
Abstract
High fluoride exposures can lead to adverse effects such as dental and bone fluorosis, as well as endocrine and cognitive developmental problems. Water is the main dietary source of this ion, although significant concentrations have also been detected in other beverages widely consumed by the population such as soft drinks. A total of 200 soft drink samples (60 flavoured, 70 extracts, 60 fruit juice and 10 soft drinks) were analysed by fluoride ion selective potentiometry. A consumption of 330 mL was estimated for exposure assessment and subsequent F-risk assessment by soft drink consumption. The highest average concentration was found in extract soft drinks (2.45 ± 1.15 mg/L), followed by flavoured (1.71 ± 2.29 mg/L) and carbonated soft drinks (1.38 ± 0.40 mg/L), while the lowest was found in fruit juice soft drinks (1.09 ± 0.62 mg/L). The flavours with the highest concentration were tea-melon and tea-passion fruit with 3.66 ± 0.40 and 3.17 ± 0.56 mg/L respectively and the lowest was lemon flavour with 0.69 mg/L. The contribution of these beverages, considering the UL (Upper level) reference values set by EFSA (European Food Safety Authority) are between 3.28–41.78%, depending on age group and sex.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The concept of soft drink, as defined by Royal Decree 650/2011 of 9 May, is "soft drinks, carbonated or not, prepared with water for human consumption, prepared waters, natural mineral water or spring water, containing one or more of the following ingredients; carbon dioxide, sugars, …, flavourings or other food ingredients" [1]. Given the ambiguity of this description, soft drinks consist of a large amalgam of products that are very heterogeneous from one another, with the only commonality being water and sugar as the main ingredients.
Given its wide distribution and high consumption [2,3,4], these types of beverages have been subjected to numerous studies [5,6,7,8,9]. However, few studies have been carried out on their fluoride content and the corresponding toxicological risk assessment [10], although the main dietary sources of this anion include water, the main ingredient, and tea [11]. In addition, fluoride can also be found in other ingredients such as vegetable extracts [12], present in these beverages.
No adverse effects have been detected due to deficiency in fluoride intake, which is why bodies such as the EFSA do not consider this anion to be an essential element. However, dietary exposure to certain levels of fluoride may be beneficial as discussed above [11, 13]. Fluoride is incorporated into the tooth enamel during its formation, promoting its mineralisation, creating fluorohydroxyapatite, which is more resistant than the conventional hydroxyapatite structure and less vulnerable to demineralisation caused by acidogenic bacteria. This process can also occur after the enamel has been formed by topical incorporation [11, 14,15,16,17].
On the other hand, the presence of fluoride in saliva and tooth surface promotes the inhibition of different enzymatic mechanisms of acidogenic bacteria. Fluoride is not able to pass through the cell wall in its ionic form, but HF can, so when these microorganisms metabolise carbohydrates producing acids, they generate the ideal conditions for the formation of hydrofluoric acid. Once in the cytoplasm, this acid dissociates and is able to inhibit different enzymatic mechanisms, mainly glycolytic, affecting in particular the functioning of enolase and therefore reducing the production of hydrofluoric acid [11, 15, 18].
Just as dietary exposure to fluoride positively affects dental health, it also promotes better bone condition. Fluoride is one of the few agents known to stimulate osteoblast proliferation, which increases mineral deposition in these tissues. A denser bone structure makes it more resistant to fracture and degradation by osteoclasts [11, 14, 15].
However, fluoride has a hormone-like character, i.e. adequate exposure is good for health, but high exposure leads to adverse effects. The best known is dental fluorosis which is characterised by brown mottling of the teeth due to abnormal mineralisation caused by decreased protease activity and apoptosis of ameloblasts and odontoblasts [19]. This results in the appearance of gaps in the crystalline structure, increasing the porosity of the tooth and retaining part of the proteins responsible for enamel formation. Dental fluorosis occurs mainly during tooth formation and is irreversible, so special care must be taken to prevent fluoride exposure in infants from birth to 8 or 10 years of age [11, 14, 15, 20, 21]. In addition, excess fluoride in the oral cavity can lead to the formation of calcium fluoride from hydroxyapatite [22].
The most important chronic effect is bone fluorosis, however, cases in which this is attributed exclusively to dietary exposure are rare, although it has been reported in China [23]. This condition favours the deposition of calcium in the bone structure, increasing its density, as well as producing calcification of ligaments and cartilage and excessive bone growth, even leading to the union of vertebrae. Its symptoms include joint pain and limited movement, and it also hinders the recovery of fractures, due to the increased activity of calcineurin, which inhibits the functioning of osteoclasts. However, it can also lead to the development of osteoporosis and osteomalacia under conditions of lower Ca levels [21, 23, 24].
