
Abstract
Background
Patients 50 years or younger are at high risk for wear-related complications of their total hip arthroplasty (THA) because of their generally higher levels of activity. Highly crosslinked polyethylene (HXLPE) is believed to be more durable for this population than conventional polyethylene because of its improved wear; however, limited information is available on the wear of HXLPE in this population, particularly the wear of HXLPE when it articulates with alternative bearings like Oxinium (Smith & Nephew, Memphis, TN, USA).
Questions/purposes
The purpose of this study was to evaluate two questions relative to this population of patients undergoing THA. First, what was the linear and volumetric wear rate of HXLPE in patients 50 years or younger at a minimum followup of 9 years and was osteolysis observed in any of these hips? Given the potential for damage to the Oxinium femoral head surface, was the wear of HXLPE in the patients with this material similar to the other bearings or was there accelerated or runaway wear that was visible in any of the patients?
Methods
From November 1999 to April 2005, 105 THAs were performed in 95 patients 50 years of age or younger (mean, 42 years; range, 20–50 years). The mean body mass index was 30 kg/m2 (range, 17–51 kg/m2).The mean followup was 12 years (range, 9–14 years). Two patients died, five patients (one bilateral) were lost to followup, and one hip was revised elsewhere for pain. The patients’ information was not included in the study, which left 87 patients with 96 hips for analysis. Highly crosslinked polyethylene was the acetabular bearing for all of the hips. We analyzed the linear and volumetric wear of all of the hips using the Martell method. Eighty hips had the same diameter head (28 mm) allowing us to more accurately compare the different bearing materials. The type of femoral head used was related to our sequential use of materials beginning with cobalt chrome (14), ceramic (23) followed by Oxinium (43) in the hips with 28-mm heads. Although cobalt-chrome was used early in this study, our previous experience with ceramic on polyethylene encouraged us to use it as an alternative bearing. The Oxinium was used consecutively for the remaining hips.
Results
The mean wear of the HXLPE after 1 year of bedding-in (true linear wear)was 0.022 mm/year (95% confidence interval [CI], 0.015–0.030 mm/year). The mean volumetric wear of HXLPE after 1 year of bedding-in (true volumetric wear) was 9 mm3/year (95% CI, 4–14 mm3/year). None of the hip radiographs had evidence of loosening or osteolysis. Wear was not associated with femoral head material (p = 0.58 for linear wear/year versus head material and p = 0.52 for volumetric wear/year versus head material).
Conclusions
In our study of patients 50 years of age or younger undergoing THA, the linear and volumetric wear rates of HXLPE were very low regardless of the bearing surface material. The laboratory concerns of Oxinium surface damage are serious but at this time we have not seen high wear of the HXLPE or osteolysis in this population.
Level of Evidence
Level III, therapeutic study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
THA is one of the most successful procedures in all of medicine [30]. One factor that challenges the long-term success of THA is polyethylene wear and the effects of polyethylene particulate debris leading to resorption of bone, osteolysis, and implant loosening. The effect of polyethylene wear has been more severe in younger patients presumably because of their high level of activity compared with an older population of patients [5, 7, 8, 10, 26, 32, 38, 39]. It is also likely that this population of young patients is still employed and has expectations for a functional hip throughout their working years as well as their lifetime. Several studies have shown 10-year results of THA with conventional polyethylene in patients 50 years or younger that are disappointing with osteolysis rates up to 56% and survival of the components of only 83% at 10 years [3, 7, 9, 23, 29, 32, 34, 35].
Highly crosslinked polyethylene (HXLPE) was developed with the purpose of minimizing or eliminating wear as a problem for THA. Since its approval by the US Federal Drug Administration in 1997, HXLPE has been used extensively by surgeons with documented results of low wear, osteolysis, or implant loosening caused by the material’s wear. The counterface or the femoral head provides another opportunity for a material that lessens the wear of the polyethylene. Our previous experience demonstrated a very low wear rate using ceramic against conventional polyethylene [40]. In our study, 64 THAs were performed in 56 patients. At the followup interval of 17 to 21 years, only five hips had been revised. The living patients (18) returned for clinical and radiographic evaluation. The mean linear and volumetric polyethylene wear rates in this series at 17 to 21 years were 0.034 mm/year and 28 mm3/year, respectively. It was this experience that led us to use an alternative material to cobalt-chrome articulating with a HXLPE. Initially, this was ceramic but because of the risk of fracture and the in vitro results of Oxinium (Smith & Nephew, Memphis, TN, USA), we transitioned to Oxinium for these patients. Recent reports of surface damage to Oxinium and the potential for accelerated wear of HXLPE because of the surface damage led us to perform this investigation in our patients 50 years or younger at a minimum 9-year followup [13, 16, 20, 27, 33]. We asked two questions. The first questions was, what is the linear and volumetric wear of THA performed with HXLPE in patients 50 years or younger and was osteolysis observed in any of these patients? The second question we asked was, does the femoral head composition, particularly the Oxinium, affect the wear of the HXLPE and were there any outliers with runaway wear that would suggest damaged head articulation?
