
Abstract
Purpose of review
The aim of this review is to provide practical guidance for clinicians to support the optimal use of endoscopy in both the diagnosis and the evaluation of treatment response in patients with eosinophilic esophagitis (EoE).
Recent findings
The systematic and high-quality assessment and grading of EoE endoscopic features improves EoE detection. Fibrotic complications of EoE that negatively impact patients’ symptoms and quality of life can be detected and treated through endoscopy. The correlation between endoscopic features of EoE and histological activity remains challenging. However, assessment of endoscopic activity is fast and reliable in the evaluation of treatment response and, therefore, is supported by current guidelines. New modalities such as FLIP panometry and molecular markers for diagnosis and monitoring of EoE are promising, but whether they may replace endoscopy in guiding treatment of EoE needs to be ascertained.
Summary
Endoscopy plays a central role in EoE management, both in routine practice and in clinical trials. Endoscopy is pivotal in EoE diagnosis and response evaluation since it allows the direct assessment of endoscopic disease activity and, indirectly, the histological evaluation. Consequently, together with clinical and histological evaluation, endoscopy is rapidly becoming essential in monitoring the effectiveness of therapy in patients with EoE.
Similar content being viewed by others


Introduction
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated disease characterized by histological evidence of eosinophil-predominant inflammation. [1] EoE was first described in 1993 by Attwood et al. and is currently considered one of the most prevalent esophageal diseases. [2] According to guidelines, EoE is diagnosed in patients with relevant esophageal symptoms, the most common of which are dysphagia and food impaction, and a peak eosinophil count (PEC) on esophageal biopsies ≥ 15 in at least one high-power field (standard size of 0.3 mm2) in any biopsy specimen, after exclusion of other causes of esophageal eosinophilia [3•].
EoE has a remarkable negative impact on the patient’s quality of life. [4] The incidence and prevalence of EoE are rising in adults and children. [5, 6] The estimated incidence from population-based studies ranges from 5 to 10 cases per 100,000 person-years, and the prevalence is approximately 50 to 100 per 100,000 persons. [7] Compared to previous studies, a recent wide population study reported higher incidence rates of EoE in Denmark, with a standardized incidence from 2008 to 2018 of 11.7 (95% CI 10.8–12.6) per 100,000 person‐years. [5] Nevertheless, it still remains unclear whether the reported increased incidence over time reflects an authentic growth or is rather an expression of the increased awareness of the disease and better adherence to guidelines [8].
Upper gastrointestinal endoscopy represents a cornerstone not only in the diagnosis of EoE, but also in the follow-up. Moreover, endoscopy allows the treatment of the fibrotic complications of chronic esophageal inflammation, such as strictures or diffuse narrowing of the esophagus. The aim of this review is to provide practical guidance for clinicians to support the optimal use of endoscopy in both the diagnosis and the response evaluation of patients with EoE.
Methods
A literature search was conducted in the EMBASE, MEDLINE, and Cochrane databases using the following individual and combined Medical Subject Heading (MeSH) terms: “Eosinophilic esophagitis,” “endoscopy,” “diagnosis,” “response evaluation,” “treatment response,” “monitoring.” Papers published up to 20 December 2022 in the English language were included. References cited in the articles selected were also searched in order to identify other potential sources of information.
Endoscopy in the diagnosis of eosinophilic esophagitis
Endoscopy plays a critical role in the diagnosis and management of EoE. As far as diagnosis is concerned, endoscopy is essential to (1) assess the endoscopic activity of the disease, (2) evaluate the presence of local and systemic causes of esophageal eosinophilia other than EoE (Table 1), and (3) obtain esophageal biopsies.
EoE can be difficult to diagnose since the clinical and endoscopic features can be non-specific and often subtle. In fact, up to 7–32% of adult and pediatric patients diagnosed with EoE, respectively, initially present a normal-appearing esophagus. [9, 10] Moreover, strict adherence to guidelines is lacking [11] and, consequently, endoscopists should perform an excellent endoscopic examination with a high level of suspicion to maximize the diagnostic yield of endoscopy. EoE is currently burdened by a remarkable diagnostic delay, both secondary to patient- and physician-dependent factors. [12] A study by Navarro et al. recently reported a considerable decrease in the diagnostic delay of EoE over a period of 10 years, from 12.7 years in 2007 to 7 months in 2017. [13] On the other hand, a recent Swiss study reported an unchanged diagnostic delay of EoE since its first description almost 30 years ago, with a median diagnostic delay of 4 years (IQR: 1–11, range, 0–56) and diagnostic delay ≥ 10 years in 32% of the patients. [14] In addition, EoE is frequently confused with other conditions. It has been shown that a previous diagnosis of GERD is reported in approximately one-fourth of patients. [12, 15] The diagnostic delay may lead to a more complicated course since the prevalence of fibrotic features of EoE is directly related to the duration of untreated disease. [16] Hence, an early diagnosis is of utmost importance to reduce this risk of complications and improve patient outcomes.
Endoscopic features of eosinophilic esophagitis
Endoscopic hallmarks of EoE include mucosal pallor or decreased vasculature (i.e., edema—prevalence 41% in patients with EoE), esophageal rings (i.e., trachealization—prevalence 44%), longitudinal furrows (prevalence 48%), white plaques or exudates (prevalence 27%), and esophageal strictures (prevalence 21%). [9, 17, 18] Additionally, fragile esophageal mucosa that readily tears in response to minor trauma (i.e., crepe paper esophagus) and narrow caliber esophagus are common among patients with EoE, although their frequency is unknown. [9, 17] Among the aforementioned endoscopic features, the presence of edema, white exudates, and furrows is an expression of active inflammation, whereas rings and strictures reflect fibrotic remodeling (Table 2). EoE-related strictures can occur anywhere along the length of the esophagus, but the distal esophagus is the most commonly involved site. [19] Not infrequently, gastroenterologists underestimate the presence of strictures in EoE during endoscopy. [20] Another frequent endoscopic finding is erosive esophagitis due to gastroesophageal reflux disease (GERD), frequently observed (prevalence 17%) in patients with EoE due to the coexistence of GERD. [9] Although controversy still exists about the relationship between EoE and GERD, it was suggested that GERD may also contribute to the development, and exacerbation, of EoE and vice versa [21].