Overexposure to fluoride has been shown to lead to adverse effects on the endocrine system, such as an overactivity of the parathyroid gland, as well as an increase in alkaline phosphatase activity and calcineurin activity. Increased parathyroid hormone concentrations have been reported. This abnormal activity of the gland causes hyperplasia, degeneration and damage to the genetic material [23, 25].
It also affects both the male and female reproductive systems. In the former case through reduced oestradiol (E2) production and decreased activity of 3β-hydroxysteroid dehydrogenase (3β-HSD) and 17β-hydroxysteroid dehydrogenase (17β-HSD). In the male reproductive system, there is decreased mRNA expression of follicle stimulating hormone receptor (FSHR), luteinising hormone receptor (LHR), sex hormone binding globulin (SHBG), α-inhibin (INHα) and β-inhibin (INHβ) in the testes, as well as a reduction in the size of the testes [25].
Poor thyroid function during the early stages of life can lead to underdevelopment of the central nervous system, as has been shown in different studies correlating increased exposure to fluoride and endemic fluorosis with lower IQ in school-age populations in China, Mexico, Canada, etc. [25,26,27,28,29,30]. Prenatal exposure to high concentrations of fluoride has also been reported as a critical stage in the development of this deficiency, mainly among male individuals [24, 29]. The stage of embryogenesis is the stage of major brain development and growth, during which the proper functioning of glutamate transporter proteins, which are affected by high fluoride exposure, is crucial, and inhibition of the thyroid during this process alters early neuronal migration in the developing foetus [31].
The proper functioning of the pancreas may also be altered, as studies have reported a correlation between chronic administration of fluoride to rats and an inhibition of insulin production, which may lead to hyperglycaemia [25]. As for the adrenal gland, although few studies have been conducted, it is believed that fluoride inhibits dehydrogenase activity and cortisol production, leading to cortisaemia, which are essential for the synthesis of steroid hormones such as progesterone, glucocorticoids, mineralocorticoids, androgens and oestrogens. In addition, lesions in the proximal convoluted tubule have been reported [25, 32, 33].
It has been confirmed that fluoride generates an increase in peroxidised and radical species, leading to an increase in oxidative stress and thus causing tissue damage. This is due to the ability of this anion to bind to various enzymes, including antioxidant enzymes such as superoxide dismutase, catalase, glutathione peroxidase, glutathione reductase and superoxide dismutase, reducing their activity [34, 35]. The genotoxic potential of F- is also attributable to this oxidative stress and its ability to form covalent bonds with DNA, and this accumulation of radical species in the cytoplasm alters the proper functioning of proteins and organelles such as the endoplasmic reticulum and mitochondria [25, 35].
There is evidence that this anion can interfere with the proper functioning of mitochondria by decreasing cellular respiration and thus ATP production. The excessive presence of fluoride causes a change in membrane potential and the release of cytochrome C and induces the production of radical species in the organelle, which is the main producer of these molecules, which under normal circumstances should be eliminated [25, 35, 36].
Drinking water is the main source of fluoride in the diet, this anion is incorporated into groundwater due to the filtration of this anion by contaminated soils and mainly due to the contact of these waters with rocks and minerals that carry this anion. This contamination is favoured by different factors, such as a higher acidity and alkalinity, which allows the fluoride contained in the fluorite to be released through the formation of calcium carbonate, as well as that of the Al-F complexes through the exchange between hydroxide and fluoride ions. Volcanic soils have a low concentration of calcium, which allows a higher concentration of fluoride in the equilibrium [21, 37,38,39,40].
This is why regions such as mainland Spain have low concentrations of fluoride in drinking water, while in the Canary Islands concentrations of < LOQ to > 1.5 mg/L have been recorded, with occasional restrictions on consumption being established for part of the population [41,42,43]. On the other hand, a study carried out in the United Arab Emirates has detected concentrations of 0.04 to 0.28 mg/L [44], studies carried out in India show concentrations of 0.38 to 3.97 mg/L [45,46,47,48]. At the global level, concentrations found in Bangladesh (2.32 mg/L), China (14.10 mg/L), Indonesia (4.20 mg/L), Serbia (11 mg/L), Iran (9.20 mg/L), South Korea (40.8 mg/L), South Africa (15.2 mg/L), Kenya (25 mg/L), Turkey (13.7 mg/L), Norway (8.26 mg/L), Canada (15.1 mg/L) or Vietnam (28.1 mg/L) among others, also stand out [40, 49, 50].
Soft drinks, being made from various ingredients and being a product widely consumed by all population groups, could be an important source of fluoride in the diet. For these reasons, the objectives of this work are 1) to determine the fluoride concentration in soft drink samples, 2) to assess dietary fluoride exposure from soft drink consumption, and 3) to assess the risk and nutritional intake of fluoride from soft drink consumption.