Patients and Methods
After institutional review board approval, we reviewed the records of a consecutive series of patients with THA who were 50 years or younger at the time of their THA. Between November 1999 and April 2005, 105 THAs were performed in 95 patients 50 years or younger who had their hips replaced using HXLPE. Two deceased patients, five (six hips) lost to followup, and one revised were not included in this analysis, which left us with 87 patients (96 hips). The medical records of all patients with a minimum followup of 9 years were included in this study. The data from the eight patients (two deceased, five lost to followup, one revised elsewhere for pain) were not used. The study included 40 men and 47 women with a mean age at surgery of 42 years (range, 20–50 years). The mean body mass index was 30 kg/m2 (range, 17–51 kg/m2). Preoperative diagnoses included osteoarthritis (36), hip dysplasia (21), avascular necrosis (17), inflammatory arthritis (10), posttraumatic arthrosis (six), and other childhood hip disease including slipped capital femoral epiphysis (three), Legg-Calvé-Perthes disease (two), and coxa vara (one). Seventy-nine of the 87 patients were employed at the time of their surgery. The patients’ work included heavy labor (eight), light labor (37), and desk work (30). Of the remaining patients, four worked from home and the remaining eight patients were either retired or disabled. The 87 patients (96 hips) agreed to either return for followup evaluation or complete a questionnaire and have radiographs mailed to us.
All of the surgeries were performed using a posterior approach. The acetabular components were press-fit (1–2 mm) with one or two screws used for supplemental fixation (Trilogy; Zimmer Warsaw, IN, USA). Electron beam-irradiated and melted HXLPE (Longevity; Zimmer) was the articulating material of the acetabular component. The acetabular component (or a previous generation) was the same component that we had used for the previous 11 years of practice. The femoral components were a press-fit tapered titanium stem (Synergy; Smith & Nephew, Memphis, TN, USA) and one porous-coated nonmodular stem (Prodigy; DePuy, Warsaw, IN, USA). This stem was selected because of the surgeon’s (KLG) familiarity and use of a tapered design. One porous-coated nonmodular stem, Prodigy (DePuy), was used as well. Our favorable experience with ceramic on polyethylene [40] and the very low wear rates using this combination led us to select this as an alternative bearing to cobalt-chrome. The initial patients in this study had cobalt-chrome but we gradually introduced ceramic. An overlap of 10 patients did occur as we transitioned from cobalt-chrome to ceramic. The reports of Oxinium were encouraging and obviated the risk of head fracture associated with ceramic [18]. We subsequently used Oxinium consecutively until the study was completed. The femoral head size was selected to maintain a polyethylene thickness of approximately 6 mm to avoid the problems associated with thin polyethylene, particularly at the rim of the acetabulum. We have since learned that polyethylene less than 6 mm is safe and has not been associated with excessive wear or fracture. The bearings of the femoral component were cobalt-chrome (19), oxidized zirconium (43), and ceramic (34). The bearing diameters were 26 mm (14), 28 mm (71), or 32 mm (11). We have reported the wear data for the patients with a 28 mm diameter (Table 1).
The radiographs were analyzed for wear, radiolucent lines, osteolysis, or a change in the position of the component over time. The HXLPE was analyzed using the Martell technique for measuring wear [28]. Radiographs were evaluated for loosening defined as a change in component position of greater than 5 mm or a circumferential radiolucent line of 2 mm or greater [31]. The acetabulum and femur were evaluated for evidence of osteolysis defined as a nonlinear radiolucency greater than 5 mm of the bone adjacent to the prosthesis. The findings were recorded for the three zones of the acetabulum described by DeLee and Charnley [11] and of the seven zones for the femur described by Gruen et al. [19]. The effect of the femoral head material on HXLPE wear was evaluated with the Kruskal-Wallis one-way analysis of variance.
