
Abstract
Purpose of Review
Advanced liver disease is a leading cause of non-AIDS-related morbidity and mortality in persons with HIV on antiretroviral therapy. As a result, persons with HIV are increasingly seeking liver transplantation.
Recent Findings
With the availability of direct-acting antiviral hepatitis C therapies, there has been a shift in the indications for liver transplantation in persons with HIV, with non-alcoholic fatty liver disease now the leading indication over hepatitis C infection. Additionally, liver transplant outcomes have improved in persons with HIV-hepatitis C co-infection persons with HIV. Preliminary results of HIV-to-HIV liver transplantation show acceptable results although rates of post-transplant infections and malignancies are areas of concern.
Summary
Future studies of liver transplantation in persons with HIV should focus on long-term outcomes, especially in the context of steatohepatitis and co-existing morbidities like diabetes, hyperlipidemia, and cardiovascular disease and other prevalent diseases in an aging population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the era of highly effective antiretroviral therapies (ART), mortality and opportunistic complications have declined dramatically in persons living with HIV (PWH), making HIV infection a chronic, manageable illness [1, 2]. With increased life expectancy and an aging demographic, liver disease, among other co-morbid medical conditions, has become a leading cause of morbidity and mortality in PWH [3, 4].
Before the availability of potent ART, HIV was an absolute contraindication for liver transplantation (LT) because of the inability to suppress HIV viremia, prevent opportunistic infections and progression to AIDS, and poor post-transplant survival [5,6,7,8]. With combination ART, the medical and surgical communities could reconsider organ transplantation as a life-saving therapy for PWH and advanced liver disease (ALD). Beginning with the results of observational studies across US and European transplant centers [9,10,11,12], accumulating evidence has demonstrated the feasibility of transplantation in this population and, ultimately, established LT as the standard of care for PWH with ALD. Further advances in HIV and hepatitis C therapies have improved the post-transplant management and outcomes of LT recipients with HIV and HIV/hepatitis C (HCV) co-infection.
This review focuses on the current landscape of LT for PWH, highlighting (1) the impact of direct-acting antiviral (DAA) HCV therapies on the epidemiology of liver disease in those seeking LT and post-transplant outcomes in HIV-HCV co-infected liver recipients, (2) improvements in post-transplant management of liver recipients with HIV with the availability of newer ART agents, and (3) expanding opportunities for PWH as organ donors and recipients with the use of HIV-positive livers for transplantation. The authors also provide a framework for the pre- and post-transplant management of LT recipients with HIV.
Indications for and Trends in Liver Transplantation in Persons with HIV
With increasing life expectancies resulting from highly effective ART, chronic liver disease has emerged as one of the most common causes of hospitalizations and the second leading cause of death in PWH, now accounting for 13% of deaths [4, 13]. There are multiple etiologies of liver disease in PWH, and numerous disease processes within a given patient may co-exist.
In persons with viral hepatitis, HIV infection accelerates the progression to liver fibrosis and cirrhosis [14, 15]. Until recently, advanced liver disease caused by chronic viral hepatitis C and B infections was the principal reason for seeking LT in PWH [16•]. Because of overlapping risk factors for acquisition, there is a disproportionate burden of hepatitis C and hepatitis B virus (HBV) infections in PWH. The estimated global prevalence of HCV is 2.4% in PWH; the populations with the highest prevalence of HIV-HCV co-infection are men who have sex with men (MSM), with reported rates of 20 to 30% and persons who inject drugs (PWID), with rates up to 95% [17,18,19,20]. The global prevalence of HIV-HBV co-infection is 6.1%, with the highest prevalence rates in sub-Saharan Africa and Southeast Asia and those with PWID, MSM, or multiple sex partners as a risk factor [15, 21]. Hemophilic patients are a unique population seeking LT with a high burden of HIV, HBV, and HCV, mainly due to the use of pooled donor plasma-derived factor concentrate before 1984 [22, 23].
Non-alcoholic fatty liver disease (NAFLD) is common in the general population and PWH and an increasingly frequent indication for LT. In the setting of HIV, the direct effects of the virus, metabolic abnormalities, adipose tissue dysfunction, mitochondrial toxicity from older ART agents, immune activation and dysregulation, and microbial translocation may contribute to the development of non-alcoholic steatohepatitis (NASH) [24•]. Accordingly, the reported prevalence of HIV-related non-alcoholic steatohepatitis ranges from 20 to 63%, with up to 63% having hepatic fibrosis [25,26,27,28,29].
Apart from their adverse metabolic effects and association with hepatic steatosis, ART contributes to the development of advanced liver disease through direct hepatotoxicity, hypersensitivity reactions, and immune reconstitution phenomena [30]. Mitochondrial toxicity is especially seen with the older nucleoside reverse transcriptase inhibitors, didanosine and stavudine [30], but is rare with newer agents. Mitochondrial toxicity remains relevant because its effects may persist in long-term survivors of HIV who seek LT. Additionally, some authors have reported nodular regenerative hyperplasia as a cause of non-cirrhotic, cryptogenic liver disease in PWH; a distinguishing feature of these cases was prolonged exposure to didanosine with or without hydroxyurea and stavudine [31, 32].
Immune-mediated phenomena are well-described causes of hepatoxicity in PWH. Rapid immune reconstitution, most notably when ART is initiated in the setting of chronic HBV infection, may result in significant liver injury. Also, hypersensitivity reactions, which can be severe, occur in the weeks following initiation of nevirapine, abacavir, and amprenavir [30].
The risk of liver injury from ART is highest in those with underlying liver disease chronic viral hepatitis [30, 33]. Also, alcohol use and other non-HIV-related causes of liver disease may occur as primary or exacerbating factors to the development of end-stage liver disease. Finally, hepatocellular carcinoma can further complicate the course of ALD, regardless of the underlying etiology of liver disease.
Contemporary ART agents pose less risk for liver injury. For example, abacavir hypersensitivity is now avoided by testing for the presence of the HLA-B*5701 allele before initiating therapy [34]. The newer non-nucleoside reverse transcriptase inhibitors, etravirine, rilpivirine, and doravirine, have much more favorable hepatoxicity profiles than nevirapine and efavirenz [35•]. Reports of liver injury related to the integrase strand inhibitors, raltegravir, dolutegravir, and elvitegravir are also uncommon [35•]. Protease inhibitors, however, require hepatic monitoring in persons with underlying liver disease. In a recent analysis performed by investigators of North America AIDS Cohort Collaboration on Research and Design (NA-ACCORD), boosted protease inhibitor regimens including atazanavir or darunavir were associated with the development of end-stage liver disease [36].
