
Abstract
Background
Open tibial shaft fractures are one of the most devastating orthopaedic injuries. Surgical treatment options include reamed or unreamed nailing, plating, Ender nails, Ilizarov fixation, and external fixation. Using a network meta-analysis allows comparison and facilitates pooling of a diverse population of randomized trials across these approaches in ways that a traditional meta-analysis does not.
Questions/purposes
Our aim was to perform a network meta-analysis using evidence from randomized trials on the relative effect of alternative approaches on the risk of unplanned reoperation after open fractures of the tibial diaphysis. Our secondary study endpoints included malunion, deep infection, and superficial infection.
Methods
A network meta-analysis allows for simultaneous consideration of the relative effectiveness of multiple treatment alternatives. To do this on the subject of surgical treatments for open tibial fractures, we began with systematic searches of databases (including EMBASE and MEDLINE) and performed hand searches of orthopaedic journals, bibliographies, abstracts from orthopaedic conferences, and orthopaedic textbooks, for all relevant material published between 1980 and 2013. Two authors independently screened abstracts and manuscripts and extracted the data, three evaluated the risk of bias in individual studies, and two applied Grading of Recommendation Assessment, Development and Evaluation (GRADE) criteria to bodies of evidence. We included all randomized and quasirandomized trials comparing two (or more) surgical treatment options for open tibial shaft fractures in predominantly (ie, > 80%) adult patients. We calculated pooled estimates for all direct comparisons and conducted a network meta-analysis combining direct and indirect evidence for all 15 comparisons between six stabilization strategies. Fourteen trials published between 1989 and November 2011 met our inclusion criteria; the trials comprised a total of 1279 patients surgically treated for open tibial shaft fractures.
Results
Moderate confidence evidence showed that unreamed nailing may reduce the likelihood of reoperation compared with external fixation (network odds ratio [OR], 0.38; 95% CI, 0.23–0.62; p < 0.05), although not necessarily compared with reamed nailing (direct OR, 0.74; 95% CI, 0.45–1.24; p = 0.25). Only low- or very low-quality evidence informed the primary outcome for other treatment comparisons, such as those involving internal plate fixation, Ilizarov external fixation, and Ender nailing. Method ranking based on reoperation data showed that unreamed nailing had the highest probability of being the best treatment, followed by reamed nailing, external fixation, and plate fixation. CIs around pooled estimates of malunion and infection risk were very wide, and therefore no conclusive results could be made based on these data.
Conclusion
Current evidence suggests that intramedullary nailing may be superior to other fixation strategies for open tibial shaft fractures. Use of unreamed nails over reamed nails also may be advantageous in the setting of open fractures, but this remains to be confirmed. Unfortunately, these conclusions are based on trials that have had high risk of bias and poor precision. Larger and higher-quality head-to-head randomized controlled trials are required to confirm these conclusions and better inform clinical decision-making.
Level of Evidence
Level I, therapeutic study.
Similar content being viewed by others


Introduction
Open fractures of the tibial diaphysis are caused by high-energy trauma, most often from traffic accidents [9, 46]. Fractures of the tibial diaphysis constitute the most common open long-bone fracture, occurring in approximately two per 10,000 persons per year in the developed world [8–10]. There is also a growing epidemic of open tibial fractures in populations in low- and middle-income countries [6, 24].With rapidly increasing rates of motorization occurring in developing countries [24], identifying optimal treatment of fractures of the tibial diaphysis is a global surgical priority.
Despite the importance of surgery to treat these injuries, a comprehensive systematic review of all approaches to treat open tibial fracture does not exist. Previous reviews have focused on intramedullary nailing and have been based on a small number of trials [3, 4]. There has been a resurgence of randomized trials evaluating different treatment modalities for open fractures, including comparisons of reamed with unreamed intramedullary nailing [27, 40, 42]; intramedullary nailing with ender nailing [41]; intramedullary nailing with external fixation [30, 39]; external fixation (AO) with the Ilizarov technique [12]; and plate osteosynthesis with intramedullary nailing [45].
Because of the many alternative surgical approaches and the small number of patients studied in available trials evaluating treatment modalities for open tibial fracture, the best stabilization strategy remains unclear. Some trials have been underpowered to evaluate key surgical outcomes [14], which suggests a need for a meta-analysis to pool results across trials. However, traditional meta-analyses can evaluate only the relative efficacy of two treatments at a time. Given the many alternative stabilization strategies that exist for open tibial shaft fractures, not all of which have been compared in head-to-head studies, new methodologic techniques are required to provide effect estimates for all comparisons.
