
Abstract
Purpose of Review
Statins are routinely applied in patients with coronary artery disease, as they allow significantly to reduce blood cholesterol levels. Although those drugs are endorsed by current guidelines and prescribed routinely, a substantial portion of patients are still statin-intolerant and image-piloted strategies may then be helpful to identify patients that need further intensified treatment, e.g., to initiate treatment with proprotein convertase subtilisin / kexin type 9 inhibitors (PCSK9i). In addition, it has also been advocated that statins exhibit nonlipid, cardio-protective effects including improved cardiac nerve integrity, blood flow, and anti-inflammatory effects in congestive heart failure (HF) patients.
Recent Findings
In subjects after myocardial infarction treated with statins, 123II-metaiodobenzylguanidine (MIBG) scintigraphy has already revealed enhanced cardiac nerve function relative to patients without statins. In addition, all of those aforementioned statin-targeted pathways in HF can be visualized and monitored using dedicated cardiac radiotracers, e.g., 123I-MIBG or 18F-AF78 (for cardiac nerve function), 18F-flurpiridaz (to determine coronary flow) or 68Ga-PentixaFor (to detect inflammation).
Summary
Statins exhibit various cardio-beneficial effects, including improvement of cardiac nerve function, blood flow, and reduction of inflammation, which can all be imaged using dedicated nuclear cardiac radiotracers. This may allow for in vivo monitoring of statin-induced cardioprotection beyond lipid profiling in HF patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prescription of statins (3-hydroxy-3-methyl-glutaryl-coenzyme A reductase inhibitor [HMG-CoA]) causes a relevant decrease of hepatic cholesterol, thereby exhibiting substantial cardioprotective effects [1]. In this regard, a 1.0 mmol/L reduction of LDL cholesterol can prevent the incidence of major cardiovascular events, including stroke, myocardial infarction (MI), or revascularization by almost 10% [2]. Of note, in a recent meta-analysis pooling 170,000 patients of 26 prospective trials, the authors even conclude on an incremental value, leading to a potential risk reduction of 40–50% by LDL cholesterol reduction by 2–3 mmol/L [2]. Beyond exerting a beneficial effect on blood cholesterol level [1], mainly preclinical studies reported on an additional impact on cardiac autonomic function, e.g., by inhibition of angiotensin type II, also leading to improved left ventricular function [3]. Moreover, statins may also enhance epicardial perfusion in patients after MI scheduled for percutaneous coronary intervention (PCI) [4], further supporting the notion of a complex interplay between hepatic-derived reduction of blood cholesterol, cardiac nerve integrity, and myocardial blood flow [3, 4]. A recent study investigating 4622 patients who underwent cardiac magnetic resonance imaging reported that 17% received statins [5]. Those individuals had significantly less wall thickening relative to controls, which may be partially explained by statin-related reduction of oxidative stress [5], followed by decreased production of growth factors, but also to increased levels of nitric oxide synthase activity, leading to improved blood flow [6]. Further cardioprotective effects may also include anti-inflammatory components, as demonstrated by reduced C-reactive protein levels in individuals under regular statin prescription [7]. Of note, chronic heart failure is characterized by all of those pathophysiological pillars, thereby indicating that regular statin prescription may not only lower cholesterol blood levels but also exert relevant nonlipid therapeutic effects in patients affected with this disease [8]. In addition, those “off-target” effects of statins beyond lipid profiling may all be visualized and monitored by nuclear cardiac imaging techniques, including assessment of autonomous nerve function of the heart, myocardial blood flow, and pro-inflammatory activity (Fig. 1) [9]. As such, in the present review, we aimed to provide a brief overview of dedicated nuclear cardiac radiotracers applied in the context of lipid-lowering medication. By providing various clinical scenarios, we will also discuss how molecular imaging can be of relevance for the referring treating cardiologist when statins are prescribed.