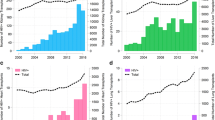
In an analysis of United Network for Organ Sharing and Organ Procurement and Transplantation Network (UNOS/OPTN) registry data from 2008 to 2018, investigators identified important trends in LT for PWH. Over this period, PWH accounted for 0.6% of LT in the USA. There were significant increases in the number of transplants performed over time, with 22 and 63 LT procedures performed in 2008 and 2018, respectively. The number of transplant centers performing LT in PWH also increased over the same period [16•].
The same study demonstrated a significant shift in the indications for LT in PWH over time. With the availability of DAA for HCV, the number of PWH seeking LT for HCV declined over the study period. From 2008 to 2017, HCV was the leading indication for LT in PWH, whereas NASH as the reason for LT increased significantly over time and became the leading indication in 2018 [16•]. International data has also confirmed this trend in HCV as the leading indication for LT [37].
Outcomes After Liver Transplantation
In the pre-HCV DAA era, the outcomes of PWH who underwent LT differed widely according to the indication for transplant. For example, there were early reports of successful results of LT in those with HIV-HBV co-infection, including persons with HBV viremia and lamivudine-resistant virus. In a single-center French report, investigators reported 100% cumulative graft and patient survival in 13 LT recipients with HIV-HBV co-infection after a mean follow-up of 32 months [38]. In a prospective multicenter US study, in the setting of passive prophylaxis with hepatitis B immunoglobulin and antiviral therapy, both graft and patient survivals were not significantly different in LT recipients with HIV-HBV co-infection and HBV mono-infection, with 1- and 3-year graft and patient survival of 85% and 100% (p = 0.09), respectively [9]. Lifelong prophylaxis is recommended due to the frequency of breakthrough HBV viremia [39].
Before DAA regimens for HCV infection, the transplant outcomes of persons with HIV-HCV co-infection were problematic, with significantly lower graft and patient survival rates than HCV-mono-infected controls [10,11,12, 40,41,42,43,44]. Estimates of 1-, 3-, and 5-year graft survival for persons with HIV-HCV co-infection ranged from 52 to 86%, 45 to 60%, and 31 to 45%, respectively, while HCV mono-infected controls ranged from 57 to 88%, 50 to 62%, and 33 to 58%, respectively. HCV-related progressive liver disease, severe infections, and sepsis contributed to poor outcomes. In the NIH-sponsored US multicenter observational study, predictors of graft loss in recipients with HIV-HCV co-infection included older donor age (HR 1.3), HCV antibody-positive donor (HR 2.5), body mass index less than 21 kg/m2, and combination liver and kidney transplants (HR 3.8). The authors suggested that these factors should be considered when selecting appropriate candidates and donors in persons with HIV-HCV co-infection [10].
In the recent US UNOS/OPTN registry data analysis, overall LT outcomes improved over time, and 1- and 3-year graft survival rates of PWH were similar to HIV-uninfected LT recipients, 85.5% and 73.0% vs. 89.7% and 81.9%, respectively. One- and 3-year patient survival rates were also similar, 87.9% and 77.5% vs. 91.9% and 84.6%, respectively, for LT with and without HIV. Over time and mirroring trends in HCV mono-infection population [45], LT outcomes are improving for persons with HIV-HCV co-infection over time. In the USA, from 2008 to 2018, the 1- and 3-year graft survival rates were 84.9% and 69.0% vs. 89.1% and 79.3% for LT recipients with HIV-HCV co-infection and HCV mono-infection, respectively. The 1- and 3-year patient survival in LT recipients with HIV-HCV co-infection vs. HCV mono-infection, 87.8% and 72.5% vs. 91.2% and 81.8%, respectively. However, in a sub-analysis of LT performed in persons with HCV after the availability of HCV DAA (2014–2018), the difference in 1- and 3-year patient survival between those with and without HIV was no longer significant, 91.1% and 84.2% vs. 93.0% and 86.4% [16•]. Other investigators in the USA have demonstrated that rates of graft failure after LT in persons with HIV-HCV co-infection are not significantly different than in persons without HIV and HCV infection [46]. A combined data analysis of European and US transplant registries showed similar results [37].
LT recipients with HIV and non-viral indications appear to have excellent post-transplant outcomes. Persons with HIV have similar results to those with HIV when undergoing LT for NASH [16•]. Also, persons with HIV and hepatocellular carcinoma, regardless of the presence of viral hepatitis as an additional indication for LT, have similar post-transplant outcomes in terms of HCC recurrence and patient survival [47, 48].
HIV-to-HIV Transplantation
The passage and implementation of the HIV Organ Policy Equity (HOPE) Act put safeguards in place to conduct and monitor outcomes in HIV-to-HIV transplantation in a research setting using well-defined donor eligibility requirements at transplant centers with experience in HIV and transplantation [49]. While expanding the potential pool of donor organs for PWH, the HOPE Act also represents an opportunity to eliminate stigma by legalizing organ donation from donors with HIV to PWH.
Transplantation utilizing liver allografts infected with HIV poses theoretical risks such as the transmission of antiretroviral-resistant or CXCR4-tropic virus and latent or unrecognized opportunistic pathogens and malignancies. Poor organ quality is another concern because of the high prevalence of liver disease in PWH [50, 51]. For this reason, the HOPE Act requires pre-implantation donor organ biopsies. While there are no restrictions regarding donor CD4 T cell count or HIV viremia, transplant clinicians must exercise caution when accepting organs from donors with active viremia and low CD4 T cell count, especially donors with a pre-donation diagnosis of HIV or prior ART. Donors with these features are more likely to have pre-existing ART antiretroviral resistance or opportunistic infections. The risks to the recipient may be minimized by scrutinizing details of donor HIV treatment and medical history. Donor HIV resistance genotyping is essential for early post-transplant ART modifications if resistance is identified. Finally, donors with active opportunistic infections are not eligible for transplantation under the HOPE Act.
As of September 2020, 24 US transplant centers have conducted 223 HIV-to-HIV transplants under the HOPE Act, including 170 kidney and 53 liver transplants [52]. Results of kidney transplantation, both early results in the US and longer-term results in South Africa, are favorable [53,54,55]. Experience with LT is growing, and US investigators conducting a multicenter pilot study recently reported the outcomes of 24 HIV-to-HIV LT recipients (HIV D + /R +) compared to 21 liver recipients with HIV who received HIV-negative organs (HIV D − /R +) after a median follow-up of 23 months [56•]. The most frequent indication for transplant was HCV infection in 56%, and the median duration of HIV infection in recipients was 23 years. Post-transplant, only one HIV D + /R + recipient required a modification of ART due to clinically suspected HIV resistance in the donor. Allograft rejection rates were similar in the HIV D + /R + and HIV D − /R + recipients. HIV D + /R + recipients also had a higher incidence of hospitalizations for infections, albeit not traditional AIDS-related conditions. The 1-year survival was 83.3% vs. 100% in HIV D + /R + v HIV D − /R + recipients, respectively, and the causes of death in the HIV D + /R + group included an early post-transplant cardiac arrest, graft ischemia and sepsis, pulmonary hypertension and sepsis, parotid gland carcinoma, and allograft rejection attributed to medication non-adherence. The remaining death was attributed to donor-derived HHV8-associated lymphoma and visceral Kaposi sarcoma (KS), and two additional HIV D + /R + recipients with HHV8-seropositive donors developed post-transplant KS. An NIH-sponsored multicenter trial of HIV-to-HIV LT (Clinical Trial Identifier: NCT03734393) is currently enrolling and expected to provide clarity on infection and cancer risks in HIV D + /R + liver recipients.
