
Abstract
Background
We investigated whether early electroencephalographic features predicted intracranial pressure (ICP), cerebrovascular pressure reactivity, brain tissue oxygenation, and functional outcomes in patients with pediatric traumatic brain injury (TBI).
Methods
This was a retrospective analysis of a prospective data set of 63 patients with pediatric TBI. Electroencephalographic features were collected in the first 24 h of recording to predict values of ICP, pressure reactivity index (PRx), and brain tissue oxygenation (PbtO2) through the initial 7 days of critical care monitoring, in addition to Glasgow Outcome Scale Extended–Pediatric Revision (GOSE-Peds) scores at 12 months. Electroencephalographic features were averaged over all surface electrodes and included seizures, interictal epileptiform discharges, suppression percentage, complexity, the alpha/delta power ratio, and both absolute asymmetry indices and power in beta (13–20 Hz), alpha (8–13 Hz), theta (4–7 Hz) and delta (0–4 Hz) bands. Demographic data and injury severity scores, such as the Glasgow Coma Scale (GCS) and Pediatric Risk of Mortality III (PRISM III) scores, at presentation were also assessed. Univariate and multiple linear regression with guided stepwise variable selection was used to find combinations of risk factors that best explain variability in ICP, PRx, PbtO2, and GOSE-Peds values, and best fit models were applied to pediatric age strata. We hypothesized that suppression percentage and the alpha/delta power ratio in the first 24 h of recording predict ICP, PRx, PbtO2, and GOSE-Peds values.
Results
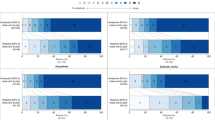
Best subset model selection identified that increased suppression percentage and PRISM III scores predicted increased ICP (R2 = 79%, Akaike information criterion [AIC] = 332.30, root mean square error [RMSE] = 6.62), with suppression percentages < 5% (slope = − 5687.0, p = 0.0001) and ≥ 45% (slope = 9825.9, p = 0.0000) being predictive of dose of intracranial hypertension. When accounting for age and GCS score, increased suppression percentage predicted increased PRx values, suggestive of inefficient cerebrovascular pressure reactivity (R2 = 53%, AIC = 3.93, RMSE = 0.23), with suppression percentages ≥ 5% (p = 0.0033) and ≥ 45% (p = 0.0027) being predictive of median PRx values ≥ 0.3. Lower GCS scores, the presence of seizures, and increased suppression percentages each were independently associated with higher GOSE-Peds scores (R2 = 52%, AIC = 194.04, RMSE = 1.58), suggestive of unfavorable outcomes, with suppression percentages ≥ 5% (p = 0.0005) and ≥ 45% (p = 0.0000) being predictive of GOSE-Peds scores ≥ 5. At the univariate level, no electroencephalographic or clinical feature was associated with differences in PbtO2 values.
Conclusions
Increased electroencephalographic suppression percentage on the initial day of monitoring may identify patients with pediatric TBI at risk of increased ICP, inefficient cerebrovascular pressure reactivity, and unfavorable outcomes.


Similar content being viewed by others


References
Maas AIR, Menon DK, Adelson PD, Andelic N, et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017;16:987–1048.
Hawey CA, Ward AB, Long J, Owen DW, et al. Prevalence of traumatic brain injury amongst children admitted to hospital in one health district: a population-based study. Injury. 2003;354:256–60.
Appavu B, Temkit M, Foldes S, Burrows BT, et al. Association of outcomes with model-based indices of cerebral autoregulation after pediatric traumatic brain injury. Neurocrit Care. 2021;35(3):340–650.
Appavu B, Riviello JJ. Electroencephalographic patterns in neurocritical care: pathologic contributors or epiphenomena? Neurocrit Care. 2018;29(1):9–19.
Sansevere AJ, Hahn CD, Abend NS. Conventional and quantitative EEG in status epilepticus. Seizure. 2019;68:38–45.
Kochanek PM, Tasker RC, Carney N, Totten AM, et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017;16:987–1048.
Kochanek PM, Carney N, Adelson PD, Ashwal S, et al. Guidelines for the acute management of severe traumatic brain injury in infants, children and adolescents – second edition. Pediatr Crit Care Med. 14(Suppl 1): S182 (2012).