Material and Methods
Sampling and Pre-treatment
A total of 200 samples of soft drinks of different characteristics were analysed; 60 flavoured, 70 extracts, 60 fruit juice and 10 soft drinks and flavours; 40 cola, 10 strawberry, 20 lemon-lime, 10 passion fruit, 10 peach, 30 tea-lemon, 20 tea-mango-pineapple, 30 lemon and 30 orange (Table 1).
The Carbonated soft drinks were treated with ultrasounds for 10 min to avoid interferences on the measure. Three aliquots were taken from each sample, in plastic containers with a 25:5 mL proportion of sample: conditioning solution.
Fluoride Determination
Fluoride determination was performed by fluoride ion selective potentiometry using the HACH SensION-MM340 potentiometer (HACH, Düsseldorf, Germany) and the HACH ISE F-9655C fluoride ion selective electrode (HACH, Düsseldorf, Germany). The instrumental parameters are: measuring range (0.01–19000 mg/L), pH range (4–8), linear range (0.1–19,000 mg/L), slope (59 mV/pF), working temperature (5-50ºC) and possible interferences, eliminated with the conditioning solution (Fe3+ and Al3+).
For this determination it was necessary to prepare 0.75 M orthophosphoric acid as a conditioning solution [51], prepared from 85% concentrated orthophosphoric acid (Honeywell-Fluka, Germany). And a calibration line for fluoride (10–5, 10–4, 10–3, 10–2, 10–1 M) in the conditioning solution, prepared from NaF of analytical purity (Merck, Germany).
Quality Control of the Method and Validation
The precision of the method was evaluated under reproducibility conditions using the standard addition method. Once the F− concentration of the samples was determined, a known amount of fluoride was added. The repeatability values in terms of relative standard deviation (RSD) were 2.40% with a reproducibility of 3.20%. The recovery rate was 85.61% with an RSD of less than 12%. The values were adequate and the recovery rate was satisfactory.
Statistical Analysis
A statistical analysis of the results obtained was carried out to determine the existence of significant differences (p < 0.05) between the different samples according to flavours and types of soft drinks. Using GraphPad Prism 9.0.2. software (GraphPad Software, USA), since the data did not follow a normal distribution, non-parametric independent variable tests (Kruskal–Wallis, Mann–Whitney) were performed.
Calculation of Dietary Intake and Exposure Assessment
Dietary exposure and subsequent assessments were based on obtaining the estimated daily intake, EDI (Eq. 1) and its subsequent comparison with EFSA reference values (Table 2), through the percentage contribution (Eq. 2), to both the Adequate Intake and Tolerable Upper Intake Level, AI and UL respectively.
Results and Discussion
Fluoride Content
The results obtained for each of the sample groups are shown in the following figures (Figs. 1 and 2). The highest fluoride concentrations were found in the strawberry flavour samples (3.94 ± 4.27 mg/L), followed by peach and passion fruit, 3.66 ± 0.40 mg/L and 3.17 ± 0.56 mg/L, respectively (Fig. 1). While the lowest concentrations were found in Lemon flavour (0.69 ± 0.24 mg/L), followed by cola and lemon-lime, 1.10 ± 0.58 mg/L and 1.21 ± 0.33 respectively, the latter considering the two categories of soft drink type where it has been studied.

Fluoride concentration (mg/L) by flavour

Fluoride concentration (mg/L) by trade description
Regarding the type of soft drink (Fig. 2), the highest concentration was recorded in extract soft drinks 2.45 ± 1.15 mg/L, while the lowest concentration was found in fruit juice soft drinks 1.09 ± 0.62.
These results highlight the influence of both the water used to manufacture these products and the different extracts and concentrates used. Since tea is a recognized dietary source of fluoride [11, 12, 41, 52] and the presence of concentrates of this plant in the extract-based beverages may be the reason why this category presents a higher concentration, considering that the geographical origin of the samples is diverse.
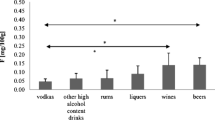
Studies on foods marketed on Tenerife Island, Spain, have found concentrations from 0.03 to 0.35 mg/L in wines[22], from 0.34 to 4 mg/L in tea [41], from 0.24 to 0.62 mg/L in bottled water [53], from 0.06 to 1.77 mg/L in beer [54], from 1.10 to 2.28 in cereals, from 0.01 to 0.99 in vegetables and from 0.32 to 1.05 in legumes [55].
While, studies of beers commercialized in the United Kingdom and Poland have found concentrations of 0.067 to 0.712 mg/L [56, 57], in Portugal concentrations of 0.40 mg/L have been found in both soft drinks and juices, as well as 0.12 and 0.16 mg/L in infusions and teas respectively [52], while in Mexico concentrations of 0.43 and 0.67 have been reported in soft drinks and juices respectively [58]. As can be seen in the present study higher concentrations have been reported in some types of soft drinks compared to the data collected by the authors previously mentioned.