While cases of transient HIV superinfection have occurred after both HIV-to-HIV kidney and LT, no instances of sustained or multi-drug resistant HIV superinfection have been reported [55, 57, 58]. Additionally, in a subset of the US multicenter study participants, none of the 17 HIV D + /R + kidney and liver recipients tested had evidence of HIV superinfection by next-generation sequencing of pol and gp41 using proviral DNA and viral RNA from serial donor and recipient samples and analysis of direct sequences and neighbor-joining phylogenetic trees [59].
Clinical Management Issues in Liver Transplant Candidates and Recipients with HIV
Eligibility Criteria for Liver Transplantation in Persons with HIV
Patients with HIV and ALD require specialized care at medical centers with expertise in managing end-stage and decompensated liver disease and LT. Centers may vary in the candidacy requirements for transplantation. Clinical trial experience and recent guidelines suggest that optimal candidates for LT are patients with suppression of HIV viremia on therapy, CD4 T cell count ≥ 100 cells per μL, no active opportunistic infection or malignancy, and have the ability to have close follow-up for management of immunosuppressive therapy. Candidates must have demonstrated adherence to ART, a notable exception being persons with decompensated liver disease who cannot tolerate ART. In this situation, the HIV provider must predict viral suppression with an ART regimen post-transplant [39, 60]. These criteria also meet eligibility for HIV-to-HIV transplantation under the HOPE Act [49, 56•].
For candidates with HIV-HCV co-infection, specialists can weigh the risks and benefits of HCV DAA treatment before transplantation. If treatment can be safely delayed, the option of utilizing HCV organs followed by post-transplant treatment increases the pool of available organs for transplant. Whether administered before or after transplant, excellent HCV treatment outcomes have been achieved with DAA therapy [61,62,63]. When evaluating HCV-coinfected persons for LT, it is important to weigh factors predictive of liver allograft and patient survival [10].
Vaccinations
Persons living with HIV, regardless of transplant status, require vaccinations against tetanus, COVID-19, annual influenza, hepatitis A, hepatitis B, Meningococcus serogroup A, C, W, Y, and pneumococcal vaccines [64]. Before transplant, candidates should have screening serologies for vaccine-preventable infections, including hepatitis A antibody, hepatitis B surface antibody (HBsAb), hepatitis B surface antigen (HBsAg), hepatitis B core antibody (HBcAb), and measles, mumps, and rubella (MMR) antibodies. These results can guide the immunization plan. Patients with a CD4 T cell count > 200 cells per μL are candidates for MMR vaccination if unvaccinated or non-immune; MMR, attenuated live virus vaccine, is contraindicated in advanced HIV infection [65, 66]. For PWH with no evidence of hepatitis B immunity or exposure, a high-dose three-vaccine hepatitis B series should be given [67]. Patients who are HBcAb-positive, but HBsAb- and HBsAg-negative, should receive a single standard dose of hepatitis B vaccine with repeat HBsAb testing [68]. If HBsAb is negative on repeat testing, the high-dose three-vaccine HBV series should be administered. We also recommend that patients who need transplants emergently to not receive any live vaccines, as there is a risk for disease in the setting of profound immunosuppression with less risk incurred in less severely immunosuppressed persons [69, 70]. Meningitis B and Haemophilus influenzae B vaccines should be administered if a splenectomy or splenic embolization is planned.
The recombinant zoster vaccine can be considered before transplant, especially in those ≥ 50 years of age; additionally, this vaccine is FDA approved for persons ≥ 18 years of age who will be at increased risk of herpes zoster due to planned or current immunosuppressive therapy [64], and there is data to support its use in varicella-seronegative transplant recipients [71]. Finally, vaccination against human papillomavirus (HPV) is currently recommended for PWH until age 26 years, after which age-shared decision-making should be done regarding this vaccine series. We recommend HPV vaccination for all those who intend to undergo LT, primarily due to its implications in HPV-related cancers [72].
MSM Health
Transplant centers that perform LT in PWH must engage in culturally competent care for MSM and provide transplant care within the context of the specialized healthcare needs of this population. MSM is a broad term that encompasses transgender men, cisgender men, and individuals who are assigned male at birth. MSM includes any member of the group above having sex with another member of this group, regardless of the individual’s self-identified sexual orientation. Persons who report male-to-male sexual contact are disproportionately affected by HIV and accounted for nearly 70% of new HIV infections in the USA from 2015 to 2019 [73]. And so, many PWH seeking LT report this risk factor for HIV acquisition.
The MSM population has had a notable increase in sexually transmitted infection (STI) rates over previous years and benefits from regular STI testing [74]. Thus, as part of the pre-transplant evaluation process, we recommend a thorough sexual history—including gender identity and gender identity of sexual partners and types of sexual intercourse in which the candidate engages. STI screening should be performed based on this information, with continued re-evaluations throughout the post-transplant period as indicated.
Similarly, rates of substance use in MSM and other sexual minority groups are higher than in men who do not identify as gay or bisexual [75]. Substance use should be assessed before and after transplant as drug use can portend poorer outcomes after LT and lead to poor ART adherence and STI acquisition [76,77,78,79].
Finally, we recommend that an anal pap smear be performed in men who report anal receptive intercourse or history of anal warts during the pre-transplant evaluation and intermittently post-transplant [80]. These pap smears should be performed with reflex to genotyping [81]. Abnormal pap smears should result in referral to a colorectal surgeon or a specialist in high-resolution anoscopy [82]. Prospective longitudinal studies related to anal cancer screening post-transplant are still in need; however, transplant patients are at higher risk, and the additive roles of immunosuppression and HIV on the development of HPV-related cancers deserve further study [83].
Pharmacologic Considerations with ART and Immunosuppression
Due to the importance of antirejection medications, therapeutic drug monitoring is required; drug-to-drug interactions between antirejection medications and ART may require adjustment of immunosuppression or the ART regimen. These interactions have been discussed in other works; however, a few key drugs and interactions will be discussed here [39, 84, 85]. Transplant providers should be mindful of these interactions and issues, as treatment experienced by PWH may have limitations in ART for viral suppression. Liver toxicity associated with these agents is outlined in Table 1.
