
Abstract
For analyzing the changes in immunoglobulins, HSP70, ghrelin levels in blood samples were collected from volunteers vaccinated against swine flu before the vaccinations and on days 3, and 15, and 1 and 2 months after the vaccination in the presence or absence of fever associated with the it. The study included 11 subjects having developed a fever, and 13 subjects not having a fever, and 20 control subjects. Immunoglobulins were measured by nephelometry, and HSP70 and ghrelins by appropriate ELISA tests. The level of ghrelin was reduced, while the level of HSP70 was significantly increased in subjects who developed fevers. When temperatures were normalized, both levels were found similar to the control group. These results indicate that the increase in serum immunoglobulins levels associated with vaccinations, along with, elevations in HSP70 and reduced ghrelin levels associated with fever, may be the important parameters in the clinical evaluation and follow-up of treatments with vaccines.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A World Health Organization (WHO) [1] alert in late March and early April 2009 was with regard to cases of human infection with a hemagglutinin (H1) and neuraminidase (N1) caused by a new H1N1 influenza virus (also known as swine flu, pig influenza, and hog flu) [2]. These were first detected in Mexico, with subsequent cases occurring in many other countries, including Turkey [3–7]. In order to prevent a pandemic, a large proportion of the population needed to have acquired an immunity either through vaccination or naturally [8]. After detection of the virus, vaccine manufacturers started developing a pandemic H1N1 vaccine. Global vaccinations inoculated against swine flu with the use of inactivated, without and with adjuvant, and live attenuated vaccines [8–11]. Health-care workers were among the first to be inoculated against swine flu in most countries, including Turkey. This was to control an epidemic that had been announced when vaccine producers started making delivery in autumn in the northern hemisphere [1].
Some reports in the media and the internet indicated that health workers were unwilling to receive swine flu vaccinations. Occasionally, any vaccine can produce some general side-effects, such as redness, allergy, swelling, headache, muscle aches and pains, swelling at the site of the injection, and a mild rash and fever, the last being the most common side-effect, occurring in 5–15 % of recipients [12, 13]. An elevated temperature occurs in 25.8 % of the general population after any vaccination [13].
Inactivated influenza vaccine can stimulate antibodies of the IgA and IgM class under the right circumstances and also lead to the production of IgG immunoglobulin in the blood depending to a great extent on their pre-vaccination levels [14, 15]. Increased fever, resultings in the synthesis of more HSPs, is also found with a variety of other environmental stressors (including vaccinations) [16–19]. Short-term cold and hot exposures also alters the synthesis of total plasma ghrelin concentrations in humans [20]. Ghrelin blocks apoptosis signal-regulating kinase 1 activity via upregulations of HSP70 [21] and ghrelin attenuates burn-induced dysfunctions [22]. Ghrelin, discovered by Kojima et al. [23], is present in two major forms in the tissues and circulation: one binds a fatty acid (octanoic acid; caprylic acid), and is called a lipopeptide (acylated) ghrelin; the other contains fatty acid, and is called desacylated ghrelin.
Owing to these properties, we hypothesized that ghrelins, HSP70, IgA, IgM, and IgG levels could change particularly in conditions such as a fever during immunization, in which circulating levels of the HSP70 and ghrelins are likely to be increased or reduced, respectively. The purpose of this study was to measure circulating levels of HSP70, acylated and desacylated ghrelins, IgA, IgM, and IgG in blood taken before vaccinations, on days 3 and 15, and after 1 and 2 months regardless of fever developing or not. This was to determine any association with clinical and biochemical parameters in health-care workers inoculated against swine flu.