Statistical Analysis among the Beverages Analysed
The hypotheses proposed in the previous section were made taking into account the results of the different statistical analyses carried out to determine the existence, or not, of significant differences between the variables studied; flavours (Table 3) and trade description (Table 4).
The difference between the different flavors (Table 4) emphasizes the importance not only of water, but also of tea extracts and concentrates and, to a lesser extent, those of other fruits and plants.
This influence becomes more evident when the different trade descriptions are compared. As the extract soft drinks are the only ones that contain tea and it is the only trade description with statistical differences in relation to the rest of the descriptions.
Fluoride Intake Assessment
0.33 L volume was established as ration content. Exposure, nutritional and risk assessment was performed for the different population groups using the equations that can be found in the Materials and Methods section.
Two different consumption scenarios were considered: 1 and 2 servings. Furthermore, it should be taken into account that the overall intake (water, coffee, vegetables, marine products, …) was not evaluated, but rather the dietary exposure due to a single product. For this reason, from percentages of contribution to the UL above 15–20% there could be concern about an excess in the intake of fluoride in the diet as a whole.
Scenario 1: Single Ration Intake (0.33 L/day)
The estimated daily intakes (EDI) of fluoride for a ration according to flavours and trade descriptions are shown in the following table (Table 5).
In all the cases studied, these beverages, under the established conditions, can be confirmed as a possible dietary source of fluoride with a percentage of Adequate Intake higher than 7.91% (Tables 6 and 7).
Regarding the percentages of contribution to the Tolerable Upper Intake Level (UL), as would be expected given the concentrations found, the flavors with the highest contribution are strawberry, passion fruit, peach and lemon tea (Table 8). These percentages are of concern in the population under 8 years old (> 30%) and under 14 years old, except for lemon tea (> 20%). In the remaining groups, the percentages of contribution to the UL are not relevant.
As for the contributions to the UL according to the trade name (Table 9), something similar to that previously mentioned occurs, where the population under 14 years of age presents percentages that are at least close to being considered problematic. Especially in extract soft drinks, where a contribution of 54.01% has been measured for children under 3 years of age.
Scenario 2: Two Rations Intake (0.66 L/day)
The fluoride estimated daily intakes (EDI) for two rations (two cans) according to flavours and trade descriptions are shown in Table 10.
In order to avoid the overcrowding of tables, to make the document easier and clearer to read and since the first scenario proposed has shown the effectiveness of soft drinks as a nutritional source of fluoride, it has been decided to not include the tables with the percentages of contribution to AI in a consumption scenario of 0.66 L/day.
When increasing the intake, it is observed that except for the Lemon flavour, all the age groups present contribution percentages to the UL higher than 10%, with the most relevant flavors being strawberry, passion fruit, peach and lemon tea, where for all the Age groups this percentage is higher than 20%. Furthermore, Strawberry, Passion fruit and Peach exceed or are close to 100% for the under 8-year-old population (Table 11).
Regarding the trade description, the population group under 8 years old presented contribution percentages higher than 30% for all product descriptions; however, only soft drinks based on extracts presented contributions that could pose a risk for the population over 15 years old (Table 12).
These results are of great interest and allow us to advance in the establishment of a global intake assessment that would consider all the possible fluoride dietary sources. This is a small contribution in this collective endeavour that aims to preserve the health of citizens and improve their life quality.
Conclusions
It has been hypothesized that the fluoride content found in soft drinks depends not only on water but is largely determined by the presence of other ingredients such as tea extracts. Extract-based soft drinks stand out for their higher fluoride concentration.
The concentrations of fluoride found in the foods analysed, and the subsequent nutritional assessment, allow us to affirm that these foods are a nutritional source of fluoride. Considering the concentrations of F− found, and the risk assessment derived from these, their consumption is not recommended for population younger than 3 years old. It is advisable to moderate consumption in the population from 4 to 8 years old, especially of beverages with tea extracts. According to the obtained results, teenagers and adults are not at risk for fluoride dietary exposure from soft drink consumption, as long as they follow a responsible consumption pattern.