Regimens containing integrase strand transfer inhibitors (INSTI) are the favored therapies for both transplant and non-transplant PWH [39, 86]. Bictegravir, dolutegravir, and raltegravir are metabolized through the liver’s uridine diphosphate glucuronosyltransferase 1A system [87]. As a result, there are clinically insignificant interactions with the calcineurin inhibitors. Small case reports evaluating the use of raltegravir have found that it is generally well tolerated and effective to use in the setting of LT with minimal side effects [88,89,90]. Due to its high barrier to resistance and its once-a-day dosing, dolutegravir is the favored INSTI [84, 91].
Whereas pre-transplant regimens containing INSTI are generally maintained post-transplant, pre-transplant regimens containing protease inhibitors (PI) should be altered if possible. PI inhibit cytochrome P450 3A4 (CYP3A4) enzyme, which in turn alter the pharmacokinetics of immunosuppressants such as calcineurin inhibitors and mTOR inhibitors. Complicating matters, ritonavir, a PI, may be used as a pharmacologic enhancer to increase ART levels in treatment experienced individuals. However, the use of ritonavir-boosted regimens in LT recipients has been associated with episodes of acute renal failure from high cyclosporine or tacrolimus levels [92, 93]. We favor avoidance of boosted regimens when possible. When not possible, cobicistat is the booster of choice—it is strictly a CYP3A inhibitor without other enzymatic collateral seen with ritonavir [94]. Regardless, PWH on boosted regimens need immunosuppression levels monitored exceptionally closely. Post-transplantation, in the event a PWH is transitioned off a boosted regimen, it should be done in coordination with the transplant center. Failure to do so may result in rejection from underdosing of immunosuppressive agents [95].
Clinical Monitoring and Care of Persons with HIV Before and After Organ Transplantation
HIV providers are vital members of the transplant team, readying patients for transplant, optimizing and managing HIV therapies, and monitoring HIV infection and for potential opportunistic complications in the post-transplant period. Table 2 outlines the recommended frequency of lab monitoring in PWH after organ transplantation, incorporating HIV guidelines and the authors’ interpretation of the guidance for organ recipients with HIV [86]. Frequent monitoring of CD4 T cell counts and HIV viral load is warranted early in the post-transplant period, in the setting of allograft rejection, and when immunosuppressive therapy is modified or intensified. Additionally, aging PWH are at risk for multiple non-AIDS comorbidities [96], and regular monitoring for and treatment of diabetes mellitus, hyperlipidemia, cardiovascular disease, and malignancy is required.
When optimizing ART before transplant, every effort should be made to obtain the results of prior HIV resistance testing. If previous resistance testing results are unavailable and the patient is virally suppressed, especially if a patient is listed for HOPE organs, the authors recommend resistance genotyping using HIV proviral DNA to guide ART modifications [97]. Post-transplant, whenever feasible, clinicians should avoid protease inhibitor- and cobicistat-based ART regimens that result in supratherapeutic calcineurin inhibitor levels [98]. Often the same ART regimen may be continued. However, clinicians must be cognizant of frequent fluctuations in kidney function that may require regular ART dose adjustments, especially early in the post-transplant period. In addition, HIV clinicians should avoid, when possible, or closely monitor patients after starting agents that may compromise liver function (Table 1) [30, 35•, 86, 99]. Because of complex drug interactions, HIV providers must communicate with the transplant center whenever a change in ART is contemplated.
Conclusion
With advances in HIV and HCV therapies, PWH have improved outcomes after LT but require multidisciplinary care to optimize post-transplant health. Still, persons with HIV and ALD have are less likely to receive LT and have higher waitlist mortality than persons without HIV [100, 101]. Even with growing transplant center experience, PWH face barriers to LT, with HIV considered an absolute (28.1%) or relative contraindication (31.6%) of surveyed US transplant centers [102]. To improve the management and outcomes of ALD in this population, it is important to clarify the barriers to transplantation further and disseminate emerging data demonstrating improved outcomes after LT. Future studies should focus on long-term outcomes, especially in the context of NASH and co-existing morbidities like diabetes, hyperlipidemia, and cardiovascular disease and other prevalent diseases in aging PWH. HIV-to-HIV transplantation offers increased access to organ transplantation and donation, but while preliminary results are encouraging, short- and long-term results are needed before broader implementation of the HOPE Act for LT.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Palella FJ Jr, Baker RK, Moorman AC, Chmiel JS, Wood KC, Brooks JT, et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43(1):27–34. https://doi.org/10.1097/01.qai.0000233310.90484.16.
Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338(13):853–60. https://doi.org/10.1056/NEJM199803263381301.
Weber R, Ruppik M, Rickenbach M, Spoerri A, Furrer H, Battegay M, et al. Decreasing mortality and changing patterns of causes of death in the Swiss HIV Cohort Study. HIV Med. 2013;14(4):195–207. https://doi.org/10.1111/j.1468-1293.2012.01051.x.
Smith CJ, Ryom L, Weber R, Morlat P, Pradier C, Reiss P, et al. Trends in underlying causes of death in people with HIV from 1999 to 2011 (D:A:D): a multicohort collaboration. Lancet. 2014;384(9939):241–8. https://doi.org/10.1016/S0140-6736(14)60604-8.
Tzakis AG, Cooper MH, Dummer JS, Ragni M, Ward JW, Starzl TE. Transplantation in HIV+ patients. Transplantation. 1990;49(2):354–8.
Dummer JS, Erb S, Breinig MK, Ho M, Rinaldo CR, Jr., Gupta P, et al. Infection with human immunodeficiency virus in the Pittsburgh transplant population. A study of 583 donors and 1043 recipients, 1981–1986. Transplantation. 1989;47(1):134–40. https://doi.org/10.1097/00007890-198901000-00030.
Erice A, Rhame FS, Heussner RC, Dunn DL, Balfour HH Jr. Human immunodeficiency virus infection in patients with solid-organ transplants: report of five cases and review. Rev Infect Dis. 1991;13(4):537–47. https://doi.org/10.1093/clinids/13.4.537.
Bouscarat F, Samuel D, Simon F, Debat P, Bismuth H, Saimot AG. An observational study of 11 French liver transplant recipients infected with human immunodeficiency virus type 1. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1994;19(5):854–9. https://doi.org/10.1093/clinids/19.5.854.
Coffin CS, Stock PG, Dove LM, Berg CL, Nissen NN, Curry MP, et al. Virologic and clinical outcomes of hepatitis B virus infection in HIV-HBV coinfected transplant recipients. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2010;10(5):1268–75. https://doi.org/10.1111/j.1600-6143.2010.03070.x.
Terrault NA, Roland ME, Schiano T, Dove L, Wong MT, Poordad F, et al. Outcomes of liver transplant recipients with hepatitis C and human immunodeficiency virus coinfection. Liver transplantation : official publication of the American Association for the Study of Liver Diseases and the International Liver Transplantation Society. 2012;18(6):716–26. https://doi.org/10.1002/lt.23411.
