Ye W, et al. A prospective randomized control trial of the approach for laparoscopic right hemi-colectomy: medial-to-lateral versus lateral-to-medial. Zhonghua Wei Chang Wai Ke Za Zhi = Chinese J Gastrointest Surg. 2010;13(6):403–5.
Author information
Authors and Affiliations
Contributions
Writing—original draft: Maatouk M, Hamdi Kbir G. Conceptualization: Ben Safta Y, Haouet K. Formal analysis: Mabrouk A, Ben Dhaou A. Review and editing: Ben Moussa M.
Corresponding author
Ethics declarations
Ethics Approval
No ethical approval is required as this research project is a systematic review of previous studies.
Conflict of Interest
The authors declare no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Maatouk, M., Safta, Y.B., Kbir, G.H. et al. Caudal-to-Cranial Approach for Right Colectomy with Complete Mesocolic Excision in Colon Cancer: A Systematic Review and Meta-analysis. J Gastrointest Canc 54, 739–750 (2023). https://doi.org/10.1007/s12029-022-00894-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-022-00894-0