
Abstract
Objectives
To evaluate disease activity status using the Acromegaly Disease Activity Tool (ACRODAT®) in a cohort of Spanish acromegaly patients, to assess the relationship between the level of disease activity according to both ACRODAT® and the physicians’ clinical evaluation, and to study the potential discrepancies in the perception of symptoms between physicians and patients.
Design
Multicenter, observational, descriptive and cross-sectional study.
Methods
Disease activity was assessed in adult patients with acromegaly under pharmacological treatment during at least 6 months using ACRODAT®.
Results
According to ACRODAT®, 48.2%, 31.8% and 20.0% of a total of 111 patients were classified as having a stable disease (S), mild disease activity (M-DA) and significant disease activity (S-DA) respectively. ACRODAT® classification of disease activity significantly correlated with physicians’ opinion, with a moderate inter-rater agreement and a specificity of 92.45% (PPV = 86.21%). No correlation was found between IGF-I levels and severity of symptoms or quality of life (QoL). A decision to take clinical action was significantly more frequent in S-DA and M-DA patients than S patients but no action was taken on 5 (22.7%) and 27 (77.1%) S-DA and M-DA patients, respectively
Conclusions
ACRODAT® detected disease activity in 51.8% of patients. Interestingly, although M-DA and S-DA patients were likely to be in the process of being controlled, action was not always taken on these patients. ACRODAT® is a validated and highly specific tool that may be useful to routinely monitor acromegaly and to identify patients with non-obvious disease activity by incorporating “patient-centred” parameters like symptoms and QoL to the clinical evaluation of acromegaly.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acromegaly, a rare and chronic disease usually caused by a pituitary adenoma, is characterized by hyper-secretion of growth hormone (GH) with a consequent increase in insulin-like growth factor I (IGF-I) [1, 2].
Acromegaly is associated with multiple co-morbidities, premature mortality, and physical disfigurement [1]. The most serious health consequences include type 2 diabetes, high blood pressure, increased risk of cardiovascular diseases, arthropathy and sleep apnoea [3, 4]. In fact, the presence at the diagnosis of diabetes mellitus, cardiovascular disease and hypertension are significantly associated with reduced survival [5]. In addition, acromegaly patients experience decreased energy and psychological disturbances (loss of initiative, mood lability, impaired self-esteem, depression and anxiety) that significantly affect their quality of life (QoL) [6,7,8,9].
The goals of acromegaly treatment are to achieve overall long-term biochemical control, control tumour mass and decrease the risk of developing systemic comorbidities, thereby reducing mortality [10, 11].. Even when biochemical control is achieved, many patients still suffer from physical and psychological residual morbidity that can lead to persistently impaired QoL [6, 12,13,14]. In fact, the correlation between “biochemical” severity (measured by IGF-I levels) and impact of disease on patient’s lives is weak [14, 15]. In addition, from the patient’s perspective, symptoms and QoL are critical parameters of disease control [6, 12], therefore they should be assessed in clinical practice for an adequate long-term management of acromegaly [13].
Discrepancy between patient’s and physician’s ratings of general health status has been previously demonstrated [6, 16, 17]. The consequence of such a discordant viewpoint regarding disease activity is that decisions are often prone to not being shared between patients and physicians [16]. Acromegaly patients place more importance on patient-centred parameters (i.e., signs/symptoms, comorbid conditions and QoL) than do expert endocrinologists [6]. Therefore, the patients’ own perspectives of their health status may be an important additional measure to assess the level of disease activity and support clinical decision-making and, together with IGF-I level and tumour status could provide a more accurate assessment of the disease status [6, 18]
To aid in the global clinical management of acromegaly, a multidimensional clinical decision support tool, the Acromegaly Disease Activity Tool (ACRODAT®) was developed [18]. The ACRODAT® software medical device is a disease specific tool that allows the classification of acromegaly disease activity using a multidimensional approach in three categories: stable (S, adequately controlled), mild disease activity (M-DA: further evaluation of the patient’s condition is needed), or significant disease activity (S-DA: clinical action is required) [18]. The development of this tool was based on the identification of five key health status parameters in acromegaly and the definition of three levels of severity for each of them: IGF-I level, tumour status, presence of co-morbidities (cardiac disease, diabetes, sleep apnoea), signs and symptoms and health-related QoL (Table 1). A scoring algorithm was built based on the classification of 243 hypothetical cases allowing the classification of the disease in the three above mentioned categories [18].
Due to the recent development of the tool, its clinical application has not been studied yet. This study was aimed to evaluate disease activity status using ACRODAT® in a cohort of Spanish patients with acromegaly. Other secondary objectives included the assessment of the relationship between patient demographic characteristics and ACRODAT® disease categories; to assess the relation between classification of disease activity by ACRODAT® and by physician criteria and to study the potential discrepancies in the perception of symptoms between physicians and patients.