Di Benedetto F, Tarantino G, De Ruvo N, Cautero N, Montalti R, Guerrini GP, et al. University of Modena experience in HIV-positive patients undergoing liver transplantation. Transpl Proc. 2011;43(4):1114–8. https://doi.org/10.1016/j.transproceed.2011.03.017.
Anadol E, Beckebaum S, Radecke K, Paul A, Zoufaly A, Bickel M, et al. Orthotopic liver transplantation in human-immunodeficiency-virus-positive patients in Germany. AIDS research and treatment. 2012;2012: 197501. https://doi.org/10.1155/2012/197501.
Ramos-Rincon JM, Menchi-Elanzi M, Pinargote-Celorio H, Mayoral A, Gonzalez-Alcaide G, de Mendoza C, et al. Trends in hospitalizations and deaths in HIV-infected patients in Spain over two decades. AIDS. 2022;36(2):249–56. https://doi.org/10.1097/QAD.0000000000003105.
Soriano V, Vispo E, Fernandez-Montero JV, Labarga P, Barreiro P. Update on HIV/HCV coinfection. Curr HIV/AIDS Rep. 2013;10(3):226–34. https://doi.org/10.1007/s11904-013-0169-5.
Soriano V, Poveda E, Vispo E, Barreiro P. Hepatitis B in HIV-infected patients. Clin Liver Dis. 2013;17(3):489–501. https://doi.org/10.1016/j.cld.2013.05.008.
• Campos-Varela I, Dodge JL, Terrault NA, Brandman D, Price JC. Nonviral liver disease is the leading indication for liver transplant in the United States in persons living with human immunodeficiency virus. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2021;21(9):3148-56. https://doi.org/10.1111/ajt.16569. U.S UNOS/registry data demonstrating improving liver transplant outcomes in liver translant recipients with HIV-HCV co-infection in the DAA era.
Platt L, Easterbrook P, Gower E, McDonald B, Sabin K, McGowan C, et al. Prevalence and burden of HCV co-infection in people living with HIV: a global systematic review and meta-analysis. Lancet Infect Dis. 2016;16(7):797–808. https://doi.org/10.1016/S1473-3099(15)00485-5.
Witt MD, Seaberg EC, Darilay A, Young S, Badri S, Rinaldo CR, et al. Incident hepatitis C virus infection in men who have sex with men: a prospective cohort analysis, 1984–2011. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2013;57(1):77–84. https://doi.org/10.1093/cid/cit197.
Irvin R, Gamble T, Malone J, Wang Z, Wilson E, Hughes JP, et al. HIV Prevention Trials Network 078: high prevalence of hepatitis C virus antibodies among urban US men who have sex with men, independent of human immunodeficiency virus status. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2021;73(7):e2205–10. https://doi.org/10.1093/cid/ciaa1869.
Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol. 2006;44(1 Suppl):S6-9. https://doi.org/10.1016/j.jhep.2005.11.004.
Platt L, French CE, McGowan CR, Sabin K, Gower E, Trickey A, et al. Prevalence and burden of HBV co-infection among people living with HIV: a global systematic review and meta-analysis. J Viral Hepatitis. 2020;27(3):294–315. https://doi.org/10.1111/jvh.13217.
Isfordink CJ, van Erpecum KJ, van der Valk M, Mauser-Bunschoten EP, Makris M. Viral hepatitis in haemophilia: historical perspective and current management. Br J Haematol. 2021;195(2):174–85. https://doi.org/10.1111/bjh.17438.
Ragni MV, Devera ME, Roland ME, Wong M, Stosor V, Sherman KE, et al. Liver transplant outcomes in HIV+ haemophilic men. Haemophilia : the official journal of the World Federation of Hemophilia. 2013;19(1):134–40. https://doi.org/10.1111/j.1365-2516.2012.02905.x.
• Lake JE, Overton T, Naggie S, Sulkowski M, Loomba R, Kleiner DE, et al. Expert panel review on nonalcoholic fatty liver disease in persons with human immunodeficiency virus. Clin Gastroenterol Hepatol. 2020. https://doi.org/10.1016/j.cgh.2020.10.018. An excellent review of the epidemiology and pathogenesis of HIV-related nonalcoholic liver disease.
Morse CG, McLaughlin M, Matthews L, Proschan M, Thomas F, Gharib AM, et al. Nonalcoholic steatohepatitis and hepatic fibrosis in HIV-1-monoinfected adults with elevated aminotransferase levels on antiretroviral therapy. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2015;60(10):1569–78. https://doi.org/10.1093/cid/civ101.
Vodkin I, Valasek MA, Bettencourt R, Cachay E, Loomba R. Clinical, biochemical and histological differences between HIV-associated NAFLD and primary NAFLD: a case-control study. Aliment Pharmacol Ther. 2015;41(4):368–78. https://doi.org/10.1111/apt.13052.
Pembroke T, Deschenes M, Lebouche B, Benmassaoud A, Sewitch M, Ghali P, et al. Hepatic steatosis progresses faster in HIV mono-infected than HIV/HCV co-infected patients and is associated with liver fibrosis. J Hepatol. 2017;67(4):801–8. https://doi.org/10.1016/j.jhep.2017.05.011.
Sterling RK, Smith PG, Brunt EM. Hepatic steatosis in human immunodeficiency virus: a prospective study in patients without viral hepatitis, diabetes, or alcohol abuse. J Clin Gastroenterol. 2013;47(2):182–7. https://doi.org/10.1097/MCG.0b013e318264181d.
Ingiliz P, Valantin MA, Duvivier C, Medja F, Dominguez S, Charlotte F, et al. Liver damage underlying unexplained transaminase elevation in human immunodeficiency virus-1 mono-infected patients on antiretroviral therapy. Hepatology. 2009;49(2):436–42. https://doi.org/10.1002/hep.22665.
Soriano V, Puoti M, Garcia-Gasco P, Rockstroh JK, Benhamou Y, Barreiro P, et al. Antiretroviral drugs and liver injury. AIDS. 2008;22(1):1–13. https://doi.org/10.1097/QAD.0b013e3282f0e2fd.
Dinh MH, Stosor V, Rao SM, Miller FH, Green RM. Cryptogenic liver disease in HIV-seropositive men. HIV Med. 2009;10(7):447–53. https://doi.org/10.1111/j.1468-1293.2009.00712.x.
Maida I, Nunez M, Rios MJ, Martin-Carbonero L, Sotgiu G, Toro C, et al. Severe liver disease associated with prolonged exposure to antiretroviral drugs. J Acquir Immune Defic Syndr. 2006;42(2):177–82. https://doi.org/10.1097/01.qai.0000221683.44940.62.
Reisler RB, Han C, Burman WJ, Tedaldi EM, Neaton JD. Grade 4 events are as important as AIDS events in the era of HAART. J Acquir Immune Defic Syndr. 2003;34(4):379–86. https://doi.org/10.1097/00126334-200312010-00004.