Beyond lowering cholesterol, statins may also exert beneficial effects, including improvement of endothelial function leading to improved blood flow, modulation of the sympathetic nervous and renin angiotensin aldosterone system, or immunomodulation. All of these pathophysiological pillars can be imaged using dedicated nuclear cardiac imaging techniques, including perfusion, neurohumoral, or inflammatory-targeted imaging and thus, those SPECT or PET radiotracers may allow to decipher the beneficial effects on every pathophysiological pathway. NE, norepinephrine; MIBG, metaiodobenzylguanidine; CXCR4, C-X-C motif chemokine receptor 4; FAPI, fibroblast activation inhibitor. Created with BioRender.com
Clinical Benefit of Conducting Nuclear Imaging for Statin Prescription
Statins have already been proposed as part of a polypill, including multiple blood-lowering drugs and aspirin in patients post-MI [10]. In this regard, a fixed-dose concept is preferred over an individual dosage concept, thereby questioning the use of nuclear cardiac imaging techniques to determine the most appropriate drug dosage or to identify patients that benefit the most from treatment initiation [9]. In addition, side effects due to statins may not occur frequently, including myopathy or rhabdomyolysis [1]. Also summarized as statin-related muscle symptoms (SRMS) [1], it may be also debatable whether single photon emission computed tomography (SPECT) or positron emission tomography (PET) may be suitable to determine such high-risk patients if those SRMS are rare [9]. Nonetheless, there is a substantial portion of patients that do not respond to statins [11]. In those subjects with statin intolerance, the PCSK9i, which allows for the degradation of the hepatocyte LDL receptor, maybe a potential alternative to commonly prescribed HMG-CoA [12]. PCSK9i, however, is higher-priced, thereby indicating a need to identify patients that would benefit from such sophisticated lipid-lowering drugs, e.g., by risk stratification using nuclear cardiac imaging [13]. As such, an image-piloted strategy could also be integrated into the therapeutic algorithm of those subjects [9], e.g., to enhance the therapeutic efficacy of combination strategies using regular statins and PCSK9i [12]. Further clinical applications of image-guided nuclear cardiology imaging studies may also emerge once the beneficial effects of statins on blood flow, cardiac autonomic function, and anti-inflammation have been further determined.
Molecular Imaging Targets in Patients under Statin
Targeting Cardiac Nerve Integrity
First applied to symptomatic heart failure patients in a prospective setting, the “AdreView Myocardial Imaging for Risk Evaluation in Heart Failure (ADMIRE-HF)” trial has provided evidence that the catecholamine analog radiotracer 123I-metaiodobenzylguanidine (MIBG) may allow determining patients that are prone to NYHA functional class progression, life-threatening arrhythmias or myocardial death [14]. As a commonly derived metric, the heart-to-mediastinum ratio (HMR) allows for quantifying the amount of denervated myocardium, with reduced HMR being linked to an increasing event rate [14]. This SPECT radiopharmaceutical has been applied by Takahashi and coworkers to subjects with ST-segment elevation MI under statins and was then compared to a control group also diagnosed with infarction but not being treated with statins [15]. Individuals under statins showed higher HMR values on a delayed image protocol along with a lower washout rate, thereby indicating that 123I-MIBG allows to monitoring the beneficial effects of statin therapy in patients post-MI. Of note, those findings were accompanied by plasma procollagen type III amino terminal peptide (PIIINP), which is used to determine cardiac fibrosis. This biomarker and left ventricular performance were both improved in the statin group, further supporting the notion that other independent clinical parameters suggest a benefit of statin therapy similar to HMR [15]. Despite those interesting results in the context of SPECT, recent radiochemical developments led to the increasing use of PET agents for identifying areas of cardiac nerve injury [16]. Relative to SPECT, those PET agents may provide a higher spatiotemporal resolution, in particular when combined with F18 radiochemistry [17]. Those compounds include but are not limited to 18F-AF78, 18F-flubrobenguane, or 18F-DOPA [17, 18, 19••, 20]. If image-piloted strategies should be applied in the context of statins, e.g., to determine individuals that should be treated with PCSK9i and/or combination approaches, those more sophisticated PET radiotracers could then be used [13]. Beyond assessing cardiac nerve integrity, hypercholesterolemia is also tightly linked to the renin–angiotensin–aldosterone system, mainly due to the release of angiotensin II [21] and thereby supporting the notion that angiotensin-targeting PET radiotracers may also be applied in the context of statin, e.g., by using the angiotensin-converting-enzyme-targeting 18F-fluorobenzoyl-lisinopril [22] or AT-1 receptor ligand 11C-KR31173, which is also directed towards the angiotensin II subtype 1 receptor (AT1R) of the human heart [23]. The recently introduced PET radiotracer 18F-FV45 could also be selectively blocked by the clinical drug valsartan, and thus, this agent may further expand the current armamentarium of radiotracers targeting angiotensin [24].