Network meta-analyses, also called multiple-treatment comparison meta-analyses, provide an approach to simultaneous consideration of the relative effectiveness of multiple treatment alternatives [17, 23, 29]. The benefit of a network meta-analysis includes the potential for providing indirect evidence, which refers to the determination of relative treatment effects between two treatments when head-to-head trials (ie, direct evidence) are not available [29].
We therefore conducted a network meta-analysis of randomized trials in orthopaedic trauma surgery to identify the surgical stabilization strategies for open tibial shaft fractures with the least complications. Specifically, our primary endpoint was to identify the stabilization technique associated with the lowest risk of unplanned reoperation. Our secondary study endpoints included malunion, deep infection, and superficial infection.
Search Strategy and Criteria
In the search process for our meta-analysis, we included published and unpublished findings from randomized and quasirandomized trials that met the following eligibility criteria: (1) the study enrolled adult patients with open fractures of the tibial diaphysis. Studies were included if more than 80% of the patients were 18 years or older at the time of enrollment; (2) the study compared any two of the following stabilization techniques: plate fixation, external fixation (by any method), reamed and unreamed intramedullary nailing, Ender intramedullary nailing, or conservative treatment (cast, brace, splint); and (3) all important unplanned reoperations were reported (Table 1).
Studies were excluded if, for any enrolled patient: (1) stabilization had been delayed more than 48 hours, or (2) irrigation and débridement of the open wound was delayed more than 12 hours, (3) the stabilization technique was preceded by another form of operative stabilization (eg, external fixation before intramedullary nailing), or (4) fractures extended into the knee or ankle.
Our primary outcome measure was unplanned, clinically important reoperations (Table 1). Our secondary outcome measures were (1) malunion (bone healing > 5° angulation, > 10° rotation, and > 1 cm shortening); (2) deep infection; and (3) superficial infection.
We searched the Cochrane Central Registry for Randomized Controlled Trials (February 2013, Issue 1), EMBASE (1980–2013), and OVID MEDLINE In-Process & Other Non-Indexed Citations (1981–2013), and OVID MEDLINE (1981–2013). In EMBASE and MEDLINE, we combined subject-specific search strategies with The Scottish Intercollegiate Guidelines Network (SIGN) filter for randomized controlled trials [38]. No language restriction was applied.
Two reviewers (CJF, KNV) searched the reference lists of all key articles for additional eligible trials. We hand searched the table of contents of four major orthopaedic journals, including Journal of Bone and Joint Surgery (American and British editions), Journal of Orthopaedic Trauma, and Clinical Orthopaedics and Related Research ®, from January 2009 to February 2013, and posters, abstracts, and presentations from three major orthopaedic meetings held between 2009 to 2013 (American Academy of Orthopaedic Surgeons, Orthopaedic Trauma Association, Canadian Orthopaedic Association). Two content experts (MB, PT) were consulted to identify any previously unidentified trials.
Detailed review of clinical trial registries included use of: (1) ClinicalTrials.gov, (2) meta-Register of Controlled Trials (mRCT), (3) The National Research Register Archive (NRR), and (4) WHO International Clinical Trials Registry Platform (ICTRP) search portal (searches ClinicalTrials.gov and registers in Australia, New Zealand, and China).
Two authors (CJF, KNV) made independent decisions regarding eligibility based on a priori criteria presented on predeveloped forms.
Two reviewers (CJF, KNV) conducted title, abstract, and full-text screening in duplicate. A third author (MB) adjudicated any differences in opinion.
Two reviewers (CJF, KNV) extracted important patient and injury characteristics, including patient age, sex, smoking status, comorbidities, American Society of Anesthesiologists grade, location of the fracture in the tibial shaft, Gustilo grade, and description of the fracture orientation (eg, transverse, oblique). In addition to the stabilization strategy, we recorded information regarding the timing of surgery, type of antibiotic used, type of irrigation solution, and irrigation pressure, timing, and type of wound closure and coverage, and adjunctive treatment, such as antibiotic bead pouch use or delayed bone grafting. We extracted all important, unplanned reoperation events reported in all manuscripts. Methodologic features included whether the trial protocol was registered, years of recruitment and publication, location and number of study centers, trial type (quasirandomized; parallel, randomized), and length and completeness of followup. Reviewers collected all this information independently, in duplicate, and resolved disagreement by discussion. If discussion failed to resolve the issue, a third party (MB) adjudicated the issue.
