
Abstract
The two major inflammatory bowel diseases, Crohn’s disease (CD) and ulcerative colitis (UC), represent clinicopathologic entities that traditionally have been diagnosed on the basis of a combination of clinical, radiologic, endoscopic, and histologic features. Serum perinuclear antineutrophil cytoplasmic antibodies (pANCA) and anti-Saccharomyces cerevisiae antibodies (ASCA) have recently been added to our diagnostic armamentarium. Several studies have demonstrated that UC-associated pANCAs recognize nuclear antigens. Additional studies have demonstrated that the pANCA human monoclonal antibody (mAb) Fab 5–3 reacts with histone H1 and with bacterial and mycobacterial antigens. Several reports have suggested that, in CD, pANCA and ASCA are correlated with colonic and small bowel disease respectively. One study found that higher ASCA levels were correlated with more aggressive CD. Serology may prove to be useful in predicting the evolution of indeterminate colitis. Magnetic resonance imaging (MRI) and leukocyte scintigraphy hold promise in identifying inflammatory CD. MRI enteroclysis is useful in identifying both luminal small bowel disease and extraluminal complications. A recent study of surveillance colonoscopy in extensive Crohn’s colitis showed a high risk of dysplasia and cancer.
Similar content being viewed by others


References and Recommended Reading
Rutgeerts P, Vermeire S: Clinical value of the detection of antibodies in the serum for diagnosis and treatment of inflammatory bowel disease. Gastroenterology 1998, 115:1006–1009.
Targan SR, Landers CJ, Cobb L, et al.: Perinuclear antineutrophil cytoplasmic antibodies are spontaneously produced by mucosal B cells of ulcerative colitis patients. J Immunol 1995, 155:3262–3267.
Saxon A, Shanahan F, Landers C, et al.: A distinct subset of antineutrophil cytoplasmic antibodies is associated with inflammatory bowel disease. J Allergy Clin Immunol 1990, 86:202–210.
Roozendaal C, Kallenberg CG: Are anti-neutrophil cytoplasmic antibodies (ANCA) clinically useful in inflammatory bowel disease (IBD)? Clin Exp Immunol 1999, 116:206–213.
Vidrich A, Lee J, James E, et al.: Segregation of pANCA antigenic recognition by DNase treatment of neutrophils: ulcerative colitis, type 1 autoimmune hepatitis, and primary sclerosing cholangitis. J Clin Immunol 1995, 15:293–299.
Billing P, Tahir S, Calfin B, et al.: Nuclear localization of the antigen detected by ulcerative colitis-associated perinuclear antineutrophil cytoplasmic antibodies. Am J Pathol 1995, 147:979–987.
Sobajima J, Ozaki S, Osakada F, et al.: Novel autoantigens of perinuclear anti-neutrophil cytoplasmic antibodies (P-ANCA) in ulcerative colitis: non-histone chromosomal proteins, HMG1 and HMG2. Clin Exp Immunol 1997, 107:135–140.
Sobajima J, Ozaki S, Uesugi H, et al.: Prevalence and characterization of perinuclear anti-neutrophil cytoplasmic antibodies (P-ANCA) directed against HMG1 and HMG2 in ulcerative colitis (UC). Clin Exp Immunol 1998, 111:402–407.
Terjung B, Herzog V, Worman HJ, et al.: Atypical antineutrophil cytoplasmic antibodies with perinuclear fluorescence in chronic inflammatory bowel diseases and hepatobiliary disorders colocalize with nuclear lamina proteins. Hepatology 1998, 28:332–340.
Terjung B, Spengler U, Sauerbruch T, Worman HJ: ‘Atypical p-ANCA’ in IBD and hepatobiliary disorders react with a 50-kilodalton nuclear envelope protein of neutrophils and myeloid cell lines. Gastroenterology 2000, 119:310–322. These elegant studies demonstrate that pANCA in UC, PSC, and AIH react with a nuclear envelope protein present in neutrophils and two myeloid cell lines. This protein likely resides within the nuclear lamina.
Eggena M, Cohavy O, Parseghian MH, et al.: Identification of histone H1 as a cognate antigen of the ulcerative colitisassociated marker antibody pANCA. J Autoimmun 2000, 14:83–97. The pANCA mAb Fab 5–3 recognizes histone H1.
Mizoguchi E, Mizoguchi A, Chiba C, et al.: Antineutrophil cytoplasmic antibodies in T-cell receptor alpha-deficient mice with chronic colitis. Gastroenterology 1997, 113:1828–1835.
Seibold F, Brandwein S, Simpson S, et al.: pANCA represents a cross-reactivity to enteric bacterial antigens. J Clin Immunol 1998, 18:153–160.