In 2013, the EoE Endoscopic Reference Score (EREFS) has been developed and validated for the quantification of the five major endoscopic features of EoE (Table 2). EREFS was introduced to standardize the definition and grading of endoscopic features and, ultimately, to ascertain the disease activity of patients [22].
Each endoscopic feature of the EREFS score should be graded based on the most involved esophageal area. [23] By doing so, the endoscopic severity of EoE is graded from 0 to 9, with higher scores indicating more severe endoscopic disease activity. Some authors recommend, to avoid mistakes in the reporting of the EREFS findings, abbreviating the second “E” of the score as “Ex” to distinguish between edema and exudates (Fig. 1) [24].

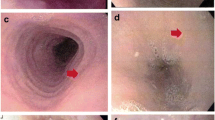
Example of EREFS reporting. In this patient’s esophagus, there are edema, mild fixed rings, and mild vertical furrows. White exudates and strictures are absent. Therefore, this esophagus could be graded in the endoscopic report as E1R1Ex0F1S0
The EREFS classification system showed an excellent ability to predict the presence of the disease in a prospective validation study (area under the receiver operator characteristic curve of 0.934). [25] Inter- and intra-observer agreement of EREFS score is good to moderate (Table 2), and not substantially different between expert and trainee endoscopists, showing the reliability and ease of using the scoring system [26].
Providing a practical checklist for endoscopy with the hallmarks of EoE, the great value of the EREFS classification system is not only the standardization of the endoscopic report, but also the enhanced detection of endoscopic signs of the disease in patients with suspected EoE. In fact, the prevalence of patients with EoE and a normal endoscopic examination is lower in prospective studies (7%) as compared to retrospective studies (17%), meaning that the systematic esophageal evaluation results in greater detection of at least one normal endoscopic finding (prospective 93% versus retrospective 80%). [9]. This is probably secondary to the systematic use of EREFS score during endoscopy in prospective studies resulting in improved detection of subtle EoE hallmarks compared to the retrospective series. While the European guidelines published in 2017 [27] did not clarify the role of EREFS for disease activity assessment, the routine use of the score during endoscopy was recently recommended in a consensus study published in 2022 by the American Society for Gastrointestinal Endoscopy (ASGE) [28].
Correlation between endoscopy and histology
Despite a fair to good inter-observer and intra-observer agreement and a good response to treatment for EoE, the accuracy of the EREFS score in predicting either clinical or histological activity is modest. [25, 29, 30] It should be underlined that, according to the previous definition of EoE, these studies were based on patients unresponsive to an 8-week trial of PPI therapy. This does no longer represent the current diagnostic criteria for the diagnosis of EoE [31].
In a multicenter prospective study conducted in Spain, only whitish exudates showed a good correlation with the peak eosinophil count and histological outcome after therapy with steroids, while the other endoscopic features of EoE remained mostly unchanged after histological remission. Nevertheless, all the individual endoscopic features and the EREFS scores (inflammatory, fibrotic, and total) showed an accuracy of < 70% to predict histological remission. [29] Due to the modest accuracy of endoscopy to predict histological activity, an endoscopic sample with subsequent histological evaluation remains irreplaceable to monitoring therapy effectiveness in patients affected by EoE. Therefore, the identification of a reliable non-invasive biomarker to replace endoscopy with biopsy in diagnosis and monitoring remains one of the critical unmet needs in EoE.
Correlation of endoscopy with symptoms and quality of life
The endoscopic appearance of EoE is correlated with patients’ symptoms. Fibrostenotic features of the esophagus are associated with dysphagia and food impaction. [32] In particular, the endoscopic presence of strictures is associated with a history of self-limited food impactions (P < 0.001). Eighty-eight percent of patients with a stricture diameter ≤ 12 mm had a history of self-limited impactions, compared to 45% of patients with a stricture ≥ 18 mm and 19% of patients without a stricture. [32] Increased ring severity (e.g., rings that do not allow the passage of a diagnostic endoscope) was also associated with a higher likelihood of food impaction [32].
Nevertheless, symptoms are not accurate in predicting the endoscopic and histologic remission of patients with EoE. [27] In a prospective multicenter study, the correlation between symptoms (eosinophilic esophagitis activity index patient-reported outcome (EEsAI PRO)) and both endoscopic and histologic activity was only modest. [33] These data are in line with a Spanish prospective multicenter study reporting on the lack of a correlation between EREFS and clinical activity evaluated through the Dysphagia Symptom Score. [29] There was an absence of correlation between dysphagia and endoscopic appearance even after evaluating the inflammatory (I-EREFS) and fibrotic (F-EREFS) features of EoE separately [29].
Existing data are conflicting regarding the correlation between the endoscopic appearance of EoE and quality of life (QoL), an important treatment outcome of affected patients. While the study by Stern et al. did not find a correlation of QoL with endoscopic features [32], another prospective multicenter study showed that the severity of fixed rings, strictures, exudates, and furrows was significantly associated with a worse QoL. No significant correlation was found between the presence of edema and the QoL score [34].
The duration of untreated disease is associated with esophageal remodeling and dysmotility and, therefore, with impaired quality of life [16, 35, 36].
How to perform high-quality endoscopy in suspected and established eosinophilic esophagitis
High-quality endoscopy is key in patients with suspected or established EoE to maximize diagnostic yield and improve subsequent treatment preventing esophageal fibrosis. The following steps should be considered during an esophagogastroduodenoscopy (EGD) performed for diagnosis or follow-up of EoE (Fig. 2).