Three authors (CJF, RM, HC) made independent assessments of risk of bias using a modification of the Cochrane Handbook for Systemic Reviews of Interventions 5.1.0 risk of bias tool (updated March 2011) [15, 20] that addresses six criteria, including random sequence generation, allocation concealment, level of blinding of participants and personnel, level of blinding of outcome assessors, completeness of followup, and risk of selective reporting bias. We rated the overall risk of bias for each trial that was defined as high-risk if more than two high-risk criteria were met, moderate-risk if one to two high-risk criteria were met, and low-risk if there were no high-risk criteria. Quasirandomized trials are at high-risk of violating the first three criteria (random sequence generation, concealment, and blinding) and therefore were categorized at high risk of bias.
We used a weighted kappa with quadratic weights to quantify reviewer agreement for inclusion of full-text articles. The three categories for agreement were agreement, disagreement, and partial agreement (in instances where it was unclear to us whether the trial should be included). We chose an a priori criterion of a kappa of 0.65 or greater as adequate agreement [3, 33].
Differences in the estimates of the magnitude-of-treatment effect among the trials suggested important sources of heterogeneity. For direct comparisons, heterogeneity of trials was assessed using the I2 statistic from the Cochran Q statistic [21]. When I2 was greater than 40%, we conducted one predefined subgroup analysis (trials with only Gustilo Grade III fractures versus inclusion of other Gustilo grades) and one sensitivity analysis (quasirandomized compared with randomized trials).
For direct comparisons, we first used a random-effects model to pool effect estimates from included trials and report odds ratios (OR) with 95% CI. These analyses were performed using RevMan Version 5 (The Cochrane Collaboration, 2014; The Nordic Cochrane Centre, Copenhagen, Denmark). Second, for our primary outcome of reoperation, we conducted a fixed-effects multiple-treatment comparison meta-analysis using a Bayesian Markov chain Monte Carlo method and reported ORs with 95% CIs. A fixed-effects model was chosen a priori based on expectations of a fixed relative effect of fracture treatment across study populations. We used a node-splitting procedure to generate separate estimates from direct and indirect evidence for all 15 possible comparisons. We evaluated if there was no difference between direct and indirect estimates using alpha = 0.05 level of significance.
We fitted a frequentist inconsistency model that allowed for the treatment effect to vary across study designs. Using this model, we performed a global test for differences between direct and indirect comparisons (incoherence).
We also calculated the probability of each treatment having the lowest reoperation rate, second lowest, third lowest, and so on. This was done by calculating the OR for each type of stabilization strategy compared with an arbitrary common control group and counting the percentage of iterations of the Markov chain in which each treatment had the lowest OR, the second lowest, and so on. The Surface Under the Cumulative RAnking curve (SUCRA) method was used to assess the cumulative probability of each stabilization strategy being superior compared with alternatives [34]. In short, SUCRA measures the area under the curve, with the vertical axis representing the cumulative probability for a given intervention to be ranked first, then first or second, then first or second or third, and so on. The horizontal axis represents the number of ranks any given intervention may assume.
Additionally, we performed a meta-regression of trials comparing unreamed nailing with external fixation to evaluate if the Gustilo grade (Grade III versus all Gustilo grades) modified the relative odds of reoperation. In trials that included all Gustilo subtypes, it would be expected that Types I and II would represent most of the fractures. Analyses were conducted using StatsDirect (version 2.5.2; StatsDirect Ltd, Altrincham, Cheshire, UK), Stata® (version 9; StataCorp LP, College Station, TX, USA) and WinBUGS version 1.4 (Medical Research Council Biostatistics Unit, Cambridge, UK).
The Grading of Recommendation Assessment, Development and Evaluation (GRADE) is a system that enables assessment of the confidence in estimates of treatment effect (quality of evidence), considering study design (in our case, randomized trials) and issues of risk of bias, imprecision, inconsistency, indirectness, and publication bias [16, 18]. Two reviewers (CJF, KNV) independently applied GRADE to make direct comparisons using established methods bias [16, 18], and to make indirect comparisons using recently suggested methods from the GRADE working group [32]. GRADE guidance includes rating down indirect comparisons when there is suspicion of possible effect modification attributable to differences in patients, optimal use of interventions, or measurement of outcomes across the direct comparisons that informed the indirect comparisons (which we refer to as intransitivity). In the event that direct and indirect evidence was consistent (yielded similar estimates of effect), we combined the results and considered the resulting network meta-analysis estimate the best estimate of effect. If results of direct and indirect estimates differed significantly (incoherence), we used the estimate warranting greater confidence as our best estimate of effect.
