
Abstract
The aim of this study was to comprehensively assess the prevalence of goiter and thyroid nodules (TNs) in relation to China’s iodine nutrition level over the past 20 years and provide an effective reference for developing health policies. PubMed, EMBASE, Chinese National Knowledge Infrastructure, Chongqing VIP, and Chinese Wan Fang databases were searched for relevant studies from Jan 1996 to Feb 2020. Two reviewers extracted valid data from the eligible citations to determine the morbidity of TNs in different urinary iodine concentrations (UICs) and in patients of different genders, of different ages, who live in different geographic regions, and who live at different altitudes, as well as the P values of interactions between groups. There were 26 articles (34 studies) included in this analysis. The overall morbidity of TNs in mainland China was 23.4%. Morbidity was higher in urban areas (P < 0.001) than in rural and mixed areas. Coastal areas (P < 0.001), female patients (P < 0.001), high-altitude areas (P < 0.001), and residence in south China (P < 0.001) were all associated with higher morbidity of TNs. The lowest morbidity value of TNs, 16%, was in the more-than-adequate iodine subgroup. The highest morbidity, 27.2%, was in the adequate iodine subgroup. The morbidity of TNs increases with age, and women are more likely to have TNs. We also need to perform more epidemiological studies, and in the future, we should cultivate better understanding of the relationship between other thyroid diseases and provide more comprehensive and useful information for other researchers.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Iodine is a trace element that plays an important role in the synthesis of the thyroid hormones thyroxin (T4) and triiodothyronine (T3), which are essential for life [1]. Normally, it involves impermanent shutdown of thyroid hormone synthesis in response to supraphysiologic iodine exposure, known as the acute Wolff–Chaikoff effect [2]. In 1990, the World Health Organization (WHO) found that 2.2 billion people in 130 countries were at risk of iodine deficiency disorder (IDD). Adequate intake of iodine is vitally important for synthesizing thyroid hormones and minimizing the risk of thyroid disease in adults. In light of WHO recommendations, urinary iodine concentration (UIC) was used to estimate iodine status in populations, which is recommended to be between 100 and 199 μg/L in schoolchildren and adults. There is also great concern that excess iodine, like iodine deficiency, may have negative effects on thyroid function [3]. A 5-year prospective survey performed in China shows that excess iodine can induce and promote the incidence and development of hypothyroidism and autoimmune thyroiditis [4].
Thyroid nodules (TNs) are independent, structurally separate neoplasms within the thyroid gland [5], with 3–7% morbidity by palpation [6]; 20–76% are found by ultrasound [7], and 8.2–65% are not found until autopsy [8, 9]. In recent years, an increasing incidence of thyroid carcinoma has been reported in many countries [10,11,12,13]. The morbidity of thyroid carcinoma in patients with thyroid nodules can be as high as 15% [14].
China implemented universal salt iodization (USI) regulations to prevent IDDs in 1996, involving all 31 provinces of mainland China. In 2011, the standard of salt iodization concentration in China was adjusted to household salt iodine content of 20–30 mg/kg, and provinces were allowed to choose salt iodization concentrations according to local conditions. During the two decades in which USI standards have been used, the population of China has been consecutively exposed to an iodine nutrition status of excessive iodine intake from 1996 to 2001, more-than-adequate iodine intake from 2002 to 2011, and adequate iodine intake from 2012 to 2016 [15].
Thus, we here present a systematic review and meta-analysis to analyze the morbidity of TNs after enforcement of the USI project in mainland China over the course of two decades.
Materials and Methods
Literature Search Strategy
We artificially retrieved all of the literature concerning population-based studies on the morbidity of thyroid nodules from January 1996 to September 2020 making use of the PubMed, EMBASE, Chinese National Knowledge Infrastructure, Chongqing VIP, and Chinese Wan Fang databases. The keywords “thyroid disorder(s),” “thyroid nodule(s),” “TN(s),” and “iodine” or the terms “prevalence(s)” or “incidence(s),” or “epidemiology” and “China” or “Chinese” were used to search for relevant studies. We also checked the reference list of identified studies in order to find more additional studies.
Selection Criteria
Our inclusion criteria were as follows: (1) the people were from stochastic community-oriented samples rather than voluntary acceptors or patients undergoing routine medical examinations; (2) the research design was population-based rather than hospital-based; (3) research results covered enough information (e.g., research geographic region, survey methodology, number of cases, sample size, diagnostic criteria, and urinary iodine concentration).