High-quality endoscopy in eosinophilic esophagitis
Firstly, the esophagus should be examined before advancing the scope into the stomach or duodenum because sweeping away the white exudates or creating mucosal breaks by scope passage will alter the EREFS score. It is also important to advance the scope slowly since pushing it “blindly” against a stricture may be harmful. Second, the esophageal mucosa should be carefully cleaned with the water jet to remove saliva, mucus, and other debris. Thereafter, the esophagus should be fully insufflated to perform a high-quality evaluation of the features of the EREFS score, therefore optimally estimating the extent of the edema, the depth of vertical furrows, and the severity of fixed rings. Mucosal ring-like structures that completely disappear upon esophageal insufflation are not classified as rings on ERFES. The fourth essential issue is to take enough time to accurately assess the esophagus. After a complete inspection of the esophagus, if indicated, biopsies can be obtained. If an endoscopic dilation is performed, it is important to completely inspect the upper GI tract since the procedure would be unsafe in presence of food or fluid in the stomach.
From a practical standpoint, in which patients should we suspect EoE and obtain esophageal biopsies? EoE is a frequent diagnosis in patients with a history of dysphagia and/or food impaction, especially in the presence of atopic comorbidities (e.g., allergic rhinitis, asthma, or atopic dermatitis) or family history of EoE.[37, 38] The clinical index of suspicion should be increased in young men and people of white ethnic origin since the disease is more common in these groups.[39, 40] It is estimated that up to 15% of patients with dysphagia undergoing endoscopy are diagnosed with EoE.[41, 42] Therefore, current guidelines recommend esophageal biopsies in all adults with endoscopic signs of EoE, or with symptoms of dysphagia and/or food impaction, even with a normal-appearing esophagus.[3•, 27] Instead, esophageal biopsies are not recommended in patients with GERD symptoms refractory to proton pump inhibitors without clinical features associated with EoE [3•], given the low prevalence of EoE in this clinical scenario [43, 44].
Current guidelines also recommend esophageal biopsies during the EGD performed for food bolus impaction in patients without a known diagnosis of eosinophilic esophagitis. [3•, 28] Indeed, affecting over 40% of patients who underwent biopsy for food bolus impaction, EoE is the most frequently detected cause of food impaction. [45] Moreover, 79% of patients are lost to follow-up if biopsies are not taken during index endoscopy. [46] Despite this evidence, esophageal biopsies are obtained in less than half of patients who undergo EGD for food bolus impaction in routine practice. [45, 47, 48] In this setting, esophageal biopsies are safe and not associated with an increased rate of perforation. [49, 50] In the rare situation where it is considered unsafe to obtain biopsies after food bolus dis-impaction (patient instability or high risk of aspiration), it is essential to reschedule EGD for subsequent esophageal biopsy to maximize the possibility to diagnose and treat EoE.
Because the eosinophilic esophageal inflammation of EoE is patchy and variable within each specimen, it is recommended to take at least six biopsies in total from at least two different anatomical sites within the esophagus, targeting areas with endoscopic mucosal abnormalities (especially white exudates and longitudinal furrows) to increase sensitivity. [27, 51•] A common approach is to obtain three to four biopsies from both the proximal and the distal esophagus [52].
Whether to place biopsy specimens from different (e.g., proximal and distal) areas of the esophagus into one or separate jars is still a matter of debate. [28] A peak concentration of ≥ 15 eosinophils in at least one high-power field (standard size of 0.3 mm2) is the accepted threshold for the diagnosis of EoE, in either the proximal or the distal esophagus. The use of different jars entails economic and environmental costs. [53, 54] Current ESGE guidelines on endoscopic tissue sampling suggest using separate histology jars [51•], while EoE guidelines do not provide a specific statement addressing this issue. [43•, ] However, the ESGE recommendation is supported by a low quality of evidence and it is still unclear whether this practice could improve patient management.
The “turn and suck” is the optimal technique to obtain accurate esophageal targeted biopsies. The technique consists in opening the biopsy forceps, pulling them back against the scope, and then closing the forceps after rotating the scope while aspirating the mucosa. Before the biopsy is obtained, the catheter may be moderately advanced to confirm the targeted area has been captured [24].
To exclude a concomitant eosinophilic gastritis and/or enteritis, duodenal and gastric mucosal biopsies should be considered at the moment of initial diagnosis of EoE, especially in patients with symptoms suggestive of gastric and/or duodenal involvement or endoscopic mucosal abnormalities [27, 28].
Endoflip as a novel diagnostic modality for eosinophilic esophagitis
In 2011, Kwiatek et al. reported for the first time the application of the functional luminal imaging probe (FLIP) in EoE. [55] The FLIP panometry has the potential to measure the luminal cross-sectional area (CSA) of the esophagus through a high-resolution impedance planimetry that provides a three-dimensional image of the esophageal lumen. FLIP panometry assesses pressure changes, diameter, and volume of the esophagus, therefore enabling the evaluation of its distensibility. [56•] The compliance of both the esophageal wall and the esophagogastric junction (EGJ) can be measured by the FLIP. [57] There is growing evidence regarding the application of this technique to EoE. [58, 59] Available studies have shown that esophageal compliance is decreased in patients with EoE, that this is associated with food impaction, and that successful treatment, as shown by histological remission, results in improved distensibility and increased esophageal luminal caliber. [59,60,61] Esophageal distensibility evaluated through FLIP is currently being assessed as a secondary endpoint in clinical trials [62].
In the future, the FLIP panometry could represent a useful tool in clinical practice to detect strictures in patients with EoE and persistent dysphagia despite histological remission and the absence of fibrotic features at endoscopy. [3•] FLIP can also define stricture anatomy and provide an accurate diameter of esophageal strictures, hence guiding the selection of the caliber of the dilators [56•].