Results
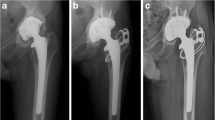
The mean linear wear after bedding-in (true linear wear) of our patients was 0.022 mm/year (95% confidence interval [CI], 0.015–0.030 mm/year). The mean volumetric wear after bedding-in (true volumetric wear) was 9 mm3/year (95% CI, 4–14 mm3/year). We did not see any evidence of osteolysis in the hips of our patients. We did see acetabular radiolucencies that were identified around nine of the acetabular components and one of these had a circumferential radiolucent line of approximately 1 mm 12 years after THA (Fig. 1A–B). Radiolucent lines were identified in two of the femurs (Zones 1 and 7) but none of these patients had a circumferential radiolucent line or evidence of subsidence. Furthermore, a change in component position or subsidence was not evident in any of the acetabular or femoral components. The linear and volumetric wear of the cobalt-chrome, ceramic, and Oxinium was also similar (Table 1). The wear of the polyethylene was not associated with the femoral head material (cobalt-chrome, oxidized zirconium, or ceramic) (p = 0.58 for linear wear/year versus head material and p = 0.52 for volumetric wear/year versus head material). None of the patients in the Oxinium group had evidence of runaway wear.

(A) The figure is an AP pelvis radiograph obtained 6 weeks after THA in a 47-year-old woman. (B) The figure is an AP pelvis radiograph obtained 12 years after THA. The radiolucencies are evident (arrows) around the acetabular component and the proximal femoral component in Zone 1 and Zone 7.
Discussion
THA for patients aged 50 years or younger poses a major challenge for the patient and surgeon because of the patient’s demand for a long-lasting hip that allows them to be active. Previous reports on this population with conventional polyethylene have been associated with unacceptably high component loosening and osteolysis [3, 7, 9, 23, 29, 32, 34, 35]. Highly crosslinked polyethylene has had much less wear and osteolysis, even in the younger population [1, 21, 22, 24, 25]. Use of a counterface material such as ceramic or Oxinium to further decrease wear is also appealing. Based on our previous experience [40], we began using ceramic to further lower the wear of the HXLPE. Oxinium with its enhanced surface wear properties but without risk of fracture was subsequently used for our patients’ femoral articulation. More recent reports have documented damage to the Oxinium surface, which is of concern to surgeons and patients because of the potential for increased wear of the HXLPE [13, 16, 20, 27, 33]. The problem is of particular importance to those patients who sustain a prosthetic dislocation [13, 16, 20, 27]. Trauma or hip dislocation can result in scratching of the Oxinium surface presumably when the femoral head meets or articulates against the metal of the acetabular component. It is because of this risk of surface damage and potential increase wear of HXLPE that we evaluated the linear and volumetric wear of our patients’ hips.
Our study does have limitations. First, our study was underpowered and would have required 160 patients in each group (cobalt-chrome, ceramic, and Oxinium) to show a statistically significant difference in wear of 30% and determine if any of the materials were superior. Second, the head sizes were also different making comparisons difficult among all of the hips. Our rationale for selecting the different head sizes was to allow a polyethylene thickness of approximately 6 mm. The technique used for evaluation of our patients’ polyethylene wear is also a possible limitation because of alternative methods used to measure wear [6]. The Martell technique to measure wear uses the revised Hip Analysis Suite, Version 8.0.3.0 (University of Chicago, Chicago, IL, USA). This version allows for accurate measurement of wear. Kraay et al. evaluated the accuracy of the new Hip Analysis Suite, Version 8.0.3.0, and found a mean accuracy of 0.008 mm and a corresponding volumetric accuracy of 3.17 mm3 [28]. Kraay concluded that the results compared favorably with radiostereometric analysis that has an acceptable accuracy of 0.050 to 0.150 mm. Another limitation is the mixing of components from different manufacturers. Although one may expect a component mismatch to result in elevated wear, we have not seen that in our practice. However, we cannot support the practice of mixing manufacturers’ implants with any scientific data and report it as a weakness of this study.