Studies were removed if they met any of the following exclusion criteria: (1) case reports or reviews; (2) the people had any relevant sickness or took drugs or therapy known to influence thyroid structure or function; (3) the study centered on people in a specific subpopulation (such as smokers or gestational women) or who shared a specific career; (4) they were the same studies republished.
Data Extraction
Two reviewers separately extracted information, specifically the first author, the date of publication, the starting year of the work, age of the participants, geographic region, sample size, outcomes, and prevalence. The literature-retrieval process is shown in Fig. 1. Any differences were resolved by consensus. In our study, the median UIC was used to sort subjects into four subgroups: insufficient group (median UIC ≤ 99 μg/L); adequate group (median UIC between 100 and 199 μg/L); more-than-adequate group (median UIC between 200 and 299 μg/L); excessive group (median UIC ≥ 300 μg/L).

Flow diagram of the literature-search process
Statistical Analysis
We summarized the frequency of TNs along with 95% confidence intervals (CIs) to evaluate the morbidity of TNs in mainland China. The χ2-based 푄 test and the 퐼2 test were used to calculate the heterogeneity of the studies. The low, moderate, and high levels of heterogeneity were set as 25%, 50%, and 75%, respectively [16]. We used a random-effects meta-analysis model to replace the fixed-effects model. We used the Egger’s test to estimate for publication bias (P < .05 was considered of statistical significance) when the level of heterogeneity was moderate or high. Stata Version 16.0 (Stata Corp LP, TX, USA) was used to perform meta-analyses. We analyzed the differences in epidemiology among distinct groups utilizing the χ2 test in SPSS Version 23.0 (SPSS Software, Chicago, IL, USA).
Results
Literature Retrieval and Study Characteristics
A total of 1788 articles are initially planned to be included in this study, and 1654 were eliminated after screening the titles and abstracts. A total of 108 articles were excluded after more detailed evaluation. As a result, 26 articles (34 studies) [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42] were brought into this meta-analysis.
The characteristics of the 34 joined studies are listed in Table 1, based on general population samples. The total number of participants in the included studies was 72,319, from 16 provinces of mainland China, and including 18,189 cases with TNs after a diagnosis with ultrasound.
Pooled Morbidity of Thyroid Nodules
As shown in Fig. 2, averaged over the past two decades, the overall morbidity of TNs in mainland China was 23.4% (95% CI: 20.4–26.4%). The pooled morbidity of TNs before 2011 was 20% (95% CI: 15.5–24.4%); after 2011, the pooled morbidity was 26.1% (95% CI: 21.8–30.4%).

Forest plot of the pooled morbidity of TNs in mainland China
The subgroup morbidity of TNs in mainland China was analyzed as shown in Table 2. The pooled morbidity was higher in urban areas (χ2 = 351.88, P < 0.001) than in rural and mixed areas. Residence in a coastal area (χ2 = 429.62, P < 0.001), female gender (χ2 = 671.85, P < 0.001), residence at high altitude (χ2 = 56.953, P < 0.001), and residence in southern China (χ2 = 173.86, P < 0.001) might indicate higher morbidity of TNs.
In the four levels of iodine intake, the lowest level of morbidity of TNs was in the more-than-adequate iodine subgroup, 16% (95% CI: 12–20%). The highest level of morbidity was in the adequate iodine subgroup, 27.2% (95% CI: 23.531%).
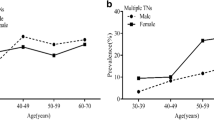
As shown Fig. 3, the morbidity of TNs increased with age, and the highest, 53.3%, was in the group over 60 years old (95% CI: 42.5–64.2%). The lowest morbidity of TNs, 13.8%, was observed in the under-20-year-old group (95% CI: 7.2–20.4%). The morbidity of TNs was 24.2% in the 21–40-year-old group (95% CI: 16.7–31.7%) and 0.38.3% in the 41–61-year-old group (95% CI: 28.7–42.9%). The conditions of the provinces and municipalities are shown in themaps in Fig 4.

Morbidity of TNs with different ages

Regional distribution of pooled morbidity of TNs in mainland China
Evaluation of Potential Bias
For the estimated overall incidence of TNs, we did not detect any significant publication bias using the Egger’s test. The funnel plot was shown in Fig 5.