Since strictures can also be detected by barium esophagram and EGD, the cost-effectiveness of an invasive and expensive tool such as FLIP in this setting needs to be ascertained by future research.
The functional assessment with FLIP could be used as a novel outcome measure in the evaluation and monitoring of disease severity. [63] In fact, since esophageal narrowing can be underestimated during endoscopy [20], FLIP panometry could improve the detection of strictures. [64] Despite these promising results, the role of FLIP in everyday clinical practice for EoE has yet to be determined.
Endoscopy in response evaluation of patients with eosinophilic esophagitis
There is no single parameter to reliably assess EoE disease activity. The patient’s perception of symptoms alone is unreliable since it can be improved by adaptative eating behaviors and worsened by hypervigilance and anxiety. [65, 66] Histology alone could be misleading due to the patchiness of eosinophilic inflammation and the presence of complementary histological features suggestive of active eosinophilic flogosis in EoE (e.g., basal cell hyperplasia, eosinophilic microabscesses and degranulation, fibrosis of the lamina propria) that are not part of the PEC. [67] Furthermore, histology can only partially assess the presence of esophageal fibrotic damage related to chronic inflammation. Consequently, together with clinical and histological evaluation, endoscopy is rapidly gaining importance in monitoring the effectiveness of therapy in patients with EoE.
Role of endoscopy in the assessment of disease activity
Assessment of endoscopic activity is fast and reliable, although it may overall correlate poorly with symptoms and a considerable number of patients affected by EoE have a normal-appearing esophagus. Due to the accuracy in diagnosis and assessment of treatment effects in both children and adults [25, 68], the assessment of endoscopic activity by the EREFS score has been widely used in randomized placebo-controlled trials for EoE, increasingly using blinded central readers in contrast to the local endoscopist. [62, 69, 70] In this setting, endoscopic activity is an objective and reliable measurement since the EREFS score showed responsiveness to therapy and remained unchanged after the administration of a placebo. [62, 69, 70] On the contrary, there is a high symptomatic response to placebo in RCTs. Therefore, together with patient-reported outcomes [71, 72] and histology [67], endoscopic activity is fundamental in the evaluation of EoE disease activity and patients’ response to treatments. In a recent study, a panel of gastroenterology and immunology experts created a composite severity scoring system (Index of Severity for Eosinophilic Esophagitis [I-SEE]) to guide EoE management. [63] The score considers clinical activity together with inflammatory and fibrostenotic features on endoscopic and histologic examination to standardize assessment of disease severity beyond eosinophil counts. In a recent international multidisciplinary consensus study, a core outcome set for Eosinophilic Esophagitis (COREOS) was defined to reduce the heterogeneity in the reported outcome measures in clinical studies. [73•] According to this study, for both RCTs and observational studies, endoscopic remission should be defined on the basis of an EREFS ≤ 2. [73•] In particular, endoscopic inflammatory EREFS-based remission should be defined as inflammation-associated components (exudate, edema, furrows) score of ≤ 2, while the absence of strictures and moderate and severe rings defines the endoscopic fibrotic EREFS-based remission. A novel tool to assess response in EoE includes the use of molecular markers (a cluster of genes associated with for instance inflammation or remodeling). [74] A recent study by Ruffner et al. suggests that the use of post-treatment response thresholds EREFS ≤ 2 is supported by gene expression profiles in clinical practice and trials [74].
Although there is some evidence regarding a possible improvement of histological fibrosis [59, 75, 76] and an increase of esophageal lumen [77] after therapy, the available treatments for EoE primarily aim to reduce the esophageal eosinophilic inflammation. As a result, the improvement of previously identified endoscopic inflammatory features represents a desired, important, and easily assessed endpoint of treatments [28].
After starting a new treatment, EGD should be scheduled after at least 8–12 weeks of continuous therapy in order to obtain an optimal evaluation of the endoscopic and histological response. [78••] In case of objective treatment unresponsiveness, it is essential to assess the adherence of the patient before changing therapy, since treatment compliance is poor in many adult patients with EoE, particularly in younger ones. [79] The optimal timing for assessment of treatment effect is still debated and varies in therapeutic interventional trials. The clinical picture of the patient, the risk of food impaction, and the presence of stenosis, as well as the reported outcome of the prescribed dietary or medical treatment, should be taken into account in clinical practice to tailor the timing to the patient’s needs and expectations. [78••] Future studies are needed to evaluate the usefulness and the optimal timing of periodic endoscopic and histologic assessments in patients in clinical and histological remission and the absence of therapy modifications. In stable patients with previously documented remission, the advantage of an objective endoscopic assessment over time should be weighed against the disadvantage of financial, social, and environmental costs [53] and discomfort for patients due to repeated EGD.
Endoscopic surveillance for esophageal neoplasia is not recommended by guidelines in patients with EoE. [4] Evidence from a large cross-sectional population-based study showed no association between esophageal cancer and EoE. [80] Despite the need for larger prospective long-term studies, there is currently no evidence that EoE may represent an esophageal pre-malignant condition, and routine surveillance endoscopies for that purpose are not recommended.
Conclusion
Endoscopy plays a central role in EoE management, both in routine practice and in clinical trials. Endoscopy is pivotal in EoE diagnosis and response evaluation since it allows the direct assessment of endoscopic disease activity and, indirectly, the histological evaluation. Moreover, endoscopy is useful for treating food bolus impaction and dilating the esophagus in patients with endoscopic signs of fibrosis that are symptomatic despite an effective anti-inflammatory drug or dietary treatment.
Since endoscopy has relevant social, financial, and environmental costs, future research is needed to clarify whether non-invasive biomarkers could replace it in the diagnosis and monitoring of patients. Moreover, it is still unclear whether periodic endoscopic assessment leads to improved outcomes in patients with documented clinical and histological remission and unchanged therapy.
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Liacouras CA, et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults, (in eng). J Allergy Clin Immunol. 2011;128(1):3-20.e6. https://doi.org/10.1016/j.jaci.2011.02.040.