Literature Search
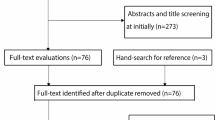
We identified 1396 articles: 232 from the Cochrane Register of Randomized Controlled Trials, 752 from EMBASE, 411 from MEDLINE, and two from bibliographic review (Fig. 1). Deduplication removed 333 references; the remaining 1064 articles underwent title and abstract review, of which 20 proved potentially eligible for our survey and underwent full-text review. Another six articles were excluded (Appendix 1. Supplemental materials are available with the online version of CORR®), leaving 14 eligible studies [2, 12, 13, 19, 22, 25, 27, 30, 39, 41–45] for our survey. The weighted kappa for full-text article eligibility was good (κ = 0.79; 95% CI, 0.46–0.98).

The PRISMA flow diagram shows the study selection process. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Of 14 eligible studies, 13 were published in English and one in Persian. Eight of the studies were randomized [2, 13, 25, 27, 30, 41, 42, 45] and six were quasirandomized controlled trials [12, 19, 22, 39, 43, 44]. Five studies included patients with open and closed fractures [13, 27, 41, 42, 45]; however, we extracted and included data only from the subset of patients with open fractures in these trials. In total, the trials assigned 1279 patients with open tibial fractures to one of six stabilization strategies. We performed our multiple-treatment comparison meta-analysis with head-to-head comparisons, including corresponding OR, 95% CIs, and GRADE confidence assessments for seven (of a possible 15) direct comparisons among six stabilization techniques (Fig. 2). Mean followup in the trials ranged between 12 months and 3.8 years (Table 2).

The network diagram shows the effect estimates and GRADE quality of evidence for available direct evidence among six stabilization strategies. Seven of 15 possible comparisons had head-to-head trials. The arrows point away from superior treatments and the caliber of the adjoining lines indicates the number of available trials. *Only distal tibial shaft fractures included; †fractures with cortical contact included; GRADE = Grading of Recommendation Assessment, Development and Evaluation.
Of the 14 studies, two reported the irrigation solution and volume, 10 provided information regarding perioperative antibiotic type, and 11 disclosed the management of soft tissues (Table 3). Only six studies provided information describing the types of fractures or level of fracture comminution (Appendix 2. Supplemental materials are available with the online version of CORR®). Definitions for nonunion varied considerably among trials (Appendix 3. Supplemental materials are available with the online version of CORR®); therefore, we did not report nonunion as a secondary outcome but included reoperations for nonunion in our primary outcome. Perioperative complications, including death, fat embolism, pulmonary thromboembolism, blood loss, and compartment syndrome were seldom reported.
One trial was at low risk of bias [42], three studies were at moderate risk [25, 27, 45], and the remainder were high risk [2, 12, 13, 19, 22, 30, 39, 41, 43, 44]. Four trials concealed allocation [25, 27, 42, 45], but only one trial blinded outcome assessors [42]. The Cochrane risk of bias plot shows the assessments conducted for each study included in our review (Fig. 3). Few patients were lost to followup in any of the studies.

The risk of bias summary is shown. Green circles = low risk of bias; red circles = high risk of bias.
Direct (head-to-head) evidence for clinically important, unplanned reoperations was found (Figs. 2 & 4). Four trials compared unreamed with reamed nailing (n = 547) as a management technique [13, 25, 27, 42] and five compared unreamed nailing with external fixation (n = 402) [19, 30, 39, 43, 44]. The five remaining trials [2, 12, 22, 41, 45] compared (1) unreamed intramedullary nailing with Ender nailing (n = 75); (2) external fixation with Ender nailing (n = 57); (3) plate with external fixation (n = 56); (4) Ilizarov with AO external fixation (n = 120); and (5) reamed nailing with plate fixation (n = 40) for treatment of patients with tibial fractures.

The forest plots of head-to-head evidence show the relative effects of the different types of surgical stabilization on reoperation rates. M-H = Mantel–Haenszel.
Results
Unplanned Reoperation
Unreamed nailing resulted in lower odds of unplanned reoperations compared with external fixation (network OR, 0.38, 95% CI, 0.23–0.62; moderate confidence) (Table 4). The meta-regression performed to evaluate the effect of Gustilo grade on odds of reoperation in trials comparing unreamed nailing with external fixation provided no difference in effect (interaction, p = 0.84), which suggested that the relative treatment effect of unreamed nailing versus external fixation was consistent across Gustilo grades.