Targeting Cardiac Blood Flow
As alluded to earlier, a recent study including 4622 patients demonstrated that individuals under statin showed less wall thickening relative to controls [5]. As a possible explanation, statins may increase levels of nitric oxide synthase activity, improving blood flow [6]. Cerit and coworkers have provided further evidence of this hypothesis by enrolling 80 patients with a diagnosis of stable coronary artery disease scheduled for PCI [4]. Upon multiple logistic regression, statin pre-treatment along with high-sensitivity C-reactive protein (CRP) were independent predictors of post-interventional epicardial perfusion [4]. This is in line with an observation of Briguori et al. who also observed a potential beneficial impact of statins on coronary blood flow. In their study, the incidence of PCI-related peri-interventional MI was significantly reduced in statin-pretreated subjects. In this regard, the authors recommended a high-dose approach of 80 mg loading of atorvastatin one day prior to the elective intervention [25]. Taken together, statin may also play a crucial role in improving blood flow, and thus, myocardial perfusion imaging could play an important role to determine statin-related effects of improved coronary flow. As a workhorse in nuclear cardiology, the SPECT radiotracers 99mTc-sestamibi, -tetrofosmin, and Thallium 201 could then be applied in individuals under statin therapy and compared to controls not receiving a statin, e.g., in the setting of MI followed by reperfusion [9]. Again, PET may provide increased diagnostic accuracy and multiple blood flow-targeting radiotracers would be also available. Those include short-lived radiotracers such as 13N ammonia (half-life, 10 min), oxygen-15 water (2 min), or 82Rb (76 s), but also F18-labeled cardiac perfusion radiotracers, e.g., flurpiridaz [9, 17]. The latter radiotracer has significant advantages when compared to other radiotracers used for this purpose, as the longer half-life of 110 min would also allow conducting of early and delayed studies and high throughput in a busy PET center [17, 26]. In addition, it has the unique potential for injecting the radiotracer at peak exercise on the treadmill, which cannot be performed with the current FDA-approved PET radiotracers [27, 28].
Targeting Inflammation
Beyond lipid-lowering effects, statins may also exert anti-inflammatory effects as another pathophysiological pillar of congestive heart failure. Among others, results of the CARE trial (Cholesterol and Recurrent Events) first reported a dual-targeting beneficial effect, including lower cholesterol levels and reduction of CRP [29]. Those findings were further corroborated in the JUPITER trial (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin), demonstrating that even in otherwise healthy subjects not diagnosed with hyperlipidemia but with elevated high-sensitive CRP, statins reduced the incidence of cardiovascular events, along with a substantial CRP decrease of 37% [30]. As such, statins may also exhibit a nonlipid, anti-inflammatory effect. Of note, inflammatory-targeted radiotracers are also penetrating the clinical arena. While 18F-fluorodeoxyglucose would be available at every PET center with access to a cyclotron (or via dispatch from a remote cyclotron facility) [31], challenging preparation protocols, including prolonged fasting, may hamper its widespread clinical adoption in the context of statin-related molecular imaging [32]. The C-X-C motif chemokine receptor 4 (CXCR4)-directed PET agent 68Ga-PentixaFor has already proven to provide predictive information in patients post-MI. Such a CXCR4-targeting, noninvasive local read-out of the inflammatory burden in the infarcted area could even better identify high-risk patients prone to later major cardiovascular events than established clinical markers, including creatine kinase, CRP, or leukocytes [33•]. Of note, 68Ga-PentixaFor does not require any particular patient preparation [34] and thus, patients with and without statins after myocardial infarction and guideline-compatible intervention could be easily compared using this radiotracer, thereby allowing to determine the anti-inflammatory effects of statins in vivo.
Conclusions
Statins are routinely applied in patients with coronary artery disease, as they allow significantly to reduce blood cholesterol levels. Although statins are prescribed routinely, a substantial portion of patients are still statin-intolerant and image-piloted strategies, including molecular cardiac imaging, may then be helpful to identify patients that need further intensified treatment, e.g., initiation of PCSK9i. In addition, it has also been advocated that statins exhibit beneficial effects, including improved cardiac nerve integrity, blood flow, and anti-inflammatory effects in congestive heart failure. All of these pathophysiological pillars could be addressed using dedicated nuclear cardiac SPECT or PET radiopharmaceuticals, including 123I-MIBG, 18F-AF78, 18F-flurpiridaz, or 68Ga-PentixaFor. As such, those cardiac radiotracers may then allow for in vivo monitoring of statin-induced cardioprotection beyond lipid profiling in heart failure.