Funnel plot with pseudo 95% confidence limits
Discussion
Thyroid nodules are frequently found in the thyroid gland. Because small nodules can be detected by ultrasound, the morbidity of TNs has been reported as high as 67% in the general population [43]. Because approximately 10–15% of nodules are cancerous, TNs should be observed closely in clinical practice [44, 45].
In our study, on the basis of the inclusion and exclusion criteria, a total of 26 original epidemiological studies were included in this study. After the merger, the sample size reached 18,189 cases and 72,319 patients with TNs, covering 16 provinces. Through a systematic review and meta-analysis of these previous works, an updated estimate of the overall morbidity of TNs was obtained.
The morbidity of TNs in China has been rising over the past 20 years, from 2.73% in 1999 to 17.50% in 2010, and the morbidity rate in 2017 reached 20.43% [46]. The results of our meta-analysis revealed that the morbidity of TNs in mainland China was 23.4%. In the years 2012–2020, the morbidity of TNs was greater than in the years 1999–2011. Teng et al. showed that the morbidity of TNs was 20.43%, which was very high. Furthermore, they also determined that the morbidity of TNs decreased with increases in iodine intake, suggesting that insufficient iodine is a risk factor for TNs and that adequate iodine and more-than-adequate iodine are protective factors for TNs [15]. They supported the conclusion that AI and MAI could be merged as an indicator of an optimal iodine intake for the general population, that is, iodine intake within the range of 100–299 μg/L. But the WHO reported that the optimal urinary iodine concentration was 100–200 μg/L, corresponding approximately to a daily intake of 150–300 μg for adults. We find the optimal median range of urinary iodine recommended by the WHO may need to be broadened. The incidence of TNs and iodine intake formed U-shaped curves, indicating that insufficient and excessive iodine intake both increase the morbidity of TNs. A study from South Korea showed that when the range of UIC was 100–199 μg/L, the morbidity rate of TNs was highest, reaching 19.4%, while the morbidity of TNs decreased with the increase of iodine intake, which further proves that the more-than-adequate iodine is the protective factor of thyroid nodules [47]. In our study, more-than-adequate iodine intake had the lowest morbidity of TNs. Our results are consistent with those of previous studies [15, 39].
Several articles have shown that high-resolution thyroid ultrasound can allow discovery of TNs in 19–68% of stochastically specific individuals, with more women and the elderly suffering from TNs [7, 48]. In our study, a subgroup analysis was carried out by gender, and the morbidity of TNs in males was 18% and 27.6% in females. Women were found to be more likely to experience higher morbidity of TNs than men, which is consistent with the results of earlier studies [49,50,51]. Possible reasons for this are as follows: (1) thyroid growth factors are susceptible to sex hormones, such as estrogen [52] and 17 beta-estradiol, so women are more likely to be diagnosed with thyroid disease than men [53]. (2) It may also be related to the increased demand for thyroxine during menstruation, pregnancy, and other factors that lead to periodic endocrine changes [54]. According to the subgroup analysis of different ages, as age increases, the morbidity of TNs gradually increases. This may be related to hypothyroidism, dyslipidemia, hormone levels, and other factors. It also indicates that age is one of the factors affecting the occurrence of TNs [55]. We also found high altitude, urban location, and coastal location to be correlated with TNs. Plateau and coastal environments were found to be associated with higher rates of TNs. This finding is similar to that observed for previous studies, and it may be caused by insufficient iodine intake at high altitudes. Excessive iodine in coastal areas necessitates education and economic remedies for the residents who live there [56, 57].
There are two limitations to this research. First, the studies included here covered 16 provinces, mainly in eastern China. Second, we rightly limited the research to mainland China, considering no other countries.
Conclusion
Our research shows that it is beneficial to formulate iodized salt standards according to local conditions, but there may be some dangerous factors, and these must be considered with care. We need to perform more epidemiological studies, and in the future, we should develop further understanding of the relationship between other thyroid diseases and provide more comprehensive and useful information for other researchers.
Data Availability
All data used during the study appear in the submitted article and availability.