Comparing unreamed with reamed nailing, direct evidence did not show a reduction in the odds of the patient requiring a clinically important reoperation (OR, 0.74; 95% CI, 0.45–1.24; moderate confidence), although indirect evidence did (OR, 0.07; 95% CI, 0.01–0.46; low confidence). The differences in the magnitudes of the direct and indirect effect estimates were statistically significant (p = 0.02), a finding referred to as incoherence. Because of this incoherence, we decreased our confidence in the combined (network) estimate to low confidence as well (network OR, 0.62; 95% CI, 0.37–1.03), and the direct estimate therefore was considered the best estimate (Table 4).
Best available evidence for the following treatments showed superiority over the associated comparator: unreamed nailing was superior to external fixation (OR, 0.39; 95% CI, 0.23–0.65; moderate confidence); unreamed nailing was superior to plate fixation (OR, 0.20; 95% CI, 0.07–0.53; low confidence); reamed nailing was superior to plate fixation (OR, 0.33; 95% CI, 0.12–0.87; low confidence); Ender nailing was superior to external fixation (OR, 0.25; 95% CI, 0.07–0.91; low confidence); external fixation was superior to plate fixation (OR, 0.25; 95% CI, 0.08–0.81; low confidence); and Ilizarov fixation was superior to plate fixation (OR, 0.21; 95% CI, 0.05–0.83; very low confidence). CIs for all other treatment comparisons overlapped with ‘no effect’, and therefore were not precise enough to be confident regarding the direction of effect (Table 5).
SUCRA scores revealed that unreamed nailing had the highest probability of being the best treatment (SUCRA of 86.3%), reamed nailing was second (SUCRA of 54.4%), external fixation was third (SUCRA of 24.1%), and plate fixation was likely the worst treatment (SUCRA of 3.6%) for open tibial shaft fractures (Table 6). Surgical treatments that were informed by only very low-quality evidence were not scored to prevent biasing of the rank list.
Infection and Malunion
CIs around pooled direct estimates of malunion and infection risk were very wide, and estimates warranted only low or very low confidence based on GRADE criteria. No conclusive results could be made on our secondary outcomes based on these data. Because of very few events, wide CIs, a sparse network, and low or very low confidence in direct estimates, we did not conduct network meta-analyses (ie, indirect and combined pooled estimates) for either infection or malunion.
Discussion
Open fractures of the tibial shaft are common and increasing in incidence, especially in the developing world [24]. Because outcomes of existing surgical treatments in open fractures are not necessarily the same as seen with closed fractures [28, 42], optimal fixation strategies need to be explored. However, there are no large studies comparing all fixation types, and a network meta-analysis offers opportunities to make comparisons that otherwise do not exist in head-to-head surgical trials. We therefore aimed to use a network meta-analysis to determine the surgical option with the lowest risk of reoperation and the lowest risks of malunion, deep infection, and superficial infection.
Limitations
There are some limitations to our review. The most important limitation is that, with the exception of two comparisons, treatment effect estimates were graded as either low or very low confidence, attributable mainly to the high risk of bias of included trials and imprecision of the pooled estimates. Although our review represents the best available evidence, this is not necessarily the best possible evidence.
Another issue was that there were several inconsistencies between direct and indirect comparisons (ie, incoherence). Incoherence typically is attributable to major differences in the trials that make up each comparison (eg, differences between included patients or cointerventions, or major methodologic differences). We dealt with this issue by first identifying the sources of inconsistency (Tables 4 and 5), and second, by using only the highest confidence comparisons as the best estimate of effect, as recommended by the GRADE working group [32].
Finally, functional outcomes were not reported in any of the trials. Quantifying differences in function among available treatment options is important information to inform evidence-based clinical decision-making. This is a research gap future trials must address.
Key Findings
We found that unreamed nail fixation was associated with a lower risk of reoperation compared with external fixation, and this was independent of the Gustilo classification of the fracture. This confirms current knowledge pertaining to higher infection rates with external fixation of open fractures [28], many of which may go on to require reoperation. Importantly, this finding refers only to definitive external fixation and not temporizing external fixation; the latter is a potentially effective strategy in cases of severe soft tissue contamination or extensive fracture comminution [1, 5].