References
Gobierno de España (2011) Real Decreto 650/2011 de 9 de mayo, por el que se aprueba la reglamentación técnico-sanitaria en materia de bebidas refrescantes. BOE 119:50089–50093
MAPA (2022) Informe consumo de bebidas fuera del hogar. Ministerio de Agricultura Pesca y Alimentación, Madrid, Spain. Available online: https://www.mapa.gob.es/es/alimentacion/temas/consumo-tendencias/consumo-extradom-bebidas-2022-anual_tcm30-624305.xlsx
MAPA (2021) Informe consumo de bebidas fuera del hogar. Ministerio de Agricultura, Pesca y Alimentación, Madrid, Spain. Available online: https://www.mapa.gob.es/es/alimentacion/temas/consumo-tendencias/consumo-extradom-bebidas-ano-2021_tcm30-565996.xlsx
MAPA (2022) Base de datos de consumo en hogares. Ministerio de Agricultura, Pesca y Alimentación, Madrid, Spain. Available online: https://www.mapa.gob.es/app/consumo-en-hogares/resultado1.asp
Gardener H, Rundek T, Markert M, Wright CB, Elkind MS, Sacco RL (2012) Diet soft drink consumption is associated with an increased risk of vascular events in the Northern Manhattan Study. J Gen Intern Med 27:1120–1126. https://doi.org/10.1007/s11606-011-1968-2
Gallus S, Turati F,Tavani A, Polesel J, Talamini R, Franceschi S, La Vecchia C (2011) Soft drinks, sweetened beverages and risk of pancreatic cancer. Cancer Causes Control 22:33–39. Available online: http://www.jstor.org/stable/41485358
Lee JG, Messer LB (2010) Intake of sweet drinks and sweet treats versus reported and observed caries experience. Eur Arch Paediatr Dent 11:5–17. https://doi.org/10.1007/BF03262704
Greenwood DC, Threapleton DE, Evans CEL, Cleghorn CL, Nykjaer C, Woodhead C, Burley VJ (2014) Association between sugar-sweetened and artificially sweetened soft drinks and type 2 diabetes: systematic review and dose–response meta-analysis of prospective studies. Br J Nutr 112:725–734. https://doi.org/10.1017/S0007114514001329. Available online: https://www.cambridge.org/core/article/association-between-sugarsweetened-and-artificially-sweetened-soft-drinks-and-type-2-diabetes-systematic-review-and-doseresponse-metaanalysis-of-prospective-studies/C69825BDE14CE0DE9AB7FF2026D18D1B (accessed on 2022/08/18)
Narain A, Kwok CS, Mamas MA (2016) Soft drinks and sweetened beverages and the risk of cardiovascular disease and mortality: a systematic review and meta-analysis. Int J Clin Pract 70:791–805. https://doi.org/10.1111/ijcp.12841
Rodríguez I, Hardisson A, Paz S, Rubio C, Gutiérrez AJ, Jaudenes JR, Burgos A, Revert C (2018) Fluoride intake from the consumption of refreshment drinks and natural juices. Journal of Food Composition and Analysis 72:97–103. https://doi.org/10.1016/j.jfca.2018.06.004. Available online: https://www.sciencedirect.com/science/article/pii/S0889157518303533
EFSA (2013) Scientific Opinion on Dietary Reference Values for fluoride. EFSA Panel Diet Prod Nut Allergies (NDA) 11:3332
Rocha Barrasa RA, Devesa i Pérez V, Vélez Pacios D (2013) Fluoruro en alimentos: contenidos, bioaccesibilidad y absorción por el epitelio intestinal. Doctoral Dissertation, Universitat Politècnica de València, Spain
World Health Organization (2017) Guidelines for Drinking-water Quality. Switzerland, WHO Library Cataloguing
ADA Position of the American Dietetic Association (2005) The Impact of Fluoride on Health. J Am Diet Assoc 105:1620–1628
Revelo-Mejía IA, Hardisson A, Rubio C, Gutiérrez ÁJ, Paz S (2021) Dental Fluorosis: the Risk of Misdiagnosis—a Review. Biol Trace Elem Res 199:1762–1770. https://doi.org/10.1007/s12011-020-02296-4
Opydo-Szymaczek J, Ogińska M, Wyrwas B (2021) Fluoride exposure and factors affecting dental caries in preschool children living in two areas with different natural levels of fluorides. J Trace Elem Med Biol 65:126726. https://doi.org/10.1016/j.jtemb.2021.126726. Available online: https://www.sciencedirect.com/science/article/pii/S0946672X2100016X
Singh A, Singh J (2021) Chapter 1-Effects on human health due to fluoride. In: Hadi Dehghani M, Karri R, Lima E (eds) Green technologies for the defluoridation of water. Elsevier, Amsterdam, pp 1–16
