
Abstract
Background
Diagnosing brain death in children is challenging. Guidelines recommend using confirmatory testing to provide ancillary information to support the diagnosis. Brain tissue oxygenation (PbtO2) is being increasingly used in the adult neurocritical care for continuous monitoring of the adequacy of brain oxygenation; however, data in pediatrics is limited. Evidence from adult studies suggests that persistent PbtO2 of 0 mmHg is associated with brain death, but this relationship has not yet been demonstrated in children; therefore, we examined our experience with PbtO2 monitoring and brain death in children with acute neurological pathology.
Methods
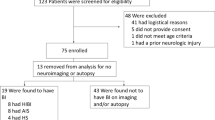
We retrospectively reviewed patient records from a prospectively maintained database of 85 children who were ventilated for coma due to acute neurological injury and who received intracerebral monitoring.
Results
We identified five children who had suffered brain death while being monitored. PbtO2 had decreased to 0 mmHg in all five children at the time of brain death diagnosis. In contrast, PbtO2 in patients, who did not develop brain death, never decreased to 0 mmHg. We review the benefits and drawbacks of using brain tissue oxygenation as ancillary information in diagnosing brain death in children.
Conclusions
Preliminary data from this study suggest that PbtO2 decreases to 0 mmHg when brain death occurs in children. Further study is needed to determine the limitations, and the sensitivity and specificity of this finding in a larger group of children.
Similar content being viewed by others


References
President’s Commission. Guidelines for the determination of death. Report of the medical consultants on the diagnosis of death to the President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. JAMA 1981; 246(19):2184–6.
Academy of Medical Royal Colleges. A code of practice for the diagnosis and confirmation of death. London: Academy of the Medical Royal Colleges; 2008.
Academy of Medical Royal Colleges. A code of practice for the diagnosis of brain stem death. London: Department of health; 1998.
Australian and New Zealand Intensive Care Society. Recommendations on brain death and organ donation. 2nd ed. Melbourne: Australian and New Zealand Intensive Care Society; 1998.
Task Force for the Determination of Brain Death in Children. Guidelines for the determination of brain death in children. Task Force for the Determination of Brain Death in Children. Arch Neurol. 1987;44(6):587–8.
Green JB, Lauber A. Return of EEG activity after electrocerebral silence: two case reports. J Neurol Neurosurg Psychiatry. 1972;35(1):103–7.
Montes JE, Conn AW. Near-drowning: an unusual case. Can Anaesth Soc J. 1980;27(2):172–4.
Shemie SD, Pollack MM, Morioka M, Bonner S. Diagnosis of brain death in children. Lancet Neurol. 2007;6(1):87–92.
Baines PB. Diagnosis and management of brain death in children. Curr Paediatr. 2005;15(4):301–7.
Kohrman MH, Spivack BS. Brain death in infants: sensitivity and specificity of current criteria. Pediatr Neurol. 1990;6(1):47–50.
Wijdicks EF. Brain death worldwide: accepted fact but no global consensus in diagnostic criteria. Neurology. 2002;58(1):20–5.
Bell MDD, Moss E, Murphy PG. Brainstem death testing in the UK—time for reappraisal? Br J Anaesth. 2004;92(5):633–40.
Heran MK, Heran NS, Shemie SD. A review of ancillary tests in evaluating brain death. Can J Neurol Sci. 2008;35(4):409–19.
Blend MJ, Pavel DG, Hughes JR, et al. Normal cerebral radionuclide angiogram in a child with electrocerebral silence. Neuropediatrics. 1986;17(3):168–70.
Drake B, Ashwal S, Schneider S. Determination of cerebral death in the pediatric intensive care unit. Pediatrics. 1986;78(1):107–12.
Monterio LM, Bollen CW, van Huffelen AC, Ackerstaff RGA, Jansen NJG, van Vught AJ. Transcranial Doppler ultrasonography to confirm brain death: a meta analysis. Intensive Care Med. 2006;32:1937–44.
Maas AI, Fleckenstein W, de Jong DA, et al. Monitoring cerebral oxygenation: Experimental studies and preliminary clinical results of continuous monitoring of cerebrospinal fluid and brain tissue oxygen tension. Acta Neurochir Suppl (Wien). 1993;59:50–7.
Guidelines for the management of severe traumatic brain injury. J Neurotrauma 2007; 24(suppl 1): chapter X. doi: 10.1089/neu.2007.9999.
Figaji AA, Fieggen AG, Argent AC, Leroux PD, Peter JC. Does adherence to treatment targets in children with severe traumatic brain injury avoid brain hypoxia? A brain tissue oxygenation study. Neurosurgery. 2008;63(1):83–91.
Figaji AA, Zwane E, Thompson C, et al. Brain tissue oxygen tension monitoring in pediatric severe traumatic brain injury: part 1: relationship with outcome 2009 (epub before print).
Stiefel MF, Udoetuk JD, Spiotta AM, Gracias VH, Goldberg A, Maloney-Wilensky E, et al. Conventional neurocritical care and cerebral oxygenation after traumatic brain injury. J Neurosurg. 2006;105(4):568–75.
Valadka AB, Gopinath SP, Contant CF, Uzura M, Robertson CS. Relationship of brain tissue PO2 to outcome after severe head injury. Crit Care Med. 1998;26(9):1576–81.
Scheufler KM, Röhrborn HJ, Zentner J. Does tissue oxygen-tension reliably reflect cerebral oxygen delivery and consumption? Anesth Analg. 2002;95:1042–8.
Smith ML, Counelis GJ, Maloney-Wilensky E, Stiefel MF, Donley K, LeRoux PD. Brain tissue oxygen tension in clinical brain death: a case series. Neurol Res. 2007;29(7):755–9.
Palmer S, Bader MK. Brain tissue oxygenation in brain death. Neurocrit Care. 2005;1(2):17–22.
Adelson PD, Bratton SL, Carney NA, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Chap. 4. Resuscitation of blood pressure and oxygenation and prehospital brain-specific therapies for the severe pediatric traumatic brain injury patient. Pediatr Crit Care Med. 2003;4:S65–7.
Lang EW, Mulvey JM, Mudaliar Y, Dorsch NWC. Direct cerebral oxygenation monitoring—a systematic review of recent publications. Neurosurg Rev. 2007;30(2):1437–2320.
Stiefel MF, Udoetuk JD, Storm PB, et al. Brain tissue oxygen monitoring in pediatric patients with severe traumatic brain injury. J Neurosurg. 2006;105:281–6.
Narotam PK, Burjonrappa SC, Raynor SC, et al. Cerebral oxygenation in major pediatric trauma: its relevance to trauma severity and outcome. J Pediatr Surg. 2006;41:505–13.
Valadka AB, Hlatky R, Furuya Y, et al. Brain tissue PO2: correlation with cerebral blood flow. Acta Neurochir Suppl. 2002;81:299–301.
Scheufler KM, Lehnert A, Rohrborn HJ, et al. Individual value of brain tissue oxygen pressure, microvascular oxygen saturation, cytochrome redox level, and energy metabolites in detecting critically reduced cerebral energy state during acute changes in global cerebral perfusion. J Neurosurg Anesthesiol. 2004;16:210–9.
Doppenberg EM, Watson JC, Broaddus WC, et al. Intraoperative monitoring of substrate delivery during aneurysm and hematoma surgery: initial experience in 16 patients. J Neurosurg. 1997;87:809–16.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Figaji, A.A., Kent, S.J. Brain Tissue Oxygenation in Children Diagnosed With Brain Death. Neurocrit Care 12, 56–61 (2010). https://doi.org/10.1007/s12028-009-9298-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-009-9298-5