Attwood SE, Smyrk TC, Demeester TR, Jones B. Esophageal eosinophilia with dysphagia A distinct clinicopathologic syndrome, (in eng). Dig Dis Sci. 1993;38(1):109–16. https://doi.org/10.1007/bf01296781.
• Dhar A, et al. British Society of Gastroenterology (BSG) and British Society of Paediatric Gastroenterology, Hepatology and Nutrition (BSPGHAN) joint consensus guidelines on the diagnosis and management of eosinophilic oesophagitis in children and adults, (in eng). Gut. 2022;71(8):1459–87. https://doi.org/10.1136/gutjnl-2022-327326. Clear recommendations on clinical management of EoE.
Lucendo AJ, Arias-González L, Molina-Infante J, Arias Á. Systematic review: health-related quality of life in children and adults with eosinophilic oesophagitis-instruments for measurement and determinant factors, (in eng). Aliment Pharmacol Ther. 2017;46(4):401–9. https://doi.org/10.1111/apt.14194.
Allin KH, Poulsen G, Melgaard D, Frandsen LT, Jess T, Krarup AL. Eosinophilic oesophagitis in Denmark: population-based incidence and prevalence in a nationwide study from 2008 to 2018, (in eng). United Eur Gastroenterol J. 2022;10(7):640–50. https://doi.org/10.1002/ueg2.12273.
Navarro P, Arias Á, Arias-González L, Laserna-Mendieta EJ, Ruiz-Ponce M, Lucendo AJ. Systematic review with meta-analysis: the growing incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies, (in eng). Aliment Pharmacol Ther. 2019;49(9):1116–25. https://doi.org/10.1111/apt.15231.
Dellon ES, Hirano I. Epidemiology and natural history of eosinophilic esophagitis, (in eng). Gastroenterology. 2018;154(2):319-332.e3. https://doi.org/10.1053/j.gastro.2017.06.067.
Masclee GMC, Bredenoord AJ. Incidence and prevalence of eosinophilic oesophagitis: are we reaching a plateau?, (in eng). United Eur Gastroenterol J. 2022;10(7):623–4. https://doi.org/10.1002/ueg2.12282.
Kim HP, Vance RB, Shaheen NJ, Dellon ES. The prevalence and diagnostic utility of endoscopic features of eosinophilic esophagitis: a meta-analysis, (in eng). Clin Gastroenterol Hepatol. 2012;10(9):988-96.e5. https://doi.org/10.1016/j.cgh.2012.04.019.
Liacouras CA, et al. Eosinophilic esophagitis: a 10-year experience in 381 children, (in eng). Clin Gastroenterol Hepatol. 2005;3(12):1198–206. https://doi.org/10.1016/s1542-3565(05)00885-2.
Eluri S, Iglesia EGA, Massaro M, Peery AF, Shaheen NJ, Dellon ES. Practice patterns and adherence to clinical guidelines for diagnosis and management of eosinophilic esophagitis among gastroenterologists, (in eng). Dis Esophagus. 2020;33(7). https://doi.org/10.1093/dote/doaa025.
Lenti MV, et al. Diagnostic delay and misdiagnosis in eosinophilic oesophagitis, (in eng). Dig Liver Dis. 2021;53(12):1632–9. https://doi.org/10.1016/j.dld.2021.05.017.
Navarro P, et al. Accurate and timely diagnosis of eosinophilic esophagitis improves over time in Europe. An analysis of the EoE CONNECT Registry, (in eng). United European Gastroenterol J. 2022;10(5):507–17. https://doi.org/10.1002/ueg2.12240.
Murray FR, et al. Diagnostic delay in patients with eosinophilic esophagitis has not changed since first description 30 years ago, (in eng). Am J Gastroenterol. 2022. https://doi.org/10.14309/ajg.0000000000001950.
Dellon ES, Farrell TM, Bozymski EM, Shaheen NJ. Diagnosis of eosinophilic esophagitis after fundoplication for ‘refractory reflux’: implications for preoperative evaluation, (in eng). Dis Esophagus. 2010;23(3):191–5. https://doi.org/10.1111/j.1442-2050.2009.01019.x.
Schoepfer AM, et al. Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner, (in eng). Gastroenterology. 2013;145(6):1230-6.e1-2. https://doi.org/10.1053/j.gastro.2013.08.015.
Straumann A, Rossi L, Simon HU, Heer P, Spichtin HP, Beglinger C. Fragility of the esophageal mucosa: a pathognomonic endoscopic sign of primary eosinophilic esophagitis?, (in eng). Gastrointest Endosc. 2003;57(3):407–12. https://doi.org/10.1067/mge.2003.123.
Straumann A, Spichtin HP, Bucher KA, Heer P, Simon HU. Eosinophilic esophagitis: red on microscopy, white on endoscopy, (in eng). Digestion. 2004;70(2):109–16. https://doi.org/10.1159/000080934.
Eluri S, et al. Distal esophagus is the most commonly involved site for strictures in patients with eosinophilic esophagitis, (in eng). Dis Esophagus. 2020;33(2). https://doi.org/10.1093/dote/doz088.
Gentile N, et al. Oesophageal narrowing is common and frequently under-appreciated at endoscopy in patients with oesophageal eosinophilia, (in eng). Aliment Pharmacol Ther. 2014;40(11–12):1333–40. https://doi.org/10.1111/apt.12977.
Spechler SJ. Gastroesophageal reflux disease and eosinophilic esophagitis, (in eng). Gastroenterol Hepatol (N Y). 2019;15(2):111–3.
Hirano I, Moy N, Heckman MG, Thomas CS, Gonsalves N, Achem SR. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system, (in eng). Gut. 2013;62(4):489–95. https://doi.org/10.1136/gutjnl-2011-301817.