Materials and methods
ACROVAL was an observational, cross-sectional, multicenter study conducted in 12 representative hospitals from all over Spain. The study included adult patients diagnosed with acromegaly, on pharmacological treatment for at least 6 months, and with complete clinical reports available. All patients provided their informed written consent. The study was approved by the Clinical Research Ethics Committee of every participant site and it was conducted in accordance with the Declaration of Helsinki principles.
Data collection
Demographic data, acromegaly clinical history, co-morbidities, IGF-I levels and tumour status were obtained from clinical records. Quality of life (QoL), severity of symptoms, job status, disease activity and decision taken regarding acromegaly treatment (surgery, radiotherapy, change in drug treatment or no action) were collected at the study visit. IGF-I levels, tumour status and therapeutic decision at the visit before study visit was also collected from clinical records.
QoL was determined by the Acromegaly Quality of life Questionnaire (AcroQoL) [19]. The AcroQoL questionnaire [19] is a 22-item, disease-specific QoL tool. Each question has five possible answers scored 1–5, with a total maximum score of 110. The score of 110 reflects the best possible QoL. AcroQoL overall score and subscores included in the AcroQoL questionnaire were normalized (0–100) being 100 the best possible QoL.
Severity of symptoms was quantified using the Patient-Assessed Acromegaly Symptom Questionnaire (PASQ) [20]. The PASQ [12] comprises six questions that evaluate six acromegaly key symptoms. Each item is scored on a 9-point scale (0 no symptoms-8 severe incapacitating symptoms). The total PASQ score is the sum of the individual symptom scores (maximum = 48). An additional seventh question addresses the overall health status, which was scored ranging from 0 (best possible) to 10 (worst possible). The questionnaire was completed by physicians (phPASQ) and by patients (paPASQ) in order to compare both perspectives. phPASQ and paPASQ were mutually blinded. Symptoms status are measured in ACRODAT® by a Signs and Symptoms Score (SSS), an abbreviated version of the PASQ score that omits the numbness or tingling of the extremities and the overall health status questions [18]. IGF-I level was measured locally and recorded as a proportion coefficient x the upper limit of normal (ULN) for the respective method used.
Tumour status was classified by the physician in the same three categories that use ACRODAT® (Table 1).
Comorbidities were assigned based on the presence or absence and severity of diabetes, sleep apnoea and cardiac disease (hypertension, hyperlipidaemia, or other cardiac abnormalities) [18] (Table 1).
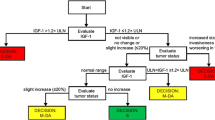
The ACRODAT® tool was used to assess disease activity, entering the data collected in the study. According to the algorithm behind ACRODAT®, IGF-I and tumour status are the predominant parameters in the classification of M-DA or S-DA. Only when the IGF-I level is ≤1.2 x ULN and tumour size did not significantly increase, the remaining three parameters contribute to the classification in a compensatory manner. Data were entered into the ACRODAT tool after the patent’s visits.
Disease activity level (stable, moderate disease activity and significant disease activity) according to physician’s point of view was also recorded. The disease activity was assessed by an endocrinologist with specific experience in acromegaly and neuroendocrinology and the disease activity level was classified according to their experience and criteria (endocrinologist had access to IGF-I levels, tumour status, phPASQ and comorbidities).
Statistical methodology
A descriptive statistical analysis of all the variables was performed, including central tendency and dispersion measures for continuous variables, and absolute and relative frequencies for categorical variables. Student’s t test, Mann–Whitney-U test or Kruskall Wallis H test were used to compare quantitative variables and Pearson’s chi-square or Fisher’s exact tests for qualitative variables. The assumptions of normality distribution (Kolmogorov-Smirnov and Shapiro-Wilk) and homoscedasticity test (Levene’s test) of the different variables were studied for the use of parametric tests.
Pearson/Spearman correlation coefficient was used to study the association between the ACRODAT® scale score and the rest of the variables of analysis, as well as between the variables phPASQ vs paPASQ, IGF-I vs phPASQ and IGF-I vs paPASQ. The Kappa agreement coefficient was calculated to test concordance of disease activity status according to ACRODAT® vs. physicians’ clinical evaluation and to test the concordance between paPASQ and phPASQ. Predictive analysis of ACRODAT® was assessed by determining the values of sensitivity, specificity, the positive predictive value (PPV), and negative (NPV) predictive value. The gold standard used as a reference was the physicians’ clinical evaluation. Tests were two-tailed with a significance level of 5%. The p-values obtained between discrepancies in disease activity and the clinical characteristics of the patients were calculated through a univariate logistic regression model whose dependent variable is the agreement between ACRODAT® classifications and the physiscian’s perception (yes/no). The independent variables are summarized in Supplementary Table 1. In order to determine the factors associated with the existence of discrepancies in the degree of acromegaly activity according to the ACRODAT® scale and the perception of physician, a multivariate regression model was carried out, whose dependent variable be the agreement between both criteria (without discrepancies vs with discrepancies) and as possible associated factors all those that are significant in the model univariate (p value < 0.250). Data were analyzed using SPSS 19.0.