Ma JD, Lee KC, Kuo GM. HLA-B*5701 testing to predict abacavir hypersensitivity. PLoS Curr. 2010;2:RRN1203. https://doi.org/10.1371/currents.RRN1203.
• Rivera CG, Otto AO, Zeuli JD, Temesgen Z. Hepatotoxicity of contemporary antiretroviral drugs. Curr Opin HIV AIDS. 2021;16(6):279–85. https://doi.org/10.1097/COH.0000000000000706. An overview of newer antiretoviral agents and their potential to cause hepatoxicity.
Young J, Lo Re V 3rd, Kim HN, Sterling TR, Althoff KN, Gebo KA, et al. Do contemporary antiretrovirals increase the risk of end-stage liver disease? Signals from patients starting therapy in the North American AIDS Cohort Collaboration on Research and Design. Pharmacoepidemiol Drug Saf. 2021. https://doi.org/10.1002/pds.5379.
Campos-Varela I, Dodge JL, Berenguer M, Adam R, Samuel D, Di Benedetto F, et al. Temporal trends and outcomes in liver transplantation for recipients with HIV infection in Europe and United States. Transplantation. 2020;104(10):2078–86. https://doi.org/10.1097/TP.0000000000003107.
Tateo M, Roque-Afonso AM, Antonini TM, Medja F, Lombes A, Jardel C, et al. Long-term follow-up of liver transplanted HIV/hepatitis B virus coinfected patients: perfect control of hepatitis B virus replication and absence of mitochondrial toxicity. AIDS. 2009;23(9):1069–76. https://doi.org/10.1097/QAD.0b013e32832c2a37.
Blumberg EA, Rogers CC, Practice ASTIDCo. Human immunodeficiency virus in solid organ transplantation. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2013;13 Suppl 4:169–78. https://doi.org/10.1111/ajt.12109.
Moreno A, Cervera C, Fortun J, Blanes M, Montejo E, Abradelo M, et al. Epidemiology and outcome of infections in human immunodeficiency virus/hepatitis C virus-coinfected liver transplant recipients: a FIPSE/GESIDA prospective cohort study. Liver transplantation : official publication of the American Association for the Study of Liver Diseases and the International Liver Transplantation Society. 2012;18(1):70–81. https://doi.org/10.1002/lt.22431.
Miro JM, Montejo M, Castells L, Rafecas A, Moreno S, Aguero F, et al. Outcome of HCV/HIV-coinfected liver transplant recipients: a prospective and multicenter cohort study. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2012;12(7):1866–76. https://doi.org/10.1111/j.1600-6143.2012.04028.x.
Sawinski D, Goldberg DS, Blumberg E, Abt PL, Bloom RD, Forde KA. Beyond the NIH multicenter HIV transplant trial experience: outcomes of HIV+ liver transplant recipients compared to HCV+ or HIV+/HCV+ coinfected recipients in the United States. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2015;61(7):1054–62. https://doi.org/10.1093/cid/civ471.
de Vera ME, Dvorchik I, Tom K, Eghtesad B, Thai N, Shakil O, et al. Survival of liver transplant patients coinfected with HIV and HCV is adversely impacted by recurrent hepatitis C. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2006;6(12):2983–93. https://doi.org/10.1111/j.1600-6143.2006.01546.x.
Duclos-Vallee JC, Feray C, Sebagh M, Teicher E, Roque-Afonso AM, Roche B, et al. Survival and recurrence of hepatitis C after liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology. 2008;47(2):407–17. https://doi.org/10.1002/hep.21990.
Young K, Liu B, Bhuket T, Wong RJ. Lower likelihood of post-transplant graft failure, death, and retransplantation in the era of direct-acting antivirals. J Clin Exp Hepatol. 2020;10(6):581–9. https://doi.org/10.1016/j.jceh.2020.02.003.
Cotter TG, Wang J, Lieber SR, Odenwald MA, Rich NE, Marrero JA, et al. “Raising HOPE”: improved outcomes for HIV/HCV-coinfected liver transplant recipients in the direct-acting antiviral era. Transplant Direct. 2021;7(7): e707. https://doi.org/10.1097/TXD.0000000000001154.
Aguero F, Forner A, Manzardo C, Valdivieso A, Blanes M, Barcena R, et al. Human immunodeficiency virus infection does not worsen prognosis of liver transplantation for hepatocellular carcinoma. Hepatology. 2016;63(2):488–98. https://doi.org/10.1002/hep.28321.
Guerrini GP, Berretta M, Guaraldi G, Magistri P, Esposito G, Ballarin R, et al. Liver Transplantation for HCC in HIV-infected patients: long-term single-center experience. Cancers (Basel). 2021;13(18). https://doi.org/10.3390/cancers13184727.
Health R, Services Administration DoH, Human S. Organ procurement and transplantation: implementation of the HIV Organ Policy Equity Act. Final rule. Fed Regist. 2015;80(89):26464–7.
Boyarsky BJ, Durand CM, Palella FJ Jr, Segev DL. Challenges and clinical decision-making in HIV-to-HIV transplantation: insights from the HIV literature. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2015;15(8):2023–30. https://doi.org/10.1111/ajt.13344.
Haidar G, Singh N. The Times, They are a-changing: HOPE for HIV-to-HIV organ transplantation. Transplantation. 2017;101(9):1987–95. https://doi.org/10.1097/TP.0000000000001728.
UNOS: Hope Act impact continues at five-year milestone. https://unos.org/news/in-focus/hope-act-impact-continues-at-five-year-milestone/. Accessed 28 Dec 2021.
Durand CM, Zhang W, Brown DM, Yu S, Desai N, Redd AD, et al. A prospective multicenter pilot study of HIV-positive deceased donor to HIV-positive recipient kidney transplantation: HOPE in action. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2021;21(5):1754–64. https://doi.org/10.1111/ajt.16205.
Muller E, Kahn D, Mendelson M. Renal transplantation between HIV-positive donors and recipients. N Engl J Med. 2010;362(24):2336–7. https://doi.org/10.1056/NEJMc0900837.
Selhorst P, Combrinck CE, Manning K, Botha FCJ, Labuschagne JPL, Anthony C, et al. Longer- term outcomes of HIV-positive-to-HIV-positive renal transplantation. N Engl J Med. 2019;381(14):1387–9. https://doi.org/10.1056/NEJMc1903013.
• Durand CM, Florman S, Motter JD, Brown D, Ostrander D, Yu S, et al. HOPE in action: A prospective multicenter pilot study of liver transplantation from donors with HIV to recipients with HIV. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2021. https://doi.org/10.1111/ajt.16886. The authors present the results of a US pilot study of HIV-to-HIV liver transplantation.