Our network meta-analysis also showed insufficient precision to determine whether there was any difference in the risk of reoperation between reamed and unreamed nailing. Although reamed nailing has been shown to be more effective than unreamed nailing in closed fractures [42], there are concerns regarding poorer outcomes with reaming of open fractures owing to potential disruption of the endosteal blood vessels in the context of preexisting periosteal compromise [35–37]. Unfortunately, based on the results of our network meta-analysis, the current literature is unable to definitively resolve this issue.
Plate fixation showed a higher risk of reoperation compared with other surgical treatment options in our network meta-analysis (ie, unreamed nailing, reamed nailing, external fixation, and Ilizarov fixation), although confidence in the estimates for these comparisons was low or very low. However, this is consistent with existing recommendations to avoid plate fixation in open tibial fractures owing to higher infection rates and, therefore, potential for reoperation [28].
Method ranking of surgical treatment alternatives in the network confirmed the aforementioned findings, showing an appreciable gradient with unreamed nailing being the highest ranked (ie, lowest risk of reoperation), followed by reamed nailing, external fixation, and internal plate fixation (ie, highest risk of reoperation). The ranking did not consider treatments informed by very low confidence.
Although our secondary objective was to quantify differences in the risks of malunion, deep infection, and superficial infection among the comparisons, small numbers of reported events prevented us from finding any appreciable differences between treatment options. Future randomized trials must clearly report these complications and be sufficiently large to capture real differences in the frequency of complications between treatments.
Our findings add important new information to the existing literature. There have been numerous systematic reviews using traditional head-to-head meta-analyses for tibial shaft fracture management [3, 4, 7, 11, 26, 31, 47]. Of these, only one evaluated [3] an intervention other than reamed or unreamed nailing. In addition, among the reviews comparing reamed and unreamed intramedullary nailing, open fracture data generally have been underemphasized, methods have been poor (eg, exclusion of non-English studies), and CIs have been very wide. Therefore, there has not been any way for orthopaedic surgeons to determine the best treatment strategy for open tibial shaft fractures. Our network meta-analysis provides clarity regarding conclusions that can be made based on the current literature, while identifying areas where research evidence is poor quality or lacking.
Conclusion
Current evidence suggests that intramedullary nailing may be superior to other fixation strategies for open tibial shaft fractures. Use of unreamed nails over reamed nails also may be advantageous with open fractures, but this remains to be confirmed. Unfortunately, these conclusions are based on trials that have a high risk of bias and poor precision. Larger and higher-quality head-to-head randomized controlled trials are required to confirm these conclusions and better inform clinical decision-making.
References
Antich-Adrover P, Marti-Garin D, Murias-Alvarez J, Puente-Alonso C. External fixation and secondary intramedullary nailing of open tibial fractures: a randomised, prospective trial. J Bone Joint Surg Br. 1997;79:433–437.
Bach AW, Hansen ST Jr. Plates versus external fixation in severe open tibial shaft fractures: a randomized trial. Clin Orthop Relat Res. 1989;241:89–94.
Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001;83:62–68.
Bhandari M, Guyatt GH, Tong D, Adili A, Shaughnessy SG. Reamed versus nonreamed intramedullary nailing of lower extremity long bone fractures: a systematic overview and meta-analysis. J Orthop Trauma. 2000;14:2–9.
Blachut PA, Meek RN, O’Brien PJ. External fixation and delayed intramedullary nailing of open fractures of the tibial shaft: a sequential protocol. J Bone Joint Surg Am. 1990;72:729–735.
Chalya PL, Mabula JB, Dass RM, Mbelenge N, Ngayomela IH, Chandika AB, Gilyoma JM. Injury characteristics and outcome of road traffic crash victims at Bugando Medical Centre in Northwestern Tanzania. J Trauma Manag Outcomes. 2012;6:1.
Coles CP, Gross M. Closed tibial shaft fractures: management and treatment complications. A review of the prospective literature. Can J Surg. 2000;43:256–262.
Court-Brown CM, Bugler KE, Clement ND, Duckworth AD, McQueen MM. The epidemiology of open fractures in adults: a 15-year review. Injury. 2012;43:891–897.
Court-Brown CM, McBirnie J. The epidemiology of tibial fractures. J Bone Joint Surg Br. 1995;77:417–421.
Court-Brown CM, Rimmer S, Prakash U, McQueen MM. The epidemiology of open long bone fractures. Injury. 1998;29:529–534.
Duan X, Al-Qwbani M, Zeng Y, Zhang W, Xiang Z. Intramedullary nailing for tibial shaft fractures in adults. Cochrane Database Syst Rev. 2012;1:CD008241.