Cohavy O, Harth G, Horwitz M, et al.: Identification of a novel mycobacterial histone H1 homologue (HupB) as an antigenic target of pANCA monoclonal antibody and serum immunoglobulin A from patients with Crohn’s disease. Infect Immun 1999, 67:6510–6517.
Cohavy O, Bruckner D, Gordon LK, et al.: Colonic bacteria express an ulcerative colitis pANCA-related protein epitope. Infect Immun 2000, 68:1542–1548. These two studies demonstrate that the pANCA mAb Fab 5–3 recognizes antigens on Mycobacterium species, E. coli, and B. caccae.
Wei B, Dalwadi HN, Gordon LK, et al.: Molecular cloning of a Bacteroides caccae TonB-linked outer membrane protein identified by an inflammatory bowel disease marker antibody [abstract]. Gastroenterology 2001, 120:A519.
Main J, McKenzie H, Yeaman GR, et al.: Antibody to Saccharomyces cerevisiae (baker’s yeast) in Crohn’s disease. BMJ 1988, 297:1105–1106.
McKenzie H, Main J, Pennington CR, Parratt D: Antibody to selected strains of Saccharomyces cerevisiae (baker’s and brewer’s yeast) and Candida albicans in Crohn’s disease. Gut 1990, 31:536–538.
Sendid B, Colombel JF, Jacquinot PM, et al.: Specific antibody response to oligomannosidic epitopes in Crohn’s disease. Clin Diagn Lab Immunol 1996, 3:219–226.
Seibold F, Ruettten C, Scheurlen M, Goeke B: T cell response to mannans of Saccharomyces cerevisiae in inflammatory bowel disease [abstract]. Gastroenterology 2000, 118:A352.
Peeters M, Joossens S, Vermeire S, et al.: Diagnostic value of anti-Saccharomyces cerevisiae and antineutrophil cytoplasmic autoantibodies in inflammatory bowel disease. Am J Gastroenterol 2001, 96:730–734. The largest study to date of pANCA and ASCA test characteristics. Also contains data on a group of patients with IC.
Vasiliauskas EA, Plevy SE, Landers CJ, et al.: Perinuclear antineutrophil cytoplasmic antibodies in patients with Crohn’s disease define a clinical subgroup. Gastroenterology 1996, 110:1810–1819.
Satsangi J, Landers CJ, Welsh KI, et al.: The presence of anti-neutrophil antibodies reflects clinical and genetic heterogeneity within inflammatory bowel disease. Inflamm Bowel Dis 1998, 4:18–26.
Jamar-Leclerc N, Reumaux D, Duthilleul P, Colombel JF: Do pANCA define a clinical subgroup in patients with Crohn’s disease? Gastroenterology 1997, 112:316–317.
Quinton JF, Sendid B, Reumaux D, et al.: Anti-Saccharomyces cerevisiae mannan antibodies combined with antineutrophil cytoplasmic autoantibodies in inflammatory bowel disease: prevalence and diagnostic role. Gut 1998, 42:788–791.
Koutroubakis IE, Petinaki E, Mouzas IA, et al.: Anti-Saccharomyces cerevisiae mannan antibodies and antineutrophil cytoplasmic autoantibodies in Greek patients with inflammatory bowel disease. Am J Gastroenterol 2001, 96:449–454.
VasiliauskasEA, Kam LY, Karp LC, et al.: Marker antibody expression stratifies Crohn’s disease into immunologically homogeneous subgroups with distinct clinical characteristics. Gut 2000, 47:487–496. This large study suggests that pANCA and ASCA titers stratify CD into clinical subgroups with distinct disease distribution and aggressiveness.
Taylor KD, Plevy SE, Yang H, et al.: ANCA pattern and LTA haplotype relationship to clinical responses to anti-TNF antibody treatment in Crohn’s disease. Gastroenterology 2001, 120:1347–1355.
Vermeire S, Joossens S, Peeters M, et al.: ASCA and pANCA do not predict response to anti-TNFa (Remicade) treatment [abstract]. Gastroenterology 2000, 118:A570.
Bitton A, Peppercorn MA, Antonioli DA, et al.: Clinical, biological, and histologic parameters as predictors of relapse in ulcerative colitis. Gastroenterology 2001, 120:13–20.
Joossens S, Cassagnou M, Vermeire S, et al.: Are anti-Saccharomyces cerevisiae antibodies (ASCA) and perinuclear antineutrophil cytoplasmic antibodies (pANCA) useful in indeterminate colitis? A prospective follow-up study [abstract]. Gastroenterology 2000, 118:A886.