Results
Patient characteristics
In total, 113 patients from 12 centres were included, of whom 111 were considered evaluable in the analysis. Two patients were excluded because their duration of pharmacological treatment was less than 6 months. The acromegaly activity according to the ACRODAT® classification was not available for 1 patient.Table 2 summarizes demographic and clinical characteristics of patients. Macroadenoma was present in most patients (82.7%) at diagnosis (Table 2). However, in 97.1% of patients, tumour was not visible or had not changed in volume since prior MRI and only 3 patients (2.9%) had experienced a slight increase (≤20%) since prior MRI (Table 2). IGF-I levels were within normal limits in 64.0% of patients, above ULN but below 1.2 ULN in 16.2% of patients and above 1.2 ULN in 19.8% of patients.
The most frequent co-morbidity was cardiac disease (54.1%), followed by arthropathy (42.7%), diabetes (36.0%) and sleep apnoea (20.9%) (Table 2). Main comorbidities were controlled in most patients. However, 11.5% of patients presented an uncontrolled cardiac disease and 14.3% an uncontrolled sleep apnoea.
Disability was present in 23.6% of patients (Table 2) and 8.8% of patients were on work leave at the study visit. Most patients had undergone pituitary surgery (75.7%), a third of patients (35.1%) received radiotherapy (34.2% of patients had undergone surgery and radiotherapy), and 23.4% of patients had not undergone surgery nor radiotherapy.
Disease activity
According to ACRODAT®, 48.2% of patients were classified as controlled (S) and 51.8% as having active disease: 31.8% M-DA and 20.0% S-DA (Fig. 1A).

Disease activity according to ACRODAT® (A) and Physicians’ Criteria (B). S stable, M-DA mild disease activity, S-DA significant disease activity
S-DA patients were significantly younger, had a significantly higher headache severity, had a significantly higher number of medication changes in the last two years and their last change in medication was significantly more recent compared to S patients (Table 2). Both M-DA and S-DA patients presented significantly higher values of IGF-I compared with S patients (p < 0.001) (Table 2, Fig. 2A). Consistently with the algorithm behind ACRODAT®, 100% of S-DA patients had IGF-I levels >1.2 ULN (Table 2, Fig. 2A). There were no statistically significant differences in comorbidities or tumour status among S, M-DA or S-DA patients (Table 2, Fig. 2B, C). Symptoms (phPASQ) were significantly more severe (p = 0.004) and QoL significantly worse (p = 0.005) in M-DA patients compared to S patients, and, in some items (joint pain and fatigue severity and physical component of AcroQoL) compared to S-DA patients (Table 2, Fig. 2D, E).

Patients’ characteristics according to ACRODAT®. A IGF-I: insulin-like growth factor-I. B Tumour status. C Comorbidities. D phPASQ: Physician-assessed Acromegaly Symptom Questionnaire fulfilled by the physician. E AcroQoL Acromegaly Quality of Life Questionnaire. S stable, M-DA mild disease activity, S-DA significant disease activity; *p < 0.01 vs. S; **p < 0.001 vs. S; ##p < 0.001 vs. M-DA
According to physicians’ clinical evaluation, 73.9%, 17.1% and 9.0% were classified as S, M-DA or S-DA respectively (Fig. 1B). ACRODAT® classification of disease activity significantly correlated with physicians’ opinion (Pearson’s correlation coefficient 0.621, p < 0.001), with a moderate inter-rater agreement [kappa agreement coefficient 0.569; 95% confidence interval (CI95%): 0.402–0.678]. Predictive analysis between controlled (S) or active disease (M-DA + S-DA) groups according to ACRODAT vs. physicians’ opinion showed a fair inter-rater agreement (kappa agreement 0.356; CI95% 0.207–0.506) a specificity value of 92.5% (CI95%: 84.4–100), sensitivity 43.9% (CI95%: 30.1–57.6), PPV 86.2% (CI95%: 71.9–100) and NPV 60.5% (CI95%: 49.2–71.8).