Esmaeilnejad Ganji SM, Bahrami M, Joukar F. Ilizarov versus AO external fixator for the treatment of tibia open fractures. Iran Red Crescent Med J. 2011;13:868–872.
Finkemeier CG, Schmidt AH, Kyle RF, Templeman DC, Varecka TF. A prospective, randomized study of intramedullary nails inserted with and without reaming for the treatment of open and closed fractures of the tibial shaft. J Orthop Trauma. 2000;14:187–193.
Freedman KB, Back S, Bernstein J. Sample size and statistical power of randomised, controlled trials in orthopaedics. J Bone Joint Surg Br. 2001;83:397–402.
Guyatt G, Busse, J. Tools to Assess Risk of Bias in Randomized Controlled Trials. Available at: http://distillercer.com/wp-content/uploads/2014/02/Tool-to-Assess-Risk-of-Bias-in-Randomized-Controlled-Trials.docx. Accessed February 7, 2015.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, Norris S, Falck-Ytter Y, Glasziou P, DeBeer H, Jaeschke R, Rind D, Meerpohl J, Dahm P, Schunemann HJ. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64:383–394.
Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, Alonso-Coello P, Falck-Ytter Y, Jaeschke R, Vist G, Akl EA, Post PN, Norris S, Meerpohl J, Shukla VK, Nasser M, Schunemann HJ; GRADE Working Group. GRADE guidelines: 8. Rating the quality of evidence—indirectness. J Clin Epidemiol. 2011;64:1303–1310.
Guyatt GH, Oxman AD, Sultan S, Glasziou P, Akl EA, Alonso-Coello P, Atkins D, Kunz R, Brozek J, Montori V, Jaeschke R, Rind D, Dahm P, Meerpohl J, Vist G, Berliner E, Norris S, Falck-Ytter Y, Murad MH, Schunemann HJ; GRADE Working Group. GRADE guidelines: 9. Rating up the quality of evidence. J Clin Epidemiol. 2011;64:1311–1316.
Henley MB, Chapman JR, Agel J, Harvey EJ, Whorton AM, Swiontkowski MF. Treatment of type II, IIIA, and IIIB open fractures of the tibial shaft: a prospective comparison of unreamed interlocking intramedullary nails and half-pin external fixators. J Orthop Trauma. 1998;12:1–7.
Higgins JP, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available at: http://www.cochrane.org/training/cochrane-handbook. Accessed February 15, 2014.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560.
Holbrook JL, Swiontkowski MF, Sanders R. Treatment of open fractures of the tibial shaft: Ender nailing versus external fixation. A randomized, prospective comparison. J Bone Joint Surg Am. 1989;71:1231–1238.
Jansen JP, Crawford B, Bergman G, Stam W. Bayesian meta-analysis of multiple treatment comparisons: an introduction to mixed treatment comparisons. Value Health. 2008;11:956–964.
Johal H, Schemitsch EH, Bhandari M. Why a decade of road traffic safety? J Orthop Trauma. 2014;28(suppl 1):S8–10.
Keating JF, O’Brien PJ, Blachut PA, Meek RN, Broekhuyse HM. Locking intramedullary nailing with and without reaming for open fractures of the tibial shaft: a prospective, randomized study. J Bone Joint Surg Am. 1997;79:334–341.
Lam SW, Teraa M, Leenen LP, van der Heijden GJ. Systematic review shows lowered risk of nonunion after reamed nailing in patients with closed tibial shaft fractures. Injury. 2010;41:671–675.
Larsen LB, Madsen JE, Hoiness PR, Ovre S. Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years’ follow-up. J Orthop Trauma. 2004;18:144–149.
Melvin JS, Dombroski DG, Torbert JT, Kovach SJ, Esterhai JL, Mehta S. Open tibial shaft fractures: II. Definitive management and limb salvage. J Am Acad Orthop Surg. 2010;18:108–117.
Mills EJ, Ioannidis JP, Thorlund K, Schunemann HJ, Puhan MA, Guyatt GH. How to use an article reporting a multiple treatment comparison meta-analysis. JAMA. 2012;308:1246–1253.
Mohseni MA, Soleimanpour J, Mohammadpour H, Shahsavari A. AO tubular external fixation vs. unreamed intramedullary nailing in open grade IIIA-IIIB tibial shaft fractures: a single-center randomized clinical trial. Pak J Biol Sci. 2011;14:490–495.