Sutton CL, Yang H, Li Z, et al.: Familial expression of anti-Saccharomyces cerevisiae mannan antibodies in affected and unaffected relatives of patients with Crohn’s disease. Gut 2000, 46:58–63. This study shows that ASCA status is a familial trait that may be genetically determined.
Vermeire S, Peeters M, Vlietinck R, et al.: Anti-Saccharomyces cerevisiae antibodies (ASCA), phenotypes of IBD, and intestinal permeability: a study in IBD families. Inflamm Bowel Dis 2001, 7:8–15.
Hugot JP, Chamaillard M, Zouali H, et al.: Association of NOD2 leucine-rich repeat variants with susceptibility to Crohn’s disease. Nature 2001, 411:599–603.
Ogura Y, Bonen DK, Inohara N, et al.: A frameshift mutation in NOD2 associated with susceptibility to Crohn’s disease. Nature 2001, 411:603–606.
Vermeire S, Joossens S, Peeters M, et al.: Comparative study of ASCA (Anti-Saccharomyces cerevisiae antibody) assays in inflammatory bowel disease. Gastroenterology 2001, 120:827–833. Different ASCA assays have large variations in sensitivity.
Dubinsky MC, Ofman JJ, Urman M, et al.: Clinical utility of serodiagnostic testing in suspected pediatric inflammatory bowel disease. Am J Gastroenterol 2001, 96:758–765.
Sandborn WJ, Landers CJ, Tremaine WJ, Targan SR: Antineutrophil cytoplasmic antibody correlates with chronic pouchitis after ileal pouch-anal anastomosis. Am J Gastroenterol 1995, 90:740–747.
Fleshner PR, Vasiliauskas EA, Kam LY, et al.: High level perinuclear antineutrophil cytoplasmic antibody (pANCA) in ulcerative colitis patients before colectomy predicts the development of chronic pouchitis after ileal pouch anal anastomosis [abstract]. Gastroenterology 1999, 116:A716.
Panaccione R, Sandborn WJ, Tremaine WJ, et al.: pANCA is associated with chronic pouchitis and predicts the future occurrence of acute pouchitis following ileal pouch-anal anastomosis (IPAA) [abstract]. Gastroenterology 1999, 116:A791.
Charron M: Pediatric inflammatory bowel disease imaged with Tc-99m white blood cells. Clin Nucl Med 2000, 25:708–715.
Molnar T, Papos M, Gyulai C, et al.: Clinical value of technetium-99m-HMPAO-labeled leukocyte scintigraphy and spiral computed tomography in active Crohn’s disease. Am J Gastroenterol 2001, 96:1517–1521.
Charron M, Di Lorenzo C, Kocoshis S: Are 99mTc leukocyte scintigraphy and SBFT studies useful in children suspected of having inflammatory bowel disease? Am J Gastroenterol 2000, 95:1208–1212.
Davison SM, Chapman S, Murphy MS: 99mTc-HMPAO leucocyte scintigraphy fails to detect Crohn’s disease in the proximal gastrointestinal tract. Arch Dis Child 2001, 85:43–46.
Maccioni F, Viscido A, Broglia L, et al.: Evaluation of Crohn disease activity with magnetic resonance imaging. Abdom Imaging 2000, 25:219–228.
Low RN, Francis IR, Politoske D, Bennett M: Crohn’s disease evaluation: comparison of contrast-enhanced MR imaging and single-phase helical CT scanning. J Magn Reson Imaging 2000, 11:127–135.
Rieber A, Wruk D, Potthast S, et al.: Diagnostic imaging in Crohn’s disease: comparison of magnetic resonance imaging and conventional imaging methods. Int J Colorectal Dis 2000, 15:176–181.
Umschaden HW, Szolar D, Gasser J, et al.: H: Small-bowel disease: comparison of MR enteroclysis images with conventional enteroclysis and surgical findings. Radiology 2000, 215:717–725.
D‘Arienzo A, Scaglione G, Vicinanza G, et al.: Magnetic resonance imaging with ferumoxil, a negative superparamagnetic oral contrast agent, in the evaluation of ulcerative colitis. Am J Gastroenterol 2000, 95:720–724.
Ludwig D, Wiener S, Bruning A, et al.: Mesenteric blood flow is related to disease activity and risk of relapse in Crohn’s disease: a prospective follow-up study. Am J Gastroenterol 1999, 94:2942–2950.
Ludwig D, Wiener S, Bruning A, et al.: Mesenteric blood flow is related to disease activity and risk of relapse in ulcerative colitis: a prospective follow up study. Gut 1999, 45:546–552.
