
Abstract
Background
Esophagectomy through cervico-thoraco-abdominal approach is a useful surgical technique in treating patients with esophageal cancer. However, the cervical reconstruction is also known to have a high rate of anastomotic leakage, as well as anastomotic stricture, intrathoracic stomach syndrome, reflux esophagitis and other complications, thereby influencing postoperative recovery and quality of life.
Aims
The objective of this study was to investigate whether tubular stomach is superior to whole stomach in reducing anastomotic leakage for esophageal reconstruction through the cervico-thoraco-abdominal (3-field) approach.
Methods
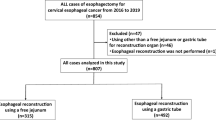
A total of 850 patients undergoing the 3-field esophagectomy were retrospectively included in this study and divided into a tubular stomach reconstruction group (Group A, n = 453) and a whole stomach reconstruction group (Group B, n = 397). All patients underwent esophagectomy through right thorax, left cervical part, abdominal triple incisions and done in esophageal reconstruction by hand-sewn two-layer anastomosis.
Results
Results revealed that in comparison with whole stomach, esophageal reconstruction with tubular stomach had a lower incidence of anastomotic leakage (5.5 vs. 9.3 %, P < 0.05), less manifestation of intrathoracic syndrome (3.3 vs. 9.8 %, P < 0.001) and less occurence of reflux esophagitis (5.1 vs. 11.1 %, P < 0.01). However, for the incidence of anastomotic stricture, there was no significant difference between the two groups (9.3 vs. 9.8 %).
Conclusions
This observation study suggests that for esophageal cancer patients undergoing the 3-field esophagectomy tubular stomach is better than whole stomach for esophageal reconstruction as reflected by a reduced postoperative anastomotic leakage, intrathoracic syndrome and reflux esophagitis.
Similar content being viewed by others


References
Udagawa H, Akiyama H (2001) Surgical treatment of esophageal cancer: Tokyo experience of the three-field technique. Dis Esophagus 14(2):110–114
Altorki N, Kent M, Ferrara C et al (2002) Three-field lymph node dissection for squamous cell and adenocarcinoma of the esophagus. Ann Surg 236(2):177–183
Lerut T, Coosemans W, Decker G et al (2004) Extended surgery for cancer of the esophagus and gastroesophageal junction. J Surg Res 117(1):58–63
Orringer MB, Marshall B, Iannettoni MD (2000) Eliminating the cervical esophagogastric anastomotic leak with a side-to-side stapled anastomosis. J Thorac Cardiovasc Surg 119(2):277–288
Cooke DT, Lin GC, Lau CL et al (2009) Analysis of cervical esophagogastric anastomotic leaks after transhiatal esophagectomy: risk factors, presentation, and detection. Ann Thorac Surg 88(1):177–184 (discussion 184-185)
Biere SS, Maas KW, Cuesta MA et al (2011) Cervical or thoracic anastomosis after esophagectomy for cancer: a systematic review and meta-analysis. Dig Surg 28(1):29–35
Ndoye JM, Dia A, Ndiaye A et al (2006) Arteriography of three models of gastric oesophagoplasty: the whole stomach, a wide gastric tube and a narrow gastric tube. Surg Radiol Anat 28(5):429–437
Poghosyan T, Gaujoux S, Chirica M et al (2011) Functional disorders and quality of life after esophagectomy and gastric tube reconstruction for cancer. J Visc Surg 148(5):e327–e335
Kim HK, Choi YH, Shim JH et al (2008) Endoscopic evaluation of the quality of the anastomosis after esophagectomy with gastric tube reconstruction. World J Surg 32(9):2010–2014
Urschel JD (1995) Esophagogastrostomy anastomotic leaks complicating esophagectomy: a review. Am J Surg 169(6):634–640
Fang W, Kato H, Chen W et al (2001) Comparison of surgical management of thoracic esophageal carcinoma between two referral centers in Japan and China. Jpn J Clin Oncol 31(5):203–208
Orringer MB, Marshall B, Chang AC et al (2007) Two thousand transhiatal esophagectomies: changing trends, lessons learned. Ann Surg 246(3):363–374
Nigro JJ, Hagen JA, DeMeester TR et al (1999) Prevalence and location of nodal metastasis in distal esophageal adenocarcinoma confined to the wall: implication for therapy. J Thorac Cardiovasc Surg 117(1):16–25
Zhang CB, Li J, Zheng J et al (2005) Feasible study for construction of gastric tube in easophageal reconstruction. J Henan Med Univ 2(3):175–179
Liebermann-Meffert DM, Meier R, Siewert JR (1992) Vascular anatomy of the gastric tube used for esophageal reconstruction. Ann Thorac Surg 54(6):1110–1115
Lerut TE, van Lanschot JJ (2004) Chronic symptoms after subtotal or partial oesophagectomy: diagnosis and treatment. Best Pract Res Clin Gastroenterol 18(5):901–915
Zhang C, Wu QC, Hou PY et al (2011) Impact of the method of reconstruction after oncologic oesophagectomy on quality of life—a prospective, randomised study. Eur J Cardiothorac Surg 39(1):109–114
D’Journo XB, Martin J, Ferraro P et al (2008) The esophageal remnant after gastric interposition. Dis Esophagus 21(5):377–388
Barbera L, Kemen M, Wegener M et al (1994) Effect of site and width of stomach tube after esophageal resection on gastric emptying. Zentralbl Chir 119:240–244
Bemelman WA, Taat CW, Slors JF et al (1995) Delayed postoperative emptying after esophageal resection is dependent on the size of the gastric substitute. J Am Coll Surg 180(4):461–464
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shu, YS., Sun, C., Shi, WP. et al. Tubular stomach or whole stomach for esophagectomy through cervico-thoraco-abdominal approach: a comparative clinical study on anastomotic leakage. Ir J Med Sci 182, 477–480 (2013). https://doi.org/10.1007/s11845-013-0917-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-013-0917-y