Ma C, et al. Reliability and responsiveness of endoscopic disease activity assessment in eosinophilic esophagitis, (in eng). Gastrointest Endosc. 2022;95(6):1126-1137.e2. https://doi.org/10.1016/j.gie.2022.01.014.
Dellon ES. Optimizing the endoscopic examination in eosinophilic esophagitis, (in eng). Clin Gastroenterol Hepatol. 2021;19(12):2489-2492.e1. https://doi.org/10.1016/j.cgh.2021.07.011.
Dellon ES, et al. Accuracy of the eosinophilic esophagitis Endoscopic Reference Score in diagnosis and determining response to treatment, (in eng). Clin Gastroenterol Hepatol. 2016;14(1):31–9. https://doi.org/10.1016/j.cgh.2015.08.040.
van Rhijn BD, et al. Evaluating the Endoscopic Reference Score for eosinophilic esophagitis: moderate to substantial intra- and interobserver reliability, (in eng). Endoscopy. 2014;46(12):1049–55. https://doi.org/10.1055/s-0034-1377781.
Lucendo AJ, et al. Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults, (in eng). United Eur Gastroenterol J. 2017;5(3):335–58. https://doi.org/10.1177/2050640616689525.
Aceves SS, et al. Endoscopic approach to eosinophilic esophagitis: American Society for Gastrointestinal Endoscopy Consensus Conference, (in eng). Gastrointest Endosc. 2022;96(4):576-592.e1. https://doi.org/10.1016/j.gie.2022.05.013.
Rodríguez-Sánchez J, et al. The Endoscopic Reference Score shows modest accuracy to predict either clinical or histological activity in adult patients with eosinophilic oesophagitis, (in eng). Aliment Pharmacol Ther. 2017;45(2):300–9. https://doi.org/10.1111/apt.13845.
van Rhijn BD, Verheij J, Smout AJ, Bredenoord AJ. The Endoscopic Reference Score shows modest accuracy to predict histologic remission in adult patients with eosinophilic esophagitis, (in eng). Neurogastroenterol Motil. 2016;28(11):1714–22. https://doi.org/10.1111/nmo.12872.
Dellon ES, Gonsalves N, Hirano I, Furuta GT, Liacouras CA, Katzka DA. ACG clinical guideline: evidenced based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis (EoE), (in eng). Am J Gastroenterol. 2013;108(5):679–92. https://doi.org/10.1038/ajg.2013.71. (quiz 693).
Stern E, Taft T, Zalewski A, Gonsalves N, Hirano I. Prospective assessment of disease-specific quality of life in adults with eosinophilic esophagitis, (in eng). Dis Esophagus. 2018;31(4). https://doi.org/10.1093/dote/dox128.
Safroneeva E, et al. Symptoms have modest accuracy in detecting endoscopic and histologic remission in adults with eosinophilic esophagitis, (in eng). Gastroenterology. 2016;150(3):581-590.e4. https://doi.org/10.1053/j.gastro.2015.11.004.
Safroneeva E, et al. Eosinophilic oesophagitis: relationship of quality of life with clinical, endoscopic and histological activity, (in eng). Aliment Pharmacol Ther. 2015;42(8):1000–10. https://doi.org/10.1111/apt.13370.
Warners MJ, Oude Nijhuis RAB, de Wijkerslooth LRH, Smout A, Bredenoord AJ. The natural course of eosinophilic esophagitis and long-term consequences of undiagnosed disease in a large cohort, (in eng). Am J Gastroenterol. 2018;113(6):836–44. https://doi.org/10.1038/s41395-018-0052-5.
Carlson DA, et al. Esophageal dysmotility is associated with disease severity in eosinophilic esophagitis, (in eng). Clin Gastroenterol Hepatol. 2022;20(8):1719-1728.e3. https://doi.org/10.1016/j.cgh.2021.11.002.
Laserna-Mendieta EJ, et al. Differences between childhood- and adulthood-onset eosinophilic esophagitis: an analysis from the EoE connect registry, (in eng). Dig Liver Dis. 2022. https://doi.org/10.1016/j.dld.2022.09.020.
Straumann A, Spichtin HP, Grize L, Bucher KA, Beglinger C, Simon HU. Natural history of primary eosinophilic esophagitis: a follow-up of 30 adult patients for up to 11.5 years, (in eng). Gastroenterology. 2003;125(6):1660–9. https://doi.org/10.1053/j.gastro.2003.09.024.
Kapel RC, Miller JK, Torres C, Aksoy S, Lash R, Katzka DA. Eosinophilic esophagitis: a prevalent disease in the United States that affects all age groups, (in eng). Gastroenterology. 2008;134(5):1316–21. https://doi.org/10.1053/j.gastro.2008.02.016.
Alexander ES, et al. Twin and family studies reveal strong environmental and weaker genetic cues explaining heritability of eosinophilic esophagitis, (in eng). J Allergy Clin Immunol. 2014;134(5):1084-1092.e1. https://doi.org/10.1016/j.jaci.2014.07.021.
Mackenzie SH, et al. Eosinophilic oesophagitis in patients presenting with dysphagia–a prospective analysis, (in eng). Aliment Pharmacol Ther. 2008;28(9):1140–6. https://doi.org/10.1111/j.1365-2036.2008.03795.x.
Prasad GA, et al. Prevalence and predictive factors of eosinophilic esophagitis in patients presenting with dysphagia: a prospective study, (in eng). Am J Gastroenterol. 2007;102(12):2627–32. https://doi.org/10.1111/j.1572-0241.2007.01512.x.
Sá CC, et al. Eosinophilic esophagitis in patients with typical gastroesophageal reflux disease symptoms refractory to proton pump inhibitor, (in eng). Clinics (Sao Paulo). 2011;66(4):557–61. https://doi.org/10.1590/s1807-59322011000400006.