References
Andersson M, Karumbunathan V, Zimmermann MB (2012) Global iodine status in 2011 and trends over the past decade. J Nutr 142:744–750
Leung AM, Braverman LE (2014) Consequences of excess iodine. Nat Rev Endocrinol 10:136–142
Zimmermann MB (2009) Iodine deficiency. Endocr Rev 30:376–408
Shan Z, Chen L, Lian X, Liu C, Shi B, Shi L, Tong N, Wang S, Weng J, Zhao J, Teng X, Yu X, Lai Y, Wang W, Li C, Mao J, Li Y, Fan C, Teng W (2016) Iodine status and prevalence of thyroid disorders after introduction of mandatory universal salt iodization for 16 years in China: a cross-sectional study in 10 cities. Thyroid 26:1125–1130
Hegedus L (2004) Clinical practice. The thyroid nodule. N Engl J Med 351:1764–1771
Singer PA, Cooper DS, Daniels GH, Ladenson PW, Greenspan FS, Levy EG, Braverman LE, Clark OH, McDougall IR, Ain KV, Dorfman SG (1996) Treatment guidelines for patients with thyroid nodules and well-differentiated thyroid cancer. American Thyroid Association. Arch Intern Med 156:2165–2172
Tan GH, Gharib H (1997) Thyroid incidentalomas: management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann Intern Med 126:226–231
Mortensen JD, Woolner LB, Bennett WA (1955) Gross and microscopic findings in clinically normal thyroid glands. J Clin Endocrinol Metab 15:1270–1280
Hull OH (1955) Critical analysis of two hundred twenty-one thyroid glands; study of thyroid glands obtained at necropsy in Colorado. AMA Arch Pathol 59:291–311
Colonna M, Grosclaude P, Remontet L, Schvartz C, Mace-Lesech J, Velten M, Guizard A, Tretarre B, Buemi AV, Arveux P, Esteve J (2002) Incidence of thyroid cancer in adults recorded by French cancer registries (1978-1997). Eur J Cancer 38:1762–1768
Montanaro F, Pury P, Bordoni A, Lutz JM, N Swiss Cancer Registries (2006) Unexpected additional increase in the incidence of thyroid cancer among a recent birth cohort in Switzerland. Eur J Cancer Prev 15:178–186
Labarge B, Walter V, Lengerich EJ, Crist H, Karamchandani D, Williams N, Goldenberg D, Bann DV, Warrick JI (2018) Evidence of a positive association between malpractice climate and thyroid cancer incidence in the United States. PLoS One 13:e0199862
Cong S, Fang LW, Bao HL, Feng YJ, Wang N, Yin P, Li YC, Duan XN, Zhou MG (2016) Disease burden of thyroid cancer in the Chinese population, in 1990 and 2013(Article in Chinese). Zhonghua Liu Xing Bing Xue Za Zhi 37:773–777
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L (2016) 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 26:1–133
Li Y, Teng D, Ba J, Chen B, Du J, He L, Lai X, Teng X, Shi X, Li Y, Chi H, Liao E, Liu C, Liu L, Qin G, Qin Y, Quan H, Shi B, Sun H, Tang X, Tong N, Wang G, Zhang JA, Wang Y, Xue Y, Yan L, Yang J, Yang L, Yao Y, Ye Z, Zhang Q, Zhang L, Zhu J, Zhu M, Ning G, Mu Y, Zhao J, Shan Z, Teng W (2020) Efficacy and safety of long-term universal salt iodization on thyroid disorders: epidemiological evidence from 31 provinces of mainland China. Thyroid 30:568–579
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Yu X, Fan C, Shan Z, Teng X, Guan H, Li Y, Teng D, Jin Y, Chong W, Yang F, Dai H, Yu Y, Li J, Chen Y, Zhao D, Shi X, Hu F, Mao J, Gu X, Yang R, Tong Y, Wang W, Gao T, Li C, Teng W (2008) A five-year follow-up study of goiter and thyroid nodules in three regions with different iodine intakes in China. J Endocrinol Investig 31:243–250
Zhu W, Liu X, Hu X, Zhou S, Wang Y, Zhang Y (2012) Investigation on the iodine nutritional status and the prevalence of thyroid carcinoma in Zhoushan Archipelago residents(Article in Chinese). Wei Sheng Yan Jiu 41:79–82
Lou X, Mo Z, Zhu W, Zhou J, Mao G, Wang X, Miu X, Ding G (2011) Thyroid nodule among populations with different levels of iodine nutrition (Article in Chinese). Chin J Public Health 27:3