Materials and methods
Ethical approval from the Turkish Republic General Directorate of Drugs and Pharmaceuticals, Elazig Ethics Board Presidency was obtained (dated December, 09, 2009 and resolution number 05). The study involved registering 20 healthy health-care-workers volunteers who had declined vaccinations and 90 matched health-care-workers volunteers in the same age group (from 40.8 ± 4.5 to 40.9 ± 3.00) and with the same body mass index (BMI: from 23.7 ± 1.7 to 24.9 ± 2.5) (45 females and 45 males) who had accepted to be vaccinated at the Department of Infectious Diseases of the Elazig Education and Research Hospital and Firat University, Elazig, Turkey. The vaccine manufacturing firm informed that the vaccines to be used contained 7.5 μg hemagglutinin, 50 μg tiomersal, adjuvant emulsion MF59: 9.75 mg squalene, 1.175 mg polysorbate, and 1.175 mg sorbitan trioleate. The vaccine used through this study was a product from one company (Novartis); its adjuvant was MF59C.1 and its viral strain was an A/California/7/2009 (H1N1) v-like. The participating individuals were given an appetite test (visual analogue scales) before and after the study [24]. Because ghrelin’s production and release are strongly affected by food intake [25, 26]. All volunteer subjects were healthy individuals without clinical or laboratory signs, symptoms of infectious diseases, or metabolic disorders. They were all non-smokers, had no alcohol consumption, and were not taking hormones, oral contraceptives, or dietary supplements with antioxidants. There were also limitations on the use of antipyretics such as paracetomol/acetaminophen. None of the subjects had diabetes mellitus, rheumatoid arthritis, liver and renal disorders, neoplasia, psychiatric disorders, or pregnancy. Blood samples were taken once from the healthy volunteers. In total, six blood samples of 8 mL were collected from the volunteers who agreed to participate in the vaccination program after an overnight fast, before vaccination, and on days 3 and 15, as well as at 1 and 2 months after the vaccination. From each sample, 4 mL was used in the analysis of biochemical parameters, immunoglobulins and HSP70. The remaining 4 mL was used to analyze peptides’ levels. For this, the samples were put into tubes that contained protease inhibitors (500 KIU aprotinin), according to the published and prescribed procedure [27, 28]. Samples were kept at room temperature for 30 min and centrifuged at 4,000 rpm for 5 min. The sera obtained were then put into Eppendorf tubes and kept at −80 °C until analysis. Sera in which HSP70 was studied were put into Eppendorf tubes without protease inhibitor and stored at −80 °C until analysis.
Biochemical analysis
The concentrations of glucose, aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyltransferase (GGT), total cholesterol, triglyceride, very low density lipoprotein (VLDL)-cholesterol, and high-density lipoprotein (HDL), high-density lipoprotein-cholesterol (HDL-C) were measured by standard methods in a certified laboratory. Low density lipoprotein (LDL), low density lipoprotein-cholesterol (LDL-C) was calculated using the Friedewald equation [29]. HSP70s values were measured according to the manufacturer’s instructions, using the ELISA method (E90873Hu Uscn Life Science Inc.). The detection range was 0.625–40 ng/mL. Serum samples were also assayed for acylated (Cat# A05106) and desacylated ghrelin (Cat# A05119) using commercially available ELISA (SPI BIO, Bertin Pharma Biotech, Montigny le Brettoneux, France). The detection limit of the acylated ghrelin ELISA was 0.3 pg/mL, and that of the desacylated ghrelin was 0.2 pg/mL. Immunoglobulins A (IgA); G (IgG); and M (IgM), were determined by a nephelometric method using a Siemens Machine (Model of BN II). The sera to be analyzed were divided into two groups depending on whether or not fever had developed due to the vaccination. Statistical analyses were conducted using SPSS 10.00 package software. The parameters are presented as mean ± standard deviation. Data among groups were compared using the Pearson correlation test. Linear regression analyses were carried out on the mean values using Pearson’s test. P < 0.05 was considered statistically significant.
Results
Of the original vaccinated health workers (n = 90), only 24 completed the study, with 11 subjects developing fever [total subjects with fever (n:19)] and 13 not having fever. The majority of the subjects who dropped out of the study did not develop fever after being vaccinated. On day 3, the swine flu-vaccination-associated fever had disappeared. Body temperatures around 36.5–37 °C were accepted as normal (even for controls), while above 37 °C was considered as development of a fever. Eleven subjects who developed fevers were curious about the results, and all wanted to complete the study. The remainder completed the study even though they showed no vaccination-associated problems. There were also 20 healthy control subjects who had not been vaccinated. Demographic characteristics of the participants showed that there was no statistical difference in BMIs, heights, and ages. None of the participants developed any major clinical symptom during the 2 months after vaccination other than a fever. Table 1 shows the biochemical parameters before the study, during the feverish period, and after fever. ALT, AST, and GGT values showed little change, but GGT values were elevated on post-vaccination at days 3 and 15, and at 1 month. These values returned to normal by the 2nd month.
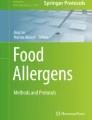
The ghrelin values of the blood samples collected before vaccination and control subjects who were not vaccinated were compared with blood samples collected at days 3 and 15 after vaccinations, these handoff subjects were lower. Their ghrelin levels at months 1 and 2 had risen back to basal levels. When ghrelin levels of the subjects who did and did not develop fevers were compared, ghrelin levels in the blood samples of the former were significantly lower. The fever generally returned to normal within 3 days. Ghrelin levels in the samples taken at months 1 and 2 were similar to basal levels and those of the control subjects (Fig. 1).