Discrepancies between ACRODAT® classification of disease activity and physicians’ criteria were observed in patients with IGF-I levels above ULN (p < 0.001), patients with higher symptomatology [joint pain (p < 0.05), numbness or tingling (p < 0.05) and global symptomatology (p < 0.01) according to phPASQ, fatigue (p < 0.05) according to paPASQ], worse health status [according to paPASQ (p < 0.001) and phPASQ (p < 0.01)] and patients showing more QoL impairment (p < 0.05). Moreover, discrepancies were also observed in patients with longer time since diagnosis (p < 0.05) or since the beginning of treatment (p < 0.05). A univariate analysis confirmed these results (Supplementary Table 1). A multivariant analysis showed that the existence of discrepancies between ACRODAT® classification and physicians’ criteria relied on IGF-I, phPASQ and time since diagnosis (p < 0.05) (Supplementary Table 2).
Quality of life
Overall, patients reported mild impairment in their QoL with a mean (SD) AcroQoL total score of 65.7 (19.2) (Tables 2 and 3). Patients scored worse in the physical domain and in the psychological-appearance domain (Tables 2 and 3).
According to ACRODAT® levels of severity for QoL (Table 1), 33.7% of patients presented a mild to moderate (21.2%) or significant (12.5%) impairment on QoL.
No correlation was found between IGF-I levels and AcroQoL (Pearson’s correlation coefficient 0.084, p = 0.395).
Among the 65 patients (60.7%) with controlled IGF-I and tumour status (IGF-I < ULN and tumour not visible or without changes), 1 (1.5%) and 7 (10.8%) presented a significant and mild to moderate impairment of QoL respectively. These patients presented a significant higher time since diagnosis than patients with no or minimal impairment of QoL (mean ± SD = 25.85 ± 0 years in patients with significant impairment; 14.57 ± 5.16 years in patients with mild to moderate impairment; 10.34 ± 7.76 in patients with no or minimal impairment; p = 0.048).
Symptoms
Overall, patients suffered from mild-moderate acromegaly symptoms [mean (SD) phPASQ total score 12.9 (8.6)] (Table 4). According to ACRODAT® levels of severity for symptoms (Table 1), 73,6% of patients showed moderate (51.8%) or severe (21.8%) symptoms.
Physicians rated patient symptoms significantly lower in severity than patients (p < 0.001). However, phPASQ significantly correlated with paPASQ with a substantial inter-rater agreement in both PASQ total score and individual symptoms sub-scores (Table 4). No characteristic traits in patients with discrepancies between phPASQ and paPASQ were found.
No correlation was found between IGF-I levels and phPASQ (Pearson’s correlation coefficient: 0.049, p = 0.615) or paPASQ (Pearson’s correlation coefficient: −0.011, p = 0.911) neither in the total score nor in symptoms or health status sub-scores.
Among the 65 patients (60.7%) with controlled IGF-I and tumour status (IGF-I < ULN and tumour not visible or without changes), 13 (20.0%) and 34 (52.3%) presented severe and moderate symptoms respectively according to their phPASQ (32.3 % and 53.8% respectively according to their paPASQ). No characteristic demographic traits were found for these subgroups of patients.
Therapeutic action
Overall, a therapeutic action regarding acromegaly management was taken in 28.0% of patients in the in the visit previous to the study visit. A significantly higher rate of action was taken on patients with IGF-I > 1.2 ULN than in patients with normal IGF-I (71.4% vs 13.4%; p < 0.001) or IGF-I > ULN but <1.2 ULN at the visit before study visit (71.4% vs 33.3%; p < 0,01).
Results of the therapeutic action taken in the previous visit was not successful in most of the patients: 88.9% (n = 16) of patients with no IGF-I and/or tumour control, remained uncontrolled at the study visit. Similarly, 82.8% (n = 53) of patients in which no action was taken in the last visit remained in the same status. Most of them (83.9%, n = 47) were controlled and remained controlled. Fourteen point one % of patients (n = 9) who were controlled in terms of IGF-I control and tumour at prior visit, spontaneously lost control at the study visit.
At the study visit, therapeutic action was taken in 27.9% of patients overall and a change of medication (dose or drug) was the most frequent action taken (20,7% of patients) (Table 5). In S-DA patients, therapeutic actions were taken on a significantly greater proportion (77.3%) compared to M-DA (22.9%, p < 0.001) and S patients (11.3%, p < 0.001) (Fig. 3). However, no action was taken on 22.7% (n = 5) of S-DA patients and in 77.1% (n = 27) of M-DA patients.