Our wear rate for all hips was 0.022 mm/year (linear) and 9 mm3/year (volumetric). The wear is low and compares favorably with other studies using HXLPE (Table 2). The low rate of HXLPE wear in our study is below the assumed wear threshold to produce particulate debris that is sufficient to cause osteolysis, assuming the particles are of comparable biologic activity and because of this, the survival should be equal to or improved when compared with conventional polyethylene. Two prospective randomized studies have demonstrated less wear but have not shown a reduction in aseptic loosening [17, 21]. The studies include a relatively small number of patients (60, 54) randomized with one study reporting one failure of a cemented femur in the standard polyethylene group and two failures in the HXLPE group (p = 1.0) [21]. The other study identified no failures in either group [17]. To our knowledge, a prospective randomized trial of THA comparing conventional polyethylene with HXLPE in patients 50 years or younger has not been published. We are aware of very few studies evaluating HXLPE in patients 50 years or younger who have been followed for a comparable interval (Table 2). Babovic and Trousdale reviewed 50 patients (54 hips) at a minimum followup of 10 years [1]. In that group, only one patient had a revision or dislocation and the wear of the HXLPE was 0.02 ± 0.0047 mm/year. The report of alumina on HXLPE has also been reported in patients 50 years or younger with comparable 10-year followup [22]. The two studies, one of 57 patients (67) hips and the other 100 patients (100 hips), evaluated the wear of the polyethylene. In each of the studies, the wear was 0.031 ± 0.004 mm/year. None of the patients required revision surgery or had evidence of osteolysis or loosening. The remaining 10-year followup studies include patients with a mean age greater than 50 [2, 4, 12, 14, 17, 21, 37].
Our second question was, does the femoral head composition, particularly Oxinium, affect the wear of HXLPE and were there any outliers with runaway wear that would suggest a damaged head articulation? In our cohort of patients with a 28-mm femoral head of Oxinium articulating with HXLPE, the mean linear wear rate was 0.024 mm/year and we did not see any patients with runaway wear. The findings of comparable wear without runaway wear are important and timely considering the recent reports of Oxinium surface damage and its potential for accelerated polyethylene wear. The linear and volumetric wear of our Oxinium hips was also very low suggesting that scratching had not occurred or if it had, it had not caused adverse or accelerated wear. Alternatively, because we did not have any hips dislocate, the femoral heads did not suffer significant surface damage. Two other studies have reported similar findings to ours at a shorter length of followup [15, 36]. One of these included Oxinium on HXLPE in 54 patients (56 hips) with a mean age of 53 years followed for a mean of 2.5 years with a linear wear rate of 0.004 mm/year. More recently Morison reported a prospective randomized study comparing Oxinium with cobalt-chrome in patients with HXLPE. Patients were followed for a mean of 6.8 years and the mean linear wear rate of the Oxinium group was 0.061 mm/year per year and the cobalt-chromium was 0.076 mm/year.
In conclusion, this study of THA evaluating patients 50 years of age or younger has demonstrated low linear and volumetric wear rates of HXLPE regardless of the bearing surface material. Additionally, we could determine no significant difference in wear when the counterface was cobalt-chrome, ceramic, or Oxinium. Although the laboratory and in vivo analyses of Oxinium surface damage are serious and a cause for concern, we have not seen significant wear of our HXLPE, osteolysis, and none of the hips have been revised for problems associated with their Oxinium or the other bearing materials. The results are encouraging; however, they must be guarded because of the demand this population will continue to place on their implants over the next decade and beyond.
References
Babovic N, Trousdale RT. Total hip arthroplasty using highly cross-linked polyethylene in patients younger than 50 years with minimum 10-year follow-up. J Arthroplasty. 2013;28:815–817.
Bedard NA, Callaghan JJ, Stefl MD, Willman TJ, Liu SS, Goetz DD. Fixation and wear with a contemporary acetabular component and cross-linked polyethylene at minimum 10-year follow-up. J Arthroplasty. 2014;29:1961–1969.
Berger RA, Jacobs JJ, Quigley LR, Rosenberg AG, Galante JO. Primary cementless acetabular reconstruction in patients younger than 50 years old. 7- to 11-year results. Clin Orthop Relat Res. 1997;344:216–226.
Bragdon CR, Doerner M, Martell J, Jarrett B, Palm H, Multicenter Study Group, Malchau H. The 2012 John Charnley Award: Clinical multicenter studies of the wear performance of highly crosslinked remelted polyethylene in THA. Clin Orthop Relat Res. 2013;471:393–402.