Tarjan Z, Toth G, Gyorke T, et al.: Ultrasound in Crohn’s disease of the small bowel. Eur J Radiol 2000, 35:176–182.
Skehan SJ, Issenman R, Mernagh J, et al.: 18F-fluorodeoxyglucose positron tomography in diagnosis of paediatric inflammatory bowel disease. Lancet 1999, 354:836–837.
Bicik I, Bauerfeind P, Breitbach T, et al.: Inflammatory bowel disease activity measured by positron-emission tomography. Lancet 1997, 350:262.
Kurahara K, Matsumoto T, Iida M, et al.: Clinical and endoscopic features of nonsteroidal anti-inflammatory drug-induced colonic ulcerations. Am J Gastroenterol 2001, 96:473–480.
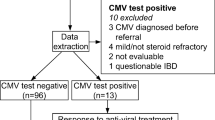
Cottone M, Pietrosi G, Martorana G, et al.: Prevalence of cytomegalovirus infection in severe refractory ulcerative and Crohn’s colitis. Am J Gastroenterol 2001, 96:773–775. CMV infection can complicate chronic colitis and cause severe, pseudo-steroid-refractory disease.
Imperiali G, Meucci G, Alvisi C, et al.: Segmental colitis associated with diverticula: a prospective study. Gruppo di Studio per le Malattie Infiammatorie Intestinali (GSMII). Am J Gastroenterol 2000, 95:1014–1016.
Eaden J, Abrams K, Ekbom A, et al.: Colorectal cancer prevention in ulcerative colitis: a case-control study. Aliment Pharmacol Ther 2000, 14:145–153.
Heuschen UA, Hinz U, Allemeyer EH, et al.: Backwash ileitis is strongly associated with colorectal carcinoma in ulcerative colitis. Gastroenterology 2001, 120:841–847. Report from the first study to suggest that backwash ileitis is a marker of increased colon cancer risk in UC.
Friedman S, Rubin PH, Bodian C, et al.: Screening and surveillance colonoscopy in chronic Crohn’s colitis. Gastroenterology 2001, 120:820–826. This report is from a study of colonoscopic surveillance of 259 patients with chronic extensive Crohn’s colitis. Dysplasia or cancer was detected in 12%.
Engelsgjerd M, Farraye FA, Odze RD: Polypectomy may be adequate treatment for adenoma-like dysplastic lesions in chronic ulcerative colitis. Gastroenterology 1999, 117:1288–1294.
Rubin PH, Friedman S, Harpaz N, et al.: Colonoscopic polypectomy in chronic colitis: conservative management after endoscopic resection of dysplastic polyps. Gastroenterology 1999, 117:1295–1300.
Eaden JA, Ward BA, Mayberry JF: How gastroenterologists screen for colonic cancer in ulcerative colitis: an analysis of performance. Gastrointest Endosc 2000, 51:123–128.
Thompson-Fawcett MW, Rust NA, Warren BF, Mortensen NJ: Aneuploidy and columnar cuff surveillance after stapled ileal pouch-anal anastomosis in ulcerative colitis. Dis Colon Rectum 2000, 43:408–413.
O‘Riordain MG, Fazio VW, Lavery IC, et al.: Incidence and natural history of dysplasia of the anal transitional zone after ileal pouch-anal anastomosis: results of a five-year to ten-year follow-up. Dis Colon Rectum 2000, 43:1660–1665.
Veress B, Reinholt FP, Lindquist K, et al.: Long-term histomorphological surveillance of the pelvic ileal pouch: dysplasia develops in a subgroup of patients. Gastroenterology 1995, 109:1090–1097.
Gullberg K, Stahlberg D, Liljeqvist L, et al.: Neoplastic transformation of the pelvic pouch mucosa in patients with ulcerative colitis. Gastroenterology 1997, 112:1487–1492.
Sarigol S, Wyllie R, Gramlich T, et al.: Incidence of dysplasia in pelvic pouches in pediatric patients after ileal pouch-anal anastomosis for ulcerative colitis. J Pediatr Gastroenterol Nutr 1999, 28:429–434.
Ettorre GM, Pescatori M, Panis Y, et al.: Mucosal changes in ileal pouches after restorative proctocolectomy for ulcerative and Crohn’s colitis. Dis Colon Rectum 2000, 43:1743–1748.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Dassopoulos, T. Diagnostic methodologies: serology, endoscopy, and radiology. Curr Gastroenterol Rep 3, 491–499 (2001). https://doi.org/10.1007/s11894-001-0070-z
Issue Date:
DOI: https://doi.org/10.1007/s11894-001-0070-z