Miller FY, Campus G, Giuliana G, Piscopo MR, Pizzo G (2012) Topical Fluoride for Preventing Dental Caries in Children and Adolescents. Curr Pharm Des 18:5532–5541
Sellami M, Riahi H, Maatallah K, Ferjani H, Bouaziz MC, Ladeb MF (2020) Skeletal fluorosis: don’t miss the diagnosis! Skeletal Radiol 49:345–357. https://doi.org/10.1007/s00256-019-03302-0
Kashyap SJ, Sankannavar R, Madhu GM (2021) Fluoride sources, toxicity and fluorosis management techniques – A brief review. J Hazard Mater Lett 2:100033. https://doi.org/10.1016/j.hazl.2021.100033. Available online: https://www.sciencedirect.com/science/article/pii/S2666911021000216
Jha SK, Mishra VK, Sharma DK, Damodaran T (2011) Chapter fluoride in the environment and its metabolism in humans. In: Whitacre DM (ed) Reviews of environmental contamination and toxicology, vol 211. Springer New York, New York, NY, pp 121–142
Paz S, Jaudenes JR, Gutiérrez AJ, Rubio C, Hardisson A, Revert C (2017) Determination of Fluoride in Organic and Non-organic Wines. Biol Trace Elem Res 178:153–159. https://doi.org/10.1007/s12011-016-0910-1
Mertz W (1986) Trace elements in human and animal nutrition, vol 1. Academic Press, Cambridge, MA
Zuo H, Chen L, Kong M, Qiu L, Lü P, Wu P, Yang Y, Chen K (2018) Toxic effects of fluoride on organisms. Life Sci 198:18–24. https://doi.org/10.1016/j.lfs.2018.02.001. Available online: https://www.sciencedirect.com/science/article/pii/S0024320518300456
Skórka-Majewicz M, Goschorska M, Żwierełło W, Baranowska-Bosiacka I, Styburski D, Kapczuk P, Gutowska I (2020) Effect of fluoride on endocrine tissues and their secretory functions -- review. Chemosphere 260:127565. https://doi.org/10.1016/j.chemosphere.2020.127565. Available online: https://www.sciencedirect.com/science/article/pii/S0045653520317604
Tang Q, Du J, Ma H, Jiang S, Zhou X (2008) Fluoride and Children’s Intelligence: A Meta-analysis. Biol Trace Elem Res 126:115–120. https://doi.org/10.1007/s12011-008-8204-x
Choi Anna L, Guifan S, Ying Z, Philippe G (2012) Developmental Fluoride Neurotoxicity: A Systematic Review and Meta-Analysis. Environ Health Perspect 120:1362–1368. https://doi.org/10.1289/ehp.1104912
Valdez-Jiménez L, Soria Fregozo C, Miranda Beltrán ML, Gutiérrez Coronado O, Pérez Vega MI (2011) Efectos del flúor sobre el sistema nervioso central. Neurología 26:297–300. https://doi.org/10.1016/j.nrl.2010.10.008. Available online: https://www.sciencedirect.com/science/article/pii/S0213485310003191
Farmus L, Till C, Green R, Hornung R, Martinez Mier EA, Ayotte P, Muckle G, Lanphear BP, Flora DB (2021) Critical windows of fluoride neurotoxicity in Canadian children. Environ Res 200:111315. https://doi.org/10.1016/j.envres.2021.111315. Available online: https://www.sciencedirect.com/science/article/pii/S0013935121006095
Till C, Green R, Flora D, Hornung R, Martinez-Mier EA, Blazer M, Farmus L, Ayotte P, Muckle G, Lanphear B (2020) Fluoride exposure from infant formula and child IQ in a Canadian birth cohort. Environ Int 134:105315. https://doi.org/10.1016/j.envint.2019.105315. Available online: https://www.sciencedirect.com/science/article/pii/S0160412019326145
Jiang C, Zhang S, Liu H, Guan Z, Zeng Q, Zhang C, Lei R, Xia T, Wang Z, Yang L, Chen Y, Wu X, Zhang X, Cui Y, Yu L, Wang A (2014) Low Glucose Utilization and Neurodegenerative Changes Caused by Sodium Fluoride Exposure in Rat’s Developmental Brain. NeuroMol Med 16:94–105. https://doi.org/10.1007/s12017-013-8260-z
Xiong, X.; Liu, J.; He, W.; Xia, T.; He, P.; Chen, X.; Yang, K.; Wang, A (2007) Dose–effect relationship between drinking water fluoride levels and damage to liver and kidney functions in children. Environ Res 103:112–116. https://doi.org/10.1016/j.envres.2006.05.008. Available online: https://www.sciencedirect.com/science/article/pii/S0013935106001265
Yang K, Liang X, Quan C (2019) In Fluoride in drinking water: effect on liver and kidney function. In: Nriagu J (ed) Encyclopedia of Environmental Health, 2nd edn. Elsevier, Oxford, pp 34–40
Shashi A, Thakur S (2022) Gene expression and alterations of antioxidant enzymes in spleen of rats exposed to fluoride. J Trace Elem Med Biol 72:126966. https://doi.org/10.1016/j.jtemb.2022.126966. Available online: https://www.sciencedirect.com/science/article/pii/S0946672X22000463