Shao HJ, Li J, He XQ, Liu N, Li YH, Yan JJ, Qu XL, Yuan XY (2016) Prevalence Of nontoxic nodular goiter after a nearly two-decade universal salt iodization in a littoral region of Shandong Province, China. Acta Endocrinol (Buchar) 12:43–46
Liu Y, Min Z, Tong N, Lv Q, Huang H (2012) An epidemiological survey of thyroid diseases in a community-based population in Chengdu (Article in Chinese). Proceedings of the 11th Annual Meeting of Chinese Society of Endocrinology, pp 114
Yang Y, Shi L (2011) A survey of the prevalence of thyroid nodules in a community-based population in Guiyang (Article in Chinese). Proceedings of the 10th Annual Meeting of Chinese Society of Endocrinology, pp 162–163
Zou S, Wu F, Guo C, Song J, Huang C, Zhu Z, Yu H, Guo Y, Lu X, Ruan Y (2012) Iodine nutrition and the prevalence of thyroid disease after salt iodization: a cross-sectional survey in Shanghai, a coastal area in China. PLoS One 7:e40718
Shen Y, Zhang Y, Yuan H, Sun S, Tao M, Zhang Q, Wang Y, Pan G (2013) Survey of iodine nutritional status of the residents in Jiading District of Shanghai(Article in Chinese). China Trop Med 13:3
Yang N, Chen Y, Yang W, Bao X, Hao W, Zhou J (2012) A survey on iodine nutrition condition of residents in Jiaojiang District, Taizhou City, Zhejiang Province (article in Chinese). J Environ Occup Med 29:6
Chen Z, Xu W, Huang Y, Jin X, Deng J, Zhu S, Liu H, Zhang S, Yu Y (2013) Associations of noniodized salt and thyroid nodule among the Chinese population: a large cross-sectional study. Am J Clin Nutr 98:684–692
Zhao X, Zhang J, Sun Y, Yao M, Zhu G, Dong H (2015) Iodine nutritional status and prevalence of thyroid nodules among residents using non-iodized salt in Ningbo City, Zhejiang Province (article in Chinese). Chin J Endemiol 34:4
Du Y, Gao Y, Meng F, Liu S, Fan Z, Wu J, Sun D (2014) Iodine deficiency and excess coexist in china and induce thyroid dysfunction and disease: a cross-sectional study. PLoS One 9:e111937
Bao C (2014) Investigation on iodine nutrition level and prevalence of thyroid nodules in Xiangshan Peninsula (article in Chinese). Mod Pract Med 26:3
Meng H, Zeng C (2015) Investigation on iodine nutrition level and prevalence of thyroid nodules among residents in Liandu District (article in Chinese). Zhejiang Prev Med 27:3
Guo Y, Wang H, Ma F, Wang X, Tuhuti H, Abudunaiyimu M, Osiman R (2016) Study on the relationship between iodine nutrition and the occurrence of thyroid nodule disease of Uighur and Han nationality in Urumqi, Xinjiang (article in Chinese). J Med Res 45:5
Gu F, Ding G, Lou X, Wang X, Mo Z, Zhu W, Zhou J, Mao G (2016) Incidence of thyroid diseases in Zhejiang Province, China, after 15 years of salt iodization. J Trace Elem Med Biol 36:57–64
Xu F, Wu Y, Zhao F, Huang Y, Qiu L, Zhao P, Wu J, Wang Y (2016) A cross-sectional study of iodine nutritional status and thyroid nodules of people in Jiangbei District of Ningbo City. Zhejiang Province (Article in Chinese). Chin J Endemiol 35:5
Wu S, Peng L, Miao S, Shao Y (2018) Status of iodine nutrition and risk factors of thyroid nodules among residents in Huizhou region(Article in Chinese). Pract Prev Med 25:4
Jing G, Fu S, Jiao C, Tang X, Teng W, Shan Z (2020) Survey on the prevalence of thyroid nodules among different sexes in rural population in Longnan area of Gansu(Article in Chinese). Journal of Hebei Medical University 41:5
Yang W, Tian J, Wang T, He L, Chang L (2018) Investigation on iodine nutrition status and thyroid nodules among community residents in Yinchuan City (article in Chinese). Ningxia Med J 40:3
Lian L, Wu D, Qi M, Guo B, Zhao X, Lv W, Hu T, Li X (2018) Investigation on iodine nutrition level and prevalence of thyroid nodules in Harbin (article in Chinese). Chin J Endemiol 37:4
Hu W, Zeng Z, Zhang H (2018) Epidemiological investigation iodine nutrient status and relationship between iodized salt and thyroid disease in Hunan province (article in Chinese). J Chin Pract Diagn Ther 32:5