Changes of acylated (a) and desacylated (b) ghrelin concentrations in the control group and in subjects with and without fever after swine flue vaccinations and with their blood taken before vaccine at days 3 and 15, and at 1 and 2 months. a P < 0.05 compared to subjects with fever versus without a fever and control subjects
When HSP70 values in samples taken before vaccinations and those of the control subjects who were not vaccinated were compared to those on post-vaccination at days 3 and 15, they were found higher. HSP70 levels in the blood samples taken at 1 and 2 months had fallen back to basal levels. A comparison of the HSP70 levels of the subjects who developed fever were significantly elevated compared to those who had no fever. Again, these serum HSP 70 levels fell back to basal levels by the 1st month (Fig. 2). When immunoglobulin (IgA, M, and G) levels were compared with basal levels and the levels in the control group, an increase was observed at all other sampling times after 15 days from vaccination (Figs. 3, 4 and 5).

Changes in HSP70 levels in controls and subjects who developed fever and who did not developed fever after swine flue vaccination, pre-vaccination, and at days 3 and 15, and at 1 and 2 months. a P < 0.05 compared to subjects with fever versus without fever and controls. b P < 0.05 compared to subjects with fever versus without fever

Changes in immunglobulin A levels in controls and subjects who developed fever or did not develop fever after vaccination, pre-vaccination, and at days 3 and 15, and at 1 and 2 months. a P < 0.05 compared to subjects with fever versus without fever and control subjects

Changes of immunglobulin M concentrations in controls and subjects who developed fever and did not develop fever after vaccination, pre-vaccination, and at days 3 and 15, and at 1 and 2 months. a P < 0.05 compared to subjects with fever versus without fever and control subjects

Changes of immunglobulin G concentrations in controls and subjects who developed fever and did not develop fever after vaccination, pre-vaccination, and at days 3 and 15, and at 1 and 2 months. a P < 0.05 compared to subjects with fever versus without fever and control subjects
Discussion
As with most natural infections, vaccinations result in the development of both humoral and cellular immunity and interferon production. Blood and nasal secretions analyzed during 12–15 days after vaccination contain immunoglobulin (Ig) G, IgM, and IgA classes of antibodies [14–30]. While IgM and IgA antibodies disappear in a few years, IgG antibodies can last for a lifetime [31–33]. Serum IgM, IgA, and IgG levels following H1N1 vaccinations were found in our investigation to have increased significantly at day 15, and at 1 and 2 months, in comparison with IgM, IgA, and IgG antibody values before vaccination and at 3 days after vaccination. Time-dependent serum levels of IgM, IgA, and IgG levels in the group that developed fever were no different from those of the control or pre-vaccination values. Lu et al. [31] reported that systemic immunization with respiratory syndrome coronavirus (SARS-CoV) virus-like particles (VLPs) increased immunoglobulins, which may play an important role in protecting against viral infections. A time-dependent increase in the serum levels of IgM, IgA, and IgG antibodies after vaccination may occur via B-cell activation following swine flu vaccinations, and therefore play an important role in clinical evaluation and follow-up.
Also measured were the serum acylated and desacylated ghrelins’ serum values before and after vaccination in the subjects whose body temperature rose above 37 °C, as well as those values in subjects whose body temperature were at or below 37 °C, and then all were compared with the control group. A decrease in these levels occurred, while HSP70 levels at these times increased. The decrease in ghrelin levels after the H1N1 vaccine may have resulted from the vaccine causing extreme stress in the body, with ghrelins being used up by scavenging free radicals (ghrelin is a natural endogenous antioxidant in the body) [34]. This is supported by serum ghrelin levels in control, pre-vaccination, and post-vaccination (at 15 days, and at 1 and 2 months) samples. These levels were first elevated and then restored to pre-vaccination levels. The significant decrease in ghrelin levels in association with fever is consistent with the results obtained by Tomasik et al. [20], who kept their subjects of environments in varying temperatures, and it was found to have increased that temperature, resulting in decreased ghrelin levels. Exogenous various hormones and drugs also affect ghrelin concentrations. Insulin [35], either oral or intravenous glucose [36], somatostatin, and cortistatin [37] suppress circulated ghrelin concentrations. These findings showed that serum ghrelin levels can be changed by cold and hot stresses, various hormones, and drugs [20]. Ghrelin levels also decrease in patients receiving interferon therapy [38], which means any foreign substance injected to the body (e.g., a vaccine) either directly suppresses ghrelin synthesis in the appropriate organs or ghrelin is metabolically used to eliminate the stress caused by the foreign substance. Ghrelin expression is inhibited by interferon gama [39]. Elevated HSP70 in the serum of patients who had developed fever associated with vaccinations may have arisen from HSP70 production in the body caused by the fever. There are numerous studies demonstrating that HSP70 increased even with the slightest increase in temperature, the manner in which the body normally reacts to fever [15, 17, 19]. This argument is supported by the fact that HSP70 expressions rose in feverish patients, whereas the pre-and post-vaccination values in the patients who did not develop fever remained the same.