Poh CH, et al. Upper GI tract findings in patients with heartburn in whom proton pump inhibitor treatment failed versus those not receiving antireflux treatment, (in eng). Gastrointest Endosc. 2010;71(1):28–34. https://doi.org/10.1016/j.gie.2009.08.024.
Sperry SL, Crockett SD, Miller CB, Shaheen NJ, Dellon ES. Esophageal foreign-body impactions: epidemiology, time trends, and the impact of the increasing prevalence of eosinophilic esophagitis, (in eng). Gastrointest Endosc. 2011;74(5):985–91. https://doi.org/10.1016/j.gie.2011.06.029.
Chang JW, et al. Loss to follow-up after food impaction among patients with and without eosinophilic esophagitis, (in eng). Dis Esophagus. 2019;32(12). https://doi.org/10.1093/dote/doz056.
Cook D, Zala A, Bollipo S, Potter MDE, Walker MM, Talley NJ. Oesophageal food bolus obstruction and eosinophilic oesophagitis, (in eng). Intern Med J. 2019;49(8):1032–4. https://doi.org/10.1111/imj.14389.
Schreiner P, et al. Management of eosinophilic esophagitis associated food impaction in Europe and the United States, (in eng). Dis Esophagus. 2022;35(9). https://doi.org/10.1093/dote/doac003.
Wolf WA, et al. Association between body mass index and clinical and endoscopic features of eosinophilic esophagitis, (in eng). Dig Dis Sci. 2017;62(1):143–9. https://doi.org/10.1007/s10620-016-4357-1.
Arias-González L, Rey-Iborra E, Ruiz-Ponce M, Laserna-Mendieta EJ, Arias Á, Lucendo AJ. Esophageal perforation in eosinophilic esophagitis: a systematic review on clinical presentation, management and outcomes, (in eng). Dig Liver Dis. 2020;52(3):245–52. https://doi.org/10.1016/j.dld.2019.10.019.
• Pouw RE, et al. Endoscopic tissue sampling - part 1: upper gastrointestinal and hepatopancreatobiliary tracts. European Society of Gastrointestinal Endoscopy (ESGE) Guideline, (in eng). Endoscopy. 2021;53(11):1174–88. https://doi.org/10.1055/a-1611-5091. (Evidence-based recommendations on biopsy sampling in the GI tract.)
Nielsen JA, Lager DJ, Lewin M, Rendon G, Roberts CA. The optimal number of biopsy fragments to establish a morphologic diagnosis of eosinophilic esophagitis, (in eng). Am J Gastroenterol. 2014;109(4):515–20. https://doi.org/10.1038/ajg.2013.463.
Bortoluzzi F, et al. Sustainability in gastroenterology and digestive endoscopy: Position Paper from the Italian Association of Hospital Gastroenterologists and Digestive Endoscopists (AIGO), (in eng). Dig Liver Dis. 2022;54(12):1623–9. https://doi.org/10.1016/j.dld.2022.08.018.
Gordon IO, Sherman JD, Leapman M, Overcash M, Thiel CL. Life cycle greenhouse gas emissions of gastrointestinal biopsies in a surgical pathology laboratory, (in eng). Am J Clin Pathol. 2021;156(4):540–9. https://doi.org/10.1093/ajcp/aqab021.
Kwiatek MA, Hirano I, Kahrilas PJ, Rothe J, Luger D, Pandolfino JE. Mechanical properties of the esophagus in eosinophilic esophagitis, (in eng). Gastroenterology. 2011;140(1):82–90. https://doi.org/10.1053/j.gastro.2010.09.037.
• Savarino E, et al. Use of the functional lumen imaging probe in clinical esophagology, (in eng). Am J Gastroenterol. 2020;115(11):1786–96. https://doi.org/10.14309/ajg.0000000000000773. (Practical guide on the use of FLIP in the esophagus.)
McMahon BP, Frøkjaer JB, Liao D, Kunwald P, Drewes AM, Gregersen H. A new technique for evaluating sphincter function in visceral organs: application of the functional lumen imaging probe (FLIP) for the evaluation of the oesophago-gastric junction, (in eng). Physiol Meas. 2005;26(5):823–36. https://doi.org/10.1088/0967-3334/26/5/019.
Desprez C, Roman S, Leroi AM, Gourcerol G. The use of impedance planimetry (Endoscopic Functional Lumen Imaging Probe, EndoFLIP(®) ) in the gastrointestinal tract: a systematic review, (in eng). Neurogastroenterol Motil. 2020;32(9):e13980. https://doi.org/10.1111/nmo.13980.
Carlson DA, Hirano I, Zalewski A, Gonsalves N, Lin Z, Pandolfino JE. Improvement in esophageal distensibility in response to medical and diet therapy in eosinophilic esophagitis, (in eng). Clin Transl Gastroenterol. 2017;8(10):e119. https://doi.org/10.1038/ctg.2017.47.
Carlson DA, Lin Z, Hirano I, Gonsalves N, Zalewski A, Pandolfino JE. Evaluation of esophageal distensibility in eosinophilic esophagitis: an update and comparison of functional lumen imaging probe analytic methods, (in eng). Neurogastroenterol Motil. 2016;28(12):1844–53. https://doi.org/10.1111/nmo.12888.
Nicodème F, et al. Esophageal distensibility as a measure of disease severity in patients with eosinophilic esophagitis, (in eng). Clin Gastroenterol Hepatol. 2013;11(9):1101-1107.e1. https://doi.org/10.1016/j.cgh.2013.03.020.
Hirano I, et al. Efficacy of dupilumab in a phase 2 randomized trial of adults with active eosinophilic esophagitis, (in eng). Gastroenterology. 2020;158(1):111-122.e10. https://doi.org/10.1053/j.gastro.2019.09.042.
Dellon ES, et al. A clinical severity index for eosinophilic esophagitis: development, consensus, and future directions, (in eng). Gastroenterology. 2022;163(1):59–76. https://doi.org/10.1053/j.gastro.2022.03.025.