Ness PC. Pentobarbital and EEG burst suppression in treatment of status epilepticus refractory to benzodiazepines and phenytoin. Epilepsia. 1990;31:61–7.
Matthis P, Scheffner D, Benninger C. Spectral analysis of the EEG: comparison of various spectral parameters. Electroencephalogr Clin Neurophysiol. 1981;52(2):218–21.
Steiner LA, Czosynka M, Pechnik SK, Smielewski P, et al. Continuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury. Crit Care Med. 2002;30:7338.
Beers SR, Wisniewski SR, Garcia-Filion P, Tian Y, et al. Validity of a pediatric version of the Glasgow outcome scale–extended. J Neurotrauma. 2012;29(6):1126–39.
Lazardis C, Desantis SM, Smielewski P, et al. Patient-specific thresholds of intracranial pressure in severe traumatic brain injury. J Neurosurg. 2014;120:893–900.
Loss SH, de Oliveira RH, Maccari JG, et al. The reality of patients requiring prolonged mechanical ventilation: a multicenter study. Rev Bras Ter Intensiva. 2014;27(1):26–35.
Foreman B, Claassen J. Quantitative EEG for the detection of brain ischemia. Crit Care. 2012;16(2):216.
Sutter R, Kaplan PW. Clinical and electroencephalographic correlates of acute encephalopathy. J Clin Neurophysiol. 2013;30(5):443–53.
Sansevere AJ, DiBacco ML, Pearl PL, et al. Quantitative electroencephalography for early detection of elevated intracranial pressure in critically ill children: case series and proposed protocol. J Child Neurol. 2022;37(1):5–11.
Chong SL, Qian S, Yao SHW, Allen JC, Dang H, Chan LCN, et al. Early posttraumatic seizures in pediatric traumatic brain injury: a multicenter analysis. J Neurosurg: Pediat. 2021;29:1–7.
Appavu BL, Fox J, Kuwabara M, Burrows BT, et al. Association of cerebral and systemic physiology with quantitative electroencephalographic characteristics of early post-traumatic seizures. J Clin Neurophysiology: In Press; 2022.
Claassen J, Hirsch LJ, Kreiter KT, Du EY, et al. Quantitative continuous EEG for detecting delayed cerebral ischemia in patients with poor-grade subarachnoid hemorrhage. Clin Neurophysiol. 2004;115(12):2699–710.
Appavu B, Foldes S, Temkit M, Jacobson A, et al. Intracranial electroencephalography in pediatric severe traumatic brain injury. Pediatric Crit Care Med. 2020;21(3):240–74.
Acknowledgements
We thank the biostatistician, Dr. M’hamed Temkit, PhD, for counsel and discussion regarding statistical tests implemented in this study.
Funding
This study was funded in part by the US Department of Defense Congressionally Directed Medical Research Programs Epilepsy Research Program (W81XWH-19-1-0514).
Author information
Authors and Affiliations
Contributions
BA and JX contributed to the conception and design of the study. BA, JF, and BTB contributed to acquisition and analysis of data and drafting of a significant portion of the manuscript and figures. PDA contributed to analysis of data and drafting of a significant portion of the manuscript and figures. All authors approved the final draft of this study.
Corresponding author
Ethics declarations
Conflicts of interest
The coauthors have no relevant conflicts to disclose. Dr. Appavu reports a research grant from the American Heart Association (19CDA34760291) outside of the submitted work. Dr. Appavu received a one-time speaking honorarium from Natus for a webinar presentation.
Ethical approval/informed consent
This study was performed under all ethical research guidelines at Phoenix Children’s Hospital, and the Institutional Review Board (IRB #19-284) at Phoenix Children’s Hospital approved this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the collection “The Curing Coma Campaign”.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Xie, J., Burrows, B.T., Fox Kensicki, J. et al. Early Electroencephalographic Features Predicting Cerebral Physiology and Functional Outcomes After Pediatric Traumatic Brain Injury. Neurocrit Care 38, 657–666 (2023). https://doi.org/10.1007/s12028-022-01633-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-022-01633-w