Callaghan JJ, Forest EE, Sporer SM, Goetz DD, Johnston RC. Total hip arthroplasty in the young adult. Clin Orthop Relat Res. 1997;344:257–262.
Callary SA, Solomon LB, Holubowycz OT, Campbell DG, Munn Z, Howie DW. Wear of highly crosslinked polyethylene acetabular components. Acta Orthop. 2015;86:159–168.
Chiu KY, Tang WM, Ng TP, Poon KC, Ho WY, Lee KM. Cementless total hip arthroplasty in young Chinese patients: a comparison of 2 different prostheses. J Arthroplasty. 2001;16:863–870.
Clohisy JC, Harris WH. Primary hybrid total hip replacement, performed with insertion of the acetabular component without cement and a precoat femoral component with cement. An average ten-year follow-up study. J Bone Joint Surg Am. 1999;81:247–255.
D’Antonio JA, Capello WN, Manley MT, Feinberg J. Hydroxyapatite coated implants. Total hip arthroplasty in the young patient and patients with avascular necrosis. Clin Orthop Relat Res. 1997;344:124–138.
Delasotta LA, Rangavajjula AV, Porat MD, Frank ML, Orozco FR, Ong AC. What are young patients doing after hip reconstruction? J Arthroplasty. 2012;27:1518–1525.e2.
DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res. 1976;121:20–32.
Engh CA Jr, Hopper RH Jr, Huynh C, Ho H, Sritulanondha S, Engh CA Sr. A prospective, randomized study of cross-linked and non-cross-linked polyethylene for total hip arthroplasty at 10-year follow-up. J Arthroplasty. 2012;27:2–7.e1.
Evangelista GT, Fulkerson E, Kummer F, Di Cesare PE. Surface damage to an Oxinium femoral head prosthesis after dislocation. J Bone Joint Surg Br. 2007;89:535–537.
Garcia-Rey E, Garcia-Cimbrelo E, Cruz-Pardos A. New polyethylenes in total hip replacement: a ten- to 12-year follow-up study. Bone Joint J. 2013;95:326–332.
Garvin KL, Hartman CW, Mangla J, Murdoch N, Martell JM. Wear analysis in THA utilizing oxidized zirconium and crosslinked polyethylene. Clin Orthop Relat Res. 2009;467:141–145.
Gibon E, Scemama C, David B, Hamadouche M. Oxinium femoral head damage generated by a metallic foreign body within the polyethylene cup following recurrent dislocation episodes. Orthop Traumatol Surg Res. 2013;99:865–869.
Glyn-Jones S, Thomas GE, Garfjeld-Roberts P, Gundle R, Taylor A, McLardy-Smith P, Murray DW. The John Charnley Award: Highly crosslinked polyethylene in total hip arthroplasty decreases long-term wear: a double-blind randomized trial. Clin Orthop Relat Res. 2015;473:432–438.
Good V, Ries M, Barrack RL, Widding K, Hunter G, Heuer D. Reduced wear with oxidized zirconium femoral heads. J Bone Joint Surg Am. 2003;85(Suppl 4):105–110.
Gruen TA, McNeice GM, Amstutz HC. ‘Modes of failure’ of cemented stem-type femoral components: a radiographic analysis of loosening. Clin Orthop Relat Res. 1979;141:17–27.
Jaffe WL, Strauss EJ, Cardinale M, Herrera L, Kummer FJ. Surface oxidized zirconium total hip arthroplasty head damage due to closed reduction effects on polyethylene wear. J Arthroplasty. 2009;24:898–902.
Johanson PE, Digas G, Herberts P, Thanner J, Karrholm J. Highly crosslinked polyethylene does not reduce aseptic loosening in cemented THA: 10-year findings of a randomized study. Clin Orthop Relat Res. 2012;470:3083–3093.
Kim Y, Choi Y, Kim J. Cementless total hip arthroplasty with alumina-on-highly cross-linked polyethylene bearing in young patients with femoral head osteonecrosis. J Arthroplasty. 2011;26:218–223.
Kim Y, Oh S, Kim J. Primary total hip arthroplasty with a second-generation cementless total hip prosthesis in patients younger than fifty years of age. J Bone Joint Surg Am. 2003;85:109–114.
Kim Y, Park J, Kulkarni SS, Kim Y. A randomised prospective evaluation of ceramic-on-ceramic and ceramic-on-highly cross-linked polyethylene bearings in the same patients with primary cementless total hip arthroplasty. Int Orthop. 2013;37:2131–2137.