Song J, Zou SR, Guo CY, Zang JJ, Zhu ZN, Mi M, Huang CH, Yu HT, Lu X, Ruan Y, Wu F (2016) Prevalence of thyroid nodules and its relationship with iodine status in Shanghai: a population-based study. Biomed Environ Sci 29:398–407
Cao C, Fu S, Tang X, Liu J, Ma L, Sun W, Niu Y, Jing G, Zhao N, Niu Q, Yang F, Li Y, Wu D, Guo H, Wang B, Song P, Teng W, Shan Z (2018) Survey of thyroid nodules and iodine nutritional status of residents in Chengguan District of Lanzhou(Article in Chinese). Clinical Focus 33:4
Yi J, Dai Y, Zhang Y, He F (2018) Investigation on iodine nutrition level and prevalence rate of thyroid nodules among residents in Zhoushan City (article in Chinese). Prev Med 30:3
Nima Y, Zhang Y, Yang L, Yue J, Shi J (2018) Investigation of thyroid nodules and goiter in Lhasa after universal salt iodization (article in Chinese). J Clin Ultrasound Med 20:4
Dean DS, Gharib H (2008) Epidemiology of thyroid nodules. Best Pract Res Clin Endocrinol Metab 22:901–911
Mazzaferri EL (1993) Management of a solitary thyroid nodule. N Engl J Med 328:553–559
Brito JP, Morris JC, Montori VM (2013) Thyroid cancer: zealous imaging has increased detection and treatment of low risk tumours. BMJ 347:f4706
Song B, Teng W (2020) Research progress on the effect of iodine on thyroid nodules (article in Chinese). Chin J Ctrl Endem Dis 35:3
Kim HJ, Kim NK, Park HK, Byun DW, Suh K, Yoo MH, Min YK, Kim SW, Chung JH (2017) Strong association of relatively low and extremely excessive iodine intakes with thyroid cancer in an iodine-replete area. Eur J Nutr 56:965–971
Guth S, Theune U, Aberle J, Galach A, Bamberger CM (2009) Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur J Clin Investig 39:699–706
Jiang H, Tian Y, Yan W, Kong Y, Wang H, Wang A, Dou J, Liang P, Mu Y (2016) The Prevalence of thyroid nodules and an analysis of related lifestyle factors in Beijing communities. Int J Environ Res Public Health 13:442
Feng S, Zhang Z, Xu S, Mao X, Feng Y, Zhu Y, Liu C (2017) The prevalence of thyroid nodules and their association with metabolic syndrome risk factors in a moderate iodine intake area. Metab Syndr Relat Disord 15:93–97
Chen Y, Zhu C, Chen Y, Wang N, Li Q, Han B, Zhao L, Chen C, Zhai H, Lu Y (2018) The association of thyroid nodules with metabolic status: a cross-sectional SPECT-China study. Int J Endocrinol 2018:6853617
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M (2008) Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371:569–578
Ngo ST, Steyn FJ, McCombe PA (2014) Gender differences in autoimmune disease. Front Neuroendocrinol 35:347–369
Kung AW, Chau MT, Lao TT, Tam SC, Low LC (2002) The effect of pregnancy on thyroid nodule formation. J Clin Endocrinol Metab 87:1010–1014
Barrere X, Valeix P, Preziosi P, Bensimon M, Pelletier B, Galan P, Hercberg S (2000) Determinants of thyroid volume in healthy French adults participating in the SU.VI.MAX cohort. Clin Endocrinol 52:273–278
Ning P, Ren Q, Teng D, Zhang Z, Lv X, Meng S, Shi X, Lou Z, Wu C, Yang P, Zhang W, Zhou L, Luo Y, Zhuoma Z, Yang L, Teng W (2020) Current iodine nutrition status and prevalence of thyroid disorders in Tibetan adults in an oxygen-deficient plateau, Tibet, China: a population-based study. Thyroid 30:759–766
Takahashi T, Fujimori K, Simon SL, Bechtner G, Edwards R, Trott KR (1999) Thyroid nodules, thyroid function and dietary iodine in the Marshall islands. Int J Epidemiol 28:742–749
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, X., Sun, J., Fang, W. et al. Current Iodine Nutrition Status and Morbidity of Thyroid Nodules in Mainland China in the Past 20 Years. Biol Trace Elem Res 199, 4387–4395 (2021). https://doi.org/10.1007/s12011-020-02565-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-020-02565-2