Therapeutic action taken depending on ACRODAT® classification at study visit. S stable, M-DA mild disease activity, S-DA significant disease activity. **p < 0.001 vs. S; ##p < 0.001 vs. M-DA
In 3 of those 5 S-DA patients, a change in treatment (dose or drug) was taken in the last visit, that took place a mean (SD) of 5.2 (2.7) months before the study visit. In the other 2 patients, no action was taken either in the last visit or in the study visit. Both presented IGF-I levels above ULN at both visits, but one of them was considered stable according to physician criteria.
Differences between M-DA patients in which no action was taken (n = 27) vs patients in which action was taken (n = 8) at the study visit were found in patients where the disease activity classification by physician’s criteria was different than ACRODAT® classification (4 vs 24 classified as S-DA, p < 0.05), patients with longer time since the beginning of treatment (mean time 5.87 vs 10.41 years, p < 0.05) and patients with longer time since the last visit (mean time 3.96 vs 6.70 years, p < 0.05).
Criteria that marked the decision to take a therapeutic action on S-DA and M-DA patients were IGF-I levels and IGF-I + tumour control at the last visit and at the study visit (p < 0.01).
Discussion
Traditional clinical treatment goals for acromegaly are mainly based on the achievement of biochemical and tumour control [6, 10]. However, even when biochemical and tumour control is achieved, many patients continue to experience symptoms and impaired HRQoL [6, 12, 13, 21]. Moreover, challenges in the IGF-I measurement [22, 23] and subjectivity in tumour growth assessment [24] limits the use of these parameters as the sole assessment of disease activity.
ACRODAT® is a new software medical device designed to assess acromegaly activity from an integrated point of view as it includes not only clinical parameters of disease but also patients’s reported outcomes (PRO), such as symptoms and HRQoL [18]. AcroVoice, a study to determine which parameters matter to acromegaly patients for defining their disease, showed that, in contrast with the physician validation study, patients placed more value on the “patient-centred” parameters [6]. Thus, validated PRO should be regularly documented in acromegaly patients as a patient-oriented indicator of treatment success [13, 15]. Indeed, objective tools such as ACRODAT® and SAGIT® have been recently recommended to assess and monitor acromegaly disease activity [1, 25, 26].
Herein, we show the first real world data evaluating disease activity status using ACRODAT® and its correlation with physicians’ criteria, in a representative cohort of 111 Spanish patients attended in a clinical practice setting. Patient population was similar to other studies [27, 28], with a mean age of 59.7 years and 51.4% of women.
60.7% of patients were controlled in terms of IGF-I and tumour volume. According to ACRODAT®, only 48.2% of patients were considered controlled or stable and 51.8% presented with active disease (Fig. 1A). According to the physicians’ clinical evaluation, 73.9% of patients were stable whereas 26.1% presented with uncontrolleddisease (Fig. 2B). ACRODAT® and physician’s opinion showed a fair inter-rater agreement. Thus, for patients who according to the physician were stable, 92.5% of them were classified by ACRODAT® as stable. However, ACRODAT® was able to identify more cases of active disease due to the integration of other than biochemical and tumour control parameters such as comorbidities, symptoms and QoL in its definition of control. Discrepancies between ACRODAT® and physicians’ criteria were mainly observed in patients with IGF-I above ULN, phPASQ (more severe signs and symptoms), patients showing more QoL impairment and a longer time since diagnosis or since the beginning of treatment. Thus, ACRODAT® may be especially useful in determining disease activity in patients with these characteristics. A source of discrepancy may be the existing differences in the definition of biochemical control: while ACRODAT® considers an IGF-I level >1 ULN as active disease, the currently used cut-offs in clinical practice ranges from 1 to 1.5 ULN [29]. A possible reason is the distrust in the accuracy of IGF-I levels due to the variability of the diagnostic assays [22, 23, 30]. However, all-cause mortality risk in acromegaly increases with higher serum IGF-I levels and that IGF-I normalization (IGF-I < ULN) is associated with all-cause mortality rates indistinguishable from the general population [31].
IGF-I levels do not correlate with symptoms or QoL as has been described in this and other studies [14, 15]. In fact, we found that 12.3% of patients with IGF-I and tumour control had a mild to moderate or significant impairment in QoL. Similarly, 72.3% of patients according to phPASQ, or 86.1% according to paPASQ, showed moderate or severe symptoms despite having reached IGF-I and tumour control. Interestingly, patients with IGF-1 and tumour control that had impairment in QoL and symptoms according to paPASQ did not statistically differences in the time since diagnosis in comparison with patients with IGF-1 and tumour control that showed stable QoL and mild symptomatology (data not shown). phPASQ and paPASQ showed a substantial inter-rater agreement, however, physicians tended to rate the intensity of symptoms significantly lower than patients. These findings support the need to consider validated PROs in disease activity assessment although, currently, this is not common clinical practice: 53.8% and 30.8% of the physicians involved in this study affirmed not using PASQ and AcroQoL, respectively (data not shown). The study also showed that there were a proportion of patients with uncontrolled cardiac disease (11.5%) or sleep apnoea (14.3%). Comorbidities should be regularly monitored and appropriate therapeutic actions should be taken to minimize disease burden and mortality.