Kim Y, Park J, Patel C, Kim D. Polyethylene wear and osteolysis after cementless total hip arthroplasty with alumina-on-highly cross-linked polyethylene bearings in patients younger than thirty years of age. J Bone Joint Surg Am. 2013;95:1088–1093.
Kinkel S, Wollmerstedt N, Kleinhans JA, Hendrich C, Heisel C. Patient activity after total hip arthroplasty declines with advancing age. Clin Orthop Relat Res. 2009;467:2053–2058.
Kop AM, Whitewood C, Johnston DJ. Damage of oxinium femoral heads subsequent to hip arthroplasty dislocation three retrieval case studies. J Arthroplasty. 2007;22:775–779.
Kraay MJ, Moore RD, Martell JM, Rimnac CM. Reassessment of computerized wear measurement for total hip arthroplasty with correction for projectional image distortion: a brief follow-up report. J Bone Joint Surg Am. 2010;92:1858–1867.
Kronick JL, Barba ML, Paprosky WG. Extensively coated femoral components in young patients. Clin Orthop Relat Res. 1997;344:263–274.
Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet. 2007;370:1508–1519.
Massin P, Schmidt L, Engh CA. Evaluation of cementless acetabular component migration. An experimental study. J Arthroplasty. 1989;4:245–251.
McAuley JP, Szuszczewicz ES, Young A, Engh CA Sr. Total hip arthroplasty in patients 50 years and younger. Clin Orthop Relat Res. 2004;418:119–125.
McCalden RW, Charron KD, Davidson RD, Teeter MG, Holdsworth DW. Damage of an oxinium femoral head and polyethylene liner following ‘routine’ total hip replacement. J Bone Joint Surg Br. 2011;93:409–413.
McLaughlin JR, Lee KR. Total hip arthroplasty in young patients. 8- to 13-year results using an uncemented stem. Clin Orthop Relat Res. 2000;373:153–163.
Mont MA, Maar DC, Krackow KA, Jacobs MA, Jones LC, Hungerford DS. Total hip replacement without cement for non-inflammatory osteoarthrosis in patients who are less than forty-five years old. J Bone Joint Surg Am. 1993;75:740–751.
Morison ZA, Patil S, Khan HA, Bogoch ER, Schemitsch EH, Waddell JP. A randomized controlled trial comparing oxinium and cobalt-chrome on standard and cross-linked polyethylene. J Arthroplasty. 2014;29:164–168.
Ranawat AS, Tsailis P, Meftah M, Koob TW, Rodriguez JA, Ranawat CS. Minimum 5-year wear analysis of first-generation highly cross-linked polyethylene in patients 65 years and younger. J Arthroplasty. 2012;27:354–357.
Sechriest VF 2nd, Kyle RF, Marek DJ, Spates JD, Saleh KJ, Kuskowski M. Activity level in young patients with primary total hip arthroplasty: a 5-year minimum follow-up. J Arthroplasty. 2007;22:39–47.
Silva M, Shepherd EF, Jackson WO, Dorey FJ, Schmalzried TP. Average patient walking activity approaches 2 million cycles per year: pedometers under-record walking activity. J Arthroplasty. 2002;17:693–697.
Urban JA, Garvin KL, Boese CK, Bryson L, Pedersen DR, Callaghan JJ, Miller RK. Ceramic-on-polyethylene bearing surfaces in total hip arthroplasty. Seventeen to twenty-one-year results. J Bone Joint Surg Am. 2001;83:1688–1694.
Acknowledgments
We thank Dr Patrick Anderl and Dr Beau Konigsberg for their assistance with the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (CWH) received funding outside of this work in the amount of USD 10,000 to USD 100,000 from Smith & Nephew (Memphis, TN, USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
Surgeries were performed at the University of Nebraska Medical Center, Omaha, NE, USA. Data were reviewed at Chicago University, Chicago, IL, USA.
About this article

Cite this article
Garvin, K.L., White, T.C., Dusad, A. et al. Low Wear Rates Seen in THAs With Highly Crosslinked Polyethylene at 9 to 14 Years in Patients Younger Than Age 50 Years. Clin Orthop Relat Res 473, 3829–3835 (2015). https://doi.org/10.1007/s11999-015-4422-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-015-4422-7