Miranda GHN, Ferreira MKM, Bittencourt LO, de Oliveira LLA, Puty B, Lima RR (2021) Chapter 17 - The role of oxidative stress in fluoride toxicity. In: Patel VB, Preedy VR (eds) Toxicology. Academic Press, pp 157–163. https://doi.org/10.1016/B978-0-12-819092-0.00017-0
Avila-Rojas SH, Aparicio-Trejo OE, Sanchez-Guerra MA, Barbier OC (2022) Effects of fluoride exposure on mitochondrial function: Energy metabolism, dynamics, biogenesis and mitophagy. Environ Toxicol Pharmacol 94:103916. https://doi.org/10.1016/j.etap.2022.103916. Available online: https://www.sciencedirect.com/science/article/pii/S1382668922001090
Rao NS (2008) Fluoride in groundwater, Varaha River Basin, Visakhapatnam District, Andhra Pradesh. India Environ Monit Assess 152:47. https://doi.org/10.1007/s10661-008-0295-5
Subba Rao N (2011) High-fluoride groundwater. Environ Monit Assess 176:637–645. https://doi.org/10.1007/s10661-010-1609-y
Sunitha V, Reddy YS, Suvarna B, Reddy BM (2022) Human health risk assessment (HHRA) of fluoride and nitrate using pollution index of groundwater (PIG) in and around hard rock terrain of Cuddapah, A.P. South India. Environ Chem Ecotoxicol 4:113–123. https://doi.org/10.1016/j.enceco.2021.12.002. Available online: https://www.sciencedirect.com/science/article/pii/S2590182621000357
Kaur A, Bala R, Bhinder SS, Kansal SK (2022) In: Ahamad A, Siddiqui SI, Singh P (eds) Chapter 5 - Health impacts due to fluoride contamination in water: current scenario; contamination of water; Academic Press, Cambridge, MA, pp 65–84
Rodríguez I, Burgos A, Rubio C, Gutiérrez AJ, Paz S, da Silva Rodrigues, Júnior Flavio M, Hardisson A, Revert C (2020) Human exposure to fluoride from tea (Camellia sinensis) in a volcanic region—Canary Islands, Spain. Environ Sci Pollut Res 27:43917–43928. https://doi.org/10.1007/s11356-020-10319-9
Vitoria I, Maraver F, Almerich-Silla JM (2014) Flúor en aguas de consumo público españolas y prevención de la caries dental. Gac Sanit 28:255–256. https://doi.org/10.1016/j.gaceta.2013.10.010. Available online: https://www.sciencedirect.com/science/article/pii/S021391111300201X
Rubio C, Rodríguez I, Jaudenes JR, Gutiérrez AJ, Paz S, Burgos A, Hardisson A, Revert C (2020) Fluoride levels in supply water from a volcanic area in the Macaronesia region. Environ Sci Pollut Res Int 27:11587–11595. https://doi.org/10.1007/s11356-020-07702-x. Available online: https://link.springer.com/article/10.1007/s11356-020-07702-x
Walia T, Abu Fanas S, Akbar M, Eddin J, Adnan M (2017) Estimation of fluoride concentration in drinking water and common beverages in United Arab Emirates (UAE). Saudi Dental J 29:117–122. https://doi.org/10.1016/j.sdentj.2017.04.002. Available online: https://www.sciencedirect.com/science/article/pii/S1013905217300342
Singh B, Gau S, Garg VK (2007) Fluoride in drinking water and human urine in Southern Haryana, India. J Hazard Mater 144:147–151. https://doi.org/10.1016/j.jhazmat.2006.10.010. Available online: https://www.sciencedirect.com/science/article/pii/S0304389406011964
Mridha D, Priyadarshni P, Bhaskar K, Gaurav A, De A, Das A, Joardar M, Chowdhury NR, Roychowdhury T (2021) Fluoride exposure and its potential health risk assessment in drinking water and staple food in the population from fluoride endemic regions of Bihar, India. Groundw Sustain Dev 13:100558. https://doi.org/10.1016/j.gsd.2021.100558. Available online: https://www.sciencedirect.com/science/article/pii/S2352801X2100014X
Amalraj A, Pius A (2013) Health risk from fluoride exposure of a population in selected areas of Tamil Nadu South India. Food Sci Hum Wellness 2:75–86. https://doi.org/10.1016/j.fshw.2013.03.005. Available online: https://www.sciencedirect.com/science/article/pii/S2213453013000165
Bhattacharya P, Adhikari S, Samal AC, Das R, Dey D, Deb A, Ahmed S, Hussein J, De A, Das A, Joardar M, Panigrahi AK, Roychowdhury T, Santra SC (2020) Health risk assessment of co-occurrence of toxic fluoride and arsenic in groundwater of Dharmanagar region, North Tripura (India). Groundw Sustain Dev 11:100430. https://doi.org/10.1016/j.gsd.2020.100430. Available online: https://www.sciencedirect.com/science/article/pii/S2352801X19303844