The evaluated results should be considered to have a few limitations as follows: (1) persons who decline vaccination may differ in unmeasured ways from those who accept vaccination. (2) People do not usually fast overnight before vaccination. (3) 66/90 (73.33 %) subjects dropped out from the vaccinated arm of the study. (4) Very low thresholds used for fever: 37 °C which is “average” normal temperature. (5) It is not known whether differently formulated vaccines have yielded different results. (6) It is not known whether the receipt of seasonal influenza vaccines, regardless of adjuvanted or unadjuvanted caused similar phenomena in vaccines. (7) It is not known whether adjuvant (MF59C.1) itself contributes to decreases in ghrelins and increases in HSP70 levels. (8) Finally, it is not known whether the observed fever could be associated to the increase in total antibodies, leading to a high reactogenicity or other side-effects.
In conclusion, the increase in serum levels of IgM, IgA, IgG seen in patients after vaccination relative to their levels before the swine flu vaccinations and those in the controls indicated that the vaccination stimulates the humoral immune system. Serum HSP70 significantly increased in the patients who developed fever after being vaccinated. Serum ghrelin levels fell significantly until the first month post-vaccination sample. The decrease in serum ghrelin levels was more marked in the patients who developed fever, with the levels falling back after the fever disappeared than those seen in patients who did not develop a fever. The results indicate that the increase in serum levels IgM, IgA, and IgG levels, elevation of HSP70 associated with fever, and reduced ghrelin levels can be important parameters in the clinical evaluation and follow-up of vaccinations. These findings could also be used in clinical or preclinical trials to develop vaccines that are less likely to induce fever, and also provide some information as to whether the rather intensive blood-drawing schedule would seem to rule out any use in “routine” practice of vaccination.
References
World Health Organization: World now at the start of 2009 influenza pandemic (2009), http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html
N. Bastien, N.A. Antonishyn, K. Brandt, C.E. Wong, K. Chokani, N. Vegh, G.B. Horsman, S. Tyler, M.R. Graham, F.A. Plummer, P.N. Levett, Y. Li, Human infection with a triple-reassortant swine influenza A (H1N1) virus containing the hemagglutinin and neuraminidase genes of seasonal influenza virus. J. Infect. Dis. 201, 1178–1182 (2010)
R. Acuña-Soto, L. Castañeda-Davila, G. Chowell, A perspective on the 2009 A/H1N1 influenza pandemic in Mexico. Math. Biosci. Eng. 8, 223–238 (2011)
A.L. Greninger, E.C. Chen, T. Sittler, A. Scheinerman, N. Roubinian, G. Yu, E. Kim, D.R. Pillai, C. Guyard, T. Mazzulli, P. Isa, C.F. Arias, J. Hackett, G. Schochetman, S. Miller, P. Tang, C.Y. Chiu, A metagenomic analysis of pandemic influenza A (2009 H1N1) infection in patients from north America. PLoS ONE 5, e13381 (2010)
S. Hilton, E. Smith, Public views of the UK media and government reaction to the 2009 swine flu pandemic. BMC Public Health 10, 697 (2010)
Y. Liu, J. Ji, Q. Xie, J. Wang, H. Shang, C. Chen, F. Chen, C. Xue, Y. Cao, J. Ma, Y. Bi, Isolation and complete genomic characterization of H1N1 subtype swine influenza viruses in southern China through the 2009 pandemic. Virol. J. 8, 129 (2011)
U. Roll, R. Yaari, G. Katriel, O. Barnea, L. Stone, E. Mendelson, M. Mandelboim, A. Huppert, Onset of a pandemic: characterizing the initial phase of the swine flu (H1N1) epidemic in Israel. BMC Infect. Dis. 11, 92 (2011)