Most patients can achieve disease control if their treatment is adequately selected and adjusted according to patient characteristics and response [32]. Indeed, Ragonese et al. showed that, when adequately titrated, pegvisomant could achieve IGF-I control in 89.6% patients [33], a higher proportion than reported whentitration was applied in usual clinical practise as described in Acrostudy [24]. In our study, therapeutic actions were taken in a significantly greater proportion of S-DA patients compared to M-DA and S patients, but no action was taken in a significant number of patients with disease activity according to ACRODAT® (22.7% of S-DA patients and 77.1% of M-DA patients) (Fig. 3). A possible explanation may be that these patients were in the process of treatment adjustment (S-DA patients had more changes of medication and more recently) and physicians were waiting to see a stabilization before making a decision. Time between visits in these cases should be optimized. Discrepancies in the IGF-I cut-offs levels or the low reliability of IGF-I determinations may explain the inaction on some M-DA patients. Indeed, Schöfl et al. [30], described that one of the main reasons not to change/escalate treatment in uncontrolled patients was the fluctuating IGF-I levels. In any case, there were a significant number of patients with IGF-I and tumour control but poor PROs that did not receive a possible change in treatment that they might have needed. Furthermore, circulating IGF-I does not guarantee normal exposure to IGF-I in all tissues as demonstrated by Neggers et al. [12]. The lack of therapeutic action may also be a consequence of clinical inertia such as “watch and wait” or “trial-error” attitude. Therapeutic decision in S-DA and M-DA patients was guided by IGF-I levels and IGF-I+ tumour control despite collecting patient PROs in the study visit, showing that that clinical and analytical data collection may not be useful if it is not integrated and interpreted. ACRODAT® may support the decision-making process by providing an integrated holistic view of the disease, even though in some cases it might be difficult to obtain all PROs in the time frame of a routine outpatient visit.
Some limitations derived from the cross-sectional nature of this study should be borne in mind. The data presented here are a cross-sectional picture of a specific moment of the state of illness of patients with a long evolution of the disease. ACRODAT® is designed to long-term monitor changes at regular intervals that can facilitate a better management of patients. Second, the PASQ used in ACRODAT® in this study was completed by physicians, although concordance was observed between the PASQ completed both by patients and physicians. Finally, therapeutic action collected in the study referred to acromegaly treatments, and specific treatment for comorbidities or symptoms were not collected.
In conclusion, ACRODAT® is a validated and highly specific tool that allows routinely monitoring of disease activity in a holistic manner by incorporating clinical, laboratory and radiological parameters (IGF-I, tumour status and comorbidities) as well as PRO parameters such as PASQ and AcroQoL. Monitoring changes at regular intervals may be useful to identify patients with non-obvious disease activity, facilitate better treatment decisions and support an integral approach to acromegaly disease management.
References
S. Melmed, M.D. Bronstein, P. Chanson, A. Klibanski, F.F. Casanueva, J.A.H. Wass et al. A consensus statement on acromegaly therapeutic outcomes. Nat. Rev. Endocrinol. 14(9), 552–61. (2018)
L. Vilar, C.F. Vilar, R. Lyra, R. Lyra, L.A. Naves, Acromegaly: clinical features at diagnosis. Pituitary. 20(1), 22–32 (2017)
A. Colao, D. Ferone, P. Marzullo, G. Lombardi, Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr. Rev. 25(1), 102–152 (2004)
I.M. Holdaway, M.J. Bolland, G.D. Gamble, A meta-analysis of the effect of lowering serum levels of GH and IGF-I on mortality in acromegaly. Eur. J. Endocrinol. 159(2), 89–95 (2008)
C. Rajasoorya, I.M. Holdaway, P. Wrightson, D.J. Scott, H.K. Ibbertson, Determinants of clinical outcome and survival in acromegaly. Clin. Endocrinol. (Oxf) 41(1), 95–102 (1994)