Yadav KK, Kumar S, Pham QB, Gupta N, Rezania S, Kamyab H, Yadav S, Vymazal J, Kumar V, Tri DQ, Talaiekhozani A, Prasad S, Reece LM, Singh N, Maurya PK, Cho J (2019) Fluoride contamination, health problems and remediation methods in Asian groundwater: A comprehensive review. Ecotoxicol Environ Saf 182:109362. https://doi.org/10.1016/j.ecoenv.2019.06.045. Available online: https://www.sciencedirect.com/science/article/pii/S0147651319306839
Mandinic Z, Curcic M, Antonijevic B, Lekic CP, Carevic M (2009) Relationship between fluoride intake in Serbian children living in two areas with different natural levels of fluorides and occurrence of dental fluorosis. Food Chem Toxicol 47:1080–1084 https://doi.org/10.1016/j.fct.2009.01.038. Available online: https://www.sciencedirect.com/science/article/pii/S027869150900057X
Delgado-Suárez I, Lozano-Bilbao E, Lozano G, Hardisson A, Rubio C, González-Weller D, Paz S, Gutiérrez ÁJ (2021) Characterization of classes of mollusks in the East Atlantic according to their element content. Environ Sci Pollut Res 28:30390–30398. https://doi.org/10.1007/s11356-021-14112-0. Available online: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85105442450&doi=10.1007%2fs11356-021-14112-0&partnerID=40&md5=525b6e5787d38572178161dd04db134a (accessed on 13 December 2021)
Fojo C, Figueira ME, Almeida CMM (2013) Fluoride content of soft drinks, nectars, juices, juice drinks, concentrates, teas and infusions marketed in Portugal. Null 30:705–712. https://doi.org/10.1080/19440049.2013.785636
Jáudenes Marrero JR, de la Torre Arturo H; Gutiérrez Fernández AJ, Rubio Armendáriz C, Revert Gironés C (2015) Evaluación del riesgo tóxico por la presencia de fluoruro en aguas de bebida envasada consumidas en Canarias. Nutrición hospitalaria: Organo Oficial de la Sociedad Española de Nutrición Parenteral y Enteral 32:2261–2268. https://doi.org/10.3305/nh.2015.32.5.9701. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0212-16112015001100048&lng=en&tlng=en
Jaudenes JR, Hardisson A, Paz S, Rubio C, Gutiérrez AJ, Burgos A, Revert C (2018) Potentiometric Determination of Fluoride Concentration in Beers. Biol Trace Elem Res 181:178–183. https://doi.org/10.1007/s12011-017-1029-8
Jaudenes JR, Gutiérrez ÁJ, Paz S, Rubio C, Hardisson A (2020) Fluoride risk assessment from consumption of different foods commercialized in a European Region. App Sci 10(18):6582. https://doi.org/10.3390/app10186582
Warnakulasuriya S, Harris C, Gelbier S, Keating J, Peters T (2002) Fluoride content of alcoholic beverages. Clin Chim Acta 320:1–4. https://doi.org/10.1016/S0009-8981(02)00043-8. Available online: https://www.sciencedirect.com/science/article/pii/S0009898102000438
Styburski D, Baranowska-Bosiacka I, Goschorska M, Chlubek D, Gutowska I (2017) Beer as a Rich Source of Fluoride Delivered into the Body. Biol Trace Elem Res 177:404–408. https://doi.org/10.1007/s12011-016-0888-8
Jiménez-Farfán MD, Hernández-Guerrero JC, Loyola-Rodríguez JP, Ledesma-Montes C (2004) Fluoride content in bottled waters, juices and carbonated soft drinks in Mexico City. Mexico. Int J Paediatr Dent 14:260–266. https://doi.org/10.1111/j.1365-263X.2004.00564.x
Acknowledgements
This research has been carried out within the framework of the Doctoral Programme in Medical and Pharmaceutical Sciences, Development and Quality of Life [Programa de Doctorado en Ciencias Médicas y Farmacéuticas, Desarrollo y Calidad de Vida] of the University of La Laguna.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by S.A-V., Á.J.G., S.P-M. and A.H. The first draft of the manuscript was written by S.A-V., C.R. and J.R.J-M. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alejandro-Vega, S., Hardisson, A., Rubio, C. et al. Soft Drinks as a Dietary Source of Fluoride Exposure. Biol Trace Elem Res 202, 3816–3828 (2024). https://doi.org/10.1007/s12011-023-03937-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-023-03937-0