P. LaRussa, Pandemic novel 2009 H1N1 influenza: what have we learned? Semin. Respir. Crit. Care. Med. 32, 393–399 (2011)
M.B. Pearce, J.A. Belser, K.V. Houser, J.M. Katz, T.M. Tumpey, Efficacy of seasonal live attenuated influenza vaccine against virus replication and transmission of a pandemic 2009 H1N1 virus in ferrets. Vaccine 29, 2887–2894 (2011)
W.L. Loeffen, N. Stockhofe, E. Weesendorp, D. van Zoelen-Bos, R. Heutink, S. Quak, D. Goovaerts, J.G. Heldens, R. Maas, R.J. Moormann, G. Koch, Efficacy of a pandemic (H1N1) 2009 virus vaccine in pigs against the pandemic influenza virus is superior to commercially available swine influenza vaccines. Vet. Microbiol. 152, 304–314 (2011)
D.J. Wang, D.A. Boltz, J. McElhaney, J.A. McCullers, R.J. Webby, R.G. Webster, No evidence of a link between influenza vaccines and Guillain-Barre syndrome-associated antiganglioside antibodies. Influ. Other Respir. Viruses (2011). doi:10.1111/j.1750-2659.2011.00294.x [Epub ahead of print]
J.F. Sadusk, G. Nesche, Influenza vaccine, Asian strain: reactions following its use in adults. Calif. Med. 87, 301–306 (1957)
W. Zhou, V. Pool, J.K. Iskander, R. English-Bullard, R. Ball, R.P. Wise, P. Haber, R.P. Pless, G. Mootrey, S.S. Ellenberg, M.M. Braun, R.T. Chen, Surveillance for safety after immunization: vaccine adverse event reporting system (VAERS)-United States, 1991–2001. MMWR Surveill. Summ. 52, 1–24 (2003)
W.E. Beyer, J.T. Van der Logt, R. van Beek, N. Masurel, Immunoglobulin G, A and M response to influenza vaccination in different age groups: effects of priming and boosting. J. Hyg. 96, 513–522 (1986)
Y. Hu, H. Jin, X. Du, C. Xiao, D. Luo, B. Wang, R. She, Effects of chronic heat stress on immune responses of the foot-and-mouth disease DNA vaccination. DNA Cell Biol. 26, 619–626 (2007)
A. Mishra, O.K. Hooda, G. Singh, S.K. Meur, Influence of induced heat stress on HSP70 in buffalo lymphocytes. J. Anim. Physiol. Anim. Nutr. 95, 540–544 (2011)
J.C. Peng, C. Hyde, S. Pai, B.J. O’Sullivan, L.K. Nielsen, R. Thomas, Monocyte-derived DC primed with TLR agonists secrete IL-12p70 in a CD40-dependent manner under hyperthermic conditions. J. Immunother. 29, 606–615 (2006)
J. Radons, G. Multhoff, Immunostimulatory functions of membrane-bound and exported heat shock protein 70. Exerc. Immunol. Rev. 11, 17–33 (2005)
C.Y. Su, K.Y. Chong, J. Chen, S. Ryter, R. Khardori, C.C. Lai, A physiologically relevant hyperthermia selectively activates constitutive hsp70 in H9c2 cardiac myoblasts and confers oxidative protection. J. Mol. Cell. Cardiol. 31, 845–855 (1999)
P.J. Tomasik, K. Sztefko, M. Pizon, The effect of short-term cold and hot exposure on total plasma ghrelin concentrations in humans. Horm. Metab. Res. 37, 189–190 (2005)
M. Yang, S. Hu, B. Wu, Y. Miao, H. Pan, S. Zhu, Ghrelin inhibits apoptosis signal-regulating kinase 1 activity via upregulating heat-shock protein 70. Biochem. Biophys. Res. Commun. 359, 373–378 (2007)
S. Sheriff, R. Joshi, L.A. Friend, J.H. James, A. Balasubramaniam, Ghrelin receptor agonist, GHRP-2, attenuates burn injury-induced MuRF-1 and MAFbx expression and muscle proteolysis in rats. Peptides 30, 1909–1913 (2009)
M. Kojima, H. Hosoda, Y. Date, M. Nakazato, H. Matsuo, K. Kangawa, Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature 402, 656–660 (1999)
H.M. McCormack, D.J. Horne, S. Sheather, Clinical applications of visual analogue scales: a critical review. Psychol. Med. 18, 1007–1019 (1988)