Papakostidis C, Kanakaris NK, Pretel J, Faour O, Morell DJ, Giannoudis PV. Prevalence of complications of open tibial shaft fractures stratified as per the Gustilo-Anderson classification. Injury. 2011;42:1408–1415.
Puhan MA, Schünemann HJ, Murad MH, Li T, Brignardello-Petersen R, Singh JA, Kessels AG, Guyatt GH; GRADE Working Group. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349:g5630.
Sackett DL, Haynes RB, Guyatt GH, Tugwell P. The clinical examination. Clinical Epidemiology: A Basic Science for Clinical Medicine. 2nd ed. Boston, MA: Little, Brown and Company; 1991:19–50.
Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. 2011;64:163–171.
Schemitsch EH, Kowalski MJ, Swiontkowski MF, Harrington RM. Comparison of the effect of reamed and unreamed locked intramedullary nailing on blood flow in the callus and strength of union following fracture of the sheep tibia. J Orthop Res. 1995;13:382–389.
Schemitsch EH, Kowalski MJ, Swiontkowski MF, Senft D. Cortical bone blood flow in reamed and unreamed locked intramedullary nailing: a fractured tibia model in sheep. J Orthop Trauma. 1994;8:373–382.
Schemitsch EH, Turchin DC, Kowalski MJ, Swiontkowski MF. Quantitative assessment of bone injury and repair after reamed and unreamed locked intramedullary nailing. J Trauma. 1998;45:250–255.
Scottish Intercollegiate Guidelines Network (SIGN) 2012. Available at: http://www.sign.ac.uk. Accessed January 17, 2014.
Shayesteh Azar M, Karimi Nasab MH, Sajadi Saravi M, Shafiee SE, Daneshpoor SM, Hadian A, Khademloo M. Comparison of intramedullary nailing and external fixation in the treatment of open tibial fractures. J Mazand Univ Med Sci. 2011;21:139–146.
Siddiqui A, Pirwani MA, Lal K, Rahman A. Reamed versus unreamed interlocking intra-medullary nailing for the fracture shaft tibia. Pak J Surg. 2009;25:53–57.
Soleimanpour J, Feizi HH, Mohseni MA, Moradi A, Arzromchilar A. Comparison between ender and unreamed interlocking nails in tibial shaft fractures. Saudi Med J. 2008;29:1458–1462.
Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators; Bhandari M, Guyatt G, Tornetta P 3rd, Schemitsch EH, Swiontkowski M, Sanders D, Walter SD. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. J Bone Joint Surg Am. 2008;90:2567–2578.
Tornetta P 3rd, Bergman M, Watnik N, Berkowitz G, Steuer J. Treatment of grade-IIIb open tibial fractures: a prospective randomised comparison of external fixation and non-reamed locked nailing. J Bone Joint Surg Br. 1994;76:13–19.
Tu YK, Lin CH, Su JI, Hsu DT, Chen RJ. Unreamed interlocking nail versus external fixator for open type III tibia fractures. J Trauma. 1995;39:361–367.
Vallier HA, Cureton BA, Patterson BM. Randomized, prospective comparison of plate versus intramedullary nail fixation for distal tibia shaft fractures. J Orthop Trauma. 2011;25:736–741.
Weiss RJ, Montgomery SM, Ehlin A, Al Dabbagh Z, Stark A, Jansson KA. Decreasing incidence of tibial shaft fractures between 1998 and 2004: information based on 10,627 Swedish inpatients. Acta Orthop. 2008;79:526–533.
Xue D, Zheng Q, Li H, Qian S, Zhang B, Pan Z. Reamed and unreamed intramedullary nailing for the treatment of open and closed tibial fractures: a subgroup analysis of randomised trials. Int Orthop. 2010;34:1307–1313.
Acknowledgments
We thank Joanne Petropoulos MSc, McMaster University, Canada, for helping with our comprehensive search; Chris Cameron PhD, Canadian Agency for Drugs and Technologies in Health, Canada, for statistical support; and Behzad Taromi MD, PhD, Trillium Heath Centre, Canada, for translation services.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
This study was performed at McMaster University, Hamilton, Ontario, Canada.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

Cite this article
Foote, C.J., Guyatt, G.H., Vignesh, K.N. et al. Which Surgical Treatment for Open Tibial Shaft Fractures Results in the Fewest Reoperations? A Network Meta-analysis. Clin Orthop Relat Res 473, 2179–2192 (2015). https://doi.org/10.1007/s11999-015-4224-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-015-4224-y