Y. Jackson, E. Flood, S. Rhoten, E.M. Janssen, M. Lundie, AcroVoice: eliciting the patients’ perspective on acromegaly disease activity. Pituitary. 22(1), 62–69 (2019)
H. Kepicoglu, E. Hatipoglu, I. Bulut, E. Darici, N. Hizli, P. Kadioglu, Impact of treatment satisfaction on quality of life of patients with acromegaly. Pituitary. 17(6), 557–563 (2014)
J. Tiemensma, A.A. Kaptein, A.M. Pereira, J.W. Smit, J.A. Romijn, N.R. Biermasz, Affected illness perceptions and the association with impaired quality of life in patients with long-term remission of acromegaly. J. Clin. Endocrinol. Metab. 96(11), 3550–3558 (2011)
R. Trepp, R. Everts, C. Stettler, S. Fischli, S. Allemann, S.M. Webb et al. Assessment of quality of life in patients with uncontrolled vs. controlled acromegaly using the Acromegaly Quality of Life Questionnaire (AcroQoL). Clin. Endocrinol. (Oxf) 63(1), 103–110 (2005)
L. Katznelson, E.R. Laws Jr., S. Melmed, M.E. Molitch, M.H. Murad, A. Utz et al. Acromegaly: an endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 99(11), 3933–3951 (2014)
F. Cordido, J.A. Garcia Arnes, M. Marazuela Aspiroz, E. Torres Vela; grupo de Neuroendocrinologia de la Sociedad Espanola de Endocrinologia y N., [Practical guidelines for diagnosis and treatment of acromegaly. Grupo de Neuroendocrinologia de la Sociedad Española de Endocrinologia y Nutricion]. Endocrinol. Nutr. 60(8), 457 e1–e15 (2013)
S.J. Neggers, M.O. van Aken, W.W. de Herder, R.A. Feelders, J.A. Janssen, X. Badia et al. Quality of life in acromegalic patients during long-term somatostatin analog treatment with and without pegvisomant. J. Clin. Endocrinol. Metab. 93(10), 3853–3859 (2008)
M. Guitelman, A. Abreu, A.L. E-d-l-M, M. Mercado, Patient-focussed outcomes in acromegaly. Pituitary. 17(Suppl 1), S18–S23 (2014)
S.M. Webb, X. Badia, N.L. Surinach; Spanish AcroQol Study G., Validity and clinical applicability of the acromegaly quality of life questionnaire, AcroQoL: a 6-month prospective study. Eur. J. Endocrinol. 155(2), 269–77 (2006)
C. Sievers, K. Brubach, B. Saller, H.J. Schneider, M. Buchfelder, M. Droste et al. Change of symptoms and perceived health in acromegalic patients on pegvisomant therapy: a retrospective cohort study within the German Pegvisomant Observational Study (GPOS). Clin. Endocrinol. (Oxf) 73(1), 89–94 (2010)
P. Studenic, H. Radner, J.S. Smolen, D. Aletaha, Discrepancies between patients and physicians in their perceptions of rheumatoid arthritis disease activity. Arthritis Rheum. 64(9), 2814–2823 (2012)
K. Webber, A.N. Davies, M.R. Cowie, Disparities between clinician and patient perception of breakthrough pain control. J. Pain Symptom Manage. 51(5), 933–937 (2016)
A.J. van der Lely, R. Gomez, A. Pleil, X. Badia, T. Brue, M. Buchfelder et al. Development of ACRODAT((R)), a new software medical device to assess disease activity in patients with acromegaly. Pituitary. 20(6), 692–701 (2017)
X. Badia, S.M. Webb, L. Prieto, N. Lara, Acromegaly quality of life questionnaire (AcroQoL). Health Qual. Life Outcomes 2, 13 (2004)
P.J. Trainer, W.M. Drake, L. Katznelson, P.U. Freda, V. Herman-Bonert, A.J. van der Lely et al. Treatment of acromegaly with the growth hormone-receptor antagonist pegvisomant. N. Engl. J. Med. 342(16), 1171–1177 (2000)
S.M. Webb, X. Badia, Quality of life in acromegaly. Neuroendocrinology. 103(1), 106–111 (2016)
A. Pokrajac, G. Wark, A.R. Ellis, J. Wear, G.E. Wieringa, P.J. Trainer, Variation in GH and IGF-I assays limits the applicability of international consensus criteria to local practice. Clin. Endocrinol. (Oxf) 67(1), 65–70 (2007)
A. Algeciras-Schimnich, D.E. Bruns, J.C. Boyd, S.C. Bryant, K.A. La Fortune, S.K. Grebe, Failure of current laboratory protocols to detect lot-to-lot reagent differences: findings and possible solutions. Clin. Chem. 59(8), 1187–1194 (2013)
P.U. Freda, M.B. Gordon, N. Kelepouris, P. Jonsson, M. Koltowska-Haggstrom, A.J. van der Lely, Long-term treatment with pegvisomant as monotherapy in patients with acromegaly: experience from ACROSTUDY. Endocr. Pract. 21(3), 264–274 (2015)
A.Giustina, A. Barkan, A. Beckers, N. Biermasz, B.M.K. Biller, C. Boguszewski, et al. A consensus on the diagnosis and treatment of acromegaly comorbidities: an update. J. Clin. Endocrinol. Metab. 105(4), e937–e946 (2020).