J.B. Li, A. Asakawa, K. Cheng, Y. Li, H. Chaolu, M. Tsai, A. Inui, Biological effects of obestatin. Endocrine 39, 205–211 (2011)
J.P. Camiña, M.C. Carreira, D. Micic, M. Pombo, F. Kelestimur, C. Dieguez, F.F. Casanueva, Regulation of ghrelin secretion and action. Endocrine 22, 5–12 (2003)
M. Blatnik, C.I. Soderstrom, A practical guide for the stabilization of acylghrelin in human blood collections. Clin. Endocrinol. 74, 325–331 (2011)
H. Hosoda, K. Doi, N. Nagaya, H. Okumura, E. Nakagawa, M. Enomoto, F. Ono, K. Kangawa, Optimum collection and storage conditions for ghrelin measurements: octanoyl modification of ghrelin is rapidly hydrolyzed to desacyl ghrelin in blood samples. Clin. Chem. 50, 1077–1080 (2004)
L. Sibal, R.D. Neely, A. Jones, P.D. Home, Friedewald equation underestimates low-density lipoprotein cholesterol at low concentrations in young people with and without type 1 diabetes. Diabet. Med. 27, 37–45 (2010)
J.E. Cradock-Watson, M.S. Bourne, E.M. Vandervelde, IgG, IgA and IgM responses in acute rubella determined by the immunofluorescent technique. J. Hyg. 70, 473–485 (1972)
B. Lu, Y. Huang, L. Huang, B. Li, Z. Zheng, Z. Chen, J. Chen, Q. Hu, H. Wang, Effect of mucosal and systemic immunization with virus-like particles of severe acute respiratory syndrome coronavirus in mice. Immunology 130, 254–261 (2010)
R.A. Manz, A.E. Hauser, F. Hiepe, A. Radbruch, Maintenance of serum antibody levels. Annu. Rev. Immunol. 23, 367–368 (2005)
R.A. Manz, A. Radbruch, Plasma cells for a lifetime? Eur. J. Immunol. 32, 923–927 (2002)
E. El Eter, A. Al Tuwaijiri, H. Hagar, M. Arafa, In vivo and in vitro antioxidant activity of ghrelin: attenuation of gastric ischemic injury in the rat. J. Gastroenterol. Hepatol. 22, 1791–1799 (2007)
D.E. Flanagan, M.L. Evans, T.P. Monsod, F. Rife, R.A. Heptulla, W.V. Tamborlane, R.S. Sherwin, The influence of insulin on circulating ghrelin. Am. J. Physiol. Endocrinol. Metab. 284, 313–316 (2003)
T. Shiiya, M. Nakazato, M. Mizuta, Y. Date, M.S. Mondal, M. Tanaka, S. Nozoe, H. Hosoda, K. Kangawa, S. Matsukura, Plasma ghrelin levels in lean and obese humans and the effect of glucose on ghrelin secretion. J. Clin. Endocrinol. Metab. 87, 240–244 (2002)
F. Broglio, P. Koetsveld Pv, A. Benso, C. Gottero, F. Prodam, M. Papotti, G. Muccioli, C. Gauna, L. Hofland, R. Deghenghi, E. Arvat, A.J. Van Der Lely, E. Ghigo, Ghrelin secretion is inhibited by either somatostatin or cortistatin in humans. J. Clin. Endocrinol. Metab. 87, 4829–4832 (2002)
S. Corbetta, M. Peracchi, V. Cappiello, A. Lania, E. Lauri, L. Vago, P. Beck-Peccoz, A. Spada, Circulating ghrelin levels in patients with pancreatic and gastrointestinal euroendocrine tumors: identification of one pancreatic ghrelinoma. J. Clin. Endocrinol. Metab. 88, 3117–3120 (2003)
J.A. Strickertsson, K.B. Døssing, A.J. Aabakke, H.O. Nilsson, T.V. Hansen, U. Knigge, A. Kjær, T. Wadström, L. Friis-Hansen, Interferon-γ inhibits ghrelin expression and secretion via a somatostatin-mediated mechanism. World J. Gastroenterol. 17, 3117–3125 (2011)
Acknowledgments
The authors wish to thank all the participants, and the Firat University Research Grands Unite (FUBAP), which supported this research (Project Number 2039).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Aydin, S., Guven, T., Sahin, İ. et al. The effects of fever on hormone ghrelins, immunoglobulins, and heat shock protein 70 expression after swine flu vaccinations. Endocrine 42, 352–358 (2012). https://doi.org/10.1007/s12020-012-9664-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-012-9664-5