
Abstract
Purpose
In this study, we aim to report the efficacy of using the anterior approach (AA) versus the conventional approach (CA), in surgical resection for large hepatocellular carcinoma (HCC) (≥7 cm) of the right hepatic lobe in terms of surgical and long-term outcomes.
Materials and Methods
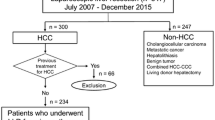
Between 2000 and 2006, 138 consecutive patients who underwent hepatic resection with curative intent for large right lobe HCC ≥7 cm were identified from a retrospective database. The 40 patients who had AA were compared with the remaining 98 patients who had CA. Clinicopathological features and surgical results were analyzed and prognostic factors were evaluated by multivariate analysis.
Results
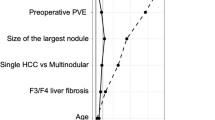
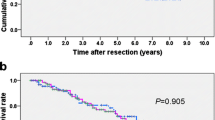
There was no significant difference between the two groups as regards clinical, laboratory, and pathological parameters. The operative results had shown a comparable proportion of patients who experienced massive operative blood loss and postoperative complications in the two groups. The AA group had a lower recurrence rate (P = 0·015), better disease-free survival (DFS) (P = 0·001), and overall survival than the CA group. Our study identified that AA is a prognostic factor of both overall survival and disease-free survival for large HCC ≥7 cm.
Conclusion
The AA is a safe and effective technique for right hepatic resection for large HCC and achieves more advantageous long survival outcome over the CA.

Similar content being viewed by others
References
Sherman M. Hepatocellular carcinoma: epidemiology, risk factors, and screening. Semin Liver Dis. 2005;25:143–54.
Zhou WP, Lai EC, Li AJ, Fu SY, Zhou JP, Pan ZY, et al. A prospective, randomized, controlled trial of preoperative transarterial chemoembolization for resectable large hepatocellular carcinoma. Ann Surg. 2009;249:195–202.
Fan N, Yang G-S, Lu J-H, Yang N. Classification of right hepatectomy for special localized malignant tumor in right liver lobe. World J Gastroenterol. 2005;11(28):4321–5.
Lortat-Jacob JL, Robert HG. Well defined technique for right hepatectomy. Presse Med. 1952;60:549–51.
Belghiti J, Dugue L. Technique for right hepatectomy. J Chir. 1998;135:19–22.
Lai EC, Fan ST, Lo CM, Chu KM, Liu CL. Anterior approach for difficult major right hepatectomy. World J Surg. 1996;20:314–7.
Liu CL, Fan ST, Lo CM, Tung-Ping Poon R, Wong J. Anterior approach for major right hepatic resection for large hepatocellular carcinoma. Ann Surg. 2000;232:25–31.
Liu CL, Fan ST, Cheung ST, Lo CM, Ng IO, Wong J. Anterior approach versus conventional approach right hepatic resection for large hepatocellular carcinoma: a prospective randomized controlled study. Ann Surg. 2006;244:194–203.
Ishizawa T, Kokudo N, Masatoshi MM. Right hepatectomy for hepatocellular carcinoma: is the anterior approach superior to the conventional approach? Ann Surg. 2008;247:391–2.
Capussotti L, Polastri R. Operative risks of major hepatic resections. Hepato-Gastroenterology. 1998;45:184–90.
Tsai TJ, Chau GY, Lui WY, Tsay SH, King KL, Loong CC, et al. Clinical significance of microscopic tumor venous invasion in patients with resectable hepatocellular carcinoma. Surgery. 2000;127:603–8.
Li L, Wang HQ, Wang Q, Yang J, Yang JY. Anterior vs conventional approach hepatectomy for large liver cancer: a meta-analysis. World J Gastroenterol. 2014;20(45):17235–43.
The Liver Cancer Study Group of Japan. The general results for the clinical and pathological study of primary liver cancer. 5th ed. Tokyo: Kanehara Shuppan; 2009.
Louha M, Nicolet J, Zylberberg H, Sabile A, Vons C, Vona G, et al. Liver resection and needle liver biopsy cause hematogenous dissemination of liver cells. Hepatology. 1999;29:879–82.
Ikai I, Arii S, Kojiro M, Ichida T, Makuuchi M, Matsuyama Y, et al. Reevaluation of prognostic factors for survival after liver resection in patients with hepatocellular carcinoma in a Japanese nationwide survey. Cancer. 2004;101:796–802.
Vauthey JN, Pawlik TM, Lauwers GY, Regimbeau JM, Belghiti J, Ikai I, et al. Is hepatic resection for large or multinodular hepatocellular carcinoma justified? Results from a multiinstitutional database. Ann Surg Oncol. 2005;12:364–73.
Poon RT, Fan ST, Lo CM, Ng IO, Liu CL, Lam CM, et al. Improving survival results after resection of hepatocellular carcinoma: a prospective study of 377 patients over 10 years. Ann Surg. 2001;234:63–70.
Ozawa K. Hepatic function and liver resection. J Gasteroenterol Hepatol. 1990;5:296.
DeMatteo RP, Fong Y, Jarnagin WR, Blumgart LH. Recent advances in hepatic resection. Semin Surg Oncol. 2000;19:200–7.
Wu TJ, Wang F, Lin YS, Chan KM, Yu MC, Lee WC. Right hepatectomy by the anterior method with liver hanging versus conventional approach for large hepatocellular carcinomas. Br J Surg. 2010;97:1070–8.
Yang J, Li C, Wen TF, Yan LN, Li B, Wang WT, et al. Is hepatectomy for huge hepatocellular carcinoma (≥10cmin diameter) safe and effective? A single-center experience. Asian Pac J Cancer Prev. 2014;15(17):7069–77.
Hasegawa K, Kokudo N, Imamura H, Matsuyama Y, Aoki T, Minagawa M, et al. Prognostic impact of anatomic resection for hepatocellular carcinoma. Ann Surg. 2005;242:2529.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Jabir, M.A., Hamza, H.M., Fakhry, H. et al. Anterior Versus Conventional Approach for Resection of Large Right Lobe Hepatocellular Carcinoma. J Gastrointest Canc 48, 25–30 (2017). https://doi.org/10.1007/s12029-016-9865-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-016-9865-x