Blasi M, Stadtler H, Chang J, Hemmersbach-Miller M, Wyatt C, Klotman P, et al. Detection of donor’s HIV strain in HIV-positive kidney-transplant recipient. N Engl J Med. 2020;382(2):195–7. https://doi.org/10.1056/NEJMc1910189.
Hathorn E, Smit E, Elsharkawy AM, Bramhall SR, Bufton SA, Allan S, et al. HIV-positive-to-HIV-positive liver transplantation. N Engl J Med. 2016;375(18):1807–9. https://doi.org/10.1056/NEJMc1603850.
Bonny TS, Kirby C, Martens C, Rose R, Desai N, Seisa M, et al. Outcomes of donor-derived superinfection screening in HIV-positive to HIV-positive kidney and liver transplantation: a multicentre, prospective, observational study. Lancet HIV. 2020;7(9):e611–9. https://doi.org/10.1016/S2352-3018(20)30200-9.
Roland ME, Barin B, Carlson L, Frassetto LA, Terrault NA, Hirose R, et al. HIV-infected liver and kidney transplant recipients: 1- and 3-year outcomes. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2008;8(2):355–65. https://doi.org/10.1111/j.1600-6143.2007.02061.x.
Grant JL, Hawkins C, Brooks H, Palella FJ Jr, Koppe SW, Abecassis MM, et al. Successful sofosbuvir-based therapy in HIV/hepatitis C virus coinfected liver transplant recipients with recurrent hepatitis C virus infection. AIDS. 2016;30(1):93–8. https://doi.org/10.1097/QAD.0000000000000887.
Manzardo C, Londono MC, Castells L, Testillano M, Luis Montero J, Penafiel J, et al. Direct-acting antivirals are effective and safe in HCV/HIV-coinfected liver transplant recipients who experience recurrence of hepatitis C: a prospective nationwide cohort study. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2018;18(10):2513–22. https://doi.org/10.1111/ajt.14996.
Peters MG, Kottilil S, Terrault N, Amara D, Husson J, Huprikar S, et al. Retrospective-prospective study of safety and efficacy of sofosbuvir-based direct-acting antivirals in HIV/HCV-coinfected participants with decompensated liver disease pre- or post-liver transplant. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2021;21(5):1780–8. https://doi.org/10.1111/ajt.16427.
Centers for Disease Control and Prevention. Table 2. Recommended adult immunization schedule by medical condition and other indications, United States, 2021. https://www.cdc.gov/vaccines/schedules/hcp/imz/adult-conditions.html. Accessed 31 Dec 2021.
Danziger-Isakov L, Kumar D, Practice AICo. Vaccination of solid organ transplant candidates and recipients: guidelines from the American society of transplantation infectious diseases community of practice. Clinical transplantation. 2019;33(9):e13563. https://doi.org/10.1111/ctr.13563.
Centers for Disease Control and Prevention. HIV Infection and Adult Vaccination.: https://www.cdc.gov/vaccines/adults/rec-vac/health-conditions/hiv.html. Accessed 2 Jan 2022.
Vargas JI, Jensen D, Martinez F, Sarmiento V, Peirano F, Acuna P, et al. Comparative efficacy of a high-dose vs standard-dose hepatitis B revaccination schedule among patients with HIV: a randomized clinical trial. JAMA Netw Open. 2021;4(8): e2120929. https://doi.org/10.1001/jamanetworkopen.2021.20929.
Piroth L, Launay O, Michel ML, Bourredjem A, Miailhes P, Ajana F, et al. Vaccination against hepatitis B virus (HBV) in HIV-1-infected patients with isolated anti-HBV core antibody: the ANRS HB EP03 CISOVAC Prospective Study. J Infect Dis. 2016;213(11):1735–42. https://doi.org/10.1093/infdis/jiw011.
Chang SY, Bisht A, Faysman K, Schiller GJ, Uslan DZ, Multani A. Vaccine-associated measles in a hematopoietic cell transplant recipient: case report and comprehensive review of the literature. Open Forum Infect Dis. 2021;8(8):ofab326. https://doi.org/10.1093/ofid/ofab326.
Desjardins M, Mitre X, Sherman AC, Walsh SR, Cheng MP, Kanjilal S, et al. Safety of live-attenuated measles, mumps, and rubella vaccine administered within 2 years of hematopoietic cell transplant. Open Forum Infect Dis. 2021;8(12):ofab504. https://doi.org/10.1093/ofid/ofab504.
L’Huillier AG, Hirzel C, Ferreira VH, Ierullo M, Ku T, Selzner N, et al. Evaluation of recombinant herpes zoster vaccine for primary immunization of varicella-seronegative transplant recipients. Transplantation. 2021;105(10):2316–23. https://doi.org/10.1097/TP.0000000000003621.
Gillison ML, Chaturvedi AK, Lowy DR. HPV prophylactic vaccines and the potential prevention of noncervical cancers in both men and women. Cancer. 2008;113(10 Suppl):3036–46. https://doi.org/10.1002/cncr.23764.
HIV Basics. Overview: data and trends: U.S. Statistics. 2021. https://www.hiv.gov/hiv-basics/overview/data-and-trends/statistics. Accessed 1 Jan 2022.
Khosropour CM, Dombrowski JC, Barbee LA, Kerani RP, Berzkalns A, Golden MR (2021) Changing patterns of sexual behavior and HIV/STI among men who have sex with men in Seattle, 2002 to 2018. Journal of acquired immune deficiency syndromes. https://doi.org/10.1097/QAI.0000000000002686.
Compton WM, Jones CM. Substance use among men who have sex with men. N Engl J Med. 2021;385(4):352–6. https://doi.org/10.1056/NEJMra2033007.
Hunter LJ, Dargan PI, Benzie A, White JA, Wood DM. Recreational drug use in men who have sex with men (MSM) attending UK sexual health services is significantly higher than in non-MSM. Postgrad Med J. 2014;90(1061):133–8. https://doi.org/10.1136/postgradmedj-2012-131428.
DiMartini A, Crone C, Dew MA. Alcohol and substance use in liver transplant patients. Clin Liver Dis. 2011;15(4):727–51. https://doi.org/10.1016/j.cld.2011.08.002.
Rivera AV, Harriman G, Carrillo SA, Braunstein SL. Trends in methamphetamine use among men who have sex with men in New York City, 2004–2017. AIDS Behav. 2021;25(4):1210–8. https://doi.org/10.1007/s10461-020-03097-5.
Abara WE, Zlotorzynska M, Kirkcaldy RD, Sanchez T. Bacterial sexually transmitted infection testing and diagnoses among men who have sex with men and report prescription opioid misuse–American Men’s Internet Survey, 2017–2018. Ann Epidemiol. 2021;58:1–6. https://doi.org/10.1016/j.annepidem.2021.02.002.