Lin Z, et al. Functional luminal imaging probe topography: an improved method for characterizing esophageal distensibility in eosinophilic esophagitis, (in eng). Therap Adv Gastroenterol. 2013;6(2):97–107. https://doi.org/10.1177/1756283x12470017.
Taft TH, Guadagnoli L, Edlynn E. Anxiety and depression in eosinophilic esophagitis: a scoping review and recommendations for future research, (in eng). J Asthma Allergy. 2019;12:389–99. https://doi.org/10.2147/jaa.S193045.
Taft TH, et al. Esophageal hypervigilance and symptom-specific anxiety in patients with eosinophilic esophagitis, (in eng). Gastroenterology. 2021;161(4):1133–44. https://doi.org/10.1053/j.gastro.2021.06.023.
Collins MH, et al. Newly developed and validated eosinophilic esophagitis histology scoring system and evidence that it outperforms peak eosinophil count for disease diagnosis and monitoring, (in eng). Dis Esophagus. 2017;30(3):1–8. https://doi.org/10.1111/dote.12470.
Wechsler JB, Bolton SM, Amsden K, Wershil BK, Hirano I, Kagalwalla AF. Eosinophilic esophagitis reference score accurately identifies disease activity and treatment effects in children, (in eng). Clin Gastroenterol Hepatol. 2018;16(7):1056–63. https://doi.org/10.1016/j.cgh.2017.12.019.
Lucendo AJ, et al. Efficacy of budesonide orodispersible tablets as induction therapy for eosinophilic esophagitis in a randomized placebo-controlled trial, (in eng). Gastroenterology. 2019;157(1):74-86.e15. https://doi.org/10.1053/j.gastro.2019.03.025.
Dellon ES, Katzka DA, Collins MH, Hamdani M, Gupta SK, Hirano I. Budesonide oral suspension improves symptomatic, endoscopic, and histologic parameters compared with placebo in patients with eosinophilic esophagitis, (in eng). Gastroenterology. 2017;152(4):776-786.e5. https://doi.org/10.1053/j.gastro.2016.11.021.
Franciosi JP, et al. Development of a validated patient-reported symptom metric for pediatric eosinophilic esophagitis: qualitative methods, (in eng). BMC Gastroenterol. 2011;11:126. https://doi.org/10.1186/1471-230x-11-126.
Schoepfer AM, et al. Development and validation of a symptom-based activity index for adults with eosinophilic esophagitis, (in eng). Gastroenterology. 2014;147(6):1255-66.e21. https://doi.org/10.1053/j.gastro.2014.08.028.
• Ma C, et al. Development of a core outcome set for therapeutic studies in eosinophilic esophagitis (COREOS), (in eng). J Allergy Clin Immunol. 2022;149(2):659–70. https://doi.org/10.1016/j.jaci.2021.07.001. (Describes outcome measures for clinical trials and observation studies in the field of EoE.)
Ruffner MA, Cotton CC, Dellon ES. Posttreatment gene scores support histologic and endoscopic response thresholds in eosinophilic esophagitis, (in eng). Am J Gastroenterol. 2022;117(9):1519–22. https://doi.org/10.14309/ajg.0000000000001802.
Aceves SS, et al. Resolution of remodeling in eosinophilic esophagitis correlates with epithelial response to topical corticosteroids, (in eng). Allergy. 2010;65(1):109–16. https://doi.org/10.1111/j.1398-9995.2009.02142.x.
Chehade M, Sampson HA, Morotti RA, Magid MS. Esophageal subepithelial fibrosis in children with eosinophilic esophagitis, (in eng). J Pediatr Gastroenterol Nutr. 2007;45(3):319–28. https://doi.org/10.1097/MPG.0b013e31806ab384.
Navarro P, et al. Proton pump inhibitor therapy reverses endoscopic features of fibrosis in eosinophilic esophagitis, (in eng). Dig Liver Dis. 2021;53(11):1479–85. https://doi.org/10.1016/j.dld.2021.05.025.
•• Arnim UV, et al. Monitoring patients with eosinophilic esophagitis in routine clinical practice - international expert recommendations, (in eng). Clin Gastroenterol Hepatol. 2022. https://doi.org/10.1016/j.cgh.2022.12.018. (First effort for recommendations for follow-up of EoE patients.)
Haasnoot ML, Safi S, Bredenoord AJ. Poor adherence to medical and dietary treatments in adult patients with eosinophilic esophagitis, (in eng). Am J Gastroenterol. 2022;117(9):1412–8. https://doi.org/10.14309/ajg.0000000000001850.
Syed A, Maradey-Romero C, Fass R. The relationship between eosinophilic esophagitis and esophageal cancer, (in eng). Dis Esophagus. 2017;30(7):1–5. https://doi.org/10.1093/dote/dox050.
Funding
AB is supported by Vidi grant 91718300 from the Netherlands Organisation for Scientific Research NWO.
Author information
Authors and Affiliations
Contributions
AS, GMCM, AJB: conceptualization. AS, GMCM: writing of the original draft. AS, GMCM, AJB: critical revision of the manuscript and editing. All the authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Conflict of Interest
Andrea Sorge declares that she has no conflict of interest. Gwen M. C. Masclee declares that she has no conflict of interest. Albert J. Bredenoord received research funding from Nutricia, Norgine, Thelial, SST, and Dr. Falk Pharma and received speaker and/or consulting fees from Laborie, Thelial, EsoCap, Medtronic, Dr. Falk Pharma, Calypso Biotech, Alimentiv, Sanofi/Regeneron, Reckett, and AstraZeneca.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sorge, A., Masclee, G.M.C. & Bredenoord, A.J. Endoscopic Diagnosis and Response Evaluation in Patients with Eosinophilic Esophagitis. Curr Treat Options Gastro 21, 256–271 (2023). https://doi.org/10.1007/s11938-023-00428-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11938-023-00428-y