References
Papers of particular interest, published recently, have been highlighted as • Of importance •• Of major importance
Adhyaru BB, Jacobson TA. Safety and efficacy of statin therapy. Nat Rev Cardiol. 2018;15:757–69.
Cholesterol Treatment Trialists C, Baigent C, Blackwell L, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–81.
Gao L, Wang W, Li YL, et al. Simvastatin therapy normalizes sympathetic neural control in experimental heart failure: roles of angiotensin II type 1 receptors and NAD(P)H oxidase. Circulation. 2005;112:1763–70.
Cerit L, Duygu H, Gulsen K, Gunsel A. Effect of statins on coronary blood flow after percutaneous coronary intervention in patients with stable coronary artery disease. Neth Heart J. 2017;25:258–63.
Statins associated with improved heart structure and function. 2017. https://www.escardioorg/The-ESC/Press-Office/Press-releases/Statins-associated-with-improved-heart-structure-and-function, last Assessed 2 Aug 2022.
von Haehling S, Anker SD, Bassenge E. Statins and the role of nitric oxide in chronic heart failure. Heart Fail Rev. 2003;8:99–106.
Ridker PM, Cannon CP, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med. 2005;352:20–8.
McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42:3599–726.
Werner RA, Thackeray JT, Diekmann J, Weiberg D, Bauersachs J, Bengel FM. The changing face of nuclear cardiology: guiding cardiovascular care toward molecular medicine. J Nucl Med. 2020;61:951–61.
Robinson JG. Is a statin as part of a polypill the answer? Curr Atheroscler Rep. 2009;11:15–22.
Harrison TN, Hsu JY, Rosenson RS, et al. Unmet patient need in statin intolerance: the clinical characteristics and management. Cardiovasc Drugs Ther. 2018;32:29–36.
Bays H, Gaudet D, Weiss R, et al. Alirocumab as add-on to atorvastatin versus other lipid treatment strategies: ODYSSEY OPTIONS I randomized trial. J Clin Endocrinol Metab. 2015;100:3140–8.
Werner RA, Thackeray JT, Bengel FM. Does lipid-lowering medication improve cardiac sympathetic nerve integrity? J Nucl Cardiol. 2021;28:1458–60.
Jacobson AF, Senior R, Cerqueira MD, et al. Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events in heart failure. Results of the prospective ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) study. J Am Coll Cardiol. 2010;55:2212–21.
Takahashi S, Kasama S, Toyama T, et al. Assessment of therapeutic effects of statin on cardiac sympathetic nerve activity after reperfusion therapy in patients with first ST-segment elevation myocardial infarction and normal low-density lipoprotein cholesterol. J Nucl Cardiol. 2021;28:1449–57.
Werner RA, Chen X, Hirano M, et al. SPECT vs. PET in cardiac innervation imaging: clash of the titans. Clin Transl Imaging. 2018;6:293–303.
Werner RA, Chen X, Rowe SP, Lapa C, Javadi MS, Higuchi T. Recent paradigm shifts in molecular cardiac imaging-establishing precision cardiology through novel (18)F-labeled PET radiotracers. Trends Cardiovasc Med. 2020;30:11–9.
Chen X, Fritz A, Werner RA, et al. Initial Evaluation of AF78: a Rationally designed fluorine-18-labelled PET radiotracer targeting norepinephrine transporter. Mol Imaging Biol. 2020;22:602–11.
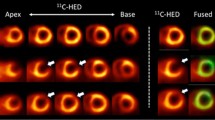
•• Zelt JGE, Britt D, Mair BA, et al. Regional distribution of fluorine-18-flubrobenguane and carbon-11-hydroxyephedrine for cardiac PET imaging of sympathetic innervation. JACC Cardiovasc Imaging. 2021;14:1425–36. This study showed that the 18F-labeled cardiac innervation radiotracer provides equivalent information on cardiac denervation when compared to its established 11C-labeled equivalent. 18F-labeled radiotracers, however, have the advantage of distribution to remote PET/CT facilities due their longer half-life.