Chin-Hong PV, Reid GE, Practice ASTIDCo. Human papillomavirus infection in solid organ transplant recipients: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019;33(9):e13590. https://doi.org/10.1111/ctr.13590.
Pernot S, Boucheron P, Pere H, Lucas ML, Veyer D, Fathallah N, et al. Comparison of anal cancer screening strategies including standard anoscopy, anal cytology, and HPV genotyping in HIV-positive men who have sex with men. Br J Cancer. 2018;119(3):381–6. https://doi.org/10.1038/s41416-018-0176-9.
Thompson MA, Horberg MA, Agwu AL, Colasanti JA, Jain MK, Short WR, et al. Primary care guidance for persons with human immunodeficiency virus: 2020 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2021;73(11):e3572–605. https://doi.org/10.1093/cid/ciaa1391.
Rosales BM, Langton-Lockton J, Hedley J, Cornall AM, Roberts JM, Garland SM, et al. Prevalence of anal cytological abnormalities and high-risk human papillomavirus prevalence in kidney transplant recipients: a cross-sectional study. Clin Transplant. 2021;35(12): e14476. https://doi.org/10.1111/ctr.14476.
Kumar RN, Stosor V. Organ transplantation in persons with HIV. AIDS. 2020;34(8):1107–16. https://doi.org/10.1097/QAD.0000000000002518.
Sparkes T, Lemonovich TL, Practice ASTIDCo. Interactions between anti-infective agents and immunosuppressants-guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clinical transplantation. 2019;33(9):e13510. https://doi.org/10.1111/ctr.13510.
Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Department of Health and Human Services. https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/AdultandAdolescentGL.pdf. Accessed 2 Jan 2022.
Dionne B. Key Principles of Antiretroviral Pharmacology. Infect Dis Clin North Am. 2019;33(3):787–805. https://doi.org/10.1016/j.idc.2019.05.006.
Tricot L, Teicher E, Peytavin G, Zucman D, Conti F, Calmus Y, et al. Safety and efficacy of raltegravir in HIV-infected transplant patients cotreated with immunosuppressive drugs. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2009;9(8):1946–52. https://doi.org/10.1111/j.1600-6143.2009.02684.x.
Di Biagio A, Rosso R, Siccardi M, D’Avolio A, Bonora S, Viscoli C. Lack of interaction between raltegravir and cyclosporin in an HIV-infected liver transplant recipient. J Antimicrob Chemother. 2009;64(4):874–5. https://doi.org/10.1093/jac/dkp269.
Cattaneo D, Puoti M, Sollima S, Moioli C, Foppa CU, Baldelli S, et al. Reduced raltegravir clearance in HIV-infected liver transplant recipients: an unexpected interaction with immunosuppressive therapy? J Antimicrob Chemother. 2016;71(5):1341–5. https://doi.org/10.1093/jac/dkv466.
Waldman G, Rawlings SA, Kerr J, Vodkin I, Aslam S, Logan C, et al. Successful optimization of antiretroviral regimens in treatment-experienced people living with HIV undergoing liver transplantation. Transplant infectious disease : an official journal of the Transplantation Society. 2019;21(6): e13174. https://doi.org/10.1111/tid.13174.
Guaraldi G, Cocchi S, Motta A, Ciaffi S, Conti C, Codeluppi M, et al. Differential dose adjustments of immunosuppressants after resuming boosted versus unboosted HIV-protease inhibitors postliver transplant. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2009;9(10):2429–34. https://doi.org/10.1111/j.1600-6143.2009.02778.x.
Schonder KS, Shullo MA, Okusanya O. Tacrolimus and lopinavir/ritonavir interaction in liver transplantation. Ann Pharmacother. 2003;37(12):1793–6. https://doi.org/10.1345/aph.1D076.
Deeks ED. Cobicistat: a review of its use as a pharmacokinetic enhancer of atazanavir and darunavir in patients with HIV-1 infection. Drugs. 2014;74(2):195–206. https://doi.org/10.1007/s40265-013-0160-x.
Hemmersbach-Miller M, Berg CL, Messina JA, Wolfe CR. Transplant drug interactions and a word of caution for the HIV provider. A case report. Open Forum Infect Dis. 2018;5(4):ofy070. https://doi.org/10.1093/ofid/ofy070.
Althoff KN, Gebo KA, Moore RD, Boyd CM, Justice AC, Wong C, et al. Contributions of traditional and HIV-related risk factors on non-AIDS-defining cancer, myocardial infarction, and end-stage liver and renal diseases in adults with HIV in the USA and Canada: a collaboration of cohort studies. Lancet HIV. 2019;6(2):e93–104. https://doi.org/10.1016/S2352-3018(18)30295-9.
Ellis KE, Nawas GT, Chan C, York L, Fisher J, Connick E, et al. Clinical outcomes following the use of archived proviral HIV-1 DNA genotype to guide antiretroviral therapy adjustment. Open Forum Infect Dis. 2020;7(1):ofz533. https://doi.org/10.1093/ofid/ofz533.
Patel SJ, Kuten SA, Musick WL, Gaber AO, Monsour HP, Knight RJ. Combination drug products for HIV-A word of caution for the transplant clinician. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg. 2016;16(8):2479–82. https://doi.org/10.1111/ajt.13826.
National Institute of Diabetes and Digestive and Kidney Diseases. LiverTox.: https://www.ncbi.nlm.nih.gov/books/NBK547852/. Accessed 2 Jan 2022.
Subramanian A, Sulkowski M, Barin B, Stablein D, Curry M, Nissen N, et al. MELD score is an important predictor of pretransplantation mortality in HIV-infected liver transplant candidates. Gastroenterology. 2010;138(1):159–64. https://doi.org/10.1053/j.gastro.2009.09.053.
Ragni MV, Eghtesad B, Schlesinger KW, Dvorchik I, Fung JJ. Pretransplant survival is shorter in HIV-positive than HIV-negative subjects with end-stage liver disease. Liver transplantation : official publication of the American Association for the Study of Liver Diseases and the International Liver Transplantation Society. 2005;11(11):1425–30. https://doi.org/10.1002/lt.20534.
Wall A, Lee GH, Maldonado J, Magnus D. Medical contraindications to transplant listing in the USA: a survey of adult and pediatric heart, kidney, liver, and lung programs. World J Surg. 2019;43(9):2300–8. https://doi.org/10.1007/s00268-019-05030-x.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Rebecca Kumar has received grants from Regeneron. Dr. Stosor has received grants from Eli Lilly and Company and the National Institutes of Health, speaker honorarium from Med Learning Group, and consulting fees from DiaSorin, Inc.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Transplant and Oncology
Rights and permissions
About this article

Cite this article
Kumar, R.N., Stosor, V. Advances in Liver Transplantation for Persons with Human Immunodeficiency Infection. Curr Infect Dis Rep 24, 39–50 (2022). https://doi.org/10.1007/s11908-022-00776-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11908-022-00776-3