A. Giustina, G. Barkhoudarian, A. Beckers, A. Ben-Shlomo, N. Biermasz, B. Biller et al. Multidisciplinary management of acromegaly: a consensus. Rev. Endocr. Metab. Disord. 21(4), 667–78. (2020)
I. Bernabeu, A. Pico, E. Venegas, J. Aller, C. Alvarez-Escola, J.A. Garcia-Arnes et al. Safety of long-term treatment with Pegvisomant: analysis of Spanish patients included in global ACROSTUDY. Pituitary. 19(2), 127–137 (2016)
R. Camara, E. Venegas, J.A. Garcia-Arnes, F. Cordido, J. Aller, M.L. Samaniego et al. Treatment adherence to pegvisomant in patients with acromegaly in Spain: PEGASO study. Pituitary. 22(2), 137–45. (2019)
M.J. van Esdonk, E.J.M. van Zutphen, F. Roelfsema, A.M. Pereira, P.H. van der Graaf, N.R. Biermasz et al. How are growth hormone and insulin-like growth factor-1 reported as markers for drug effectiveness in clinical acromegaly research? A comprehensive methodologic review. Pituitary. 21(3), 310–22. (2018)
C. Schofl, M. Grussendorf, J. Honegger, A. Tonjes, D. Thyroke-Gronostay, B. Mayr et al. Failure to achieve disease control in acromegaly: cause analysis by a registry-based survey. Eur. J. Endocrinol. 172(4), 351–356 (2015)
N.A. Tritos, A.F. Mattsson, G. Vila, B.M.K. Biller, A. Klibanski, S. Valluri et al. All-cause mortality in patients with acromegaly treated with pegvisomant: an ACROSTUDY analysis. Eur. J. Endocrinol. 182(3), 285–92. (2020)
C. Schofl, H. Franz, M. Grussendorf, J. Honegger, C. Jaursch-Hancke, B. Mayr et al. Long-term outcome in patients with acromegaly: analysis of 1344 patients from the German Acromegaly Register. Eur. J. Endocrinol. 168(1), 39–47 (2013)
M. Ragonese, S. Grottoli, P. Maffei, A. Alibrandi, M.R. Ambrosio, G. Arnaldi et al. How to improve effectiveness of pegvisomant treatment in acromegalic patients. J. Endocrinol. Invest. 41(5), 575–81. (2018)
Acknowledgements
We thank all the investigators of ACROVAL study and participant patients at Hospital Universitari Son Espases (Dr. Honorato García), Hospital Universitario Príncipe de Asturias (Dra. Concepción Blanco), Hospital Universitario Central de Asturias (Dr. Edelmiro Menéndez), Hospital Universitario de la Princesa (Dra Mónica Marazuela), Hospital Clínico Universitario de Santiago (Dr. Ignacio Bernabeu), Hospital Universitario Miguel Servet (Dr. Pablo Trincado), Hospital Universitario de Basurto (Dr. Miguel Paja), Hospital Universitario de Cruces (Dra. Mª Dolores Moure), Hospital Regional Universitario de Málaga (Dra. Inmaculada González), Hospital General Universitario de Valencia (Dr. Juan Carlos Ferrer), Hospital Universitario Puerta de Hierro (Dr. Javier Aller) and Hospital Universitario Reina Sofia de Córdoba (Dra. Ángeles Gálvez).
Funding
This study was funded by Pfizer (Spain).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
L.S.-C. and M.D.-M. are employees of Pfizer (Spain). M.L.S. works for Pfizer (Spain). M.M., C.B., I.B., E.M., R.V., M.P., M.S.-N. have received compensation from Pfizer (Spain) for their participation as investigators of ACROVAL study. M.M. has received compensation from Pfizer (Spain) for their participation as research coordinator of ACROVAL study. M.M., I.B. and M.P. have received speaker honoraria from Pfizer (Spain). M.M., I.B. and M.S.-N. have received speaker honoraria from Novartis. M.M. and C.B. have received speaker honoraria from Ipsen. M.M. has participated in advisory boards for Ipsen, Novartis and Pfizer (Spain). I.B. is a grant recipient and advisory board member for Pfizer. This study was sponsored by Pfizer. Medical writing support was provided by Esther Tapia PhD, and was funded by Pfizer.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Marazuela, M., Blanco, C., Bernabeu, I. et al. Acromegaly disease activity according to ACRODAT®, a cross-sectional study in Spain: ACROVAL study. Endocrine 75, 525–536 (2022). https://doi.org/10.1007/s12020-021-02900-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-021-02900-0