Werner RA, Rischpler C, Onthank D, et al. Retention kinetics of the 18F-labeled sympathetic nerve PET tracer LMI1195: comparison with 11C-hydroxyephedrine and 123I-MIBG. J Nucl Med. 2015;56:1429–33.
Daugherty A, Rateri DL, Lu H, Inagami T, Cassis LA. Hypercholesterolemia stimulates angiotensin peptide synthesis and contributes to atherosclerosis through the AT1A receptor. Circulation. 2004;110:3849–57.
Dilsizian V, Eckelman WC, Loredo ML, Jagoda EM, Shirani J. Evidence for tissue angiotensin-converting enzyme in explanted hearts of ischemic cardiomyopathy using targeted radiotracer technique. J Nucl Med. 2007;48:182–7.
Fukushima K, Bravo PE, Higuchi T, et al. Molecular hybrid positron emission tomography/computed tomography imaging of cardiac angiotensin II type 1 receptors. J Am Coll Cardiol. 2012;60:2527–34.
Chen X, Hirano M, Werner RA, Decker M, Higuchi T. Novel (18)F-labeled PET imaging agent FV45 targeting the renin-angiotensin system. ACS Omega. 2018;3:10460–70.
Briguori C, Visconti G, Focaccio A, et al. Novel approaches for preventing or limiting events (Naples) II trial: impact of a single high loading dose of atorvastatin on periprocedural myocardial infarction. J Am Coll Cardiol. 2009;54:2157–63.
Berman DS, Maddahi J, Tamarappoo BK, et al. Phase II safety and clinical comparison with single-photon emission computed tomography myocardial perfusion imaging for detection of coronary artery disease: flurpiridaz F 18 positron emission tomography. J Am Coll Cardiol. 2013;61:469–77.
Werner RA, Chen X, Rowe SP, Lapa C, Javadi MS, Higuchi T. Moving into the next era of PET myocardial perfusion imaging: introduction of novel (18)F-labeled tracers. Int J Cardiovasc Imaging. 2019;35:569–77.
Dilsizian V, Taillefer R. Journey in evolution of nuclear cardiology: will there be another quantum leap with the F-18-labeled myocardial perfusion tracers? JACC Cardiovasc Imaging. 2012;5:1269–84.
Ridker PM, Rifai N, Pfeffer MA, Sacks F, Braunwald E. Long-term effects of pravastatin on plasma concentration of C-reactive protein. The Cholesterol and Recurrent Events (CARE) Investigators. Circulation. 1999;100:230–5.
Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359:2195–207.
Ducharme J, Goertzen AL, Patterson J, Demeter S. Practical aspects of 18F-FDG PET when receiving 18F-FDG from a distant supplier. J Nucl Med Technol. 2009;37:164–9.
Dilsizian V, Bacharach SL, Beanlands RS, et al. ASNC imaging guidelines/SNMMI procedure standard for positron emission tomography (PET) nuclear cardiology procedures. J Nucl Cardiol. 2016;23:1187–226.
• Werner RA, Koenig T, Diekmann J, et al. CXCR4-targeted imaging of post-infarct myocardial tissue inflammation: prognostic value after reperfused myocardial infarction. JACC Cardiovasc Imaging. 2022;15:372–4. Findings from this study showed that a local non-invasive molecular imaging read-out of the inflammation in the infarcted area may have better predictive potential to identify high-risk patients prone to later major cardiovascular events than other established clinical parameters right after myocardial infarction.
Buck AK, Serfling SE, Lindner T, et al. CXCR4-targeted theranostics in oncology. Eur J Nucl Med Mol Imaging. 2022.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work has been supported by the German Research Foundation (453989101, TH, RAW; 507803309, RAW), the Okayama University (RECTOR Program, TH), and the Japan Society for the Promotion of Science (21K19450, TH).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
The present study did not involve human or animal subjects.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Nuclear Cardiology
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Higuchi, T., Serfling, S.E., Rowe, S.P. et al. Therapeutic Effects of Lipid Lowering Medications on Myocardial Blood Flow, Inflammation, and Sympathetic Nerve Activity Using Nuclear Techniques. Curr Cardiol Rep 24, 1849–1853 (2022). https://doi.org/10.1007/s11886-022-01792-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11886-022-01792-4